Bulletin of Educational Psychology, 2010, 41(4), 859-884 National Taiwan Normal University, Taipei, Taiwan, R.O.C.
The Treatment of Substance Abuse Disorders by the
Psychological Forgiveness
Wei-Fen Lin
Department of Educational Psychology and Counseling National Hsinchu University of Education
The purpose of this study was to explore the effect of Enright forgiveness intervention with substance abusers who have been hurt in domestic interpersonal relationships. In this study, the researcher examined the relative merits of Enright’s forgiveness intervention and an alternative treatment intervention for adults. The researcher recruited 12 experiment and 12 alternative treatment participants. The participants were administrated these six measures at pretest, posttest, and follow-up test: the Enright Forgiveness Inventory, the Beck Depression Inventory-II, the Coppersmith Self- Esteem Inventory, the State-Trait Anxiety Inventory, the Spielberger State-trait Anger Scale, and the Lin Vulnerability to Drug Use Scale. The results showed that the experiment group had significantly greater gains in forgiveness, and self-esteem, and greater decreases in depression, anxiety, and vulnerability to drug use from pretest to posttest. Furthermore, the experimental group had significantly greater gains in forgiveness, and self-esteem, and greater decreases in depression, anger, anxiety, and vulnerability to drug use from pretest to a 4-weeks follow-up. The level of forgiveness was significantly negatively correlated with depression, anger, anxiety, and vulnerability to drug use, and positively correlated with self-esteem at posttest.
KEY WORDS: anger, anxiety, depression, forgiveness, self-esteem
Substance abuse is a serious disorder that powerfully modifies the abusers' nervous system and every organ functioning in the human body either directly or indirectly. The National Institute of Alcohol Abuse and Alcoholism (2000) pointed out that about 100,00 deaths in the united states are related with substance abuse, making them the fourth leading cause of mortality after heart disease, cerebrovascular
本論文曾於「2008 年全球化趨勢下的教育革新與展望-兩岸四地學術研討會」上發表,並依評論委員意見加以修
disease, and cancer (Enright, & Fitzgibbons, 2004). Furthermore, approximately 32% of suicides and half of all homicides are substance-related. In addition, a significant percentage of violent and non-violent crimes are related to the influence of substance. In social and family problems, substance use can also have some negative social consequences, such as loss of career, friends, and family. Moreover, some domestic violence, such as physical or sexual abuse, is related to substance abuse. Medical complications can even reach into the next generation, in that maternal drinking during pregnancy can cause infant psychological syndrome, and other serious birth defects. Parental alcohol abuse is the leading known cause of mental retardation (Straussner, 1993). With respect to the social costs of substance abuse, it is estimated that more than 25% of property crimes and 15% of violent crimes are related to it. Financial losses related to these crimes have been estimated at 1.7 billion per year. Homicide is also strongly linked to activities surrounding substance dealing. Approximately 14.8% of all homicides per year are causally related to that. The costs for criminal justice activities directed against substance trafficking on the federal level were approximately 2.5 billion dollars (Clark & Winters, 2002).
The Definition of Substance Abuse
In essence, the severity of substance abuse differs from mild to severe, which refers to compulsive use of a chemical and continued use despite adverse consequences. The potential for addiction of different substances varies greatly. However, the negative emotions related to different substances are similar. In this study, the researcher will use the definition of substance abuse from DSM-IV. The definitions of substance abuse from DSM-IV are as follows: 1. A substance is often taken in larger amount or over a longer period than the person intended. 2. Persistent desire on one or more unsuccessful effects to cut down or control substance use. 3. A great deal of time spent in activities necessary to get the substance, take the substance, and recover from its effects. 4. Frequent intoxication or withdrawal symptoms when expected to fulfill major role obligations at work, school, or home, or substance use is physically hazardous. 5. Important social, occupational, or recreational actives given up or reduced because of substance use. 6. Continued substance use despite knowledge of having a persistent or recurrent social, psychological, or physical problem that is caused or exacerbated by the use of the substance. 7. Marked tolerance; need for markedly increased amounts to the substance in order to achieve intoxication or desires effect, or markedly diminished effect, which continued use of the same amount. 8. Characteristic withdrawal symptoms. 9. Substance often taken to relieve or avoid withdrawal systems.
A Framework of Anger Relapse of Substance Abuse
Spielberger (1983) defines anger as an immediate emotional state that can range from mild irritation to rage. He believes that anger includes these subtypes: (1) aggression, an actual behavior intended to harm another; (2) hostility, an attitude toward a specific person or the world; (3) resentment, a process in which anger is stored; and (4) hatred, the end product of resentment. Williams and Williams (1993) define anger in a similar position. They define anger as an emotional state influenced by personal expectations, often unrealistic in nature that generates reactions from minor irritation to aggressive behavioral acts. Clancy (1996) defines anger as a combination of biopsychosocial factors whose interaction leads to a highly variable pattern of response choice.
In this study, anger is defined as a chronically negative emotion which combines pain and fear. The source of anger in this study comes from interpersonal conflict or offense. Anger not only influences
individuals' psychological functioning, but also causes physical problems.
A Model of High Risk for Relapse of Anger in Substance Abuse Disorders
Clancy (1996) provides an anger-relapse model to illustrate how anger-reducing events perceptive the occurrence of substance abuse. In the first phase, an event igniting anger happen, which causes an individual to react? In the second, an individual may feel pain and fear, with reduced self-esteem. In this phase, individuals use different defense mechanisms to reduce their anger. They may assess options before using one of defense mechanisms. For substance abusers, their choices do not preserve their self-esteem. In the third phase, after individuals try to use defense mechanisms, they will use their coping strategies to solve their anger. However, substance abusers may lack accurate skills to cope with the events. In this phase, individuals may lose their sense of control because their anger becoming high. In the fourth phase, individuals express their anger by using substance. They can temporary relieve their anger (pain and fear) and clam down for a while. In the final phase, individuals will become addicted since the even becoming unsolved.
Psychological Profiles of Substance Abuse Disorders Anger
Anger is perhaps the most serious symptom for alcohol or other drug abuser (Clancy, 1996). According to Alcoholic Amorous(AA, 1976), anger is the number one〝offender〞. It destroys more alcoholics than anything else. It is plain that a life that includes deep anger leads only to futility and unhappiness. Tivis, Parsons, and Nixon (1998) exploring the relationships among anger variables, past drinking behavior, and substance abuse consequences in alcoholics by using the Spielberger Anger Expression Inventory, the Beck Depression Inventory, and the Spielberger State Anxiety Inventory. Results found that anger was one of the significant factors related to alcohol and other drug abuse. Forgays, Richards, Fgays, and Sujan (1999) searched for the link between negative emotions and later health problems. Results indicated that participants, who regularly use tobacco and alcohol, significantly had more anger, hostility, and aggressive behavior than those who used such substance less.
Anxiety
Anxiety is one of common psychological symptoms for substance abusers since alcohol or other drug abusers are likely to experience stress in their life. Although some anxiety has a positive effect on the individual's functioning (e.g., anxiety motives us to be more productive.), it complicates life when it becomes more serious. Given the nature of anxiety disorders, it is not surprising that individuals use substance to relieve their symptoms. Fields (1992) pointed out that estimates of those suffering from anxiety disorders that use substance have varied from less than 12 percent to more than 35 percent. Kushner, Sher, and Erickson (1999) used cross-sectional studies to investigate the association between anxiety disorders (generalized anxiety disorder, agoraphobia, and social phobia or panic) and the use of alcohol or other drugs. Results showed a robust association between anxiety disorders and substance use. They also found that participants diagnosed with anxiety disorders at younger ages consumed more substance (Dodge & Potocky, 2000).
Depression is a common symptom in those who abuse substance. Patten and Charney (1998) found that substance abusers had significantly more diagnosed depression disorders than non-abusers. They evaluated associations between alcohol consumption and major depression in a Canadian population by analyzing data from the Canadian National Population Health Survey (NPHS). The NPHS used a probability sample of 17,626 participants (age 12 to 80) and included measures of alcohol ingestion and a diagnostic screening for major depression (the Composite International Diagnostic Interview Short Form). Results showed that participants reporting any drinking in the year preceding the interview were more likely to have experienced an episode of major depression during that time than participants reporting no drinking. Participants reporting maximal ingestions of 5 or more drinks (and especially 10 or more drinks) on at least 1 occasion during the preceding year were also at greater risk of major depression than participants who had non-drinking or reporting smaller maximal ingestions.
Hopelessness One psychological symptom of substance abusers is hopelessness. Kingree, Thompson, and Kaslow (1999) suggested that hopelessness is one of three important factors related to the use of substance. MacQueen (1999) also pointed out that hopelessness may be one of causes related to the use of substance. He suggested that increased hope was an important strategy to help substance to recover.
Suicide Research indicates that 20 to 36% of suicide victims have a history of substance abuse or drinking shortly before their suicide (Colliver & Malin, 1986; U.S. Department of Health and Human Research, 1990). Many studies have shown a significant relationship between suicide ideation and the use of substance. For example, Lester (1995) investigated the time-series associations among alcohol use and rates of personal violence (suicide and homicide) in various nations (10 European nations, New Zealand, Canada, and the US) and 9 nations for homicide rates (6 European nations, New Zealand, Canada, and the US). Results indicate that, in many but not all nations, in times when alcohol consumption was higher, suicide and homicide rates were also higher. The association between rates of personal violence and alcohol consumption was significant.
The most common condition prompting substance abuse is that individuals want to seek relief after they have been hurt or have feelings of frustration (Clancy, 1996). Wanberg and Milkman(1998) pointed out that substance abuse disorder is associated with social and psychological difficulties that give rise to anger in the user and others, including family conflicts, parental neglect, child abuse, social isolation behavior, and unemployment. The clinical experiences of many therapy support anger is prevalent in the substance abuse disorders. Much empirical research has also pointed out that substance use is one kind of expression which releases anger. Huizinga, Loeber, and Thomberry (1994) pointed conduct disorders in adolescents have been shown to precede substance abuse by several years. Thomas (1993), and Wood and Duffy (1996), for example, suggested that substance not only provide the users with missing feelings of adequacy and acceptance needed for them to express their anger, but also provides the permission to release anger. Conversely, alcohol's depressive effect can release or increase the user's feeling of anger.
Some studies showed that cynical hostility can be a factor to general anger readiness (Clancy, 1996). This notion may provide some insight into the relationship between substance and anger. Leiker and Hailey (1988) found that participants scoring higher on hostility and anger scales tended to drink more alcohol, compared to participants scoring lower on these scales.
Therefore, anger is a risk factor that may cause individuals to abuse substance. Marlatt (1985) emphasized the importance of anger and frustration as triggers for relapse in both intrapersonal and in
personal domains. He noted that 29% of relapses are related to intrapersonal frustration and anger, and that 16% are related to interpersonal conflict and associated anger and frustration.
Thus, many therapists identify substance abuse disorders as their angriest, most abusive, and violent patients (McCord, 1992). Some patients in recovery stage show that their sobriety is threatened because they lack an understanding of ways to cope effectively with their anger. The expression of anger in patients continues to be the method most often recommended by therapists. Yet, the limitation of the approach have been described in the literature (Daley & Raskin, 1991; Fitzgibbons, 1998). Forgiveness, however, has been recommended as a way of working through past anger. The Enright process model of forgiveness is a pioneering effort to be empirically validated (Enrighy & Fitzgibbons, 2004).
The importance of forgiveness has been explored in a range of philosophical and psychological settings. In philosophy, forgiveness is often labeled as sublime, restorative, humming, courageous, and healthy. In a psychological setting, forgiveness had been demonstrated to be one of the best interventions to healing hurts caused by interpersonal injures. Forgiveness is a way to release negative emotions, such as anger, depression, anxiety, and hostility. The forgiveness process also can help the injured to face their pain, release their anger, anxiety, and depression, increase positive affect for the injurer, and even lead to a new relationship with the offender in the future.
The Definition of Interpersonal Forgiveness
The definition of interpersonal forgiveness refers to one person forgiving another, not to the deity-human relationship or to one group “forgiving” another. An informal definition of forgiveness is this: One who is deeply hurt by another often resents the other; as the injured party ceases resentment toward the other, he or she gives the person the unconditional gift of acceptance as a human being. A more formal definition is this: “Forgiveness is the overcoming of negative affect and judgment toward the offender, not by denying ourselves the right to such affect and judgment, but by endeavoring to view the offender with compassion, benevolence, and love while recognizing that he or she has abandoned the right to them” (Enright, Gassin & Wu, 1992).
A Model of Forgiveness Intervention Process
Genuine acts of forgiveness can lead to an overall improvement in a person's emotional health. As Enright (2001) points out, as one forgives, one grows as a person capable of courage, nurturance of others, and loves. Through forgiveness intervention, individuals can leave negative emotions and find new meanings in life. The forgiveness intervention is based on a process model developed by Enright and the Human Development Study Group (1991). This model contains four phases and twenty units.
The first phase is the uncovering phase. The goal of this phase is for clients to have a much better understanding about how original of fairness and their reaction to it have affected their psychological health. This involves a number of pains. At the end of this phase, the layers of pain that the client may have explored anger, shame, depleted energy, cognitive rehearsal, comparisons between the offender and self. (Enright & Fitzgibbons, 2004) Here the person examines the depth of anger, resentment, and psychological pain. As Holmgren (1995) pointed out, as a person develops self-respect, he or she sees and acknowledges the injustice. This phase includes: (1) The examination of psychological defenses, which includes denial, repression, projection, reaction formation; (2) Anger needs to be confronted with the intention of releasing it; (3) Shame needs to be admitted, if appropriate; (4) Being aware of cathexis,
which is an attachment of excessive emotional energy to the hurtful event; (5) Awareness of cognitive rehearsal, which is the replay of the hurtful event over and over in one's mind; (6) Comparing one's distress with the perceived better condition of the offender' life; (7) Confronting the fact that one may be permanently and adversely changed by the injury; (8) Being aware of undeserved psychological pain ( Ostermdorf, 1999).
The second phase is the decision phase. Emotional pain can be a great motivator to seek help and to change. The knowledge gained in this phase can serve as the motivator to continue. This motivation cab is the ides to decide forgiveness (Enright & Fitzgibbons, 2004) It includes: (9) Understanding that previous strategies have not achieved the desired result; (10) Considering forgiveness as an option; (11) Making the commitment to forgive. At the end of this phase, one is willing to forgive the offender.
The third phase is the work phase. When a patient progresses to this phase, he or she is entering into the deep process of forgiveness. The work can help clients for emotional relief and possibly even reestablished relationships (Enright & Fitzgibbons, 2004). This phase consists of (12) Reframing the offender by viewing him/her in context; (13) Feeling empathy towards the offender; (14) Developing compassion towards the offender; (15) Absorbing the pain, which may be physical, emotional, mental or all three relief.
The last phase is the deepening phase: deepening insights, relationships to others, and relations to the world at large emerge. In this phase the clients would feel resentments reduce and as a sense of beneficence grows, lower levels of anxiety or depression and higher levels of hope and self-esteem emerge (Enright & Fitzgibbons, 2004). This phase includes: (16) Finding meanings in suffering; (17) Being aware of his/her needs for another person's forgiveness in the past; (18) Realizing he/she is not alone since he/she can get support in this process; (19) Experiencing a new purpose in life because of the injury; (20) Being awareness of emotional relief. The therapeutic goals for each of the four phases are described in table1 and table2.
Table 1 Goal of the Phases of Forgiveness1
Phase Goal
Uncovering Client gains insight into whether and how the injustice and subsequent injury have compromised his or her life .
Decision Client gains an accurate understanding of the nature of forgiveness and makes a decision to commit to forgiving on the basis of this understanding .
Work Client gains a cognitive understanding of the offender and begins to view the offender in a new light , resulting in positive change in affect about the offender, about the self, and about the relationship .
Deepening Client finds increasing meaning in the suffering, feels more connected with others,and experiences decreased negative affect and, at times, renewed purpose in life .
1Enright & Fitzgibbons, 2004, p.67 (見下例)
Table 2 The Phases and Units of Forgiving and the Issues Involved2
UNCOVERING PHASE
1. Examination of psychological defenses and issues involved 2. Confrontation of anger ; the point is to release, not harbor, the anger 3. Admittance of shame, when this is appropriate
4. Awareness of deleted emotional energy 5. Awareness of cognitive rehearsal of the offense
6. Insight that the injured party may be comparing self with the injurer
7. Realization that oneself may be permanently and adversely changed by the injury 8. Insight into a possibly altered“ just world” view
DECISION PHASE
9. A change of heart/conversion/new insights that old resolution strategies are not working 10. Willingness to consider forgiveness as an option
11. Commitment to forgive the offender WORK PHASE
12. Reframing, through role-taking, who the wrongdoer is by viewing him or her in context 13. Empathy and compassion toward the offender
14. Bearing/accepting the pain 15. Giving a moral gift to the offender DEEPEING PHASE
16. Finding meaning for self and others in the suffering and in the forgiveness process 17. Realization that self has needed others’forgiveness in the past
18. Insight that one is not alone
19. Realization that self may have a new purpose in life because of the injury
20. Awareness of decreased negative affect and, perhaps, increased positive affect, if this begins to emerge, toward the injurer; awareness of internal, emotional release
Synthesis of the Literature on Forgiveness and Substance Abuser Disorders
Forgiveness intervention has shown to be an effective in improving psychological health. Research has pointed out that forgiveness interventions can increase self-esteem, hope, psychological well-being, and levels of forgiveness, and decrease anger, anxiety, and depression.
The psychological profile of substance abusers indicates, among other variables, higher anger, anxiety, depression, suicidal attempts, and lower self-esteem, hope than the general population. Treatment intervention for substance abusers around general quitting skills or some psychotherapy (i.e, person-centered therapy, behavioral therapy, rational-emotive therapy), or anger-management do not target the cause of substance abuse in the treatment process. Substance abusers have more anger than the general population. Forgiveness interventions can reduce anger caused by interpersonal hurt. Thus, a forgiveness intervention might be a good tool for substance abusers in resolving psychological problems and increasing mental health. In this study, the researcher will examine the relative merits of a forgiveness program and a support (client- centered) program for adults in a drug rehabilitation center.
Enright and the Human Development Study Group (1991) have examined this construct in depth and have produced a process model describing the steps through which one cycles in forgiving another (Enright, Gassin, & Wu, 1992), and an instrument designed to measure the extent to which one has forgiven another. They have demonstrated that forgiveness is an effective intervention to heal negative emotions and pain among incest survivors (Freedman, 1994), love-deprived adolescents (Al-Mabuk, & Enright, 1995), men who suffer from their partner's abortion (Coyle, & Enright, 1997), insecure -attachment college students (Lin, 1998), elderly females who suffered from interpersonal hurt (Hebl, & Enright, 1993), adult children, the marital enrichment (Ripley & Worthington 2002), and adult children of Alcoholics (Ostermdorf, 1999). The results of these studies supported that forgiveness intervention has a significant healing effect for persons who suffered interpersonal hurt.
In substance abuse psychotherapy, there are many therapies which focus on quitting skills. These quitting skill interventions have not been particularly effective in stopping alcohol or drug abuse. The clinical setting found that many substance abusers start to use alcohol or drugs again after finishing the quitting skill intervention, although recently, some researchers have started to pay more attention to the psychological factors which relate to addiction behaviors, such as individual emotional cycles, coping strategies, personality, and problem-solving abilities. These psychotherapists offer some strategies to help these abusers. Anger-management intervention, behavioral therapy, cognition-behavior therapy, and client-centered interventions are the most common approaches used to reduce the psychological problems of alcohol or drug abusers. Therefore, this study is to test the effect of a forgiveness intervention on the treatments of substance abuser disorders in the short and long run. Hester and Miller (1995), and Enright (2004) suggested that the success of intervention should include short-term and long-term effects. The four to eight weeks follow-up is an appropriate time to test the long-term effect of a psychotherapy. Thus, in this study, the four week follow-up test will be measured to examine any wah-out for the forgiveness group once treatment ceases.
Purpose of This Study
The purpose of this study is as follows:
1. To explore the effect of Enright forgiveness intervention on substance abuse disorders who have been hurt by interpersonal offense.
2. To increase the positive emotions of substance abuse disorders who have been hurt by interpersonal offense.
3. To lessen the negative emotions of substance abuse disorders who have been hurt by interpersonal offense.
4. To reduce the sense of vulnerability to drug use in this sample exposed to Enright forgiveness intervention.
5. To explore the relationship between the degree of forgiveness and anger, anxiety, depression, self-esteem, and vulnerability to drug use on substance abuse disorders who have been hurt by interpersonal offense.
6. To provide a new intervention for educational and clinical practice for substance abuse disorders who have been hurt by interpersonal offense.
Method
Participants and Setting
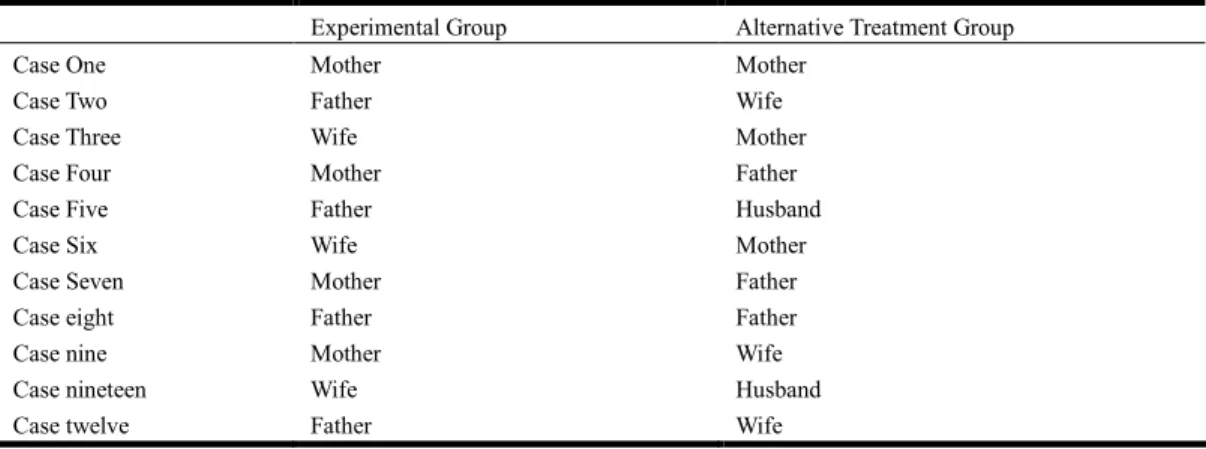
The participants were chosen from a drug rehabilitation center for residential patients in the Midwestern of united States. The characteristics, psychotherapeutic diagnosis, and injurer of participants are shown in the Table 3 and Table 4. Each participant was asked to identify the one central person who acted so unfairly to the participant and to contribute to that participant’s drug use. The offender identified became the focus of that participant’s forgiveness intervention. That offender also was the focus of the subsequent administration of the forgiveness scale. In the treatment group, Eight of them were deeply hurt by their parents. Four were deeply hurt by their wife/husband. In the alternative treatment group, half of them were deeply hurt by parents, and others were deeply hurt by their wife-husband.
The substance rehabilitation center offers intense and structured residential inpatient treatment for persons suffering from substance dependencies often with co-existing mental health problems. Twenty-four in- participants are in the treatment of this study at any given time. The mission of the center is to provide chemically dependent persons with the safe, caring, and chemical free environment which is necessary for clients to stop their substance use and begin the recovery process toward sobriety and improved mental health.
Table 3 The Characteristics of Participants
Experimental Group Alternative Treatment Group Total Gender Male Female 6 6 6 6 12 12 Age Range Means 20 - 60 37 25 - 63 35 20 - 63 36.6 Ethnicity White Other 10 2 9 3 19 5 Occupation Musician; maintenance tech.;
director; business owner; manager;
waiter; self employed; computer operator; student; construction; Education 4-year degree Some college 8th-12thgrade 4 5 3 1 5 6 5 10 9 Religion Catholic Lutheran No religion 5 3 4 4 3 5 9 6 9
Table 4 Injurer of Each Participant in Both Groups
Experimental Group Alternative Treatment Group
Case One Mother Mother
Case Two Father Wife
Case Three Wife Mother
Case Four Mother Father
Case Five Father Husband
Case Six Wife Mother
Case Seven Mother Father
Case eight Father Father
Case nine Mother Wife
Case nineteen Wife Husband
Case twelve Father Wife
Design and Testing Procedure
The participants were randomly assigned to either the experimental group or the alternative treatment group. Each group of people received treatment, in a group intervention with the counselor. The experimental group was the forgiveness intervention. The alternative treatment group was based on some general substance quitting skills, typically introduced at the center. The interventions took twelve weeks. Participants met with the counselor once a week. Every session took two hours. The participants began their intervention immediately after pretest. The dependent variables are two different experiment
treatments. That is, the forgiveness treatment group received forgiveness intervention while the alternative treatment group began with the intervention for quitting the substance. The independent variables are forgiveness, depression; self- esteem; anxiety, anger, vulnerability to drug use. Two-way ANOVA were used to test the hypotheses on the six independent variables for the effects of treatments.
Before the participants had the intervention, they were administrated these six measures: (1) the Enright Forgiveness Inventory, (2) the Beck Depression Inventory-II, (3) the Coppersmith Self- Esteem Inventory, (4) the State-Trait Anxiety Inventory, (5) the Spielberger State-Trait Anger Scale, (6) the Lin Vulnerability to Drug Use Scale. All were given in random order.
The experimental group then began the forgiveness intervention and the alternative treatment group began with the intervention for quitting the substance. After the participant finished the intervention, the post-test was administered with the same instruments used at pre-test. The follow-up test was administered after four weeks later after the intervention had ended. The same dependent variables were employed. The point here was to examine any wash-out effects for the forgiveness group once treatment ceased.
Counselor
The counselor was a counselor who has over 10 years of experiences on counseling. The counselor has the experience to teach both the forgiveness program and the general substance abuse quitting program.
Instruments
Enright Forgiveness Inventory (EFI)
The EFI is a 60-item self-report measure of interpersonal forgiveness in which items are equally divided among six subscales: Positive and Negative Affect, Positive and Negative Behavior, and Positive and Negative Cognition. Score range from 60-360, with high scores representing high levels of forgiveness. In previous studies, internal consistency has been above .90 and test-retest reliability has range from .67 to .91; in addition, the scale’s validity has been documented ( Enright & Fitzgibbons, 2004; Subkoviak, Enright , Wu, & Gassin, 1995)
Beck Depression Inventory-II (BDI- II) The BDI-II is a 21 item self-report measure of symptoms and attitudes related to depression. Score range from 0-63, with scores indicating high levels of depression. Widely used in clinical research, the BDI-II has high construct validity and high reliability and is able to reflect changes in severity of depression over time (Beck, Steer, & Brown, 1996)
Coopersmith Self- Esteem Inventory(CSEI) The adult form of the CSEI is a 25-item self-report measure adapted from the school short form. This measure consists of true-false items evaluating attitudes toward the self in the following domains: general self, social, and home-parents. Raw scores are multiple by 4, generating a range of scores from 0-100. Higher scores indicate higher self-esteem. Validity and reliability have been well documented (Coopersmith, 1981)
State-Trait Anxiety Inventory(STAI) The STAI is composed of separate self-report questionnaires assessing two distinct types of anxiety: 20 state-anxiety items asses how an individual feels at a particular moment, and 20 trait-anxiety items assess how an individual generally feels. Each item is scored from 1-4, yielding a total subscale range 20-80. Reliability and validity are adequate (Spielberger, Gorsuch, & Lustene, 1970). In the current study, pretest internal consistency was .97.
Spielberger State-Trait Anger Inventory (SSTAEI) The SSTAEI asks participants to rate 10 items regarding state anger and 10 items regarding trait anger. Inventory range from 10-40 on each subscale. A high inventory reflects a high degree of anger. Internal consistency reliability has been reported as .88-.97, and the inventory’s validity has been established (Spielberger, 1996).
Lin Vulnerability To Drug Use Inventory (LVDUI) The vulnerability to drug use inventory was developed by Lin (2001). Because all participants were in residential treatment at the time of the study and because substance use was prohibited by the institution, we could not obtain reliable data on actual drug use by participants. A reasonable compromise was to construct a “vulnerability to drug use” inventory.
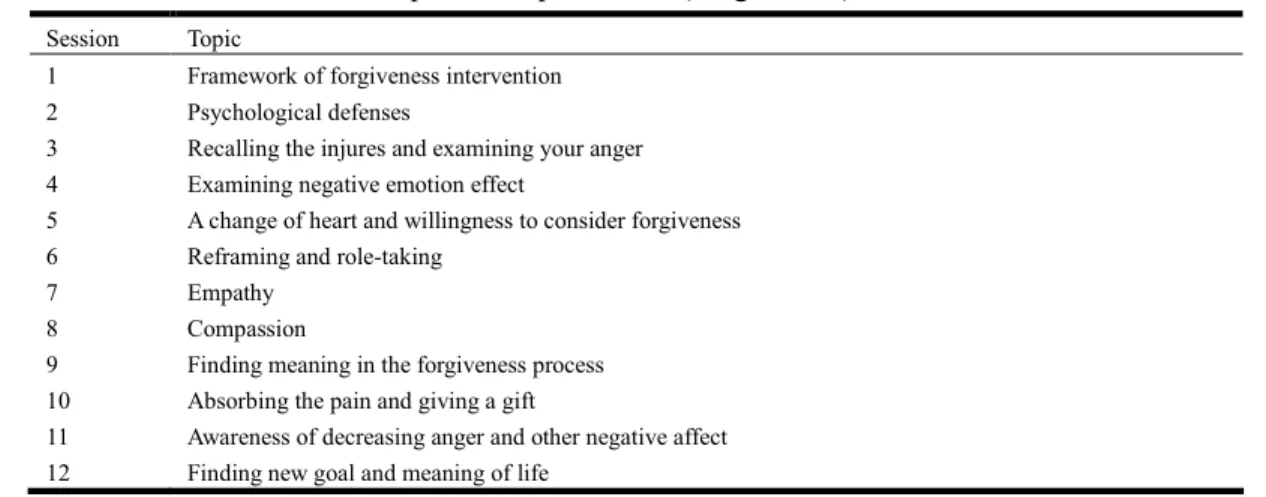
Experimental Group Intervention Procedure The forgiveness intervention (which the experimental group receives) were organized around the twenty psychological processes of forgiveness. As previously stated, each participant met with the counselor in the group. The goals of the phases of forgiveness and the units of forgiving and issues are described in Table5.
Table 5 Topics of Experimental (Forgiveness) Intervention
Session Topic
1 Framework of forgiveness intervention 2 Psychological defenses
3 Recalling the injures and examining your anger 4 Examining negative emotion effect
5 A change of heart and willingness to consider forgiveness 6 Reframing and role-taking
7 Empathy
8 Compassion
9 Finding meaning in the forgiveness process 10 Absorbing the pain and giving a gift
11 Awareness of decreasing anger and other negative affect 12 Finding new goal and meaning of life
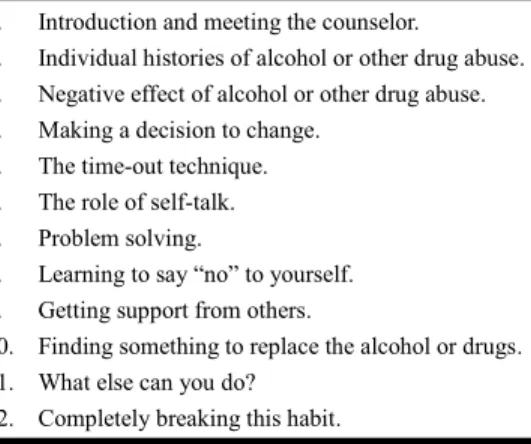
Alternative Treatment Group Intervention Procedure
The content of alternative treatment group intervention was a knowledge-based and support- based intervention, which focused on general substance abuse quitting skills. This intervention was organized around a 12-step quitting procedure, which is typically used at the center. The 12 steps of A substance abuse disorders were described in Table 6. This intervention helped the alternative treatment group participants to examine their individual need for substance abuse, decided whether they wanted to quit these habits, developed their own treatment plan, chose the best techniques, and created their own
success. This intervention contained 12 sessions.
Table 6 Topics of Alternative Treatment Group Intervention
1. Introduction and meeting the counselor.
2. Individual histories of alcohol or other drug abuse. 3. Negative effect of alcohol or other drug abuse. 4. Making a decision to change.
5. The time-out technique. 6. The role of self-talk. 7. Problem solving.
8. Learning to say “no” to yourself. 9. Getting support from others.
10. Finding something to replace the alcohol or drugs. 11. What else can you do?
12. Completely breaking this habit.
Treatment Fidelity
The researcher tape- recorded the sessions for participants and checked three sessions at random for three participants in the experimental and alternative treatment groups. The counselor followed the pre-determined protocol through the interventions..
Results
The participants of the current study was twenty-four: twelve in the experimental group (six female and six males) and twelve (six females and six males)in the alternative treatment group. Each participant completed pretests before being assigned to the experimental or alternative treatment group, and finished the posttest after he/she finished the intervention. The follow-up test was administrated after four weeks later after each participant finished the intervention.
Means and Standard Deviation for Each of the Dependent Variables of Each Group
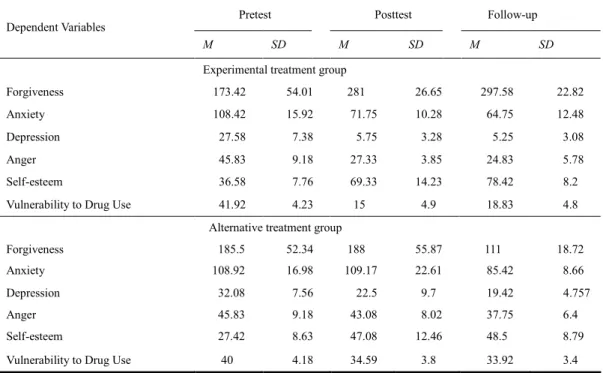
Means and stand deviation for all dependent variables at pretest, posttest, and follow-up test for the experimental and alternative treatment group are reported on the following page in Table 7.
Table 7 Means and Standard Deviation of Dependent Variables for Experimental Group
Pretest Posttest Follow-up
Dependent Variables
M SD M SD M SD
Experimental treatment group
Forgiveness 173.42 54.01 281 26.65 297.58 22.82
Anxiety 108.42 15.92 71.75 10.28 64.75 12.48
Depression 27.58 7.38 5.75 3.28 5.25 3.08
Anger 45.83 9.18 27.33 3.85 24.83 5.78
Self-esteem 36.58 7.76 69.33 14.23 78.42 8.20
Vulnerability to Drug Use 41.92 4.23 15 4.9 18.83 4.80
Alternative treatment group
Forgiveness 185.5 52.34 188 55.87 111 18.72
Anxiety 108.92 16.98 109.17 22.61 85.42 8.66
Depression 32.08 7.56 22.5 9.7 19.42 4.757
Anger 45.83 9.18 43.08 8.02 37.75 6.40
Self-esteem 27.42 8.63 47.08 12.46 48.5 8.79
Vulnerability to Drug Use 40 4.18 34.59 3.8 33.92 3.40
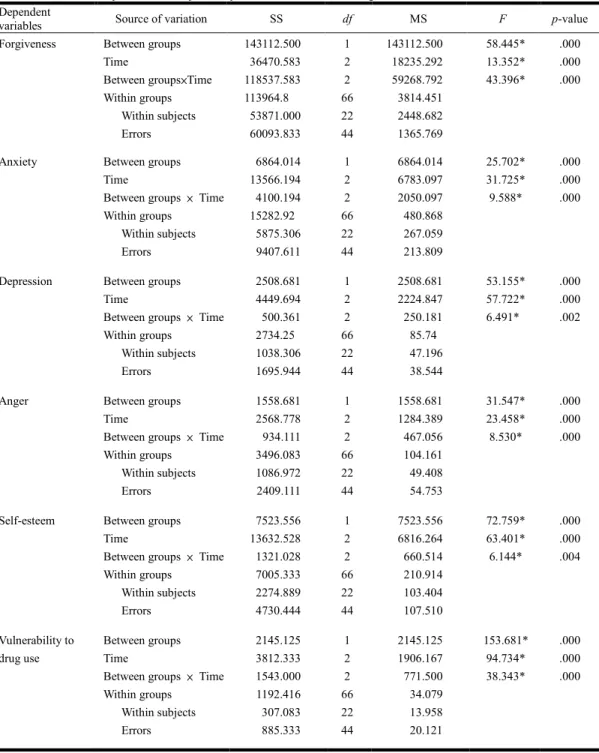
Two- way ANOVA were used to test the hypotheses on the six measures. The results are shown on Table 8.
Table 8 Summary of two-way Analysis of Variance of Dependent Variables
Dependent
variables Source of variation SS df MS F p-value
Forgiveness Between groups Time Between groups×Time Within groups Within subjects Errors 143112.500 36470.583 118537.583 113964.8 53871.000 60093.833 1 2 2 66 22 44 143112.500 18235.292 59268.792 3814.451 2448.682 1365.769 58.445* 13.352* 43.396* .000 .000 .000
Anxiety Between groups Time
Between groups × Time Within groups Within subjects Errors 6864.014 13566.194 4100.194 15282.92 5875.306 9407.611 1 2 2 66 22 44 6864.014 6783.097 2050.097 480.868 267.059 213.809 25.702* 31.725* 9.588* .000 .000 .000
Depression Between groups Time
Between groups × Time Within groups Within subjects Errors 2508.681 4449.694 500.361 2734.25 1038.306 1695.944 1 2 2 66 22 44 2508.681 2224.847 250.181 85.74 47.196 38.544 53.155* 57.722* 6.491* .000 .000 .002
Anger Between groups Time
Between groups × Time Within groups Within subjects Errors 1558.681 2568.778 934.111 3496.083 1086.972 2409.111 1 2 2 66 22 44 1558.681 1284.389 467.056 104.161 49.408 54.753 31.547* 23.458* 8.530* .000 .000 .000
Self-esteem Between groups Time
Between groups × Time Within groups Within subjects Errors 7523.556 13632.528 1321.028 7005.333 2274.889 4730.444 1 2 2 66 22 44 7523.556 6816.264 660.514 210.914 103.404 107.510 72.759* 63.401* 6.144* .000 .000 .004 Vulnerability to drug use Between groups Time
Between groups × Time Within groups Within subjects Errors 2145.125 3812.333 1543.000 1192.416 307.083 885.333 1 2 2 66 22 44 2145.125 1906.167 771.500 34.079 13.958 20.121 153.681* 94.734* 38.343* .000 .000 .000 *p < .005.
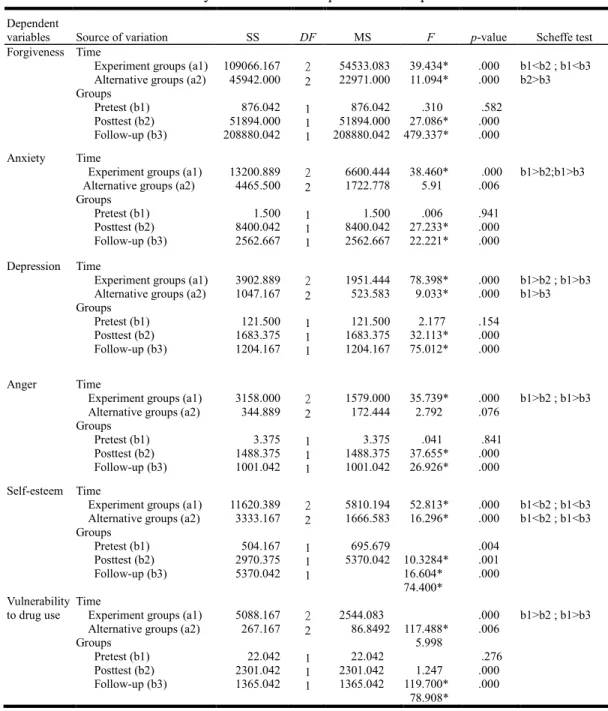
There were significant interactions on forgiveness, anxiety depression, anger, self-esteem and vulnerability to drug use variables on Table8. The Scheffe test is to understand the simple main effects. The result was shown on Table 9.
Table 9 Summary of Posteriori Comparisons of Dependent Variables
Dependent
variables Source of variation SS DF MS F p-value Scheffe test
Forgiveness Time
Experiment groups (a1) Alternative groups (a2) Groups Pretest (b1) Posttest (b2) Follow-up (b3) 109066.167 45942.000 876.042 51894.000 208880.042 2 2 1 1 1 54533.083 22971.000 876.042 51894.000 208880.042 39.434* 11.094* .310 27.086* 479.337* .000 .000 .582 .000 .000 b1<b2 ; b1<b3 b2>b3 Anxiety Time
Experiment groups (a1) Alternative groups (a2) Groups Pretest (b1) Posttest (b2) Follow-up (b3) 13200.889 4465.500 1.500 8400.042 2562.667 2 2 1 1 1 6600.444 1722.778 1.500 8400.042 2562.667 38.460* 5.91 .006 27.233* 22.221* .000 .006 .941 .000 .000 b1>b2;b1>b3 Depression Time
Experiment groups (a1) Alternative groups (a2) Groups Pretest (b1) Posttest (b2) Follow-up (b3) 3902.889 1047.167 121.500 1683.375 1204.167 2 2 1 1 1 1951.444 523.583 121.500 1683.375 1204.167 78.398* 9.033* 2.177 32.113* 75.012* .000 .000 .154 .000 .000 b1>b2 ; b1>b3 b1>b3 Anger Time
Experiment groups (a1) Alternative groups (a2) Groups Pretest (b1) Posttest (b2) Follow-up (b3) 3158.000 344.889 3.375 1488.375 1001.042 2 2 1 1 1 1579.000 172.444 3.375 1488.375 1001.042 35.739* 2.792 .041 37.655* 26.926* .000 .076 .841 .000 .000 b1>b2 ; b1>b3 Self-esteem Time
Experiment groups (a1) Alternative groups (a2) Groups Pretest (b1) Posttest (b2) Follow-up (b3) 11620.389 3333.167 504.167 2970.375 5370.042 2 2 1 1 1 5810.194 1666.583 695.679 5370.042 52.813* 16.296* 10.3284* 16.604* 74.400* .000 .000 .004 .001 .000 b1<b2 ; b1<b3 b1<b2 ; b1<b3 Vulnerability to drug use Time
Experiment groups (a1) Alternative groups (a2) Groups Pretest (b1) Posttest (b2) Follow-up (b3) 5088.167 267.167 22.042 2301.042 1365.042 2 2 1 1 1 2544.083 86.8492 22.042 2301.042 1365.042 117.488* 5.998 1.247 119.700* 78.908* .000 .006 .276 .000 .000 b1>b2 ; b1>b3 *p < .005.
The Treatment Effects on Forgiveness
The first comparison for forgiveness between the pretest and the posttest for the forgiveness intervention group showed statistical significance. The experimental group also showed a significantly greater improvement in forgiveness from pretest to to follow-up. The alternative treatment group did not get any improvement. It showed that the forgiveness intervention was successful in its goal of leading the participants toward forgiveness. Moreover, It showed that the forgiveness intervention was not only successful in leading the participants toward forgiveness but also been in successfully maintaining this effect for at least four weeks.
The Treatment Effects on Anxiety
The next comparison was the composite anxiety scale. The experimental group showed a greater reduction in anxiety from pretest to posttest. The alternative treatment had no differences from pretest to posttest. This illustrates that there was a greater reduction in anxiety for the experimental group from pretest to posttest compared with the alternative treatment group in the short run. In addition, the experimental group also showed a greater improvement from pretest to follow-up. This illustrates that there was a significant reduction in anxiety for long-run.
The Treatment Effects on Depression
The third comparison for depression showed statistical significance. The statistical result showed that the experimental group reduced significantly in depression compared with the pretest and posttest. In the follow-up, the statistical result showed that the experimental group and alternative treatment group reduced significantly in depression after four weeks post-intervention. The researcher wanted to know if both treatments reduced the participants' depression. This indicated that both groups, after four weeks, seemed to reduce in depression.
The Treatment Effects on Anger
The anger scale examined in fourth comparison showed statistical significance from pretest to posttest for the experimental group. This shows that there was significant change in a positive direction in anger for the experimental group after participants received the forgiveness intervention than did in the alternative treatment group. The anger scale examined in the follow-up did show a statistical significance from pretest to follow-up test for the experimental group compared. There were no difference between the alternative treatment group in the score.
The Treatment Effects on Self-esteem
Self-esteem was the next variable examined. The comparison between the pretest and posttest for both groups indicated a significant difference in self-esteem. This showed that forgiveness intervention and the alternative treatment group improved the participants' self-esteem.The comparison between the pretest and follow-up for the forgiveness intervention and alternative treatment group indicated a significant gain in self-esteem. This showed that both interventions has a greater long-term effect in improving the participants' self-esteem.
The Treatment Effects on Vulnerability to Drug Use
The last comparison for vulnerability to drug use also showed statistical significance between the pretest and the posttest in the forgiveness intervention group. The experimental group significantly
improved in refraining from drug use, compared with the alternative treatment group. The results in the follow-up showed that the experimental group had a statistically significant improvement from pretest to follow-up test. The vulnerability to drug use variables was sustained four weeks later in that the forgiveness intervention participants engaged in drug use to a lessen extent
Summary
As hypothesized expectation, all the dependent variables for the experimental group showed significantly greater change from pretest to posttest. This indicates that the forgiveness intervention had a greater effect to improve participants' psychological functioning than did the alternative treatment from pretest to posttest subscales. In addition, all the dependent variables showed that the experimental group improved their psychological functioning and lowered vulnerability to drug use from pretest and from pretest to follow-up. The results indicate that there is no “washout effect” for the participants in the experimental group. The only exception is in self-esteem, where both groups experienced a signification improvement. Forgiveness intervention is a useful tool in leading to the goal of healthy psychological functioning in both short and long-term improvement.
Correlations between Forgiveness and the Other Five Dependent Variables
The Pearson product-moment correlations were used to determine if there were any relationships between forgiveness and the other five dependent variables at posttest for experimental and alternative treatment groups. The result was shown as follows: Depression (-.614*), Anger (-.404*), Anxiety (-.254*), Self-esteem (.460*), Vulnerability to Drug Use (-.670*), p < .05.
Discussion
Conclusion of the Results
As Hester, and Miller (1995) pointed out that substance abuse is one of the most common means abusers use to reduce anxiety, anger, depression and cope with stressful situations. Leshner (1999) stated that understanding the patient's motivation to use drugs and alcohol is critical. If people use substance to self-regulate their emotions, then an effective approach to addiction treatment to attend to is individuals' emotional of needs, not just his/ her drug/ alcohol use.
Therefore the goal of this study was to help substance abusers to develop the virtue of forgiveness and withdraw the revenge or resentment to the injurer, then lead the abusers to decrease negative psychological emotions (such as anger, anxiety, depression), and increase their positive psychological functioning (for instances, self-esteem), and reduce their vulnerability to alcohol or drug use. Thus, the major predications of this study were the participants in the forgiveness treatment group would become more forgiving of their injurer than the alternative treatment group, and as result of participants' emotional health would improve in the areas hypothesized.
The findings of the present research show that the forgiveness intervention can lead participants to relieve negative emotions, and increase positive emotions, and the effect of the intervention was
maintained four weeks after the intervention. The majority of the hypotheses of this study were supported as expected.
Important Findings of This Study
Providing Specialized Intervention (Forgiveness Intervention) to Solve Unique Needs of the Clients. One of the important findings from this study is that providing specialized intervention to solve unique needs of individual clients is critical. People differ in their reasons for using alcohol and drugs. In this study, the addicted had emotional pain caused by interpersonal offense. Forgiveness is an effective tool in improving psychological health of substance abusers who had been deeply hurt by interpersonal offense.
"Group Treatment" and " Longer Time" May be Efficient Factors to Produce Larger Effect Sizes.Another potentially important finding is "group treatment" and " longer time" is efficient factors to produce larger effect sizes. Enright and Fitzgibbons (2004) stated that the longer the intervention, at least to a point, the more effective the treatment. Their tentative opinion is that at least 10-12 weeks with group treatment is necessary to induce change in the outcome. A meta-analysis done on effect sizes of forgiveness interventions by Baskin and Enright also supports this explanation (cited in Ostermdorf, 1999). They pointed out that longer interventions and group interventions yield larger effect sizes when compared to shorter interventions and group interventions on forgiveness.
The difference between individual and group intervention is the participants of the group intervention are more likely to get other persons’ feedback, direct advice and direct empathy from the facilitator. Hester and Miller (1995) pointed out that certain keys for change of the addicted, including group member’s feedback, advice, empathy, responsibility and self-efficacy. Group treatment could provide individual feedback, satisfy the addicted needs, and give clear and direct advice, which can trigger the addict's motivation to change.
The Forgiveness Manual may be Playing a Factor in the Significantly Outcomes.Next, the forgiveness manual may be playing a factor in the significant outcomes. As Freedman (1994) observed, having something concrete to take home and read might be helpful for the participants in understanding and practicing forgiveness in their daily life. Thus, having an appropriate working manual may be an important factor to bring significant outcome.
Forgiveness Intervention is Effective to Relieve Negative Emotion (Anger, Anxiety, Depression, Vulnerability to Substance use) in the Short and Long-term Next, the forgiveness manual may be playing a factor in the significant outcomes. As Freedman (1994) observed, having something concrete to take home and read might be helpful for the participants in understanding and practicing forgiveness in their daily life.
The anxiety results also provide scientific evidence that forgiveness intervention is an effective tool to heal psychological pain and improve emotional functioning. The result indicates that the forgiveness intervention is effective in significantly reducing anxiety in the short and long-term. Forgiveness might decrease anxiety directly as a result of the resolution of anger, especially in clients whose anxiety is caused by the fear of their unconscious anger. In this study, participants after receiving forgiveness intervention significantly decreased their anger and increased their safety and trust in their lives.
The results also showed a significant reduction favoring the forgiveness intervention compared to the alternative treatment group in depression from pretest to follow-up. The participants are between
moderately depressed and severely depressed. After the intervention, the participants decreased their depression to non-depressed. The participants also maintain their non-depressed status for at least four weeks. The participants in the alternative treatment group also decreased in depression, but they still were moderately depressed as based on clinically established cut-off. The result indicates that the forgiveness intervention worked better than the alternative treatment group. Depression is an important issue in those with substance abuse. Alcoholism, in particular, is strongly associated with depression (Abraham & Fava, 1999). Depression is also a major predictor of relapse (Pickens, Hatsukami, Spicer, & Svikis, 1985). The effective treatment of depression might be responsible, at least in part, for the statistically significant reduction in reported vulnerability to substance use by the forgiveness group.
The Vulnerability to Drug Use was the last variable examined. The vulnerability to drug use scale is the most important evidence indicating how the forgiveness intervention changes the drug abuser. Data from the study show that there was a significant difference between the experimental and alternative treatment group. The experimental group significantly decreased in their sense of their own vulnerability to drug abuse compared with the alternative treatment group. The effect also was maintained for at least four weeks. The result is consistent with the other five measures. After participation in the forgiveness intervention, the experimental group showed a sober pattern. This indicates that the forgiveness intervention is effective in treating the substance abusers whose addict problem is related to a deep interpersonal hurt. Forgiveness intervention is not only to enhance the abuser's psychological health, but also to help the addicted to become and remain sober. The more positive feelings the participants experienced after the intervention are important factors to reduce the participants' sense of their own vulnerability to drug and alcohol abuse. When there is a change in forgiveness, there is an improvement in emotion functioning, which can affect behaviors.
Forgiveness Intervention is Effective in Improving Positive Affect ( Self-esteem and forgiveness) in the Short and Long-term Self-esteem was another important variable the researcher examined. Hill, Shen, Locke, and Lowers (2000) examined psychological risk factors to predict substance abuse. They found that the level of self-esteem is one factor to predict alcohol and drug abuse. Negative self-esteem is positively related to substance abuse. Negative self-esteem is positively related to substance abuse. Daderman and Lidberg (1999) also suggested that self-esteem is an important key related to alcohol and drug abuse. Drug abusers usually use alcohol and drugs to increase the feeling of power and self-esteem. The paradox, as the researchers pointed out, is that if the substance abusers cab improve their self-esteem, they could solve their substance problems.
Participants in the forgiveness intervention group significantly improved their self-esteem relative to the alternative treatment group at the posttest and follow-up. When substance abusers forgive their injurer, their feelings about themselves up to four weeks after the intervention.
In this study, participants in the forgiveness intervention group and alternative treatment group significantly improved their self-esteem at the posttest and follow-up. When substance abusers forgive their injurer, their feelings about themselves improve. Furthermore, the experimental group participants continued to feel good about themselves up to four weeks after the intervention. This research provides a new and effective treatment intervention to improve self-esteem. Thus, forgiveness intervention has shown to be an effective in improving psychological health.
Drug and alcohol abuse is a very serious problem in modern society. As Daley and Raskin (1991), from data of the National Institute of Mental Health's Epidemiological Catchment Area Survey of 20,000 adults, indicated that 13.7% of adults meet current lifetime criteria for substance abuse. It is necessary to validate the current findings by means of replication. An initial follow-up to this study should involve replication to illustrate the effective of forgiveness intervention, time of active forgiveness intervention, and therapist.
In addition to evaluating short-term effects, further research should also evaluate longer long-term effects, such as a one-year follow-up.
Although this forgiveness intervention have been applied on other population, and has been found to be significantly beneficial to psychological functioning, such as female incest survivors, parentally love-deprived college students, male suffered post-abortion hurt, elderly females, and adult children of alcoholics, there are numerous population that have been deeply interpersonal hurt who have not been treated by forgiveness intervention. Future research could investigate other populations to assessing the applicability of forgiveness intervention effects, such as battered women, people suffering from posttraumatic stress, victims of crimes, victims of domestic violence, and victims of divorce.
Limitation and Implications for Practice
The present study used the group form of forgiveness intervention. In the group treatment, the individual and special personal needs are harder than individual counseling did. However, many researchers also suggest the most effective therapy for alcohol and drug abusers are to combine individual and group therapy(Fiorentine, 1998) In the future, the researcher could test the effects of individual and group therapy. In addition, the small sample size is one of the current research limitations. To increase the sample could give strong significant effects of forgiveness.
The findings of the present study show that forgiveness intervention can be psychological beneficial for substance abusers who have been hurt by interpersonal offenses. The data suggest that the benefits include increasing higher levels of psychological functioning: higher levels of forgiveness, self-esteem, lower levels of depression, anger, anxiety, and vulnerability to drug use. This present, scientific study validated the 20-unit forgiveness model is a new venue, with those experiencing drug and alcohol abuse.
Scientific knowledge about substance abuse has grown rapidly during the last decades. As important development is creating different intervention approaches to meet the heterogeneous characteristic of substance abusers (Tucker, Donovan, & Marlatt, 1999). The working manual (Enright, 2001) provides a new intervention approach for professional psychotherapists and other service providers in drug and alcohol rehabilitation. This manual seems to be psychologically therapeutic for drug and alcohol abusers who have been hurt by interpersonal offense. As such, it provides another psychotherapeutic choice for professionals to help this population to resolve their psychological problems and recover from substance abuse.
References
Abraham, H. D., & Fava, M. (1999). Order of onset of substance abuse and depression in a sample of depressed outpatients. Comprehensive Psychiatry, 40(1), 44-50.
Alcoholic Anomous. (1976). The big book. NY: Alcoholics World Services.
Al-Mabuk, R. H., & Enright, R. D. (1995). Forgive with parentally love-deprived college students.
Journal of Moral Education, 24, 427-444.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck Depression Inventory manual. San Antonio, TX: Psychological Corporation.
Clancy, J. (Ed.) (1996). Anger and addict: Breaking the relapse cycle. A teaching guide for professionals. Madison, CT: Psychosocial Press/International Universities Press.
Clark, D. B., & Winters, K. C. (2002). Measuring risk and outcomes in substance use disorders prevention research. Journal of Consulting and Clinical Psychology, 70, 1207-1223.
Colliver, J. D., & Malin, H. (1986). State and national trends in alcohol related mortality. Alcohol Health
and Research World, 10(3), 60-64.
Coopersmith, S. (Ed.) (1981). Manual of adult self-esteem scale. Palo Alto, CA: Consulting Psychologists Press.
Coyle, C. T., & Enright, R. D. (1997). Forgiveness intervention with post-abortion men. Journal of
Consulting and Clinical Psychology, 65(6), 1042-1046.
Daderman, A., & Lidberg, L. (1999). Flunitrazepam abuse in combination with alchol causes premeditated grievous violence in male juvenile offenders. Journal of the American Academy of
psychiatry and the Law, 27, 83-89.
Daley, D. C., & Raskin, M. S. (1991). Relapse prevention and treatment effectiveness studies. In D. C. Daley & M. S. Raskin (Eds.). (1991). Treating the chemically dependent and their families. (pp. 128-171). Newbury Park, CA: Sage.
Dodge, K., & Potocky, M. (2000). Female substance abuse: Characteristics and correlates in a sample of inpatient clients. Journal of Substance Abuse Treatment, 18(1), 59-64.
Enright, R. D. (2001). Forgiveness is a choice. Washington, DC: APA Books.
Enright, R. D., & Fitzgibbons, R. P. (2004). Helping clients forgive: An empirical guide for resolving
Enright, R. D., Gassin, E. A., & Wu, C. (1992). Forgiveness: A developmental view. Journal of Moral
Education, 21, 100-114.
Enright, R. D., & The Human Development Study Group (1991). The moral development of forgiveness. In W. Kurtines and J. Gewirtz (Eds.), Moral behavior and development: Vol. 1. Theorg (pp.123-152). Hillsdale, NJ: Erlbaum.
Fields. R. (1992). Drug and alcohol in perspective. Washington: W. C. Brown.
Fiorentine, R. (1998). Effective drug treatment: Testing the distal needs hypothesis. Journal of Substance
Abuse Treatment, 15, 281-289.
Fischer, E. H., & Goethe, J. W. (1998). Anxiety and alcohol abuse in patients in treatment for depression.
American Journal of Drug and Alcohol Abuse, 24(3), 453-463.
Forgays, D., Richards, J. C., Fgays, D. G., & Sujan, S. (1999). Examination of the AHA! Illness relation in male and female university students from Australia, India, and the United States. International
Journal of Behavioral Medicine, 6(1), 64-77.
Freedman, S. R. (1994). Forgiveness as an educational intervention goal with incest survivors. Unpublished doctoral dissertation, University of Wisconsin, Madison.
Fitzgibbons, R. P. (1998). Anger and the healing Power of forgiveness: A psychiatrist’s view. In R. Enright & J. North (Eds.), Exploring forgiveness (p.6374). Madison: University of Wisconsin Press.
Hebl, J. H., & Enright, R. D. (1993). Forgiveness as a psychotherapeutic goal with elderly females.
Psychotherapy, 30, 658-667.
Hester, R. K., & Miller, W. R, (Eds.). (1995). Handbook of alcoholism treatment approaches: Effective
alternatives (2nd ed.). Needham Heights, MA.
Hill, S. Y., Sheen, S., Locke, J., & Lowers, L. (2000). Developmental changes in postural sway in children at high and low risk for developing alcohol-related disorders: Biological Psychiatry,
47(6), 501-511.
Holmgren, M. (1995). Behandling av ihallande syn- och hoerselhallucinationer has en 23-arig kvinna--en fallstudie. Treatment of a 23-year-old woman's chronic visual and auditory hallucinations: A case study. Scandinavian Journal of Behaviour Therapy, 24(2-3), 99-105.
Huizinga, D., Loeber, R., & Thornberry, T. (1994). Urban development and substance abuse. In Program of research Office of Juvenile Justice and Delinquence Prevention, U. S. Department of Justice. Kingree, J. B., Thompson, M. P., & Kaslow, N. J. (1999). Risk factors for suicide attempts among
Kushner, M. G., Sher, K. J., & Erickson, D. J. (1999). Prospective analysis of the relation between DSM-III anxiety disorders and alcohol use disorders. American Journal of Psychiatry,
156(5), 723-732.
Leiker, M., & Hailey, B. J. (1988). A link between hostility and disease: Poor health habits? Behavioral
Medicine, 14(3), 129-133.
Leshner, A. (1999). Science-based views of drug addiction and its treatment. Journal of The American
Medical-Association, 282(14), 314-1316.
Lester, D. (1995). The association between alcohol consumption and suicide and homicide rates: A study of 13 nations. Alcohol and Alcoholism, 30(4), 465-468.
Lin, W. F. (2001). Forgiveness as an intervention goal within a drug rehabilitation center. Unpublished doctoral dissertation University of Wisconsin-Madison.
Lin, W. N. (1998). Forgiveness as an intervention goal for late adolescents with insecure attachment in
Taiwan. Unpublished doctoral dissertation. University of Wisconsin- Madison.
MacQueen, A. R. (1999). Spiritual dimensions of alcohol and other drug problems. Addiction, 94(3), 436. Marlatt, G. A. (1985). Relapse prevention: Theoretical rationale and overview of model. In G. A. Marlatt
& J. R. Gordon (Eds.), Relapse prevention (pp. 3-67). NY: Guilford Press.
McCord, J. (1992). Another time, another drug. In M. D. Glantz, & R. W. Pickens, (Eds), Vulnerability to
drug abuse (pp.473-489). Washington, DC: American Psychological Association.
National Institute of Alcohol Abuse and Alcoholism (2000). Seventh special report to the U.S. Congress
on alcohol and health. Rockville, MD: Author.
Ostermdorf, C. (1999). Effects of a Forgiveness Education Intervention with Adult Children of Alcoholics. Unpublished doctoral Dissertation. University of Wisconsin- Madison.
Patten, S. B., & Charney, D. A. (1998). Alcohol consumption and major depression in the Canadian population. Canadian Journal of Psychiatry, 43(5), 502-506.
Pickens, R. W., Hatsukami, D. K., Spicer, J. W., & Svikis, D. S. (1985). Relapse by alcohol abusers. Alcoholism. Journal and Experimental Research, 9(3), 244-247.
Ripley, J. S., & Worthington, E. L. (2002). Hope-focused and forgiveness-base group interventions to promote marital enrichment. Journal of Counseling and Development, 80, 452-463.
Spielberger, C. D. (1983). State-Trait Anxiety Inventory: A comprehensive bibliography. Palo Alto, CA: Consulting Psychologists Press.
Spielberger, C. D. (1996). State-Trait Anger expression Inventory Manual. Odessa, FL: Psychological Assessment Resources.
Spielberger, C. D, Gorsuch, R., & Lustene, R. E. (1970). Mamual for the State-Trait Anxiety Inventory
(Self-valuative Questionnaire). Palo Alto, CA: Counseling Psychologists Press.
Straussner, S. L. A. (Ed.). (1993). Clinical work with substance-abusing clients. New York, NY, USA: The Guilford Press.
Subkoviak, M. J., Enright, R. D., Wu, C. R., & Gassin, E. A. (1995). Measuring interpersonal forgiveness in late adolescence and middle adulthood. Journal of Adolescence, 18(6), 641-655.
Tivis, L. J., Parsons, O. A., & Nixon, S. J. (1998). Anger in an inpatient treatment sample of chronic alcoholics. Alcoholism: Clinical and Experimental Research, 22(4), 902-907.
Thomas, S. P. (Ed.). (1993). Women and anger. NY: Springer.
Tucker, J. A., Donovan, D. M., & Marlatt, G. A. (1999). Hanging addictive behavior: Bridging clinical
and public health strategies. New York, NY: The Guilford Press.
U. S. Department of Health and Human Research. (1990). Alcohol and health. National Ibstitute on Alcohol and Alcoholism.
Wanberg, K. W., & Milkman, H. B. (1998). Criminal conduct and substance abuse treatment: Strategies for self-improvement and change: The provider’s guide, Thousand Oaks, CA: Sage Publications. Williams, R., & Williams, V. (1993). Anger Kills. NY: Times Books.
Wood, H. P., & Duffy, E. L. (1996). Psychological factors in alcoholic women. American Journal of
Psychiatry, 123(3), 341-345. 收 稿 日 期:2008 年 06 月 09 日 一稿修訂日期:2008 年 12 月 03 日 二稿修訂日期:2009 年 02 月 02 日 三稿修訂日期:2009 年 04 月 01 日 接受刊登日期:2009 年 04 月 02 日
國 立 臺 灣 師 範 大 學 教 育 心 理 與 輔 導 學 系 教育心理學報 ,民 99,41 卷,4 期,859-886 頁