A
ccording to data released by the Chinese Primary Care Association,(1) 30% of physiciansin the practice of direct care of patients were involved in primary care in 2001, compared to 38.2% in 1990. The annual growth rate for the num-ber of total outpatient visits in primary care clinics has also dropped from 5.49% in 1998 to 2.32% in 1999, to -3.92% in 2000, especially after
implemen-tation of the National Health Insurance (NHI) pro-gram in 1995. The rate of outpatient visits was expected to have dropped even further in the first quarter of 2001. For monetary estimation, the annu-al growth rate for the totannu-al amount of medicannu-al claims for primary care decreased from 9.51% in 1998 to 3.89% in 1999, to -3.85% in 2000, and to -4.48% in the first quarter of 2001. As a result, implementation
Factors Related to Dissatisfaction with the National Health
Insurance among Primary Care Physicians in Taiwan
Herng-Ching Lin, PhD; Wen-Yin Chang
1, PhD; Yu-Chi Tung
2, MA
Background: Few studies were found that evaluated dissatisfaction with the National
Health Insurance (NHI) by primary care physicians in Taiwan. Therefore, the purpose of this study was to identify factors related to dissatisfaction with the NHI among primary care physicians.
Methods: A structured questionnaire was developed through a literature review, a panel discussion, and 5 focus group interviews. In total, 9336 primary care physi-cians were surveyed. A logistic regression analysis was employed to identify factors related to dissatisfaction with the NHI by primary care physicians.
Results: There were 1822 surveys returned, yielding a 19.5% response rate. They showed that 5.7% of respondents were very dissatisfied and 22.3% were dis-satisfied with the current medical environment under the NHI. The dissatis-faction of primary care physicians was significantly related to age (OR = 1.029, p < 0.05) and dissatisfaction with the following aspects: malpractice claims (OR = 1.744, p < 0.001), complexity of medical claims (OR = 1.454,
p < 0.01), excessive work hours (OR = 1.790, p < 0.001), decreased income
(OR = 2.812, p < 0.001), difficulty in finding nurses (OR = 1.379, p < 0.05), and the separation of dispensing medicine from medical practice (OR = 1.389, p < 0.05).
Conclusions: These results can provide valuable information to help policy makers
identi-fy areas for improvement and intervention in order to reduce levels of dissat-isfaction of primary care physicians under the NHI.
(Chang Gung Med J 2003;26:81-90)
Key words: dissatisfaction, primary care physicians, National Health Insurance.
From the Graduate Institute of Health Care Administration, 1Graduate Institute of Nursing, Taipei Medical University; 2Graduate
Institute of Health Care Organization Administration, National Taiwan University, Taipei. Received: May, 8, 2002; Accepted: Oct. 28, 2002
Address for reprints: Yu-Chi Tung, MA, Graduate Institute of Health Care Organization Administration, National Taiwan University. 19, Shiu-Jou Rd., Taipei 100, Taiwan, R.O.C. Tel: 882-2-2312-3456 ext. 1902; Fax: 882-2-2375-8291; E-mail: [email protected]
of the NHI has not only expedited shrinkage of pri-mary care, but has also led to reduced incomes for primary care physicians.(2,3)
Based on the US experience under managed care, physician dissatisfaction may lead to increased physician turnover and early retirement, poorer patient adherence, declining patient satisfaction, decreased continuity of care for patients, and increased costs to the medical system.(4-8) Similarly
to managed care organizations as dominant players in US health market, the Bureau of National Health Insurance, as a monopsonist, exerts its overwhelming purchasing power to limit physicians' autonomy and judgments in medical practice. Studies have also identified that physician dissatisfaction is related to excessive workloads and time pressures, limited per-sonal time, excessive paperwork, insufficient med-ical facilities, isolation due to specialization, a lack of leisure activities, low incomes, personal limita-tions in knowledge or ability, and a lack of profes-sional promotions.(7,9-13) Haas also concluded that
age, gender, income, practice in an urban setting, and work hours are related to the dissatisfaction of physi-cians.(14)
However, most of the factors fostering dissatis-faction described above are based on US experi-ences. They cannot fully account for the dissatisfac-tion of primary care physicians in Taiwan due to dif-ferences in medical and cultural practices. In addi-tion, it may be an oversimplification to consider fac-tors related to physicians' dissatisfaction without ref-erence to the possible effects of the NHI on primary care. Therefore, it is reasonable to project that dis-satisfaction among primary care physicians not only may affect the quality of patient care, but also may influence the supply of primary care physicians in Taiwan. Finding ways to overcome the dissatisfac-tion among primary care physicians has become an imperative issue for policy makers to stop the rapid shrinkage of primary care in Taiwan. However, few studies could be found related to primary care in Taiwan and dissatisfaction among primary care physicians after implementation of the NHI. Therefore, the purpose of this study was to identify factors related to dissatisfaction among primary care physicians in Taiwan under the NHI. Understanding the factors related to dissatisfaction with the NHI not only can reflect discomfort with changes and unmet expectations of primary care physicians, but also can
indicate areas for improvement and intervention in primary care.
METHODS
This national survey study was conducted using a structured questionnaire to assess factors related to dissatisfaction among primary care physicians under the NHI system.
Study population
Subjects for this study were all primary care physicians in Taiwan. Sampled physicians were those who had registered as an active primary care physician with the Department of Health in 2001. In total, 9336 subjects, including 8846 physicians in private primary care clinics, and 490 physicians in public primary care clinics, were surveyed in this study. All human rights and confidentiality were protected.
Instrument
A structured questionnaire was developed by the research team through a literature review, a panel discussion, and 5 focus group interviews. The ques-tionnaire consisted of 3 parts. The first part was comprised of overall satisfaction questions related to the NHI. Satisfaction level was measured on a 5-point Likert scale and ranged from very dissatisfied(1)
to very satisfied.(5) The second part of the
question-naire consisted of 18 items related to dissatisfaction under the NIH by primary care physicians includ-ing(1) increased number of malpractice claims,(2) the
process of purchasing medical equipment,(3) lack of
leisure time,(4) lack of time for continuing
educa-tion,(5) inadequate medical equipment or resources,(6)
complexity of medical claims processes,(7) internal
managerial problems in clinics,(8) excessive working
hours,(9) gangster blackmail,(10) decreased incomes,(11)
difficulty with patient referrals,(12)tax claims,(13)
diffi-culties in finding nurses,(14)instability of NHI
regula-tions,(15) the separation of dispensing medicine from
medical practice,(16) labor standard laws,(17) standards
for group practice, and(18)lack of supportive systems.
Respondents were asked to answer whether or not they were dissatisfied with these 18 items.
Finally, demographics such as gender, age, mar-ital status, certification of specialty, years of medical practice, and years of practice in primary care were
included. Instructions were provided at the begin-ning of the questionnaire indicating that a respondent was to indicate whether or not he/she was dissatis-fied with each item under the NHI. To test for con-tent validity, 8 experts were invited to examine ques-tions related to appropriateness, importance, and clarity of each item of the dissatisfaction question-naire. The content validity index (CVI) was used and resulted in a value of greater than 0.8. Some words or sentences were revised in accordance with the experts' suggestions.
Data collection processes and analysis
Data were collected from October 2001 to December 2001 from all eligible primary care physi-cians. Primary care physicians' names and address were obtained from the Department of Health in 2001. A stamped, self-addressed return envelope was mailed with the questionnaire to all primary care physicians.
Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS 10.0 for Windows, 1997, SPSS, Chicago, IL). All variables were analyzed using descriptive measures such as frequency, percentage, mean, and standard deviation. A logistic regression analysis was employed to identify the statistically significant fac-tors related to dissatisfaction among primary care physicians under the NHI. The independent vari-ables included the 18 above-described items as well as the demographics of the primary care physicians such as age, gender, marital status, clinic location, certification of specialty, years of experience in med-ical practice, and years of experience in primary care practice. Marital status was categorized as married, unmarried, widowed, separated, and remarried. Clinical location was divided into northern (Taipei City, Taipei County, Taoyuan County, Ilan County, and Hsinchu County), central (Miaoli County, Taichung County, Changhua County, Nantou County, and Yunlin County), southern (Chiayi County, Tainan County, Kaohsiung County, Kaohsiung City, and Pingtung County), and eastern (Hualien County and Taitung County) Taiwan. The dependent variable was determined based on whether or not a primary care physician was dissatisfied under the NHI (1 = dissatisfaction, 0 = others). Primary care physicians who answered "very dissatisfied" and "dissatisfied" were coded as 1 and those who answered "very
fied", "satisfied", and "neither dissatisfied nor satis-fied" were recorded as 0. In the case of categorically independent variables, dummy variables were creat-ed to model the effects of the different levels of a qualitative independent variable. All regression coefficients were considered significant at p < 0.05. In addition, a "goodness-of-fit test" was performed to examine whether or not there was a difference between the characteristics of participants and the total primary care physicians population.
RESULTS
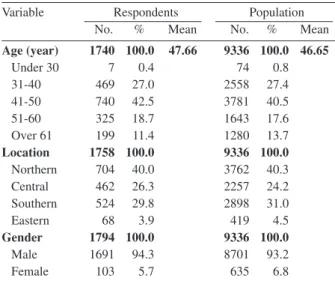
In total, 1822 questionnaires were returned after 2 telephone follow-up calls over a 3-week period which yielded a 19.5% response rate. The demo-graphic characteristics of the respondents were simi-lar to those of all physicians who registered as active primary care physicians at the Department of Health in 2001 with regard to age, gender, and clinic loca-tion (see Table 1). Respondents' age ranged from 25 to 88 years, with a mean age of 47.66 years (the mean age of the total population was 46.65 years) and a standard deviation of 10.50 years (see Table 2). Not surprisingly, males (94.3%) represented the majority of primary care physicians in Taiwan (the male percentage of the total population was 93.18%). With regard to marital status, the overwhelming majority of respondents (96.3%) were in the
"mar-Table 1. Characteristics of Respondents and Population
Variable Respondents Population
No. % Mean No. % Mean
Age (year) 1740 100.0 47.66 9336 100.0 46.65 Under 30 7 0.4 74 0.8 31-40 469 27.0 2558 27.4 41-50 740 42.5 3781 40.5 51-60 325 18.7 1643 17.6 Over 61 199 11.4 1280 13.7 Location 1758 100.0 9336 100.0 Northern 704 40.0 3762 40.3 Central 462 26.3 2257 24.2 Southern 524 29.8 2898 31.0 Eastern 68 3.9 419 4.5 Gender 1794 100.0 9336 100.0 Male 1691 94.3 8701 93.2 Female 103 5.7 635 6.8
Note: The above variables were examined by the goodness-of-fit test and showed no significant differences.
ried" category. Only 6 of 1794 respondents had remarried. As to clinic location, 40% of respondents were currently practicing in clinics located in north-ern Taiwan, 26.3% in central Taiwan, 29.8% in southern Taiwan, and only 3.9% in eastern Taiwan.
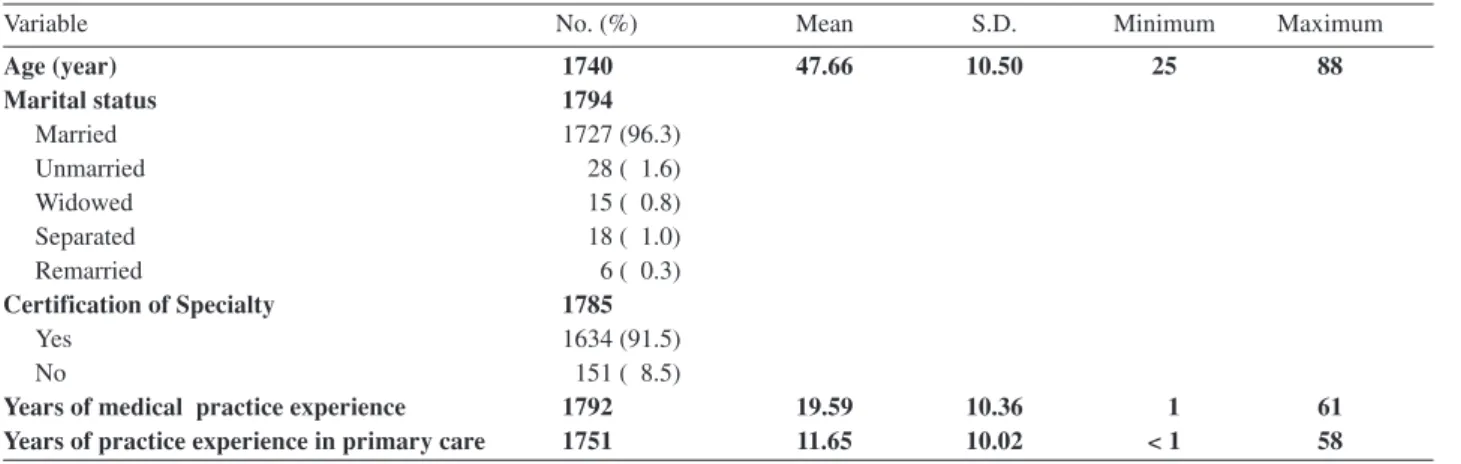
Of the sampled physicians, 91.5% had specialist certificates. The mean years of medical practice were 19.59, and the minimum and maximum years were 1 and 61, respectively. Years of practice in pri-mary care ranged between < 1 and 58, with a mean of 11.65 years and a standard deviation of 10.02 years.
Overall satisfaction level of primary care physi-cians under the NHI
Of the total sample, 5.7% (N = 101) of respon-dents were very dissatisfied with, 22.3% (N = 397) were dissatisfied with, 16.5% (N = 294) were satis-fied with, and only 1.9% (N = 32) were very satissatis-fied with the current medical environment under the NHI. In other words, 28% (N = 498) of respondents were very dissatisfied or dissatisfied with the current med-ical environment. Only 18.4% (N = 326) of respon-dents were satisfied or very satisfied with the current medical environment. The majority of respondents (53.6%) rated themselves as "neither dissatisfied nor satisfied" with the current medical environment. Items considered unsatisfactory by primary care physicians
The top 5 items which primary care physicians felt the most dissatisfied with under the NHI were decreased income (59%), instability in NHI
regula-tions (56.1%), excessive working hours (52.8%), no leisure time (46.9%), and complicated medical claims under the NHI (44.3%) (Table 3). On the other hand, the bottom 5 items which primary care physicians felt least satisfied with were purchases of medical equipment (10.7%), gangster blackmail (10.9%), internal management in clinics (13.9%), inadequate medical equipment (14.2%), and difficul-ties in transferring or referring patients (14.2%). Logistic analysis
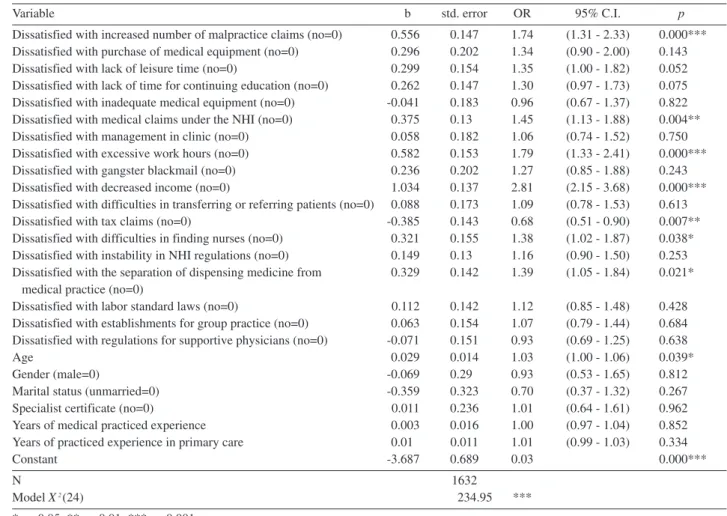
The logistic regression analysis revealed that the dissatisfaction level of primary care physicians was significantly positively related to age (OR = 1.029; 95% CI 1.002-1.058; p < 0.05) and dissatisfaction with the items of the number of malpractice claims (OR = 1.744; 95% CI 1.307-2.326; p < 0.001), med-ical claims under the NHI (OR = 1.454; 95% CI 1.128-1.876; p < 0.01), excessive work hours (OR = 1.790; 95% CI 1.327-2.413; p < 0.001), decreased incomes (OR = 2.812; 95% CI 2.150-3.679; p < 0.001), difficulties in finding nurses (OR = 1.379; 95% CI 1.019-1.867; p < 0.05), and the separation of dispensing medicine from medical practice (OR = 1.389; 95% CI 1.051-1.835; p < 0.05) (see Table 4). As a result, primary care physicians who were older and unhappy about the increased number of malpractice claims, complicated medical claims under the NHI, excessive working hours, decreased income, difficulty in finding nurses, and the separation of dispensing medicine from medical practice were more likely to be dissatisfied under the NHI.
Table 2. Demographic Information of Primary Care Physicians
Variable No. (%) Mean S.D. Minimum Maximum
Age (year) 1740 47.66 10.50 25 88 Marital status 1794 Married 1727 (96.3) Unmarried 28 ( 1.6) Widowed 15 ( 0.8) Separated 18 ( 1.0) Remarried 6 ( 0.3) Certification of Specialty 1785 Yes 1634 (91.5) No 151 ( 8.5)
Years of medical practice experience 1792 19.59 10.36 1 61
However, paradoxically, the level of dissatisfac-tion of primary care physicians was significantly negatively related to dissatisfaction with tax claims (OR = 0.681; 95% CI 0.514-0.901; p < 0.01). This result may suggest that primary care physicians who were dissatisfied with tax claims tended to be more satisfied under the NHI. Variables including gender, marital status, clinic location, years of medical prac-tice, and years of practice in primary care were not significantly related to the level of dissatisfaction of primary care physicians under the NHI.
DISCUSSION
The response rate was only 19.5% in this study even though the research team expended much effort to increase the result. The response rate was still low, but it was similar to that of Lin and Chiang's study,(15)which surveyed 7500 physicians and yielded
only a 21.6% response rate. It could be concluded that the response rate is reasonable for a national sur-vey study. However, although the respondents were similar to those of physicians who registered as active primary care physicians at the Department of Health in 2001 with regard to age, gender, and clinic location, other demographic characteristics such as
income and specialty of the respondents and popula-tion were not available in this study. Therefore, there is no means to demonstrate that the respondents were similar to the entire population regarding all demo-graphic characteristics, so the findings of this study should be used very conservatively to generalize to the entire population.
The findings indicate that age, increased mal-practice claims, increasingly complicated medical claims, excessive working hours, decreased income, tax claims, difficulties in finding nurses, and the sep-aration of dispensing medicine from medical practice were important factors identified with which primary care physicians were dissatisfied under the NHI.
The results also indicate that age is related to the dissatisfaction of primary care physicians under the current medical environment of the NHI. However, this finding was inconsistent with several previous findings concerning the relationships between physi-cians' satisfaction and age.(14,16,17) Previous studies
showed that younger physicians had a greater ten-dency to be dissatisfied. The differences may be due to the fact that those studies were conducted in the US, and there are differences in the medical culture and practice between the US and Taiwan health care systems. In addition, the target populations in those
Table 3. Dissatisfactory Items for Primary Care Physicians (N=1822)
Variables No. %
Dissatisfied with increased malpractice claims 525 29.3
Dissatisfied with purchase of medical equipment 192 10.7
Dissatisfied with lack of leisure time 840 46.9
Dissatisfied with lack of time for continuing education 562 31.4
Dissatisfied with inadequate medical equipment 254 14.2
Dissatisfied with complicated medical claims under the NHI 794 44.3
Dissatisfied with internal management in clinics 249 13.9
Dissatisfied with excessive working hours 946 52.8
Dissatisfied with gangster blackmail 195 10.9
Dissatisfied with decreased income 1058 59.0
Dissatisfied with difficulty in transferring or referring patients 254 14.2
Dissatisfied with tax claims 566 31.6
Dissatisfied with difficulties in finding nurses 337 18.8
Dissatisfied with instability in NHI regulations 1006 56.1
Dissatisfied with the separation of dispensing medicine from medical practice 440 24.6
Dissatisfied with labor standard laws 478 26.7
Dissatisfied with establishment standards for group practice 372 20.8
Dissatisfied with regulations for supportive physicians 433 24.2
preceding studies were focused on hospital-based physicians or physicians under managed care rather than primary care physicians. Therefore, findings based on the US experience might not fully explain the relationship between age and dissatisfaction of primary care physicians under the NHI in Taiwan.
A possible reason contributing to the positive relationship between age and dissatisfaction among primary care physicians in Taiwan could be the ero-sion of profesero-sional sovereignty. Most older primary care physicians experienced the "golden years" of primary care in Taiwan between 1970 and 1990.(2)
During this period of time, the medical profession was the highest-paid occupation in society and exer-cised dominant control over health markets and med-ical organizations. Moreover, the profession turned its authority into social privilege, economic power,
and political influence. The medical profession thus had an influential claim to authority. However, after implementation of the NHI system in 1995, most physicians were paid by whatever services they pro-vided under the BNHI instead of by traditional out-of-pocket payments from patients. The physicians' authority in medicine has been threatened and chal-lenged by the BNHI, which now controls the amount and rate of remuneration for physicians and the allo-cation of medical resources. Colby in 1997 stated that the loss of autonomy to corporations owned by others was probably the greatest fear of physicians.(18)
Stoddard and his colleagues in 2001 also indicated that professional autonomy was a strong independent predictor of physician satisfaction.(19) Loss of control
over clinical and related matters is reflected in physi-cians' dissatisfaction with the current health
environ-Table 4. Relationships between Satisfaction and Factors among Primary Care Physicians
Variable b std. error OR 95% C.I. p
Dissatisfied with increased number of malpractice claims (no=0) 0.556 0.147 1.74 (1.31 - 2.33) 0.000*** Dissatisfied with purchase of medical equipment (no=0) 0.296 0.202 1.34 (0.90 - 2.00) 0.143 Dissatisfied with lack of leisure time (no=0) 0.299 0.154 1.35 (1.00 - 1.82) 0.052 Dissatisfied with lack of time for continuing education (no=0) 0.262 0.147 1.30 (0.97 - 1.73) 0.075 Dissatisfied with inadequate medical equipment (no=0) -0.041 0.183 0.96 (0.67 - 1.37) 0.822 Dissatisfied with medical claims under the NHI (no=0) 0.375 0.133 1.45 (1.13 - 1.88) 0.004** Dissatisfied with management in clinic (no=0) 0.058 0.182 1.06 (0.74 - 1.52) 0.750 Dissatisfied with excessive work hours (no=0) 0.582 0.153 1.79 (1.33 - 2.41) 0.000*** Dissatisfied with gangster blackmail (no=0) 0.236 0.202 1.27 (0.85 - 1.88) 0.243 Dissatisfied with decreased income (no=0) 1.034 0.137 2.81 (2.15 - 3.68) 0.000*** Dissatisfied with difficulties in transferring or referring patients (no=0) 0.088 0.173 1.09 (0.78 - 1.53) 0.613 Dissatisfied with tax claims (no=0) -0.385 0.143 0.68 (0.51 - 0.90) 0.007** Dissatisfied with difficulties in finding nurses (no=0) 0.321 0.155 1.38 (1.02 - 1.87) 0.038* Dissatisfied with instability in NHI regulations (no=0) 0.149 0.133 1.16 (0.90 - 1.50) 0.253 Dissatisfied with the separation of dispensing medicine from 0.329 0.142 1.39 (1.05 - 1.84) 0.021*
medical practice (no=0)
Dissatisfied with labor standard laws (no=0) 0.112 0.142 1.12 (0.85 - 1.48) 0.428 Dissatisfied with establishments for group practice (no=0) 0.063 0.154 1.07 (0.79 - 1.44) 0.684 Dissatisfied with regulations for supportive physicians (no=0) -0.071 0.151 0.93 (0.69 - 1.25) 0.638
Age 0.029 0.014 1.03 (1.00 - 1.06) 0.039*
Gender (male=0) -0.069 0.293 0.93 (0.53 - 1.65) 0.812
Marital status (unmarried=0) -0.359 0.323 0.70 (0.37 - 1.32) 0.267 Specialist certificate (no=0) 0.011 0.236 1.01 (0.64 - 1.61) 0.962 Years of medical practiced experience 0.003 0.016 1.00 (0.97 - 1.04) 0.852 Years of practiced experience in primary care 0.010 0.011 1.01 (0.99 - 1.03) 0.334
Constant -3.687 0.689 0.03 0.000***
N 1632
Model X2(24) 234.95 ***
ment under the NHI.
Traditionally, primary care physicians would stay in their own clinics as long as possible to avoid losing any potential patients. Lin in 1999 concluded that the average primary care physician in Taiwan works 9.36 hours per day and 6.20 days per week.(2)
The long working hours led to a shortage of time for primary care physicians to attend continuing educa-tion programs. Moreover, according to a study by Mawardi, physicians may be dissatisfied with their limited medical knowledge or abilities,(11) since the
pace of growth in medical technology was faster than expected during the past 2 decades. Thus, primary care physicians in Taiwan have to absorb updated medical knowledge to stay competitive with hospi-tal-based physicians in the healthcare market. In par-ticular, the increasingly complicated procedures of medical claims under the NHI require physicians to receive continuing education so they can remain competent. However, the lack of time for continuing education was not significantly related to the level of dissatisfaction under the NHI in this study. Further investigation is needed in the future to understand the relationship between continuing education and dissatisfaction.
In this study, as many as 46.9% of respondents expressed dissatisfaction with their lack of leisure time. However, no statistically significant relation-ship was found between dissatisfaction of primary care physicians and dissatisfaction with the lack of leisure time in this study. This is inconsistent with the conclusion by Lee and Chou in 1991 who found that the lack of leisure time was an important factor related to the dissatisfaction of primary care physi-cians.(12)
Not surprisingly, this study revealed that dissat-isfaction with decreased income was one of the most important factors predicting dissatisfaction among primary care physicians under the NHI. We found that 59% of respondents were dissatisfied with their decreased income. This finding is supported by 2 related studies.(12,16) The decreased income can be
partly attributed to a reduction in the number of total outpatient visits for primary care clinics. For exam-ple, the growth rate in the number of total outpatient visits for primary care clinics was -3.91% in 2000, in contrast to a 4.16% gain for medical centers and a 2.84% gain for regional hospitals. Similarly, the growth rate of the total monetary amount of medical
claims for primary care clinics was -3.94% in 2000, in contrast to a 5.82% gain for medical centers and a 2.53% gain for regional hospitals. Both of these con-tributed to the drop in physicians' incomes.
This study also found that dissatisfaction with increased medical malpractice claims was related to dissatisfaction among primary care physicians under the NHI. According to data released by the Department of Health, Taiwan, in 2000, the number of malpractice lawsuits increased 58.5% after the inception of the NHI in 1995. A possible explana-tion for the increase in the number of malpractice lawsuits is that people have progressively recognized the importance of protecting their own rights when facing an imbalanced relationship in medical knowl-edge with physicians. As a result of the widespread use of Web sites to search for medical knowledge, public trust in physicians has decreased accompanied by an increase in the number of malpractice lawsuits. Some other studies have also documented that mal-practice lawsuits were related to physician dissatis-faction.(11,20)
Aside from the decreased trust in physicians, another possible explanation for the increase in the number of malpractice lawsuits is that primary care physicians do not practice much defensive medicine since the BNHI does not reimburse for that. Shi and Singh defined defensive medicine as excessive med-ical tests and procedures performed as a protection against malpractice lawsuits.(21) Further research is
needed to explore the effects of increased medical malpractice claims on changes in physician behavior and incomes in Taiwan.
Physician dissatisfaction with the complicated procedures for medical claims under the NHI also had a statistically significant relationship with dissat-isfaction among primary care physicians; 44.3% of respondents were dissatisfied with medical claims in the study. This reflects physician dissatisfaction with the increased administrative burden and unstable reg-ulations under the NHI. One recent study of Stoddard and his colleagues in 2001 also indicated that physicians consider external regulations and paperwork as problems in medical practice.(19)
Exploring the factors related to dissatisfaction of primary care physicians not only can help policy makers understand differences between reality and expectations, but can also identify areas for improve-ment and intervention. In particular, almost 1/3 of
primary care physicians were reportedly dissatisfied with the current medical environment under the NHI. Primary care physician dissatisfaction may lead to increased physician turnover and early retirement which will contribute to the continued shrinkage of primary care. Therefore, in order to stop the contin-ued erosion of primary care services, the Department of Health or the BNHI should encourage primary care physicians to join a group practice, which is characterized as the provision of health care services by 2 or more physicians who are formally organized as a legal entity. Particularly, primary care physi-cians have long working hours and are overloaded with paperwork in a solo practice. A group practice setting can provide primary care physicians with more leisure time, greater access to capital, more regular working hours, more time for continuing education, and more opportunities to employ a full-time person to deal with medical claims under the NHI compared to solo primary care practitioners. Moreover, further research is needed to include the possible effects of the implementation of a policy for a reasonable number of outpatients and a global bud-get system on dissatisfaction among primary care physicians.
Limitations
Because the data were obtained from a self-reporting survey by primary care physicians through-out Taiwan, some data may have been over- or under-reported. The extent of over-reporting and under-reporting was difficult to estimate, but could have resulted in overestimation or underestimation of the level of satisfaction of primary care physicians under the NHI. Additionally, as this study may be the first national survey study concerning dissatisfac-tion among primary care physicians under the NHI, comparison with other studies is not possible. Therefore, further study is needed to understand whether or not these primary care physicians' reports are valid.
Since this study was a cross-sectional national survey, it is difficult to understand the relationship between causes and effects of the dissatisfaction of primary care physicians. Therefore, a longitudinal study is also needed to clarify this relationship in the future. Additionally, the low response rate may be a natural limitation of a national survey study; thus, the findings of this study should be used very
conser-vatively to generalize to the entire population.
REFERENCES
1. Shi CY. How to raise the quality and competition power for the primary care. Chin Prim Care News 2001;9:1. 2. Cheng JY. Where is primary care going? Taiwan Med J
2001;4:48-50.
3. Lin YY. The impact of National Health Insurance on physician productivity and income. Hospital 1999;32:1-14. (in Chinese)
4. Burda D. Many docs mull early retirement- survey. Mod Healthc 1994;24:38.
5. DiMatteo MR, Sherbourne CD, Hays RD, Ordway L, Kravitz RL, McGlynn EA, Kaplan S, Rogers WH. Physicians' characteristics influence patients' adherence to medical treatment: results from the Medical Outcomes Study. Health Psychol 1993;12:93-102.
6. Linn LS, Brook RH, Clark VA, Davies AR, Fink A, Kosecoff J. Physician and patient satisfaction as factors related to the organization of internal medicine group practices. Med Care 1985;23:1171-8.
7. Lichtenstein RL. The job satisfaction and retention of physicians in organized settings: a literature review. Med Care Rev 1984;41:139-79.
8. Mick SS, Sussman S, Anderson-Selling L, DelNero C, Glazer R, Hirsch E, Rowe DS. Physician turnover in eight New England prepaid group practices: an analysis. Med Care 1983;21:323-37.
9. Murray A, Montgomery JE, Chang H, Rogers WH, Inui T, Safran DG. Doctor discontent. A comparison of physi-cian satisfaction in different delivery system settings, 1986 and 1997. J Gen Intern Med 2001;16:452-9. 10. Linn LS, Yager J, Cope D, Leake B. Health status, job
sat-isfaction, job stress, and life satisfaction among academic and clinical faculty. JAMA 1985;254:2775-82.
11. Mawardi BH. Satisfactions, dissatisfactions, and causes of stress in medical practice. JAMA 1979;241:1483-6. 12. Lee MC, Chou MC. Job and life satisfaction among
remote physicians in Taiwan. J Formos Med Assoc 1991; 90:681-7.
13. Epstein RM. Time, autonomy, and satisfaction. J Gen Intern Med 2000;15:517-8.
14. Haas JS. Physician discontent: a barometer of change and need for intervention. J Gen Intern Med 2001;16:496-7. 15. Lin YY, Chiang TL. An opinion survey of physicians on
national health insurance. J Natl Public Health Assoc 1992;11:220-7.
16. Kravitz RL, Linn LS, Shapiro MF. Physician satisfaction under the Ontario Health Insurance Plan. Med Care 1990;28:502-12.
17. Haas JS, Cleary PD, Puopolo AL, Burstin HR, Cook EF, Brennan TA. Differences in the professional satisfaction of general internists in academically affiliated practices in the greater-Boston area. Ambulatory Medicine Quality
Improvement Project Investigators. J Gen Intern Med 1998;13:127-30.
18. Colby DC. Doctors and their discontents. Health Aff (Millwood) 1997;16:112-4.
19. Stoddard JJ, Hargraves JL, Reed M, Vratil A. Managed care, professional autonomy, and income: effects on physician career satisfaction. J Gen Intern Med 2001;
16:675-84.
20. Skolnik NS, Smith DR, Diamond J. Professional satisfac-tion and dissatisfacsatisfac-tion of family physicians. J Fam Pract 1993;37:257-63.
21. Shi L, Singh DA. Delivering health care in America. Gaithersburg, MD: An Aspen Publication, 1998:554.
1 2
9336
1822 19.5% 5.7% 22.3%
(OR = 1.029, p < 0.05) (OR = 1.744, p < 0.001) (OR = 1.454,
p < 0.01) (OR = 1.790, p < 0.001) (OR = 2.812, p < 0.001) (OR = 1.379, p < 0.05) (OR = 1.389, p < 0.05) (ܜطᗁᄫ 2003;26:81-90) έΔᗁጯ̂ጯ ᗁચგநጯࡁտٙĂ1᜕நࡁտٙć2઼ϲέ៉̂ጯ ᗁᒚ፟ၹგநࡁտٙ צ͛͟ഇĈϔ઼91ѐ5͡8͟ćତצΏྶĈϔ઼91ѐ10͡28͟Ą ৶פ٩ОώĈ⟳൝̈ؓĂ઼ϲέ៉̂ጯ ᗁᒚ፟ၹგநࡁտٙĄέΔξषэྮ19ཱིĄTel.: (02)23123456ᖼ1092; Fax: (02)23758291; E-mail: [email protected]