Visuospatial Inattention and Daily Life Performance
in People With Alzheimer’s Disease
Chiung-ju Liu,
Joan McDowd,
Keh-chung Lin
KEY WORDS
• activities of daily living • dementia
• visual attention
Chiung-ju Liu, is Doctoral Student, Department of Gerontology, University of Kansas, 1000 Sunnyside Avenue, Lawrence, Kansas 66045; [email protected]. At the time of this study, she was Graduate Student, Department of Occupational Therapy Education, University of Kansas Medical Center, Kansas City, Kansas. Joan McDowd, PhD, is Professor, Department of Occupational Therapy Education, University of Kansas Medical Center, Kansas City, Kansas.
Keh-chung Lin, ScD, OTR, is Associate Professor, School of Occupational Therapy, College of Medicine, National Taiwan University, Taipei, Taiwan.
This article was accepted for publication under the editorship of Betty Hasselkus.
OBJECTIVE.The purpose of this study was to examine the relationship between visual inattention and daily life performance in people with Alzheimer’s disease.
METHODS.Twenty persons with Alzheimer’s disease (Mini Mental Status Exam [MMSE] > 20) and 21 community dwelling persons (MMSE >26) voluntarily participated in this study. One line bisection test and two cancellation tests were used for testing attention abilities. The Functional Spatial Abilities Questionnaire (FSAQ), the Disability Assessment for Dementia (DAD), and the behavioral subtests of the Behavioral Inattention Test (BIT) were used to assess daily functioning. The presence of visuospatial neglect in people with Alzheimer’s disease was determined by comparing performance on the three attention tests with the control group.
RESULTS.People with Alzheimer’s disease who omitted more targets on the symbol cancellation test showed more deficits on the behavioral subtests of the BIT (p = .02). They also used less systematic search-ing strategies (p = .001), spent more time looksearch-ing for targets (p = .001), and made more commission errors (p = .007) than controls on the cancellation test. However, those with Alzheimer’s disease who had visuospatial neglect did not differ from those without neglect on the FSAQ, DAD, and most of the BIT behavioral subtests. CONCLUSION.People with Alzheimer’s disease have visual inattention problems; however, visuospatial neglect did not interfere with their performance in daily activities as measured in this study. Further research focusing on the relationship between visual attention and daily life function as the disease progresses is sug-gested.
Liu, C.-J., McDowd, J., & Lin, K.-C. (2004). Visuospatial inattention and daily life performance in people with Alzheimer’s disease. American Journal of Occupational Therapy, 58, 202–210.
A
lzheimer’s disease is a progressive disease leading to increasing impairment in intellectual function and daily life performance. Over 50% of persons with dementia are Alzheimer type and the proportion increases in people more than 65 years old (Bouchard & Rossor, 1999; Evans, 1990). Because the elderly adult population in the United States is increasing, the baby boomers especially will be at risk for this disease in the next 2 decades (Evans). Understanding the relation-ship between specific cognitive impairments and activities of daily living (ADL) is important for occupational therapists working with clients with Alzheimer’s disease.Visual inattention refers to decreased ability to locate stimuli in visual space, and is typically observed after brain injuries. This phenomenon includes nonlater-alized inattention, which is the reduced ability to pay attention to overall visual space as well as lateralized inattention, which is the reduced ability to pay attention to visual space contralesional to the injured cerebral hemisphere (Chen-Sea, Henderson, & Cermak, 1993). Lateralized inattention is also known as visuospa-tial neglect and is usually observed in people with focal brain lesions (Heilman, Watson, & Valenstein, 1993; Mesulam, 2000). While performing tasks requiring visual perception and visual search skills, such as the line bisection test and the
can-cellation test, people with visuospatial neglect tend to per-ceive the center of a horizontal line to be far away from the true center, and to omit more targets on one side of the paper than the other (Albert, 1973; Friedman, 1992; Schenkenberg, Bradford, & Ajax, 1980). Additionally, they are likely to use a disorganized search strategy in cancella-tion tests (Weintraub & Mesulam, 1988).
The presence or absence of visuospatial neglect is a sig-nificant predictor of functional outcome in people with focal brain lesions. Previous research has found that people with left visuospatial neglect are more dependent in ADL than those without neglect (Chen-Sea et al., 1993; Denes, Semenza, Stoppa, & Lis, 1982; Gialanella & Mattioli, 1992; Halligan, Cockburn, & Wilson, 1991; Jehkonen et al., 2000; Katz, Hartman-Maeir, Ring, & Soroker, 1999; Kinsella & Ford, 1985).
Deficits in visual attention have been less explored than other cognitive abilities in people with Alzheimer’s disease (Graf, Tuokko, & Gallie, 1990). However, recent studies have found that Alzheimer’s disease is associated with visu-al inattention in tasks requiring visuvisu-al search skills that include figure copying tasks, cancellation tasks, and picture description tasks (Cherrier, Mendez, Dave, & Perryman, 1999; Geldmacher, Doty, & Heilman, 1995; Meguro, Shimada, Someya, Horikawa, & Yamadori, 2001). Other studies also showed that people with Alzheimer’s disease ignored more targets as the number of stimuli increased or as the features of the targets became more complex during the search process (Foldi, Jutagir, Davidoff, & Gould, 1992; Foster, Behrmann, & Stuss, 1999). Moreover, people with Alzheimer’s disease not only reduce attention to overall visual space, but also may have asymmetrical attentional performance in right and left hemispace, which suggests the presence of lateralized inattention deficits (Cherrier et al., 1999; Foster et al.; Meguro et al., 2001).
Lateralized inattention, or visuospatial neglect, is usual-ly observed in people with focal brain lesions. However, recently researchers have reported this deficit in people with Alzheimer’s disease, which is typically characterized by dif-fuse cerebral damage (Bartolomeo et al., 1998; Freedman & Dexter, 1991; Huff et al., 1987; Ishiai, Okiyama, Koyama, & Seki, 1996; Ishiai et al., 2000; Kaida, Takeda, Nagata, & Kamakura, 1998; Mendez, Cherrier, & Cymerman, 1997; Venneri, Pentore, Cotticelli, & Della Sala, 1998). People with mild to moderate Alzheimer’s disease are able to per-form visuospatial tests, but they have shown decreased attention to the left side of space compared to healthy older adults (Ishiai et al., 2000; Mendez et al., 1997). Decreased attention to right visual space on visuospatial tests is also found in some people with the disease (Bartolomeo et al., 1998; Freedman & Dexter, 1991; Mendez et al.). In
addi-tion, some studies have suggested an association between visuospatial neglect and serious limitations in daily func-tioning in the severe stage of the disease (Venneri et al., 1998). Because Alzheimer’s disease is a progressively degen-erative disease, evaluation of visual attention in the mild stage could identify related deficits early in the disease, and guide therapeutic interventions before functional limita-tions are severe.
Visual attention is an important component skill for people doing daily tasks. Attention deficits could influ-ence instrumental ADL performance in people with Alzheimer’s disease such as on-road driving (Duchek, Hunt, Ball, Buckles, & Morris, 1998); however, how the deficit might affect other daily tasks is rarely addressed. Additional research in this area is necessary in order to provide knowledge for health care professionals about how visuospatial attention deficits might influence everyday life among people with Alzheimer’s disease. The purpose of this study is to examine the relationship between visual inattention and daily life performance in people with mild Alzheimer’s disease.
In this study, we predict that: (1) People with Alzheimer’s disease will demonstrate more deficits on visual search tasks than healthy adults. In other words, people with Alzheimer’s disease would be more likely to use an unsys-tematic searching strategy, make more omission errors as well as commission errors, and spend more time than the control adults on the cancellation tests. Additionally, people with Alzheimer’s disease would be more likely to omit more targets on one side of the cancellation tests. (2) Impaired visual search skills will be related to scores on daily life tests. Namely, more omission errors would be associated with lower scores on the daily life tests. (3) People with Alzheimer’s disease who show visuospatial neglect on the visuospatial attention tests will demonstrate lower perfor-mance levels on the daily life test than those without neglect.
Methods
Design
This study was a between-group design. There were two groups for testing the first hypothesis, the participants with Alzheimer’s disease and the control adults. For the third hypothesis, in addition to the control adults, the people with Alzheimer’s disease were divided into two groups, neglect positive and neglect negative, based on their perfor-mance on the visuospatial attention tests.
Participants
People with Alzheimer’s disease and their caregivers were recruited from the Alzheimer’s Disease Research Center at a
Midwest medical center. The caregivers were the persons who accompanied the participants to the study, typically a spouse or an adult child. The inclusion criteria for people with Alzheimer’s disease were: (a) the clinical diagnosis of probable Alzheimer’s disease as defined by the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) Work Group (McKhann et al., 1984); (b) a record of a Mini Mental Status Exam (MMSE) (Folstein, Folstein, & McHugh, 1975) score above 20 within 3 months of study (indicating mild Alzheimer’s disease; Reisberg et al., 1989); (c) a score of at least two on the language comprehension section of the MMSE that required the person perform a three-step command; and (d) no history of stroke, traumatic brain injuries, depression, or other neurological diseases. Twenty persons with Alzheimer’s diseases and their caregivers vol-unteered to participate in this study. The researchers also recruited 21 community dwelling older adults without a diagnosis of Alzheimer’s disease as a control group. Their average age and years of education were matched to the par-ticipants with Alzheimer’s disease.
The MMSE was administrated to the control adults by trained undergraduate occupational therapy students. The attending neurologist of the medical center suggested the score of 26 on the MMSE as a cutoff score for the control group (G. Lopez, personal communication, September 15, 2000). No person in the control group had a history of neu-rological disease. Corrected visual acuity for each partici-pant was 20/70 or better as assessed on a near vision chart. Nine males and 12 females were in the control group (19 participants were right-handed and 2 were left-handed) and 7 males and 13 females in the group with Alzheimer’s disease (18 participants were right-handed and 2 were left-handed). The control adults were a mean age of 73.87 + 8.66 years old (range: 51.54–87.23) and people with Alzheimer’s disease were a mean age of 74.61 + 8.87 years old (range: 52.28–88.33). Average number of years of edu-cation were 13.90 + 2.07 (range: 10–16) for the control group and 13.95 + 2.06 (range: 12–18) for the group of people with Alzheimer’s disease. MMSE scores were 28.76 + 1.00 (range: 27–30) among control adults and 23.65 + 3.33 (range: 20–29) among participants with Alzheimer’s disease.
Materials
Visuospatial Attention Tests. A line bisection test and two visual search tests (an unstructured symbol cancellation test and an unstructured letter cancellation test) were used as visuospatial attention tests. The line bisection test was adapted from Schenkenberg’s line bisection test
(Schen-kenberg et al., 1980). Schen(Schen-kenberg et al. included various lines on a single page, a format that required visual search skill as well as line bisection skill in a way that might make the task too complex for people with Alzheimer’s disease. The test format used in the present study was modified to include only one line per page, as suggested by Kinsella, Packer, Ng, Olver, and Stark (1995). There were 20 trials on the line bisection test. Each trial consisted of a single horizontal line on a sheet of letter-sized paper (8.5˝ high × 11˝ wide). The first two trials with 150-mm lines were prac-tice so that these two trials were not analyzed. The remain-ing 18 trials consisted of three sets of six different lengths of lines (100, 120, 140, 160, 180, and 200 mm) presented on the left, middle, or right portion of the paper. The right and left set of lines were 20 mm away from the short axis of the paper. The participant was asked to indicate the midpoint of the line by drawing a small pen mark. The order of line length and set was randomized for each participant. Lateralized performance on the line bisection test was cal-culated as a percentage of deviation from the true center (Schenkenberg et al.).
The unstructured letter cancellation test was com-posed of different alphabetic letters while the unstructured symbol cancellation test was composed of various geomet-ric figures (Weintraub & Mesulam, 1985). Each cancella-tion test consisted of 60 targets and near 300 nontargets scattered on letter-sized paper; the left and right sides of each page contained 30 targets. The participant was asked to circle all the targets with a pen and to put the pen down when he or she finished. The order of the two cancellation tests was counterbalanced among participants. The total time to finish each cancellation test, as well as number of omission errors and commission errors, were calculated. The sequence of circling each target was also observed for each participant and numbered on a separate copy of the cancellation test. By connecting the numbers, systematic searching patterns were identified as those in which the participants circled targets back and forth vertically, hori-zontally, or diagonally.
Daily Life Performance Tests. The Functional Spatial Abilities Questionnaire (FSAQ) was developed for evaluat-ing spatial orientation in people with Alzheimer’s disease (Liu, Gauthier, & Gauthier, 1996). It contains 12 ques-tions related to one’s orientation in a new environment such as “this person has difficulty following a map,” and in a familiar environment such as “this person gets lost in the home.” Caregivers completed the proxy version of the questionnaire regarding the abilities of their care recipients. A three point ordinal scale is used for answering each question: “YES,” “NO,” “NOT APPLICABLE.” The test–retest reliability is .84 to .85 (intraclass correlation
coefficient [ICC]) and the concurrent validity with MMSE is r = .07 to .34 including the self-rated and proxy-rated versions. A higher total score corresponds to better orien-tation ability.
The Disability Assessment for Dementia (DAD) (Gélinas, Gauthier, McIntyre, & Gauthier, 1999) is a ques-tionnaire designed to evaluate daily function in communi-ty-residing individuals with cognitive deficits. The care-givers completed this questionnaire based on the performance of their care recipients in the past 2 weeks. Activities in the DAD include self-care, instrumental, and leisure functions. “YES/NO” questions are asked about the care-recipient’s ability to initiate, organize, and perform the activity in each domain and the answer “yes” means the individual is able to do the task. The interrater reliability (ICC) = .95 and test–retest reliability (ICC) = .96. The internal consistency is .96 (Cronbach’s alpha) (Gélinas et al., 1999). A total score is obtained by counting the num-ber of yes responses and converting that total to a propor-tion; a higher score on this questionnaire indicates less dis-ability in daily function.
The FSAQ and the DAD measure daily life perfor-mance from the caregiver’s perspective. In addition to these measures, the behavioral subtests of the Behavioral Inattention Test (BIT) (Wilson, Cockburn, & Halligan, 1987a) were used to objectively measure daily life task per-formance among people with Alzheimer’s disease and con-trol adults. Occupational therapists often use the BIT (Wilson et al., 1987a) to evaluate inattention in people with focal brain injuries because the behavioral subtests of the BIT reveal everyday problems that people with focal brain injury typically face (Wilson, Cockburn, & Halligan, 1987b). The nine subtests are simulated daily tasks: picture scanning, telephone dialing, menu reading, article reading, telling and setting the time, coin sorting, address and sen-tence copy, map navigation, and card sorting. Whether peo-ple with Alzheimer’s disease with visual inattention will experience similar problems as those with focal brain injuries on these subtests is unknown, and needs further examination. The only available psychometric information on the BIT comes from a study of people with focal brain injuries (Halligan et al., 1991). This study reported excel-lent test–retest reliability (r = .97) and high interrater relia-bility (r = .99). Construct validity with the conventional tests of the BIT was high (r = .79) and concurrent validity with another functional assessment was r = .53. The BIT behavioral subtests include two parallel forms; one was ran-domly chosen (version A) for the present study. A nine-point scale is used for each subtest. The total score possible for the behavioral subtests is 81. A higher score indicates better performance.
Procedure
The University’s Institutional Review Board approved the research protocol and associated consent forms. Informed consent was obtained from each participant prior to testing. The control group and the people with Alzheimer’s disease performed the three visuospatial attention tests and the nine behavioral subtests of the BIT. These tests were adminis-tered in a quiet room with appropriate lighting. Participants were asked to use the preferred hand to perform the tests and all test materials were placed in front of the participant’s midline. The test session took about an hour to finish. The caregivers completed the FSAQ and the DAD based on the abilities of their care recipients.
Performance on the line bisection test was measured as the length from the left end of the line to the subjective cen-ter minus half of the true line length. A bias index was com-puted for each line (Schenkenberg et al., 1980)1for the
pur-pose of adjusting for different line lengths. A positive value means the subjective center deviated to the right, and a neg-ative value to the left. The mean of the bias indices was obtained for each person in both participant groups. Performance on each cancellation test was calculated as the ratio of the difference between number of cancelled targets in right and left hemispace over the total number of targets cancelled (Bartolomeo & Chokron, 1999)1. A positive
value means more omission errors on the left while a nega-tive value means more omission errors on the right. Visuospatial neglect was operationally defined as present in individuals with Alzheimer’s disease if their lateralized inat-tention performance exceeded two standard deviations (SDs) of the control group on one of the three visuospatial attention tests. A score exceeding +2 SDs was considered left visuospatial neglect, while exceeding -2 SDs was con-sidered right neglect.
Data Analysis
Chi-square and t tests were used to test for differences
between the control adults and the people with Alzheimer’s disease on the cancellation tests. A 2 ×2 analysis of variance (ANOVA) was used to evaluate the effects of hemispace (left and right) and group (Alzheimer’s disease and control) on omission errors in each cancellation test. Next, Pearson’s correlation was used to examine the relation between the omission errors made by people with Alzheimer’s disease on the letter or the symbol cancellation test and the FSAQ, DAD, and behavioral subtests of the BIT. After dividing people with Alzheimer’s disease into neglect positive and neglect negative groups, nonparametric Mann-Whitney U tests were used to compare FSAQ and the DAD scores between the two subgroups. Finally, one-way ANOVA was
conducted to evaluate differences among the control, neglect positive, and neglect negative groups on each behav-ioral subtest of the BIT. The significance level was set at .05.
Results
Visual Search Tasks
People with Alzheimer’s disease and the control group did not differ in the frequency of using an unsystematic search strategy on the letter cancellation test, 25% versus 4.76%, Fisher’s exact p > .05. On the other hand, more people with Alzheimer’s disease used unsystematic searching strategies than the control group on the symbol cancellation test, 50% versus 4.76%, χ2= 10.66. p = .001. No participants
made commission errors on the letter cancellation test; however, people with Alzheimer’s disease made more com-mission errors (1.3 + 1.84) than the control group (.05 + .22) on the symbol cancellation test, t(19.51) = 3.03, p = .007. Time spent in searching for each target was calculat-ed by dividing the total time to finish the test by the num-ber of targets that were located. People with Alzheimer’s dis-ease spent more time (4.55 + 2.35 sec) than controls (2.45 + .74 sec) searching for a target on the letter cancellation test, t(21.19) = 3.74, p = .001, and the symbol cancellation test, 6.76 + 6.94 sec and 2.22 + .84 sec, respectively;
t(19.53) = 2.91, p = .009. The number of omission errors
on the letter cancellation test for the control group were 1.10 + 1.26 items and 1.48 + 1.72 items for left and right hemispace, respectively, and for people with Alzheimer’s disease were 2.60 + 3.08 items and 2.90 + 2.71 items for left and right hemispace, respectively. Similarly, the number of omission errors on the symbol cancellation test for the con-trol group were 0.67 + 1.11 items and 1.14 + 1.74 items for left and right hemispace, respectively, and for people with Alzheimer’s disease were 5.50 + 7.05 items and 5.05 + 4.93 items for left and right hemispace, respectively. People with Alzheimer’s disease made more omission errors than the control adults on the letter cancellation test, F(1, 78) = 8.32, p = .005, and the symbol cancellation test, F(1, 78) = 20.47, p < .001, but statistically significant effects were not found for the side of hemispace or interaction between the group and hemispace.
Cancellation Tests and Daily Life Performance Tests
The FSAQ and the DAD data were missing for two persons with Alzheimer’s disease because the caregivers who accom-panied them were not the main caregivers, and did not spend sufficient time providing care to accurately assess the patient’s abilities. Additionally, one person with Alzheimer’s disease did not complete the article reading subtest, so this person’s total BIT behavioral subtest score was not
includ-ed in the data analysis. Table 1 shows the relation between omission errors on the cancellation tests and performance on the daily life tests. Only one correlation was significant, that between the symbol cancellation test and the BIT sub-tests, r (17) = -.517, p = .02.
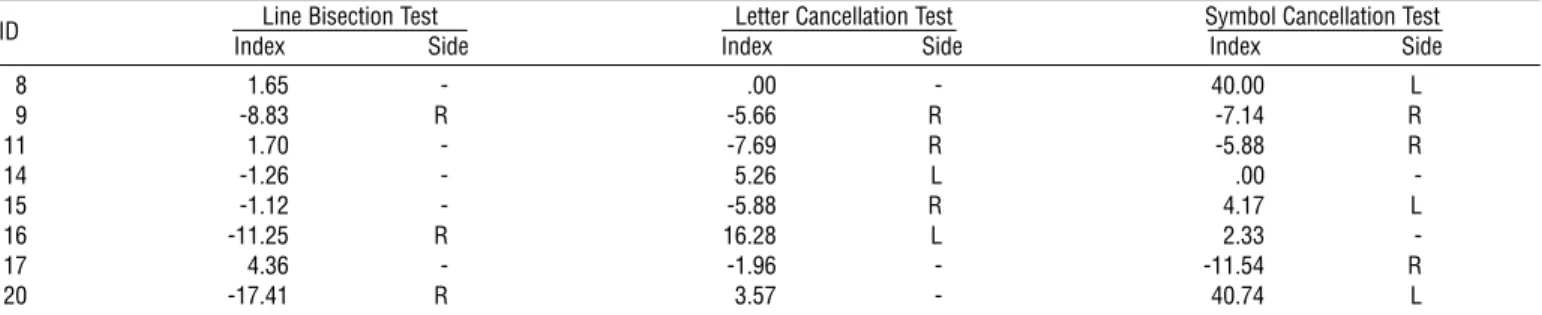
Visuospatial Neglect and Daily Performance Tests
The lateralized indices from the line bisection test, the let-ter cancellation test, and the symbol cancellation test for the control group were -1.03 + 2.86, -.71 + 2.42, and -. 87 + 2.41, respectively. Based on these indices, 8 persons with Alzheimer’s disease showed visuospatial neglect on at least one of the three visuospatial attention tests (neglect positive group). Table 2 displays the neglect side of the neglect pos-itive group and their bias index on the line bisection test and the two cancellation tests. Two persons in the neglect positive group had left neglect and three had right neglect. Because the other three persons did not consistently show the same side of visuospatial neglect across the neglect tests, with right neglect on some tests and left neglect on the other tests, they were considered to have “bilateral neglect” (Freedman & Dexter, 1991). The other 12 persons who did not have visuospatial neglect were grouped into the neglect negative group. The neglect negative and the neglect posi-tive group were not statistically different in age, 76.51 + 8.87; 71.75 + 8.62, t(15.47) = 1.19, p > .05, years of edu-cation, 14.58 + 2.19; 13.00 + 1.51, t(17.94) = 1.91, p > .05, or MMSE score, 24.58 + 3.63; 22.13 + 2.53, t(17.92) = 1.78, p > .05.
Because of small sample size, nonparametric Mann-Whitney U tests were conducted to compare performance on the FSAQ and the DAD between the neglect positive and the neglect negative groups. These two groups were not significantly different based on the scores of the FSAQ (Z = -.58, p > .05; the scores ranged from 16 to 36 and the mean rank was 10.31 for the neglect positive group, while the scores ranged from 14 to 29 and the mean rank was 8.85 for the neglect negative group). There was also no sta-tistical difference between the two groups based on the scores of the DAD (Z = -.044, p > .05; the scores ranged from 57 to 97 and the mean rank was 9.56 for the neglect positive group; whereas the scores ranged from 37 to 98
Table 1. The Correlations Between Omission Errors of Cancellation Tests and Daily Life Performance Tests in People With Alzheimer’s Disease.
FSAQ DAD BIT
Letter Cancellation Test .05 -.26 -.31 Symbol Cancellation Test -.33 -.31 -.52*
Note. FSAQ = the functional spatial abilities questionnaire. DAD = the disability
assessment for dementia. BIT= the behavioral subtests of Behavioral Inattention Test.
and the mean rank was 9.45 for the neglect negative group).
Every participant achieved the maximum score on the map navigation subtest of the BIT, so this subtest was excluded from the analyses described here. Table 3 shows mean scores, standard deviations, and significance testing among the control, neglect negative, and neglect positive groups on the remaining eight behavioral subtests. There were significant group differences on the subtests of picture scanning, F(2,38) = 8.56, p < .001, η2= .31, telling and
set-ting the time, F(2,38) = 12.82, p < .001, η2 = .40, coin
sorting, F(2,38) = 9.49, p < .001, η2= .33, and card
sort-ing, F(2,38) = 9.02, p < .001, η2= .32. A Tukey test was
conducted to do pairwise comparisons between the neglect negative and neglect positive groups for the four subtests that produced a significant group effect. The neglect posi-tive group had a lower score than the neglect negaposi-tive group only on the card sorting subtest, p = .008, d = 1.09.
Discussion
This study was designed to investigate the relationship between visual inattention and daily life performance in people with Alzheimer’s disease. Our findings indicate that this group was more likely to use unsystematic scanning strategies to search for targets and to make more commis-sion errors than the control group on the symbol cancella-tion test. Furthermore, people with Alzheimer’s disease made more omission errors and spent more time on both cancellation tests, indicating that their visual search skills
were impaired. We also observed an association among peo-ple with Alzheimer’s disease between impaired visual search and impaired performance on the behavioral subtests of the BIT. In addition, those with Alzheimer’s disease who had visuospatial neglect had a significantly lower score than those without neglect on the card sorting subtest of the BIT. Thus we show some evidence that people with Alzheimer’s disease experience attentional deficits that affect aspects of their everyday activities.
Although people with Alzheimer’s disease showed visu-al inattention deficits in visuvisu-al search tasks in this study, the type of stimuli involved in the visual search tasks had an influence on performance. They tended to use unsystemat-ic search strategies more frequently than the control adults when the stimuli were symbols, but this difference was not found when the stimuli were letters. Additionally, they did not make commission errors on the letter cancellation test but did make commission errors on the symbol cancellation test. Participants may adopt systematic scanning patterns when confronted with letters because of overlearned read-ing habits. In addition to searchread-ing for target letters by shape, people with Alzheimer’s disease could also recognize targets by their phonological features. However, they could only search for target symbols by comparing target features to a page of symbols that included many look-alike distrac-tors. Further research is needed to examine which features of target and distracter stimuli best support or interfere with visual search performance in this population.
Somewhat surprisingly, performances on the FSAQ and DAD were not related to performance on the
cancella-Table 2. The Bias Index and the Neglect Side of the Neglect Positive Group on the Three Visuospatial Attention Tests.
ID Line Bisection Test Letter Cancellation Test Symbol Cancellation Test
Index Side Index Side Index Side
8 1.65 - .00 - 40.00 L 9 -8.83 R -5.66 R -7.14 R 11 1.70 - -7.69 R -5.88 R 14 -1.26 - 5.26 L .00 -15 -1.12 - -5.88 R 4.17 L 16 -11.25 R 16.28 L 2.33 -17 4.36 - -1.96 - -11.54 R 20 -17.41 R 3.57 - 40.74 L
Note. - = visuospatial neglect was absent on the test. R = right visuospatial neglect. L = left visuospatial neglect.
Table 3. The Performance of Behavioral Subtests of the BIT in the Three Groups.
Control Neglect Negative Neglect Positive
n M SD n M SD n M SD aF
Picture scanning 21 7.48 1.36 12 6.50 1.09 8 5.13 1.81 ***
Telephone dialing 21 8.95 .22 12 8.92 .29 8 8.75 .71 ns
Menu reading 21 9 0 12 8.83 .58 8 8.75 .71 ns
Article reading 21 9 0 11 8.82 .60 8 8.50 .93 ns
Telling and setting the time 21 9 0 12 6.25 2.30 8 6.13 2.95 ***
Coin sorting 21 9 0 12 6.08 3.29 8 5.38 3.70 ***
Address and sentence copy 21 8.81 .68 12 7.92 2.61 8 7.75 2.05 ns
Card sorting 21 8.86 .65 12 8.50 1.17 8 6.75 2.12 ***
tion tests or to the presence of visuospatial neglect. One possible explanation is that the sample size of this study was too small to detect real associations. On the other hand, because the FSAQ and the DAD were two proxy measures completed by caregivers gauging orientation abilities and general daily life abilities, these measures might not have been as sensitive as the behavioral subtests of the BIT that directly measured the performance in people with Alzheimer’s disease. Moreover, items on these two ques-tionnaires were not specifically designed to detect visuospa-tial neglect and associated disabilities, so it is perhaps not surprising that the neglect positive and neglect negative groups did not differ on these measures.
Overall, we observed more visual inattention among participants with Alzheimer’s disease than among control older participants. However, the presence of visuospatial neglect generally did not influence daily life performance except in the card sorting subtest of the BIT. Because the behavioral subtests of the BIT were suggested by clinical practitioners to reflect the everyday problems that people with focal brain injuries with inattention deficits typically face (Wilson et al., 1987b), the test may be less appropriate for people with Alzheimer’s disease. Alternatively, the failure to find differences due to neglect may reflect the fact that our participants were in the relatively early stage of the dis-ease and visuospatial neglect might be less of a factor in deteriorating ADL in the early stage than in the late stage of the disease. Venneri et al. (1998) reported that visuospatial neglect was initially apparent only on some psychological tests and a line cancellation test in two individuals with late stage of the disease but not in every day life. A few months later, however, neglect severely interfered with the daily function of the two persons. Therefore, studies including follow up of people with early Alzheimer’s disease who first show visuospatial neglect on the visuospatial attention tests could help in understanding how neglect influences daily life performance as the disease progresses.
In addition to left visuospatial neglect, people with Alzheimer’s disease in the present study also had right visu-ospatial neglect or bilateral neglect. This finding is in accord with previous research that also found right or bilateral visuospatial neglect in people with Alzheimer’s disease (Bartolomeo et al., 1998; Freedman & Dexter, 1991). The presence of right, left, or bilateral visuospatial neglect might have various influences on a person’s ADL. Previous research that suggested that people with focal brain injuries with left visuospatial neglect had deficits in daily function did not provide enough information to predict daily life performance in people with Alzheimer’s disease who might also show right or bilateral neglect. Future researchers could further examine the influence of left, right, and bilateral
visuospatial neglect on the daily function in people with Alzheimer’s disease.
There were some limitations to the present study. First, this study did not include measures for specific cognitive functions such as memory and judgment that might inter-act with attention ability in daily life performance. Second, the daily life performance tests used here may not have been sufficiently sensitive to attention deficits and daily function in people with Alzheimer’s disease. They were either proxy measures or were borrowed from those measures used to evaluate associated disabilities in another population. Thus, future research with other cognitive measures in addition to attention, and having daily life performance tests particu-larly for visuospatial neglect in people with Alzheimer’s dis-ease may provide more definitive results. Additionally, visu-ospatial neglect might be subtler in people with early Alzheimer’s disease than in people with advanced disease and different from people with focal brain lesions. Longitudinal follow up of people who initially show visu-ospatial neglect on neglect specific tests in the early stage of the disease is necessary, because visuospatial neglect might become more serious and contribute to the functional loss as the disease progress.
Conclusion
One major goal of occupational therapists who work with people with Alzheimer’s disease is to maintain clients’ abili-ties to perform ADL as long as possible. Understanding fac-tors impeding daily tasks could help occupational therapists design intervention strategies to enhance functional perfor-mance. This research was designed to investigate the rela-tionship between visuospatial inattention and daily life per-formance in people with Alzheimer’s disease. The findings reported here provide some initial evidence that visual attention abilities are negatively affected in Alzheimer’s dis-ease, and further exploration of these deficits and their role in daily function is suggested.▲
Acknowledgments
The authors would like to thank Grisel Lopez, MD, and Jill Peltzer, RN, MSN, for their assistance in participant recruitment. This study was undertaken by the first author in partial fulfillment of the requirements for degree of mas-ter’s of science from the Department of Occupational Therapy Education, University of Kansas Medical Center, Kansas City, Kansas. Portions of this paper were presented at the 20th annual conference of the Occupational Therapy Association of Republic of China, Taipei, Taiwan, November 2001.
References
Albert, M. L. (1973). A simple test of visual neglect. Neurology,
23, 658–664.
Bartolomeo, P., & Chokron, S. (1999). Egocentric frame of ref-erence: Its role in spatial bias after right hemisphere lesions.
Neuropsychologia, 37, 881–894.
Bartolomeo, P., Dalla Barba, G., Boissè, M.-F., Bachoud-Lèvi, A.-C., Degos, J.-D., & Boller, F. (1998). Right-side neglect in Alzheimer’s disease. Neurology, 51, 1207–1209.
Bouchard, R. W., & Rossor, M. N. (1999). Typical clinical fea-tures. In S. Gauthier (Ed.), Clinical diagnosis and
manage-ment of Alzheimer’s disease (2nd ed., pp. 57–71). London:
Martin Dunitz.
Chen-Sea, M.-J., Henderson, A., & Cermak, S. A. (1993). Patterns of visual spatial inattention and their functional sig-nificance in stroke patients. Archives of Physical Medicine and
Rehabilitation, 74, 355–360.
Cherrier, M. M., Mendez, M. F., Dave, M., & Perryman, K. (1999). Performance on the Rey-Osterrieth complex figure test in Alzheimer disease and vascular dementia.
Neuropsychiatry, Neuropsychology, and Behavioral Neurology, 12, 95–101.
Denes, G., Semenza, C., Stoppa, E., & Lis, A. (1982). Unilateral spatial neglect and recovery from hemiplegia: A follow-up study. Brain, 105, 543–552.
Duchek, J. M., Hunt, L., Ball, K., Buckles, V., & Morris, J. C. (1998). Attention and driving performance in Alzheimer’s disease. Journal of Gerontology: Psychological Sciences, 53B, 130–141.
Evans, D. A. (1990). Estimated prevalence of Alzheimer’s disease in the United States. The Milbank Quarterly, 68, 267–289. Foldi, N. S., Jutagir, R., Davidoff, D., & Gould, T. (1992).
Selective attention skills in Alzheimer’s disease: Performance on graded cancellation tests varying in density and complex-ity. Journal of Gerontology: Psychological Sciences, 47, 146–153.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). “Mini-Mental State”: A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric
Research, 12, 189–198.
Foster, J. K., Behrmann, M., & Stuss, D. T. (1999). Visual atten-tion deficits in Alzheimer’s disease: Simple versus conjoined feature search. Neuropsychology, 13, 223–245.
Freedman, L., & Dexter, L. E. (1991). Visuospatial ability in cor-tical dementia. Journal of Clinical and Experimental
Neuropsychology, 13, 677–690.
Friedman, P. J. (1992). The star cancellation test in acute stroke.
Clinical Rehabilitation, 6, 23–30.
Geldmacher, D. S., Doty, L., & Heilman, K. M. (1995). Letter cancellation performance in Alzheimer’s disease.
Neuropsychiatry, Neuropsychology, and Behavioral Neurology, 8, 256–263.
Gèlinas, I., Gauthier, L., McIntyre, M., & Gauthier, S. (1999). Development of a functional measure for persons with Alzheimer’s disease: The disability assessment for dementia.
American Journal of Occupational Therapy, 53, 471–481.
Gialanella, B., & Mattioli, F. (1992). Anosognosia and extraper-sonal neglect as predictors of functional recovery following
right hemisphere stroke. Neuropsychological Rehabilitation, 2, 169–178.
Graf, P., Tuokko, H., & Gallie, K. (1990). Attentional deficits in Alzheimer’s disease and related dementias. In J. T. Enns (Ed.), The development of attention: Research and theory
(pp. 527–543). Amsterdam: Elsevier.
Halligan, P. W., Cockburn, J., & Wilson, B. A. (1991). The behavioural assessment of visual neglect. Neuropsychologi-cal Rehabilitation, 1,5–32.
Heilman, K. M., Watson, R. T., & Valenstein, E. (1993). Neglect and related disorders. In K. M. Heilman & E. Valenstein (Eds.), Clinical neuropsychology (3rd ed., pp. 279–336). New York: Oxford University Press.
Huff, F. J., Boller, F., Lucchelli, F., Querriera, R., Beyer, J., & Belle, S. (1987). The neurologic examination in patients with probable Alzheimer’s disease. Archives of Neurology, 44, 929–932.
Ishiai, S., Koyama, Y., Seki, K., Orimo, S., Sodeyama, N., Ozawa, E., et al. (2000). Unilateral spatial neglect in AD: Significance of line bisection performance. Neurology, 55, 364–370.
Ishiai, S., Okiyama, R., Koyama, Y., & Seki, K. (1996). Unilateral spatial neglect in Alzheimer’s disease: A line bisection study.
Acta Neurologica Scandinavica, 93, 219–224.
Jehkonen, M., Ahonen, J.-P., Dastidar, P., Koivisto, A.-M., Laippala, P., Vilkki, J., et al. (2000). Visual neglect as a pre-dictor of functional outcome one year after stroke. Acta
Neurologica Scandinavica, 101, 195–201.
Kaida, K.-I., Takeda, K., Nagata, N., & Kamakura, K. (1998). Alzheimer’s disease with asymmetric parietal lobe atrophy: A case report. Journal of the Neurological Science, 160, 96–99.
Katz, N., Hartman-Maeir, A., Ring, H., & Soroker, N. (1999). Functional disability and rehabilitation outcome in right hemisphere damaged patients with and without unilateral spatial neglect. Archives of Physical Medicine and
Rehabilitation, 80, 379–384.
Kinsella, G., Packer, S., Ng, K., Olver, J., & Stark, R. (1995). Continuing issues in the assessment of neglect.
Neuropsychological Rehabilitation, 5, 239–258.
Kinsella, G., & Ford, B. (1985). Hemi-inattention and the recov-ery patterns of stroke patients. International Rehabilitation
Medicine, 7, 102–106.
Liu, L., Gauthier, L., & Gauthier, S. (1996). The functional spa-tial abilities questionnaire for use with persons who are in the early stages of Alzheimer disease: Preliminary data on relia-bility and validity. Canadian Journal of Occupational Therapy,
63, 224–233.
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., & Stadlan, E. M. (1984). Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the Auspice of the Department of Health and Human Services Task Force on Alzheimer’s disease.
Neurology, 34, 939–944.
Meguro, K., Shimada, M., Someya, K., Horikawa, A., & Yamadori, A. (2001). Hemispatial visual-searching impair-ment correlated with decreased contralateral parietal blood flow in Alzheimer’s disease. Neuropsychiatry, Neuropsychology,
Mendez, M. F., Cherrier, M. M., & Cymerman, J. S. (1997). Hemispatial neglect on visual search tasks in Alzheimer’s dis-ease. Neuropsychiatry, Neuropsychology, and Behavioral
Neurology, 10, 203–208.
Mesulam, M. M. (2000). Attentional networks, confusional states, and neglect syndromes. In M. M. Mesulam (Ed.),
Principles of behavioral and cognitive neurology (2nd ed., pp.
174–256). New York: Oxford University Press.
Reisberg, B., Ferris, S. H., de Leon, M. J., Kluger, A., Franssen, E., Borenstein, J., et al. (1989). The stage specific temporal course of Alzheimer’s disease: Functional and behavioral con-comitants based upon cross-sectional and longitudinal obser-vation. Progress in Clinical and Biological Research, 317, 23–41.
Schenkenberg, T., Bradford, D. C., & Ajax, E. T. (1980). Line bisection and unilateral visual neglect in patients with neu-rologic impairment. Neurology, 30, 509–517.
Venneri, A., Pentore, R., Cotticelli, B., & Della Sala, S. (1998). Unilateral spatial neglect in the late stage of Alzheimer’s dis-ease. Cortex, 34, 743–752.
Weintraub, S., & Mesulam, M. M. (1985). Mental state assess-ment of young and elderly adults in behavioral neurology. In M. M. Mesulam (Ed.), Principles of behavioral neurology (pp. 71–123). Philadelphia: F. A. Davis.
Weintraub, S., & Mesulam, M. M. (1988). Visual hemispatial inattention: Stimulus parameters and exploratory strategies.
Journal of Neurology, Neurosurgery, and Psychiatry, 51,
1481–1488.
Wilson, B., Cockburn, J., & Halligan, P. (1987a). Behavioural
Inattention Test. Fareham, Hants, England: Thames Valley
Test Co.
Wilson, B., Cockburn, J., & Halligan, P. (1987b). Development of a behavioral test of visuospatial neglect. Archives of
Physical Medicine and Rehabilitation, 68, 98–102.
Endnotes
1(A - B)/(A + B) * 100
A: The number of targets cancelled on the right half of the page. B: The number of targets cancelled on the left half of the page.