Prognostic Significance of Multiple Molecular Markers for
Patients With Stage II Colorectal Cancer Undergoing
Curative Resection
Yih-Huei Uen, MD,* Shiu-Ru Lin, PhD,† Deng-Chyang Wu, MD, PhD,‡§ Yu-Chung Su, MD,‡§
Jeng-Yih Wu, MD,‡ Tian-Lu Cheng, PhD,¶ Chin-Wen Chi, MD,
储 and Jaw-Yuan Wang, MD, PhD§**
Objective: The aim of this study was to determine whether our constructed high-sensitivity colorimetric membrane-array method could detect circulating tumor cells (CTCs) in the peripheral blood of stage II colorectal cancer (CRC) patients and so identify a subgroup of patients who are at high risk for relapse.
Summary Background Data: Adjuvant chemotherapy is not rou-tinely recommended in patients diagnosed with UICC stage II CRC. However, up to 30% of patients with stage II disease relapse within 5 years of surgery from recurrent or metastatic disease. The identi-fication of reliable prognostic factors for high-risk stage II CRC patients is imperative.
Methods: Membrane-arrays consisting of a panel of mRNA mark-ers that included human telomerase revmark-erse transcription (hTERT), cytokeratin-19 (CK-19), cytokeratin-20 (CK-20), and carcinoembry-onic antigen (CEA) mRNA were used to detect CTCs in the peripheral blood of 194 stage II CRC patients who underwent potentially curative (R0) resection between January 2002 and De-cember 2005. Digoxigenin (DIG)-labeled cDNA were amplified by RT-PCR from the peripheral blood samples, which were then hybridized to the membrane-array. All patients were followed up regularly, and their outcomes were investigated completely. Results: Overall, 53 of 194 (27.3%) stage II patients were detected with the expression of all 4 mRNA markers using the membrane-array method. After a median follow up of 40 months, 56 of 194 (28.9%) developed recurrence/metastases postoperatively. Univari-ately, postoperative relapse was significantly correlated with the depth of invasion (P⬍ 0.001), the presence of vascular invasion (P ⬍ 0.001), the presence of perineural invasion (P⫽ 0.048), the
expres-sion of all 4 mRNA markers (P ⬍ 0.001), and the number of examined lymph nodes (P⫽ 0.031). Meanwhile, using a multivar-iate logistic regression analysis, T4 depth of tumor invasion (P⫽ 0.013), the presence of vascular invasion (P ⫽ 0.032), and the expression of all 4 mRNA markers (P⬍ 0.001) were demonstrated to be independent predictors for postoperative relapse. Combination of the depth of tumor invasion, vascular invasion, and all 4 mRNA markers as predictors of postoperative relapse showed that pa-tients with any 1 positive predictor had a hazard ratio of about 27-fold to develop postoperative relapse (P⬍ 0.001; 95% CI ⫽ 11.42– 64.40). The interval between the detection of all 4 positive molecular markers and subsequently developed postoperative relapse ranged from 4 to 10 months (median: 7 months). Further-more, the expression of all 4 mRNA markers in all stage II CRC patients, or either stage II colon or rectal cancer patients were strongly correlated with poorer relapse-free survival rates by survival analyses (all P⬍ 0.001).
Conclusions: The pilot study suggests that the constructed mem-brane-array method for the detection of CTCs is a potential auxiliary tool to conventional clinicopathological variables for the prediction of postoperative relapse in stage II CRC patients who have under-gone curative resection.
(Ann Surg 2007;246: 1040 –1046)
C
olorectal cancer (CRC) is one of the most frequent malignancies and is also the third major cause of cancer-related death in Taiwan, with over 8000 new cases and 4000 deaths per year (http://www.doh.gov.tw/statistic/index.htm; accessed in January 2007). Adjuvant chemotherapy with 5-fluorouracil (FU)-based therapy has now become an ac-cepted standard of care for patients with International Union Against Cancer (UICC) stage III colon cancer since the early 1990s, and has resulted in a 30% to 40% decrease in relapse and mortality rates versus treatment with surgery alone.1–3 More recently, the addition of oxaliplatin to 5-FU-based therapy has further improved patient outcomes, thus estab-lishing this combination as a new standard of care.4,5Patientswith stage II CRC are generally considered to be at low risk for developing postoperative relapse; therefore, patients with CRC in this stage are not recommended to undergo routine
From the *Division of General Surgery, Department of Surgery, Chi Mei Foundation Medical Center, Taipei Medical University, Taipei, Taiwan; †Graduate Institute of Medical Genetics, College of Medicine, ‡Depart-ment of Internal Medicine; §Faculty of Medicine; ¶Faculty of Biomed-ical Science and Environmental Biology, College of Life Science, Kaohsiung Medical University, Kaohsiung; 㛳Division of General Sur-gery, Department of Medical Research and Education, Veterans General Hospital-Taipei, Taipei; and **Department of Surgery, Kaohsiung Med-ical University Hospital, Kaohsiung, Taiwan.
Supported by a grant from the Chi Mei Medical Center Foundation (CMYM9503).
Reprints: Jaw-Yuan Wang, MD, PhD, Department of Surgery, Kaohsiung Medical University Hospital, 100 Tzyou 1st Road, Kaohsiung 807, Taiwan. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & Wilkins ISSN: 0003-4932/07/24606-1040
adjuvant chemotherapy.3,6 – 8However, about 25% to 30% of
CRC patients with stage II disease are at high risk for postoperative relapse. Indeed, the clinical outcome of patients with high-risk stage II disease is similar to that of patients with stage III disease.
With regard to stage II CRC, a wide variety of potential clinical and pathologic risk factors for recurrence have been investigated. The most important factors for predicting the risk of recurrence are emergency presentation (bowel perfo-ration or obstruction), poorly differentiated tumor (histologic grade), depth of tumor invasion and adjacent organ involve-ment (T4), extramural venous invasion, and peritoneal in-volvement.9,10Recently, we have also demonstrated that the
depth of invasion, the presence of vascular invasion and number of examined lymph nodes may prominently affect the prognosis of patients with stage II CRC.11 It is therefore of high importance to define reliable prognostic factors for this patient group to help identify high-risk patients (for tumor relapse) who might benefit from adjuvant therapeutic regimes.12,13
With recent developments in molecular technology, the use of polymerase chain reaction (PCR), reverse transcrip-tion-PCR (RT-PCR), or real-time quantitative-CR (Q-PCR) assays now permit sensitive detection of circulating tumor cells (CTCs) in peripheral blood. Accumulated reports have described the detection of CTCs in the peripheral blood of CRC patients, which has important prognostic and therapeu-tic implications.14 –18 Our recently developed membrane ar-ray-based multimarker assay can detect CTCs in the periph-eral blood of CRC patients; this is found to be a rational approach for the surveillance of postoperative CRC pa-tients.18 –21 Though many mRNA (messenger RNA) molec-ular markers have been evaluated as putative prognostic markers in CRC patients, no information about the multima-rker assay关human telomerase reverse transcription (hTERT), cytokeratin-19 (CK-19), cytokeratin-20 (CK-20), and carci-noembryonic antigen (CEA)兴 in the detection of CTCs as a prognostic tool for stage II CRC patients has ever been obtained. The aim of this study was to analyze stage II CRC patients who have undergone curative resection by a panel of molecular markers using a constructed membrane-array method and evaluate their significance in postoperative surveillance.
PATIENTS AND METHODS Patients and Samples
Included in this prospective study were 194 stage II CRC patients admitted to the Department of Surgery of Kaohsiung Medical University Hospital for elective sur-gery between January 2002 and December 2005. Patients with other malignant disease in their medical history were excluded. Circulating tumor cells in peripheral blood of these 194 patients were detected using our constructed membrane-array method. All 194 patients underwent rad-ical resection for the primary lesion. Radrad-ical (R0) resec-tion is defined as any gross residual tumor that did not remain in the surgical bed, and the surgical resection margin is pathologically negative for tumor invasion.
Post-operative surveillance consisted of medical history, phys-ical examination, and laboratory studies, including serum CEA levels every 3 months. Abdominal ultrasonography or computed tomography was performed every 6 months, and chest radiography and total colonoscopy were per-formed once a year. Patients were followed up at 3-monthly intervals for 2 years and 6-monthly intervals thereafter; median follow up was 40 months (range, 14 – 62 months). The development of new recurrent or metastatic lesions after operation was defined as a postoperative relapse. The type of postoperative relapse was designated as local recurrence (tumor growth restricted to the anasto-mosis or the region of primary operation) or distant me-tastases (distant meme-tastases or diffuse peritoneal seeding). A 4-mL sample of peripheral blood was obtained from each CRC patient postoperatively (at least 1 week after surgery) for total RNA isolation. No additional blood samples were drawn for the detection of CTCs. To prevent contamination of epithelial cells, peripheral blood samples were obtained through a catheter inserted into a peripheral vessel, and the first 5 mL of blood were discarded. Written informed consent was obtained from each subject and/or guardian. Sample acquisition and subsequent use were also
TABLE 1. Clinicopathologic Characteristics of 194 Stage II Colorectal Cancer Patients
Variables No. (%)
Gender
Male/female 105 (54.1)/89 (45.9)
Age (yr)
⬍65/ⱖ65 84 (43.3)/110 (56.7)
Maximum tumor size (cm)
⬍5/ⱖ5 100 (51.5)/94 (48.5)
Tumor location
Colon/rectum 128 (66)/66 (34)
Depth of tumor invasion
T3/T4 185 (95.4)/9 (4.6) Vascular invasion Yes/no 52 (26.8)/142 (73.2) Perineural invasion Yes/no 66 (34)/128 (66) Histology WD/MD/PD 17 (8.8)/157 (80.9)/20 (10.3) Type of tumor Mucinous carcinoma Yes/no 10 (5.2)/184 (94.8)
Four molecular markers
Yes/no 53 (27.3)/141 (72.7)
Number of examined lymph nodes
⬍12 nodes/ⱖ12 nodes 119 (61.3)/75 (38.7) Preoperative colonic obstruction/perforation Yes/no 10 (5.2)/184 (94.8) Adjuvant chemotherapy Yes/no 125 (64.4)/69 (35.6)
WD indicates well differentiated; MD, moderately differentiated; PD, poorly differentiated.
approved by the hospital’s institutional review board. Clinical stage and pathologic features of primary tumors were defined according to the criteria of the American Joint Commission on Cancer/International Union Against Cancer (AJCC/UICC).22
mRNA Isolation and First Strand cDNA Synthesis Total RNA was extracted from the fresh whole blood of CRC patients and healthy volunteers using a QIAmp RNA Blood Mini Kit (QIAGEN Inc., Valencia, CA) ac-cording to the manufacturer’s instructions. The RNA con-centration was determined spectrophotometrically on the basis of absorbance at 260 nm. First strand cDNA was synthesized from total RNA by using a RT-PCR kit (Pro-mega Corp., Madison, WI).
Membrane-Arrays
The procedure of the membrane-array method for the detection of CTC-related mRNA molecular markers was performed according to our recent work.18,23 Patients
over-expressing all 4 molecular markers by membrane-array meth-ods were considered as positive results.18 In our previous
investigation, the sensitivity limit of this technique was
es-tablished at approximately 1 tumor cell per 106white blood cells (5 cells per 1 mL blood).19
Statistical Analysis
All data have been statistically analyzed using the Statistical Package for the Social Sciences, version 11.5 (SPSS Inc., Chicago, IL). A P value less than 0.05 was considered to be statistically significant. Two-sided Pearson 2
test and the Fisher exact test were used to analyze the potential correlation between the expression of molecular markers used in combination and the clinicopathologic fea-tures of the study subjects. The multivariate analysis of independent prognostic factors for postoperative relapse was determined using the logistic regression analysis. The re-lapse-free survival rates of CRC patients were further cate-gorized according to the tumor location. The relapse-free survival rates were calculated by the Kaplan-Meier method, and the differences in survival rates were analyzed by the log-rank test.
RESULTS
One hundred five men (54.1%) and 89 women (45.9%) were included in the study. The average age was 64.9 years (range, 28 –90 years). With regard to the histologic type of
TABLE 2. Correlation Between Postoperative Relapse and Clinicopathologic Features of Stage II Colorectal Cancer Patients Using Univariate Analysis
Postoperative Relapse (ⴙ) (N ⴝ 56) (%) Postoperative Relapse (ⴚ) (N ⴝ 138) (%) P Gender Male/female 28 (50)/28 (50) 77 (55.8)/61 (44.2) .463 Age (yr) ⬍65/ⱖ65 20 (35.7)/36 (64.3) 64 (46.4)/74 (53.6) .174 Maximum size (cm) ⬍5/ⱖ5 27 (48.2)/29 (51.8) 73 (52.9)/65 (47.1) .554 Tumor location Colon/rectum 36 (64.3)/20 (35.7) 92 (66.7)/46 (33.3) .751
Depth of tumor invasion
T3/T4 48 (85.7)/8 (14.3) 137 (99.3)/1 (0.7) ⬍.001 Vascular invasion Yes/no 34 (60.7)/22 (39.3) 18 (13)/120 (87) ⬍.001 Perineural invasion Yes/no 25 (44.6)/31 (55.4) 41 (29.7)/97 (70.3) .048 Histology WD/MD/PD 3 (5.4)/44 (78.5)/9 (16.1) 14 (10.1)/113 (81.9)/11 (8) .163 Mucinous carcinoma Yes/no 3 (5.4)/53 (94.6) 7 (5.1)/131 (94.9) .935
Four molecular markers
Yes/no 45 (80.4)/11 (19.6) 8 (5.8)/130 (94.2) ⬍.001
Number of examined lymph nodes
⬍12/ⱖ12 41 (73.2)/15 (26.8) 78 (56.5)/60 (43.5) .031
Preoperative colonic obstruction/perforation
Yes/no 3 (5.4)/53 (94.6) 7 (5.1)/131 (94.9) .935
Adjuvant chemotherapy
Yes/no 34 (60.7)/22 (39.3) 91 (65.9)/47 (34.1) .491
these tumors, 17 (8.8%) were well-differentiated, 157 (80.9%) were moderately well differentiated, and 20 (10.3%) were poorly differentiated carcinomas. The clinicopathologic characteristics of these 194 stage II patients are listed in Table 1. Overall, 53 of 194 (27.3%) patients were detected with the expression of all 4 mRNA markers using the membrane-array method. During the follow-up period, 36 of 128 (28%) colon cancer patients and 20 of 66 (30%) rectal cancer patients were identified with postoperative relapse. The sensitivity and specificity of the membrane-array method for the prediction of postoperative relapse was 80.4% (45 of 11) and 94.2% (130 of 138), respectively. Eight patients (15%) with positive result of molecular marker expression did not develop post-operative relapse, whereas 11 patients (7.8%) without posi-tive result of molecular marker expression developed post-operative relapse subsequently.
From the correlation between postoperative relapse and clinicopathologic features or molecular markers of stage II CRC patients using univariate analyses, depth of tumor in-vasion (P⬍ 0.001), vascular invasion (P ⬍ 0.001), perineural invasion (P ⫽ 0.048), positive molecular markers (P ⬍ 0.001), and the number of examined lymph nodes (P ⫽ 0.031) were statistically significant (Table 2). No significant differences existed between the positive molecular markers and the presence of local recurrence or distant metastasis respectively, in either colon or rectal cancer patients (both
P⬎ 0.05; Table 3).
Using a multivariate logistic regression analysis, the depth of invasion (P⫽ 0.013; hazard ratio ⫽ 4.080), vascular invasion (P ⫽ 0.032; hazard ratio ⫽ 3.541), and positive molecular markers (P⬍ 0.001; hazard ratio ⫽ 38.597) were demonstrated to be independent predictors for postoperative relapse (Table 4). Moreover, the combination of depth of tumor invasion, vascular invasion, and 4 positive molecular markers as high-risk predictors of postoperative relapse is shown in Table 5. Stage II CRC patients with 1 high-risk
TABLE 3. Circulating Tumor Cells Used for the Prediction of Postoperative Relapse (Local Recurrence and Distant Metastasis) in 36 Colon and 20 Rectal Cancer Patients
Local Recurrence P Distant Metastasis P Colon (Nⴝ 8) Rectum (Nⴝ 8) Colon (Nⴝ 28) Rectum (Nⴝ 12)
Four molecular markers
Positive 6 7 .522 23 9 .605
Negative 2 1 — 5 3 —
TABLE 4. Correlation Between Postoperative Relapse and Clinicopathologic Features of Stage II Colorectal Cancer Patients Using Multivariate Logistic Regression Analysis
Variables  SE P Hazard Ratio 95% CI
Depth (T4/T3) 1.406 0.565 .013 4.080 2.348–11.348
Vascular invasion (yes/no) 2.684 0.911 .032 3.541 1.681–13.432
Four molecular markers (yes/no) 3.653 0.520 ⬍.001 38.597 13.931–106.938
 indicates coefficient; SE, standard error; CI, confidence interval.
TABLE 5. Combination of the Depth, Vascular Invasion, and Molecular Markers as Predictors of Postoperative Relapse for Stage II Colorectal Cancer Patients
T4 or Vascular Invasion (ⴙ) or Molecular Markers (ⴙ) No. Relapse Patients (nⴝ 56) No. Nonrelapse Patients (nⴝ 138) P Hazard Ratio 95% CI
Any one predictor
Positive 48 25 ⬍.001 27.12 11.421–64.397
Negative 8 113 — — —
CI indicates confidence interval.
1 3 9 15 11 4 2 0 2 4 6 8 10 12 14 16 4 5 6 7 8 9 10 Months N umb er o f p at ien ts
FIGURE 1. The interval between subsequently developed postoperative relapse and the presence of all 4 positive mo-lecular markers in the 45 CRC patients.
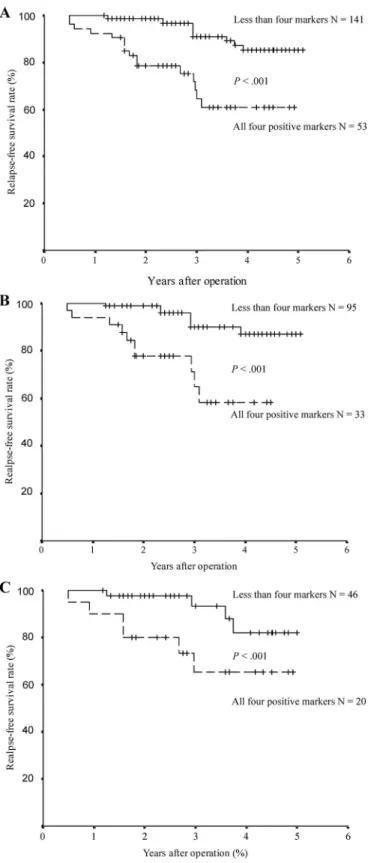
predictor had a relative risk of 27.12 of developing postop-erative relapse compared with those without any 1 high-risk predictor (P⬍ 0.001). The lead-time between the detection of all 4 positive molecular markers and subsequently developed postoperative relapse ranged from 4 to 10 months (Fig. 1; median: 7 months). Furthermore, statistically significant dif-ference was observed in terms of relapse-free survival rate between CRC patients with expression of all 4 markers and those with less than 4 positive markers using the log-rank test, in all patients with CRC, and in colon cancer or rectal cancer (Fig. 2; all P⬍ 0.001).
DISCUSSION
Patients who undergo radical resection of stage II primary CRC are reported to have a 5-year survival rate of around 75%.24There is growing evidence that the prognosis of certain stage II CRC patients with unfavorable prognostic factors can be improved by adjuvant chemotherapy.25,26 Ac-cordingly, there is clearly a need to identify novel predictive factors to guide the identification of stage II CRC patients who are likely to experience relapse. More recently, there has been an attempt to identify novel panels of molecular and biochemical markers that may be used to more precisely define prognosis, and predict benefit of adjuvant treatment in CRC. Several retrospective studies have suggested that a number of molecular markers may now define patients with a higher risk of relapse with both stage II and stage III dis-ease.27–30 However, none of these are currently in clinical application regarding the decision whether patients with stage II CRC should receive adjuvant chemotherapy.
Detection of micrometastases and CTCs in patients with malignancies undergoing surgery for cure remains a challenge for oncologists, because dissemination of neoplas-tic cells is the main determinant of distant relapse and cancer-related death. There are numerous publications about conventional RT-PCR or Q-PCR detection of CTCs in CRC patients,14 –17,31,32but 1 of the limitations is that the
method-ology could analyze only 1 molecular target at a time. Because of the heterogeneity of tumor-related genes, a mul-timarker assay is regarded as more reliable and sensitive than a single marker assay.33–35 Our membrane-array assay was
able to simultaneously detect a panel of informative molec-ular markers for the presence of CTCs in stage II CRC patients, with advantages of time-saving and cost-effective-ness.18Consistent with our findings, Koch e al also showed
the prognostic significance of tumor cells detected in blood samples of patients with stage II CRC using CK-20 RT-PCR.36 Similarly, Lloyd et al have disclosed that for a subgroup of patients with stage I and II CRC, detection of
FIGURE 2. Relapse-free survival rates of stage II colorectal cancer patients were analyzed by the Kaplan-Meier method with the differences compared by a log-rank test. A, All 194 stage II colorectal cancer patients with all 4 mRNA markers expression in the peripheral blood showed a significantly poorer survival rate than those with less than 4 positive
mRNA maker expression (P⬍ 0.001); B, One hundred and
twenty-eight stage II colon cancer patients with all 4 mRNA markers expression in the peripheral blood showed a signifi-cantly poorer survival rate than those with less than 4 posi-tive mRNA maker expression (P⬍ 0.001); C, Sixty-six stage II rectal cancer patients with all 4 mRNA markers expression in the peripheral blood showed a significantly poorer survival rate than those with less than 4 positive mRNA maker ex-pression (P⬍ 0.001).
marker-positive cells by immunobead RT-PCR in peritoneal lavage fluid taken during laparotomy was a significant risk factor for reduced survival after curative resection.37This risk factor was independent of the established prognostic factors of tumor stage and site of primary tumor and may be useful in determining those patients who would benefit from adju-vant chemotherapy.37
Conversely, some recently published studies report con-flicting results regarding the prognostic value of CTCs.38,39A
major problem of most of the published studies is that only small, inhomogeneous patient groups with short follow-up periods were evaluated. Moreover, the methods used for CTCs detection also need to be taken into account, as sensi-tivity and specificity are of major importance and may differ significantly.18,36 A false positive rate of 15% and a false negative rate of 7.8% for the prediction of postoperative relapse using our membrane-array assay suggest that there is room for the improvement of this method. In fact, using microarray technology and gene-expression profiling to iden-tify more specific markers of risk of relapse in stage II patients might improve the accuracy of molecular detection methods.40
Despite curative resection, 28.9% of Stage II CRC patients ultimately developed postoperative relapse in our observation. Our constructed membrane-array method could detect CTCs in 80% of these stage II CRC patients with postoperative relapse. This method is helpful for the predic-tion of both local recurrence and distant metastasis in either colon or rectal cancer patients postoperatively. Multivariate analysis revealed 3 independent prognostic markers in our patient cohort, including T4 depth of tumor invasion, the presence of vascular invasion and all 4 molecular markers. Likewise, Koch et al confirmed that tumor cell detection in blood, T-category and number of removed lymph nodes to be independent prognostic factors for survival rates of stage II CRC patients.36Overall, stage II CRC patients with 1 high-risk predictor, T4 or positive vascular invasion or all 4 molecular markers, have a 27-fold risk of developing post-operative relapse compared with those without any 1 high-risk predictor. Concomitant molecular diagnosis of CTCs with a multimarker panel is a justifiable supplementary ap-proach to the current pathologic staging system, which may help physicians make appropriate judgments on clinical man-agement and predictive prognosis for stage II CRC patients. Hence, therapeutic decision-making models are likely to be further redefined by the inclusion of such molecular markers. Finally, this current investigation has demonstrated that our membrane-array methods could identify stage II CRC patients at high risk of relapse at an earlier stage, with a median lead-time (the time between the presence of molec-ular markers and the onset of clinically detectable recurrence) of 7 months. In practice, 7 months is adequate for the consideration of new therapeutic strategies to possibly cure these patients. Incidentally, the lead-time advantage of rou-tine serum CEA measurement for surveillance of CRC pa-tients is only 4 months.41 Therefore, it is an approximate
3-month benefit for the earlier prediction of postoperative relapse when comparing our membrane-array method and
serum CEA measurement. Moreover, relapse-free survival rates of stage II colon or rectal cancer patients during a median follow up of 40 months are significantly lower in those patients with 4 molecular markers. Consequently, to determinate whether the introduction of adjuvant chemother-apy for stage II patients with positive CTCs is advantageous and efficacious would be an imperative issue for future investigation.
In conclusion, the constructed membrane-array method for the detection of CTCs has been demonstrated to be complementary to the surveillance of stage II CRC patients. The highly sensitive and high-throughput assay is a promis-ing tool for early detection of postoperative relapse, with a median lead-time of 7 months before the development of postoperative relapse. However, large scale and long-term clinical studies follow up is warranted, to confirm the clinical significance of membrane-arrays as decision-making models for adjuvant chemotherapy.
ACKNOWLEDGMENTS
The authors thank Drs. Wing-Yiu Lui, Chien-Yu Lu, and Jan-Sing Hsieh for having contributed financially and materially to the study.
REFERENCES
1. NIH Consensus Conference. Adjuvant therapy for patients with colon and rectal cancer. JAMA. 1990;264:1444 –1450.
2. Moertel CG, Fleming TR, Macdonald JS, et al. Levamisole and fluorou-racil for adjuvant chemotherapy of resected colon carcinoma. N Engl
J Med. 1990;322:352–358.
3. International Multicentre Pooled Analysis of Colon Cancer Trials (IMPACT) Investigators. Efficacy of adjuvant fluorouracil and folinic acid in colon cancer. Lancet. 1995;345:939 –944.
4. Andre T, Boni C, Mounedji-Boudiaf L, et al. Oxaliplatin, 5-fluorouracil and leucovorin as adjuvant treatment of colon cancer: results of the international randomized MOSAIC trial. N Engl J Med. 2004;350:2343– 2351.
5. Goldberg RM, Sargent DJ, Morton RF, et al. A randomized controlled trial of fluorouracil plus leucovorin, irinotecan, and oxaliplatin combi-nations in patients with previously untreated metastatic colorectal can-cer. J Clin Oncol. 2004;22:23–30.
6. Moertel CG. Chemotherapy for colorectal cancer. N Engl J Med. 1994;330:1136 –1142.
7. MacDonald JS. Adjuvant therapy for colon cancer. CA Cancer J Clin. 199747:243–256.
8. Figueredo A, Charette ML, Maroun J, et al. Adjuvant therapy for stage II colon cancer: a systematic review from the Cancer Care Ontario Program in evidence-based care’s gastrointestinal cancer disease site group. J Clin Oncol. 2004;22:3395–3407.
9. Mulcahy HE, Toner M, Patchett SE, et al. Identifying stage B colorectal cancer patients at high risk of tumor recurrence and death. Dis Colon
Rectum. 1997;40:326 –331.
10. Andre T, Sargent D, Tabernero J, et al. Current issues in adjuvant treatment of stage II colon cancer. Ann Surg Oncol. 2006;13:887– 898. 11. Tsai SL, Lu CY, Hsieh JS, et al. The prognostic significance of total lymph node harvest in patients with T2– 4N0M0 colorectal cancer.
J Gastrointest Surg. 2007;11:660 – 665.
12. Cascinu S, Georgoulias V, Kerr D, et al. Colorectal cancer in the adjuvant setting: perspectives on treatment and the role of prognostic factors. Ann Oncol. 2003;14:25–29.
13. Graziano F, Cascinu S. Prognostic molecular markers for planning adjuvant chemotherapy trials in Dukes’ B colorectal cancer patients: how much evidence is enough? Ann Oncol. 2003;14:1026 –1038. 14. Weitz J, Kienle P, Lacroix J, et al. Dissemination of tumor cells in
patients undergoing surgery for colorectal cancer. Clin Cancer Res. 1998;4:343–348.
15. Wharton RQ, Jonas SK, Glover C, et al. Increased detection of circu-lating tumor cells in the blood of colorectal carcinoma patients using two reverse transcription-PCR assays and multiple blood samples. Clin
Cancer Res. 1999;5:4158 – 4163.
16. Wong IH, Yeo W, Chan AT, et al. Quantitative relationship of the circulating tumor burden assessed by reverse transcription-poly-merase chain reaction for cytokeratin 19 mRNA in peripheral blood of colorectal cancer patients with Dukes’ stage, serum carcinoem-bryonic antigen level and tumor progression. Cancer Lett. 2001;167: 183–191.
17. Wang JY, Wu CH, Lu CY, et al. Molecular detection of circulating tumor cells in the peripheral blood of patients with colorectal cancer using RT-PCR: significance in the prediction of postoperative metasta-sis. World J Surg. 2006;30:1007–1013.
18. Wang JY, Lin SR, Wu DC, et al. Multiple molecular markers as predictors of colorectal cancer in patients with normal perioperative serum CEA levels. Clin Cancer Res. 2007;13:2406 –2413.
19. Chen YF, Wang JY, Wu CH, et al. Detecting circulating cancer cells with K-ras oncogene using membrane array. Cancer Lett. 2005;229: 115–122.
20. Wang JY, Yeh CS, Chen YF, et al. Development and evaluation of a colorimetric membrane-array method for the detection of circulating tumor cells in the peripheral blood of Taiwanese patients with colorectal cancer. Int J Mol Med. 2006;17:737–747.
21. Yeh CS, Wang JY, Wu CH, et al. Molecular detection of circulating cancer cells in the peripheral blood of patients with colorectal cancer by using membrane array with a multiple mRNA marker panel. Int J Oncol. 2006;28:411– 420.
22. International Union Against Cancer. TNM Classification of Malignant
Tumors. 6th ed. New York: Wiley-Liss, Inc; 2002.
23. Wu CH, Lin SR, Yu FJ, et al. Development of a high-throughput membrane-array method for molecular diagnosis of circulating tumor cells in patients with gastric cancers. Int J Cancer. 2006;119:373–379. 24. Norum J. Adjuvant chemotherapy in Dukes’ B and C colorectal carci-noma has only a minor influence on psychological distress. Support Care
Cancer. 1997;5:318 –321.
25. Mamounas E, Wieand S, Wolmark N, et al. Comparative efficacy of adjuvant chemotherapy in patients with Dukes’ B versus Dukes’ C colon cancer: results from four National Surgical Adjuvant Breast and Bowel Project adjuvant studies (C-01, C-02, C-03, and C-04). J Clin Oncol. 1999;17:1349 –1355.
26. Wolmark N, Colangelo L, Wieand S. National Surgical Adjuvant Breast and Bowel Project trials in colon cancer. Semin Oncol. 2001;28(1 suppl 1):9 –13.
27. Jen J, Kim H, Piantadosi S, et al. Allelic loss of chromosome 18q and prognosis in colorectal cancer. N Engl J Med. 1994;331:213–221.
28. Watanabe T, Wu TT, Catalano PJ, et al. Molecular predictors of survival after adjuvant chemotherapy for colon cancer. N Engl J Med. 2001;344: 1196 –1206.
29. Allegra CJ, Parr AL, Wold LE, et al. Investigation of the prognostic and predictive value of thymidylate synthase, p53 and Ki-67 in patients with locally advanced colon cancer. J Clin Oncol. 2002;20: 1735–1743.
30. Ribic CM, Sargent DJ, Moore MJ, et al. Tumor microsatellite-instability status as a predictor of benefit from fluorouracil-based adjuvant chemo-therapy for colon cancer. N Engl J Med. 2003;349:247–257.
31. Guller U, Zajac P, Schnider A, et al. Disseminated single tumor cells as detected by real-time quantitative polymerase chain reaction represent a prognostic factor in patients undergoing surgery for colorectal cancer.
Ann Surg. 2002;236:768 –776.
32. Iinuma H, Okinaga K, Egami H, et al. Usefulness and clinical signifi-cance of quantitative real-time RT-PCR to detect isolated tumor cells in the peripheral blood and tumor drainage blood of patients with colorectal cancer. Int J Oncol. 2006;28:297–306.
33. Racila E, Euhus D, Weiss AJ, et al. Detection and characterization of carcinoma cells in the blood. Proc Natl Acad Sci USA. 1998;95:4589 – 4594.
34. Hoon DS, Wang Y, Dale PS, et al. Detection of occult melanoma cells in blood with a multiple-marker polymerase chain reaction assay. J Clin
Oncol. 1995;13:2109 –2116.
35. Conzelmann M, Linnemann U, Berger MR. Molecular detection of clinical colorectal cancer metastasis: how should multiple markers be put to use? Int J Colorectal Dis. 2005;20:137–146.
36. Koch M, Kienle P, Kastrati D, et al. Prognostic impact of hematogenous tumor cell dissemination in patients with stage II colorectal cancer. Int
J Cancer. 2006;118:3072–3077.
37. Lloyd JM, McIver CM, Stephenson S-A, et al. Identification of early-stage colorectal cancer patients at risk of relapse post-resection by immunobead reverse transcription-PCR analysis of peritoneal lavage fluid for malignant cells. Clin Cancer Res. 2006;12:417– 423. 38. Bessa X, Pinol V, Castelli-Bel S, et al. Prognostic value of postoperative
detection of blood circulating tumor cells in patients with colorectal cancer operated for cure. Ann Surg. 2003;237:368 –375.
39. Bosch B, Guller U, Schnider A, et al. Perioperative detection of dissem-inated tumor cells is an independent prognostic factor in patients with colorectal cancer. Br J Surg. 2003;90:882– 888.
40. Wang Y, Jatkoe T, Zhang Y, et al. Gene expression profiles and molecular markers to predict recurrence of Dukes’ B colon cancer.
J Clin Oncol. 2004;22:1564 –1571.
41. Northover J. Carcinoembryonic antigen and recurrent colorectal cancer.