無膝痛症狀者髂脛束超音波影像型態在歐伯檢查姿勢以及
改良式歐伯檢查姿勢之表現
計畫類別: 個別型計畫 計畫編號: NSC93-2314-B-002-097- 執行期間: 93 年 08 月 01 日至 94 年 07 月 31 日 執行單位: 國立臺灣大學醫學院物理治療學系暨研究所 計畫主持人: 王興國 共同主持人: 王亭貴 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 94 年 10 月 18 日
Assessment of stretch effectiveness of the iliotibial tract in Ober and modified Ober maneuvers; an ultrasonographic study.
Abstract
Background and Purpose. Effects of therapeutic exercises on morphologic soft-tissue changes as direct indicators of the stretch are unclear. We assessed the accuracy and reliability of ultrasonographic measurements of the iliotibial tract, morphologic changes, and effectiveness of stretching.
Subjects and Methods: In 8 patients with knee injury (mean age= 37.6, SD = 13.5 years), we compared the accuracy of ultrasonographic and magnetic resonance imaging measurements. In 36 healthy volunteers (mean age= 24.3, SD = 4.0 years), width and thickness of the iliotibial tract were sonographically measured with the Ober and modified Ober maneuvers in 3 hip positions. Ten volunteers were retested to assess reliability.
Results: Ultrasonography was accurate (P =.011, r=0.828) and reliable (ICC range = 0.76-0.82) in measuring the width of the iliotibial tract, which significantly changed in the modified maneuver (P =.045). Stretch effectiveness (percentage change) was significantly correlated with hip adduction angles during the modified maneuver (= =.042, r=0.169).
Discussion and Conclusion. Sonographic iliotibial measurements were accurate and reproducible. The modified Ober maneuver appeared to be more valid than the Ober maneuver.
Key Words: iliotibial tract, Ober maneuver, modified Ober maneuver, ultrasonography.
INTRODUCTION
Active or passive stretching with patients in certain positions is frequently used in therapeutic exercises. These stretching exercises increase the length (extensibility) of the soft tissues, mainly by increasing the joint angle in an antagonistic direction.1The effectiveness of such therapeutic stretching is defined as an increase in tissue tension, in the length of the tissue and moment arm, or in the joint angle.2,3For the iliotibial band (ITB), this effectiveness is estimated by stretching the band for palpation and cinemographic and goniometric analyses.2-4Noninvasive in vivo laboratory studies have shown that the gastrocnemius tendon of the leg and the patellar tendon and cruciate ligaments of the knee increase in length from an ankle-neutral position to dorsiflexion and from full extension of the knee to flexion, respectively.5-7Results of cadaveric studies confirm that the main morphologic changes in the soft tissues during a longitudinal stretch are simultaneously decreased cross-sectional area, width, or thickness, in addition to elongation.8,9However, to our knowledge, no studies have been performed to evaluate the effect of therapeutic exercises on morphologic changes in the soft tissues as direct indications of the stretch, and none have been conducted to analyze correlations between percentage of morphological changes and increased joint angles.
To treat ITB friction syndrome, clinicians and physiotherapists often use the Ober or modified Ober maneuver.10In these maneuvers, the ITB or iliotibial tract is
stretched by applying pressure at the end of the range of motion in the hip joint (ie, increasing the hip adduction angle) to increase flexibility of the iliotibial tract and to decrease impingement or friction of the iliotibial tract on the lateral femoral
epicondyle. The Ober maneuver with knee flexed 90° was originally designed to test and stretch the tightness of the ITB and the tensor fascia latae muscle in patients with
low back pain or sciatica.11Kendall modified the Ober maneuver by extending the knee at 0° flexion.12He reported that this modification is more valid and effective than the original maneuver in stretching the ITB and in testing its tightness.13Because of their experience with palpation, some researchers believe that the Ober maneuver may stretch the tensor fascia latae muscle more than the ITB, and they, too, believe that the modified maneuver provides a more effective stretch.2However, without objective and direct evidence, physiotherapists cannot know whether the 2 maneuvers differ in terms of their effectiveness in stretching the iliotibial tract.
Ultrasonography is a real-time, high-resolution, noninvasive imaging tool that has been shown to be valid in measuring the ITB,14,15and the iliotibial tract is where ITB friction commonly occurs.16Therefore, the purpose of this study was to evaluate the use of morphologic changes as indicators of stretch in the iliotibial tract and to define stretch effectiveness in terms of percentage changes by using the Ober and modified Ober maneuvers. We also assessed the accuracy and reliability of ultrasonographic measurements in the iliotibial tract.
SUBJECTS AND METHODS Subjects
From August 2004 to October 2004, we recruited 8 patients with knee injury (7 men and 1 woman, mean agestandard deviation, 34.1 14.1 years) for this study. These patients had a diagnosis of unilateral knee injury and were recruited from the department of medical imaging at a university hospital. Exclusion criteria for these patients included 1) who had an undergone knee surgery; and 2) who had a poorly defined border of the iliotibial tract when the ultrasonographic measurements were
conducted. Table 1 summarizes their clinical features.
From February 2004 to July 2004, we recruited 36 asymptomatic, healthy volunteers (17 men and 19 women, mean agestandard deviation, 24.3 4.0 years; heightSD, 166.9 8.6 cm; weight SD, 58.8 10.6kg) through the university student center. These volunteers served as controls for morphologic changes caused by the stretching force, without the effect of various mechanical conditions on the iliotibial tract, such as injuries. Premeasurement screenings for these healthy
volunteers included history taking and physical assessments. The inclusion criterion for these volunteers was the absence of a history of hip or knee pain that caused them to seek medical help. Exclusion criteria of physical assessments for these healthy subjects were the following: (1) leg-length discrepancy of more than 1.5 cm, genu varum with a tibiofemoral angle of less than 4°, and functional overpronation of the foot (no foot arch when standing) on physical examination; (2) positive response to the Ober or modified Ober maneuver (ie, a hip adduction angle of 0° or less or a hip adduction angle of less than 10°, respectively). In addition, healthy subjects were excluded from this study if they had a focally thickened and poorly defined border of the iliotibial tract, with a fluid collection between the iliotibial tract and the lateral femoral epicondyle when the ultrasonographic measurements were conducted. These anatomic abnormalities and morphologic changes have been postulated as factors that predispose individuals to develop irritation of the iliotibial tract at the level of the lateral femoral epicondyle.14,16,17Our institutional review board approved this study, and all patients and subjects provided informed consent.
Procedure
obtained. In both patients and healthy subjects, measurement accuracy, reliability, and hypothesis testing was performed. Our null hypotheses were that no morphologic changes occur in the iliotibial tract during stretching and that the hip adduction angle is not correlated with the magnitude of any morphologic changes during the Ober and modified Ober maneuvers.
Accuracy of ultrasonographic measurements in patients
All 8 patients with knee injury underwent both ultrasonography for measurement of the width and thickness of the iliotibial tract and magnetic resonance imaging (MRI) for assessment of their injured knee in the department of medical imaging.
Ultrasonography and follow-up MRI were conducted with the patient in a supine position with their injured knee in a relaxed and extended position. Ultrasonographic and MRI measurement was performed respectively by using a portable
Sonosite180plus†and a 1.5-T Magnetom Sonata unitwith an extremity surface coil. The routine protocol at our hospital comprised the following: fast spin-echo
T1-weighted imaging (repetition time/echo time = /19 ms, 800 ms/95 ms, echo train length = 3) and fat-saturated fast spin-echo proton density–weighted imaging
(repetition time/echo time = 4000 ms/19 ms, echo train length = 10) in a sagittal plane, and gradient-echo T2-weighted imaging (repetition time/echo time = 600 ms/15 ms, flip angle = 20º) in the coronal plane. These sequences were performed to facilitate the detection of subtle alterations in signal intensity in the subcutaneous fat. Imaging parameters also included a 256 × 192 matrix, 3-mm section thickness with a 0.5- or 1-mm intersection gap, and a 16-cm field of view for all sequences.
Ultrasonographic measurements and reliability in control subjects
In healthy volunteers, ultrasonographic measurements were performed in the ultrasonography theatre at the university hospital by using an HDI 5000 imaging unit with a 10-5 MHz linear-array transducer (model CL10-5)‡and a maximal axial resolution of 0.7 mm. Because of the configuration of the ultrasonography theatre, only the left lower extremity was measured. Before the measurements were made, the subjects were placed in a relaxed, seated position on an examination table with their knees extended. For ultrasonographic estimation, an investigator drew a line on the subject’sskin by using amarker.Thislinecrossed thelongitudinalaxisofthe iliotibial tract to represent the position of transducer at the level, corresponding to the superior border of patella. The subjects were randomly chosen to perform the Ober maneuver or the modified Ober maneuver first; the other maneuver was performed 30 minutes after the first maneuver.
Measurements were obtained with the subjects lying on the side opposite the side being tested. Their left knee was flexed 90° for the Ober maneuver and positioned at 0° for the modified maneuver. The examiner positioned the transducer on and parallel to the marked line and held it perpendicular to the skin surface to avoid compressing the skin and underlying tissues. With each maneuver, the morphology of the iliotibial tract at the distal end of the knee joint was measured with the hip in 3 positions: neutral, adducted, and stretching.
To prevent internal rotation and flexion of the hip for neutral measurements, an examiner stabilized thesubject’spelvisby pushing theleftanterioraspectofthe superiorilium and by supporting thesubject’sipsilateralkneeduring measurementsof the iliotibial tract. A second examiner placed the inclinometer(AcuAngle, Middletown,
USA),§which had markings of 1º increments, over the lateral epicondyle to confirm that the hip adduction angle was neutral (ie, 0°). Then ultrasonographic measurements of the thickness and width at the suprapatellar level of the iliotibial tract were taken.
In the adducted hip position,thesupportthathad been applied to thesubject’sleft (test) knee was removed, and the knee was allowed to drop (adduct) into the available range of adduction until hip movement stopped. The examiner controlled the speed with which the knee joint was lowered to allow the ultrasonographic examiner to trace the image of the iliotibial tract and measure its thickness and width without moving the transducer from the marked line. The end angle of hip adduction was measured by placing the inclinometer on the lateral epicondyle after the ultrasonographic and hip-angle measurements were recorded. Each subject was then instructed to relax and return the hip to its neutral position.
For the stretching position and applying a pressure, a 3-kg sand bag was hung on thedistalend ofthesubject’sleftkneeto createpressureon theiliotibialtractatthe end of the range of motion of the hip joint. Then the support that had been applied to test the knee in the neutral hip position was removed. The left knee was allowed to drop further in the available range of adduction until hip movement stopped. Again, we measured the thickness and width of the iliotibial tract and the end angle of hip adduction by using sonograms and the inclinometer.
Morphologic changes in the thickness and width of the iliotibial tract were measured as the percentage change relative to the origin and defined as stretch effectiveness. To assess intratester test-retest reliability, 10 of the 36 subjects were randomly chosen to undergo a repeat of the same protocol on a second day with the same investigators.
Statistical analysis
In patients, the accuracy of ultrasonographic measurements in the iliotibial tract was estimated by means of a paired t test (with 95% confidence limits) and a Pearson bivariate test. With these tests, we compared mean differences in morphologic
parameters, including width and thickness of the iliotibial tract, measured with ultrasonography and with MRI. We also estimated the linear correlation of the morphologic parameters obtained with ultrasonographic and MRI.
In healthy volunteers, repeated 1-way analysis of variance with post hoc testing was used to analyze differences in the width and thickness of the iliotibial tract in the 3 hip positions for each maneuver. Correlations between stretch effectiveness
(percentage changes) and changes in hip adduction angles, from the neutral to the stretching positions, were analyzed by using the Pearson bivariate correlation test. In addition, a paired t test was used to analyze mean differences in the hip angles during the Ober and the modified Ober maneuvers. The intrarater intraclass correlation coefficient was used to estimate the reliability of the ultrasonographic measurements.
Results
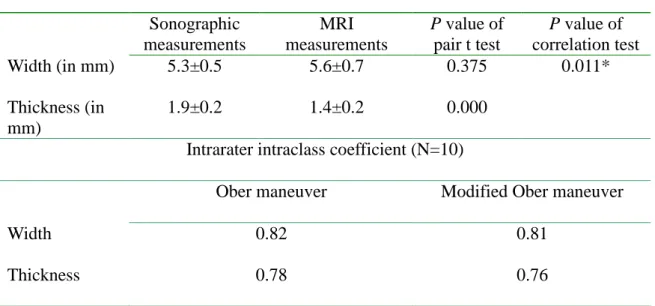
Table 2 presents the results of our analysis of mean differences and correlations among the morphologic parameters, including width and thickness, obtained with ultrasonography and MRI. The intrarater intraclass correlation of ultrasonographic measurements ranged from 0.76 to 0.82 (Table 2).
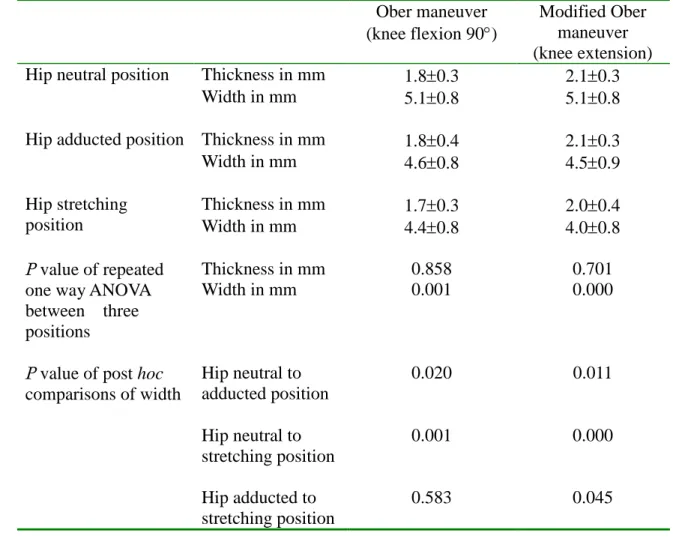
Changes in the width of the iliotibial tract when a 3-kg pressure was applied were
significant with the modified Ober maneuver (P = .045) (Table 3). Correlations between the hip angles and the stretch effectiveness of the iliotibial tract width was significant with the modified Ober maneuver (P = .042, r = 0.169). Furthermore, the angle of hip adduction in modified Ober maneuver was significantly greater than that of Ober maneuver (P = .010, power = 0.8) (Table 4).
Discussion
The ITB is a continuation of the tensor fascia latae and the gluteus maximus at the lateral aspect of the thigh. It attaches distally to the Gerdy tubercle of the lateral tibial condyle, to the lateral patella retinaculum, and to the head of the fibula. At its attachment, the ITB separates into 2 functional components, the iliopatellar band and the iliotibial tract.18
Our main results showed the following: First, ultrasonographic measurements of the width of the iliotibial tract were both accurate and reliable. Second, significant reductions in width occurred during stretching in the modified Ober maneuver. Third, the hip adduction angle and the percentage change in the width of the iliotibial tract (stretch effectiveness) were significantly correlated in the modified Ober maneuver. The magnitudes of these morphologic changes under effective stretching are believed to be associated with total forces applied in the longitudinal axis, mechanical
properties of the soft tissues, and passive angular displacement of the joints.4-9Our findings may indicate that iliotibial tract was subjected to more significant and specific stretching in the modified Ober maneuver than that in the original maneuver; therefore, the authors suggest that the modified Ober maneuver is more valid and provides more effective stretching than does the Ober maneuver.
extended, places less stress on the medial aspect of the knee and also minimizes potential interference by a tight rectus femoris muscle.13In the Ober maneuver, such potential interference mainly involves the rectus femoris and tensor fascia latae
muscles because the rectus femoris muscle, which crosses the hip and the knee, is also stretched when the knee is flexed in theOber’smaneuver.4,12In addition, both the iliotibial tract and the tensor fascia latae are the main structures under stretch in the Ober maneuver; therefore, the specificity of stretching on the iliotibial tract is
reduce.13Gajdosik et al suggested that the increased tightness of the fascia latae over the anterolateral aspect of the thigh, which is appreciated by palpating the flexed knee and comparing it to the extended knee, demonstrates the influence from the tensor fascia latae muscle.4In our study, we objectively found significant morphologic changes in the width of the iliotibial during the modified Ober maneuver and could usethestretch effectiveness(percentagechange)to supportKendall’sassumption.In addition, the decreased width and increased length that Fredericson et al2described are consistent with findings of previous studies of stretching regarding the
coracoclavicular and cervical spine ligaments.8,9These results may signify that morphologic changes surely occur during effective therapeutic stretching. Further studies of therapeutic stretches in which morphologic changes are used as indicators of stretching effectiveness are needed.
In the modified Ober maneuver, the effectiveness of stretching the iliotibial tract—ie, percentage changes between the adducted or stretched hip position and the neutral position—were significantly correlated with increased hip adduction angles (Table 3). This finding may suggest that a significant correlation between stretch effectiveness and increased joint angle should be included as a criterion of a valid stretch. In the modified Ober maneuver, changes in the magnitude of stretching on the
iliotibial tract can be estimated by using the change in the hip adduction angle. This finding confirms that, during an effective stretching exercise, stretch effectiveness can be increased by increasing the joint angle in an antagonistic direction.
In this study, we used an inclinometer, which has been proven to be reliable in measuring the flexibility of the ITB during the Ober and modified Ober maneuvers.3 The angle of hip adduction in the position for the modified Ober maneuver was greater than that of the Ober maneuver. This finding is consistent with previous observations.3,4Furthermore, sonographic measurements of the width of the iliotibial tract have been proven accurate and reliable. In our study, the mean thickness of iliotibial tract was similar to the findings at the lateral femoral condyle that Goh et al15 reported, though they are not significantly correlated with the MRI measurements. Thickness of the iliotibial tract did not change when it stretched in either the Ober or the modified Ober maneuvers. Probable reasons for the poor accuracy of the thickness results include the following: First, ultrasonography does not have the same precision as that of MRI in measuring the thickness of the healthy iliotibial tract. Second, the initial thickness of the iliotibial tract was only 1.8 mm, and the changes might have been too small to be depicted given the limited axial resolution (0.7 mm) of the ultrasonic probe. Bonaldi et al. reported that thickening of the iliotibial tract, which increases to 13 mm, is one of main findings in patients with ITB friction syndrome. Our control subjects were healthy and lacked any history of hip or knee pain. As such, the correlations between stretch effectiveness and hip adduction angles in these subjects may not be applicable to patients with ITB friction syndrome, as the mechanical properties differ between the groups.
We recommend a new method for assessing the effectiveness of stretching with ultrasonography. However, some doubts should be discussed. For instance, direct
comparison of the effects of stretching between the Ober maneuver and the modified Ober maneuver could be questioned. It is possible that the iliotibial tract was not measured at the same point in the 2 maneuvers, though all ultrasonographic
measurements were performed at the suprapatellar level. Movement of the iliotibial tract between knee angles of flexion and extension make direct comparison
questionable. However, the initial thickness and width of iliotibial tract were the same on both maneuvers, implying that the same area was measured. We assumed that the change in the width of the iliotibial tract mainly reflected the strain on the structure. However, without inserting a strain gauge parallel to the iliotibial tract and without measuring length of the whole ITB directly, we could not exclude the possibility that the changes in width were a consequence of ourchanging theposition ofthesubject’s leg and knee.
Conclusion
Ultrasonographic examination may provide an objective and dynamic method for verifying clinical maneuvers. Stretch effectiveness differed between the modified Ober maneuver and the Ober maneuver. The modified maneuver resulted in
morphologic changes in the iliotibial tract that were correlated to the angle of hip adduction.
REFERENCES
1. Winters MV, Blake CG, Trost JS, Marcello-Brinker TB, Lowe LM, Garber MB, Wainner RS. Passive versus active stretching of hip flexor muscles in subjects with limited hip extension: a randomized clinical trial. Phys Ther.
2004;84:800-807.
2. Fredericson M, White JJ, MacMahon JM, et al. Quantitative analysis of the relative effectiveness of 3 iliotibial band stretch. Arch Phy Med Rehabil. 2002;83:589-592.
3. Reese NB, Bandy WD. Use of an inclinometer to measure flexibility of the iliotibialband using theOber’stestand themodified Ober’stest:differencein magnitude and reliability of measurements. J Orthop Sports Phys Ther.
2003;33:326-330.
4. Gajdosik RL, Sandler MM, Marr HL. Influence of knee positions and gender on theOber’stestforlength oftheiliotibialband.Clin Biomech. 2003;18:77-79.
5. Maganaris CN, Paul JP. Tensile properties of the in vivo human gastrocnemius tendon. J Biomech. 2002;35:1639-1646.
6. Sheehan FT, Drace JE. Human patellar tendon strain: a noninvasive, in vivo study.
Clin Orthp. 2000;370:201-207.
7. Li G, Defrate LE, Sun H, Gill TJ. In vivo elongation of the anterior cruciate ligament and posterior cruciate ligament during knee flexion. Am J Sports Med. 2004;32:1415-1420.
8. Costic RS, Vangura Jr A, Fenwick JA, et al. Viscoelastic behavior and structural properties of the coracoclavicular ligament. Scand J Sports Med. 2003;13: 305-310.
of human cervical spine ligaments. J Biomech. Eng. 2000;122:623-629. 10. Fredericson M, Guillet M, DeBenedictis L. Quick solutions for iliotibial band
syndrome. Phys Sportsmed. 2000;28:53-68.
11. Ober FR. The role of the iliotibial band and fascia lata as a factor in the causation of low back disabilities and sciatica. J Bone Joint Surg Am. 1936;18:105-110. 12. Kendall HO, Kendall FP, Boynton DA. Posture and Pain. Baltimore, Williams
and Wilkins;1970:135-138.
13. Kendall FP, McCreary EK, Provance PG.. Muscles testing and function, fourth ed. Baltimore, Williams and Wilkins;1993:56-59.
14. Bonaldi VM, Chhem RK, Drolet R, et al. Iliotibial band friction syndrome: sonographic findings. J Ultrasound Med. 1998;17:257-260.
15. Goh LA, Chhem RK, Wang SC, et al. Iliotibial band thickness: sonographic measurement in asymptomatic volunteers. J Clin Ultrasound. 2003;31:239-244. 16. Muhle C, Ahn JM, Yeh L, et al. Iliotibial band friction syndrome: MR imaging
findings in 16 patients and MR arthrographic study of six cadaveric knees.
Radiology. 1999;212:103-110.
17. Nishimura G, Yamato M, Tamai K, et al. MR findings in iliotibial band syndrome.
Skeletal Radiol. 1997;26:533-537.
18. Terry GC, Hughston JC, Norwood LA. The anatomy of the iliopatellar band and iliotibial tract. Am J Sports Med. 1986;14:39-45.
Table1. Clinical summary of eight knee injured patients. Patient no. Gender Age (years) Injured knee Duration of symptoms Athletic activity level Comments
1 Male 33 Left 1 months Recreational ACL injury
2 Female 64 Right 2 years Non-athlete ACL injury
3 Male 33 Right 1 months Non-athlete PCL injury
4
Male 22 Right 2 weeks
Recreational Medial meniscus lesion
5 Male 44 Left 4 months Recreational PCL injury
6 Male 39 Left 2 months Non-athlete ACL injury
7 Male 23 Right 1 month Recreational Tendinitis
8 Male 43 Right 2 months Non-athlete LCL injury
ACL and PCL are abbreviations of anterior cruciate ligament and posterior cruciate ligament respectively. LCL means lateral collateral ligament.
Table 2. Accuracy and reliability of ultrasonographic measurements on the iliotibial tract.
Mean difference and correlation (N=8) Sonographic measurements MRI measurements P value of pair t test P value of correlation test Width (in mm) 5.3±0.5 5.6±0.7 0.375 0.011* Thickness (in mm) 1.9±0.2 1.4±0.2 0.000
Intrarater intraclass coefficient (N=10)
Ober maneuver Modified Ober maneuver
Width 0.82 0.81
Thickness 0.78 0.76
Table 3. Mean values and standard errors of ultrasonographic estimation of the iliotibial tract in Obe and modified Ober maneuvers.
Ober maneuver
(knee flexion 90) Modified Obermaneuver (knee extension)
Thickness in mm 1.80.3 2.10.3
Width in mm 5.10.8 5.10.8
Hip neutral position
Thickness in mm 1.80.4 2.10.3
Width in mm 4.60.8 4.50.9
Hip adducted position
Thickness in mm 1.70.3 2.00.4 Width in mm 4.40.8 4.00.8 Hip stretching position Thickness in mm 0.858 0.701 P value of repeated
one way ANOVA between three positions
Width in mm 0.001 0.000
P value of post hoc
comparisons of width Hip neutral to adducted position 0.020 0.011 Hip neutral to stretching position 0.001 0.000 Hip adducted to stretching position 0.583 0.045
Table 4.Mean and standard errors of changes in percentage (stretch effectiveness) of the iliotibial tract width and correlations between changes and hip angles in Ober and modified Ober maneuvers.
Ober maneuver (knee flexion 90) Modified Ober maneuver (Knee extension) Change of ITB width to
neutral position in (%)
Hip angle
in Change of ITB width toneutral position in (%)
Hip angle in Adduced 9.510.6 18.84.6 11.810.8 21.15.5* Stretching 13.310.4 27.16.8 21.19.6 28.75.8a Correlations between hip angle and changes p=0.212 r=0.149 p=0.042 r=0.169
* andarepresent significant difference of hip angles between Ober and the modified Ober maneuvers, * means p value = 0.010,ameans p value = 0.168.
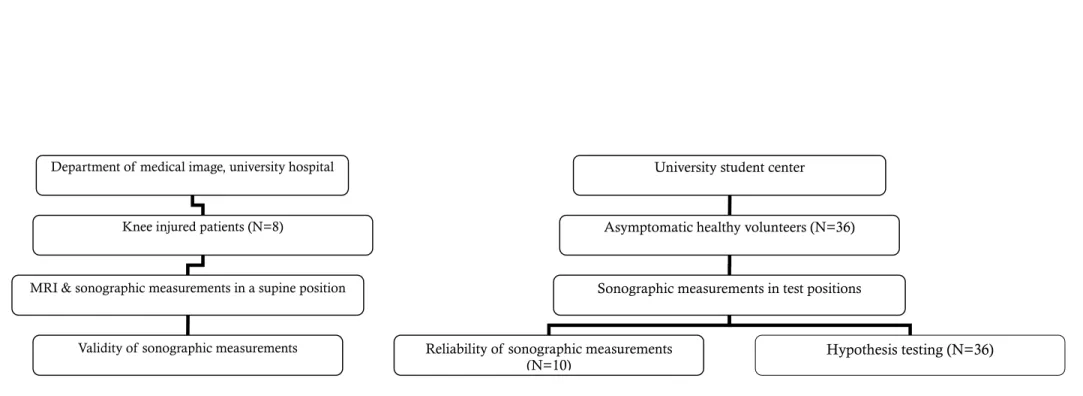
Figure 1. Study design and sequence of measurement, according to objectives.
Department of medical image, university hospital University student center
Knee injured patients (N=8) Asymptomatic healthy volunteers (N=36)
MRI & sonographic measurements in a supine position Sonographic measurements in test positions
Validity of sonographic measurements Reliability of sonographic measurements