Virtual Reality for Post-Stroke Shoulder-Arm Motor Rehabilitation:
Training System & Assessment Method
Shih-Ching Yeh
1, Si-Huei Lee
2, Jia-Chi Wang
2, Shuya Chen
3, Yu-Tsung Chen
1, Yi-Yung Yang
2Huang-Ren Chen
,
1, Yen-Po Hung
11
Department of Computer Science and Information Engineering National Central University
2 Taipei Veterans General Hospital
3 Department of Physical Therapy, China Medical University
ABSTRACT
Stroke is one of the major diseases around the world. The brain injury caused by stroke will derive sustaining neurological disorder of different forms, which in turn will lead to all kinds of limb and body exercise hindrance and will cause significant challenge to the life of the patient, that is, the quality of life of the patient is going to be strictly affected. Along with the development and popularity of technology, scholars in the medical care and rehabilitation fields are trying to integrate all kinds of new technologies to perform the development of new rehabilitation training system.
This research aims at rehabilitation items of upper limbs, which include the reciprocating stretching of upper limb, reaching of the upper arm, bi-lateral coordination and balance of the body. In association with interactive technology, game technology, sensor technology and stereo image technology, virtual reality physical-based training task is developed, and initial pilot test is done on patient with stroke, meanwhile, multi-dimensional experimental results are acquired, which include clinical test assessment, task performance, historical data of exercise track and psychological emotional data. The research objectives are to verify the functionality of the system, to verify the effectiveness of the system on rehabilitation, to develop new assessment method and to investigate topics related to human machine interaction. The experimental results have verified the functionality of this rehabilitation training task in all aspects. Through the exercise analysis of the historical data of exercise track and the statistical analysis of task performance of the past therapy sessions, this system can acquire successfully reliable and valuable information to be used for future verification of medical therapeutic effectiveness and the development of new type of clinical assessment method. In the mean time, according to the measured psychological emotional data as perceived subjectively, this system indeed can urge the patient to engage continuously rehabilitation therapeutic session that is based on this training system and enjoy it, besides, the authors are very confident on the possibly generated rehabilitation effect of these two training tasks.
I. INTRODUCTION
Neurological exercise disorder originates the injury on the cortex exercise area of the brain, however, the cortex of the brain of human beings and the related nervous system are always in the plasticity state [6] and nervous re-organization processes [14], which in turn will affect and accelerate the learning (recovery) processes of the exercise function, and related researches also prove that systematic and group exercise rehabilitation model can indeed assist the enhancement of rehabilitation therapy, however, for the rehabilitation therapeutic session based on the guiding learning from rehabilitation therapist, under economic and cost consideration, systematic and group exercise rehabilitation model is so difficult to be implemented; in addition, some researches also pointed out that for the learning of a new exercise technical model, the providing of the behavioral performance of the user to be used as expanded feedback mechanism is one of the important rings in the learning principles of enhancing the learning effectiveness. Similarly, exercise rehabilitation of brain injury can be seen as one type of exercise learning process, and the above principle can also be used to provide continuously the patient with rehabilitation performance as feedback [6][14], in another view, the feedback of vision and hearing is also one of the important factors to keep the exercise function [11].
The constant advancement of 3D animation technology and internet technology not only provides technological enhancement, but also provides economic popularization, hence, lots of scholars performing medical rehabilitation related researches and the front line doctor or therapist in the world have tried to integrate the above technologies, and they try to use virtual reality, Augmented Reality and mixed virtual reality e as the theoretical basis, meanwhile, User Centered design concept is also put in, furthermore, user’s perception on the system and usability and immersion of the system are also considered, and finally, the interactive model and strategy provided by the human machine interface are also used to perform the development of all kinds of new rehabilitation therapeutic sessions and rehabilitation technologies.
In addition, in order to assess the current status of the patient effectively so that medical personnel and the physical therapist can seize the current status of the patient more
accurately and set up the rehabilitation goal. Moreover, in order to let the medical personnel be able to perform personalized therapeutic session design and provide the fittest rehabilitation therapeutic schedule and related rehabilitation strength design and to achieve the rehabilitation goal, effective physiological assessment tool is very important. Currently, there are lots of assessment tools designed for different parts of the bodies, for different functions and for different objectives, which include physical assessment and self assessment. Clinically, the frequently used physical assessment tools include Fugl-Meyer Assessment table, Wolf Motor Function. Test (WMFT) and TEMPA (Upper Extremity Performance Evaluation Test for The Elderly), and they will perform respective assessment on the exercise function of the upper extremity, the usage capability of the wrist and palm and whether daily actions can be finished smoothly or not. In self assessment aspect, EXCITE MAL Score Sheet, CONFIDENCE IN ARM AND HAND MOVEMENTS (CAHM) and Stroke Impact Scale (SIS)[5][7][8][9][10] are frequently adopted to make self assessment on the usage injured part of the patient for confidence index and the actions needed for daily life after the carry-out of rehabilitation training, and the assessment includes whether the action needed for the life can be finished or not, the confidence index and the cause the action cannot be finished.
During the rehabilitation process, in addition to the physiological state of the patient, the emotional factor of the patient is also very important. For the psychological emotional behavioral model of stroke patient, researchers including Maclean[2][3], Colombo[12] and Paolucci[13], have made studies regarding the correlation between the motive factor of stroke patient and rehabilitation effectiveness, hence, and the patient’s acceptance on new technology includes:
Factors such as whether the system is easy to be operated, whether the patient thinks this system is helpful or not, the level of pleasure provided by the system, whether strong focus is put on the system during the experimental process and whether it is easy to adapt to the environment set up by the system might all affect the patient’s participation and the willingness and motive in the rehabilitation therapeutic session.
In this research, for the rehabilitation items of upper extremity, for example, reciprocating stretching of the upper arm, reaching of the upper arm, bi-lateral coordination and the balance of the body, virtual reality physical-based training task is going to be developed in association with interactive technology, gaming technology, sensor technology and stereo imaging technology. In the mean time, this research is going to perform clinical experiment, to recruit right handed patient with Fugl-Meyer Assessment score reaching the range of 40 to 50 to carry out a series of gaming type rehabilitation training therapeutic sessions that are based on virtual reality in association with physical-based equipment. There are a total of 12 therapeutic sessions, and each session lasts for two hours, and before and after the training, functional assessments will be performed, which include physical assessment and self assessment. In the
training process, the exercise track and task performance of the patient is going to be completely measured and recorded, then after the finishing of the training, patient’s technological acceptance on the new rehabilitation system is going to be measured. Based on the above measurement result, exercise analysis and statistical analysis will be performed so as to verify the functionality of the system, to verify the system’s effectiveness on rehabilitation, to develop new assessment methods, and to investigate the topics related to human machine interactions.
II. LITERATURE SURVEY
In recent years, lots of research teams applied virtual reality in the rehabilitation of medical care [4], and after long term and repeated experiments, this technology has been proved to be effective in the rehabilitation training of the stroke patient. Virtual reality can display the realized training action in gaming way in the virtual environment, and in the gaming process, all kinds of rehabilitation actions can be implemented. Since all the objects interacted with the user are all virtual objects, not only the usage timing with the object can be controlled, the mutual accuracy with the user can be controlled, the feedback for achieving the task can be displayed, but also the safety of the rehabilitation training environment can be ensured. Moreover, real time gaming feedback let the user confirm his own rehabilitation progress, and it can also display the successful reaching of the goal and recognize the user’s self capability and enhance the user’s confidence. The application of virtual reality not only can let the user learn all kinds of learning skills, but also can train the recognition functions of the patients.
In this research, virtual reality with gaming characteristic is used as a rehabilitation tool for the tracking of the full body. In the past, the team of scholar Ksenia [1] has designed a set of system using optical capturing to acquire body action. When this system is used, it is needed to paste optical cursor ball at all the joints of the body, then six action capturing camera equipment are used to position all the optical cursors so as to get the absolute positions of all the joints of the user in the space and to provide these information to the user of the virtual reality game, eventually, body action can be used to achieve the interaction that uses body action to control the gaming object. The task of the game is to use the stretching of both hands to catch the bubble spit out by the octopus in the virtual world, in this case, the vertical and horizontal angles of the bubbles spit out can be designed, and the maximal action scope can also be controlled too.
This experiment has certain achievement in rehabilitation training, however, the needed equipment and the usage environment setup is not that easy for general medical care personnel, meanwhile, in each game training, it is needed to put on lots of optical cursors on the body of the patient for positioning, in the entire rehabilitation process, it will for sure consume massive time, in addition, the patient might be unable to wear positioning equipment due to body factor, or the medical care personnel without information engineering background might not meet the system requirement during the wearing process, and all the above cases might lead to
incorrect game result or even the failure of the task. Therefore, we hope to use simple equipment and operation environment to achieve better training effect, not only it is easy to use, but also it makes the rehabilitation process smoother and more efficient, besides, this can save the money for purchasing massive equipment and the subsequent maintenance fee too.
III. RESEARCH METHOD:SYSTEM DESIGN
In this experiment, we have referred to all kinds of traditional rehabilitation items of upper extremity. Here the rehabilitation items for upper extremity include the reciprocating stretching of the upper arm, the reaching of the upper arm and bi-lateral coordination, and three different training tasks are designed respectively for them. Moreover, the training content is performed with task simulation and design using the game engine Unity so as to urge the patient to implement the setup target action to complete the task; furthermore, virtual reality is constructed using the product 3D-Vision of Nvidia corporation, and the advantages are that this product is supported by the current mainstream stereo display and stereo projector display equipment, besides, 3D-Vision has price lower than other product and is easier to get, meanwhile, the equipment only needs USB to be connected to PC, then through simple setup, it can be applicable to any software supported by Nvidia corporation. However, physical-based device uses Kinect of Microsoft. Kinect is different than traditional physical-based equipment, there is no need to carry any sensor on the body, and the player only needs to face Kinect lens, and the chip inside it will then calculate the joint information of the skeleton of each player. In the followings, three training tasks will be introduced respectively:
A. Shoulder and elbow exercise:upper arm diagonal reciprocating stretching
The task design is a simulation of a ”Glass wiping” task, and the rehabilitation patient is going to face a virtual window, and different location of the virtual window is distributed with fog of different density, the rehabilitation patient will hold an interactive brush, and the fog on different location of the window with different fog density will, through the shoulder and elbow exercise in upper and lower movement way along the diagonal, be removed. The level of removal will be dependent on the count of
reciprocating wiping and the level of pressure application of the user; besides, sufficient pressure is applied onto the interactive brush so as to finish the assigned ”glass wiping” task. The entire system is as shown in figure 1.
Figure 1 Upper arm reciprocating stretching training system
The operation way of the game is that the user will hold the virtual wiper composed of SUNSPOT and pressure sensor and will wipe it on the wall, during the wiping process, the pressure sensor will acquire the current applied force and convert it into digital unit, then through the receiving by SUNSPOT, it will be transmitted in wireless way to the sensor on the computer end, and the game software will then, in the VRPN form, receive the pressure value and convert it into the wiping force in the virtual environment. While the pressure is received, Kinect will be used additionally to detect the body location so as to get the absolute coordinate of the hand within the projection range of the screen to position the location of the wiper in the game space. With the wiper location and pressure size, through the collision detection action in the virtual space from the wiper on the stain and through the use of algorithm to decide if the stain is removed or not, by doing so, we can then simulate the stain wiping action.
B. Shoulder elbow exercise: upper arm reaching
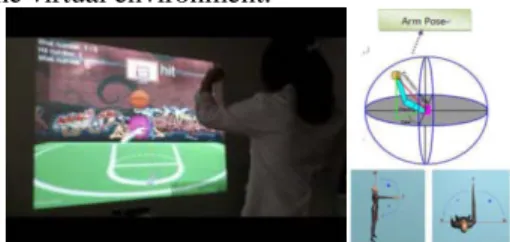
The task is designed as simulating ”To move the basket ball to a fixed position and have it thrown out automatically”, and the rehabilitation patient uses the reaching exercise of upper arm to control the basket ball in the environment, then through different upper arm reaching gesture, ball shooting target will appear at different location and different height in the three dimensional space. The entire system is as shown in figure 2.
The adjustable difficulty design is to urge the rehabilitation patient to use different upper arm gesture to complete the task of basketball shooting, and the location and height of the ball shooting target point will be decided by the upper arm gesture expected by rehabilitation target, and the upper arm gesture is defined by upper arm extension length, pitch and yaw that is based on the shoulder as the origin. Meanwhile, the registration between upper arm gesture and location in the real environment and the target object in the virtual environment.
Figure 2 Upper arm reaching training system
C. Shoulder elbow exercise: upper arm bi-lateral coordination exercise
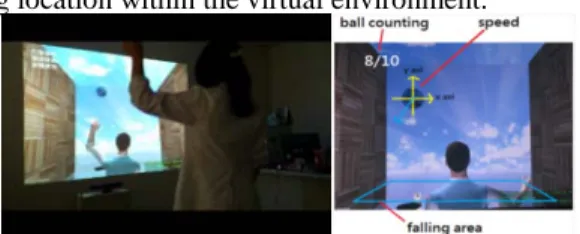
The task is designed as simulating ”shoot and catch the ball using both hands”. Rehabilitation patient uses the reaching exercise of the upper arm of both hands to control both hands of the figure in the virtual environment, and the patient needs to use both eyes to predict the dropping locus of the ball, then different upper arm reaching gesture should be used to shoot and catch the virtual ball in the game. The entire system is as in figure 3.
Adjustable difficulty level design urges the rehabilitation patient use different kinds of upper arm gestures to finish
ball shooting and catching task, and the location of the ball dropping range will be decided by the upper arm gesture expected by rehabilitation target. Moreover, the upper arm gesture is defined by upper arm extension length based on the shoulder as the origin, and the ball dropping speed is defined by the reaction time of hand and eye. Meanwhile, it is necessary to perform the registration between upper arm gesture and location of real environment and the ball dropping location within the virtual environment.
Figure 3 Upper arm bi-lateral coordination training system
IV. RESEARCH METHOD:DESIGN OF EXPERIMENT
A. The received case and case receiving standard
The received case contains nine members, namely, three stroke patients in acute, sub-acute and chronic case respectively. The functions of the upper extremity of the patients all reach Fugl-Meyer Assessment with score in the range from 40 to 50, and all the patients are right handed.
The selection standard is the unilateral brain stroke patient of the first onset of the disease, and the period between stroke onset time and the participation time should not be more than one year, and the age is in the range from 20 to 85 years old. Meanwhile, the near end action functions of the upper extremity of the disease side should all be above the fourth term (included) of Brunnstrom’s stage) and the patient should have exercise disorder of the upper extremity. Moreover, the patient should have no significant recognition function loss to follow simple command, to understand experimental objective and to act in accordance with research procedure and is willing to sign the agreement for person under test.
Each patient will be recorded with his age, gender, left handed or right handed, existed diseases (including hypertension, diabetes, hyperlipemia, arrhythmi, epilepsy), the location of the brain injury, stroke type (infarct type or hemorrhagic type), date of stroke onset, number of months of rehabilitation, and the score of Barthel’s Index. A professional assessment person will be responsible for the assessment of the above data and scale.
B. Experimental process
This experiment is going to be designed in reversal replication design. In the beginning of the experiment, the person under test will be explained with experimental process and its objective, then the person under test will be asked to sign the agreement. In addition, we have to remind the person under test not to attend any other rehabilitation training activities during the test period.
The entire experiment lasts for 31 days. The first eight days will be the situation assessment of the patient, and the
physiological and psychological state of the person under test before the experiment will be recorded. The medical personnel can, based on the assessment situation of the patient, make all kinds of rehabilitation training difficulties. During the test period, two major assessments and four simple assessments will be done. After eighth day, rehabilitation training lasting for 15 days will be carried out, and the therapy frequency for the patient will be three times a week. Select a game with difficulty meeting the capability of the patient, then collect the data for one hour of rehabilitation training, then record the game played, the performance, the gaming time and make sure there is no error in the game output for the person under test. The interval between therapy should be more than 24 hours to avoid the generation of fatigue on the patient. After the completion of the therapy, simple assessment will be performed for a total of eight times, at the last time of rehabilitation training, a major assessment will be performed so as to record the effectiveness after the patient has received the rehabilitation training. In the last eight days, no rehabilitation training will be carried out, instead, four simple assessments and one last assessment will be performed to observe if in this rehabilitation way, the patient can, without carry-out of any training, keep the level previously achieved just right before the ending of a series of rehabilitation training.
C. Data analysis and performance assessment method
The data type and format acquired in this research includes clinical assessment tool data, task performance data, exercise raw data and the psychological emotional data of subjective perception.
Clinical assessment tools include physical assessment and self assessment. We have used the following physical assessments: FM(first assessment), WMFT, TEMPA (four major assessment), and self assessment: MAL, CAHM, SIS(second and third major assessment). Moreover, the difference between pre-test and post-test will be used to assess rehabilitation effectiveness.
Game task performance includes task success rate, task completion time, response time and task score. Furthermore, statistical analysis will be performed to assess the improvement trend of the exercise performance.
The exercise raw data is the exercise locus information, and further exercise analysis will be performed to calculate different exercise indexes, which include stability, discontinuity, efficiency, oscillation and level of loading. Furthermore, the difference between the pre-test and post-test is going to be used to assess the rehabilitation effectiveness, in the mean time, statistical analysis will be performed to assess the trend of exercise function improvement.
The psychological emotional data of subjective perception is technological acceptance survey questionnaire, which will be used to do survey on user for the followings: awareness on the game content, presentences of virtual reality, usefulness of the training task, playfulness of the training task, intension to use of the training task and ease of use of the training task, the main objective is to obtain the
assessment on this system from the person under test, and it is hoped that the result can be used as better system reference in the future design. In the mean time, related analysis will be done with the above mentioned data to investigate the correlation between psychological emotional factor and rehabilitation effectiveness.
V. CASESTUDY
In the experiment, nine patients are expected to be recruited to participate in the experiment. Currently, one person under test has been recruited, with data as: age 82 years old, female who is a patient of Ischemic Stroke, and the score obtained from FM assessment is 27, TEMPA and WMFT performances are all middle and low. According to the above mentioned experimental process flow, we have finished Pilot Test, in the following, we are going to show all the experimental results of the person under test.
A. Exercise analysis
According to the measured historical data of multi-node exercise locus of multi-node of the skeleton of the patient and in association with the spatial data of target object in the virtual environment, we can perform exercise analysis to further understand and investigate the exercise model and behavioral strategy for a patient to complete the task.
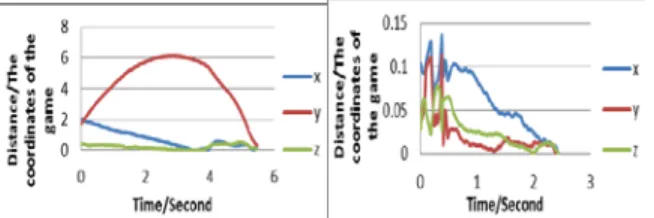
For the training task of dual hand ball shooting and catching of upper arm bilateral coordination, the task target is to use hand to touch the moving target object (the ball), then subtract, at each time point, the hand spatial location by the target object spatial location, we can then obtain the relative location between both of them, then use Cartesian coordinate as basis, we can cut it into three partials (x, y, z) for representations, and the unit is always the coordinate defined by the game engine, and the user is used as the center, wherein x the difference in the left and right direction between the hand and the target object, y represents the difference in the up and down direction between hand and target object, z represents the difference in the front and rear direction between hand and target, when the hand touches the target object successfully, x, y, z values will all be zero. When the x, y, z values in each time point in the task process is plotted as time-history diagram, it means the approaching time-history diagram between hand and target object, which is as shown in figure 4, and in the figure, the behavioral model of hand movement of the patient in three directions of Cartesian coordinate during the task completion process can be clearly seen, and the behavioral strategy can then be investigated. For the basket shooting task of upper arm reaching, we can also follow the above mentioned concept to draw the approaching time-history diagram between hand and target object, which is as shown in figure 5. For the black board wiping training task of regarding upper arm diagonal reciprocating stretching, the task target is to correspond the hand moving range to the planar coordinate (x, y) in the virtual space so as to get the location of the virtual wiper, then the pressure detected by the sensor is recorded, and the moving locus and applied force of the wiper can then be recorded, then the hand moving range
distribution and maximal applied force diagram in a task can then be drawn, which is as shown in figure 6.
Figure 4(left) Approaching time-history diagram of hand and target object (dual-hand ball catching)
Figure 5(right) Approaching time-history diagram of hand and target object (basket shooting)
Figure 6 The maximal pressure distribution of wiper in the game world.
B. Task performance
According to the measured patient’s task performance and the count of training therapeutic session, we can perform statistical analysis on the time axis to assess the level of improvement and development trend of the task
performance. The task performances of three training tasks in different therapeutic sessions are as show in figure 7 and figure 8.
Figure 7(left) Task performance: Training task of ball shooting and catching of both hands of bilateral coordination
of upper arm
Figure 8(right) Task performance: Training task of basketball shooting of upper arm reaching
C. Psychological emotional data of subjective perception
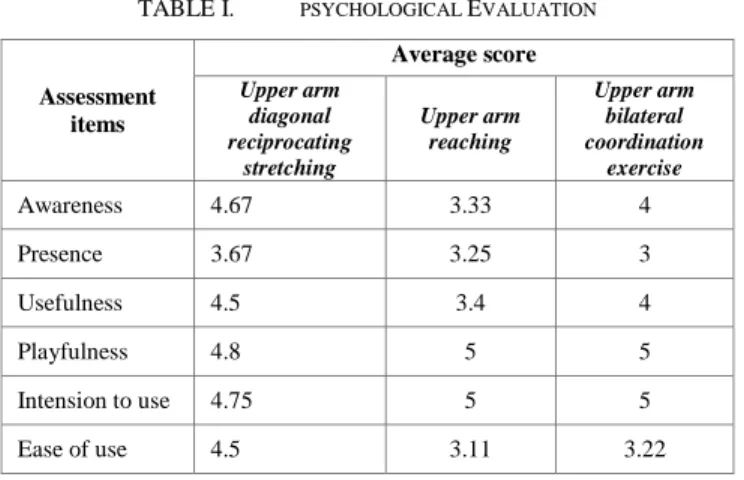
The measurement result of psychological emotional data of subjective perception is as shown in table 1. The result shows that for all the training tasks, in two items of playfulness and intention to use, full score of five are obtained. It shows that this system indeed can urge the patient to get involved in rehabilitation therapeutic session that is based on this system and enjoy them; upper arm diagonal reciprocating stretching training task and upper arm bilateral coordination exercise training task all lead to score of four in terms of awareness and usefulness, which shows
that these two training tasks can provide the patients with sufficient information to see all the state information and related clues while the task is going on. In the mean time, the patients are also very confident on the rehabilitation effects possibly generated by these two training tasks. In all the training tasks, upper arm diagonal reciprocating stretching training task shows the highest score in the item of ease of use, and the possible cause might be because the patient hold a real wireless interactive wiper, which is more intuitive. For all the training tasks, the score obtained in presence items are in the range of 3 to 4, and even if the system has provided stereo vision and physical-based interaction, seems like the user’s perception is not reflected, and the possible reason might be because that the person under test is of higher age, which makes them have less sensitive perception on the virtual technology.
TABLE I. PSYCHOLOGICAL EVALUATION
Assessment items Average score Upper arm diagonal reciprocating stretching Upper arm reaching Upper arm bilateral coordination exercise Awareness 4.67 3.33 4 Presence 3.67 3.25 3 Usefulness 4.5 3.4 4 Playfulness 4.8 5 5 Intension to use 4.75 5 5 Ease of use 4.5 3.11 3.22 VI. CONCLUSIONS
In this study, for the rehabilitation items of upper extremity (namely, upper arm reciprocating stretching, upper arm reaching, bi-lateral coordination and body balance), some technologies are successfully associated (for example, interactive technology, gaming technology, sensor technology and stereo imaging technology), to develop virtual reality physical-based training tasks. In the mean time, this research has designed rehabilitation therapeutic session for right handed patient with Fugl-Meyer Assessment score in the range 40 to 50, and pilot test has been successfully completed. The experimental result has proved the functionality of this set of rehabilitation training task in all aspects. Through the exercise analysis of the historical data of exercise locus and the statistical analysis of the task performance of the past therapeutic sessions, this system can successfully acquire reliable and valuable information to be used in the future for verifying medical care effectiveness and for developing new clinical assessment method. In the mean time, according to the measured psychological emotional data of subjective perception, it can be seen that this system can indeed urge the patient to continue getting involved in rehabilitation therapeutic session based on this training system and enjoy it. Meanwhile, it makes the patient
more confident on the rehabilitation effect possibly generated by these two training tasks.
In the future, the pilot test of this research is going to be used as the basis to perform the system improvement, and large scale clinical test is going to be conducted continuously so as to verify the medical care effectiveness of this system, in the mean time, clinical assessment method will be developed too.
ACKNOWLEDGEMENT
We are grateful for the support of the National Science Council, Taiwan, under NSC 100-2221-E-008-043- & NSC 100-2631-S-008-001, and Microsoft in Taiwan.
REFERENCES
[1] Lehrer, N., Y. Chen, et al. (2011). "Exploring the bases for a mixed reality stroke rehabilitation system, Part II: Design of Interactive Feedback for upper limb rehabilitation." Journal of NeuroEngineering and Rehabilitation 8(1): 54.
[2] Pandora Pound, Charles Wolfe and Anthony Rudd, The Concept of Patient Motivation: A Qualitative Analysis of Stroke Professionals' Attitudes Niall Maclean, Stroke 2002;33;444-448.
[3] Niall Maclean, Pandora Pound, Charles Wolfe, Anthony Rudd, Qualitative analysis of stroke patients’ motivation for rehabilitation BMJ VOLUME 321 28 OCTOBER 2000
[4] Albert A. Rizzo, PhD, Todd Bowerly, PhD, J. Galen Buckwalter, PhD, Dean Klimchuk, BA,Roman Mitura, MSc, PEng, and Thomas D. Parsons, PhD. A Virtual Reality Scenario for All Seasons: The Virtual Classroom. 2006.
[5] Ashford S, Slade M, Malaparade F, Turner-Stokes L, (2008) Evaluation of functional outcome measures for the hemiparetic upper limb – A systematic review. Journal of Rehabilitation Medicine, 40 (10), 787-795
[6] Krakauer JW, Mazzoni P, Ghazizadeh, A., Ravindran, R., Shadmehr, R., Generalization of Motor Learning Depends on the History of Prior Action (2006). PLoS Biology. October; 4(10): e316.
[7] Lin, J.-H., Hsu, M.-J., et al. (2009). "Psychometric comparisons of 4 measures for assessing upper-extremity function in people with stroke." Phys Ther 89: 840-850
[8] Farrell, T. R., and Weir, R. F. ff., Heckathorne, C. W., (2005): The Effect Of Controller Delay On Box And Block Test Performance. Proceedings of the Myoelectric Controls Conference (MEC2005), Fredericton, New Brunswick, Canada, August 15th – 19th, University of New Brunswick, New Brunswick, Canada
[9] Moriello C, Byrne K, Cieza A, Nash C, Stolee P, Mayo N. Mapping the Stroke Impact Scale (SIS-16) to the International Classification of Functioning, Disability and Health. Journal of Rehabilitation Medicine. 40(2): 102-106, 2008
[10] Desrosiers J, Hebert R, Dutil E, Bravo G. Development and reliability of an upper extremity function test for the elderly: the TEMPA. Can J Occup Ther 1993;60:9-16
[11] Cheng PT, Wang CM, Chung CY, Chen CL. Effects of visual feedback rhythmic weight-shift training on hemiplegic stroke patients. Clin Rehabil 2004; 18: 747 _/753
[12] Roberto Colombo, Fabrizio Pisano, Alessandra Mazzone, Carmen Delconte, Silvestro Micera, M Chiara Carrozza, Paolo Dario and Giuseppe Minuco, Design strategies to improve patient motivation during robot-aided rehabilitation Journal of NeuroEngineering and Rehabilitation 2007, 4:3
[13] Stefano Paolucci; Gabriella Antonucci; Maria Grazia Grasso; Daniela Morelli;Post-Stroke Depression, Antidepressant Treatment and Rehabilitation Results, Cerebrovascular Diseases; 2001; 12, 3; [14] Winstein, CJ, Merians, A, & Sullivan, K. (1999). Motor learning after