Exploring Cerebral Palsy from the International Classification of Functionin皂, Disability and Health Framework 359
Exploring Cerebral Palsy from the
Intemational Classification of
Functioning,
Disability and Hea1th
Framework
黃宜君固立彰化師範大學復健諮商研究所
Abstract
This article aims to provide a detailed account of cerebral palsy. lt is conceived from the classification Intemational Classification of Functioning, Disability and Health published by World Health Organization in 2001 and explores cerebral palsy from six main components of such a theoretical model, namely health condition, body functions and structures, activities, participation, environmental factors and personal factors. Through this format of introduction, this article helps to provide a holistic, multidimensional approach to understanding cerebral palsy. Moreover, it exemplifies the advantages of practical application of the lntemational Classification of Functioning, Disability and Health framework.
360 成長與茁壯
以國際健康功能與身心障礙分類象統為架構
探討腦性麻痺相關議題 摘要 本文旨在提供腦性麻痺之詳盡說明 , 其主要採世界衛生組織於 2001 年提出的國際健康功能與身心障礙分類系統為架構,將腦性麻 痺相關議題依該分類系統中六項主要構成要素(健康狀況 、 身體功 能與構造 、 活動、 參與 、環境因素與個人因素)逐一介紹 ,藉此模 式,本文能夠更全面、多元的探討腦性麻痺所造成的種種議題,並 為國際健康功能與身心障礙分類系統之實際應用提供有利之實例。Exploring Cerebral Palsy from thc International Classification of Functioning, Disability and Health Framework 361
Introduction
Since the release of the Intemational Classification of Impairments, Disabilities and Handicaps (ICIDH) by the World Health Organization (WHO) in1980, there is continuous discussion between researchers,
clinicians and disability movement advocacies. Although the ICIDH has its origins in a biomedical understanding, its narrow confinement, which fails to recognize the crucial role of the environment, as well as
the causality that is described between impairment, disability and handicap has been strongly criticized (Simeonsson et al, 2003; Dahl, 2002). ln order to take these shortcomings into consideration, in 2001 the WHO introduces a new approach to disability, known as the lntemational Classification of Functioning, Disability and Health (ICF). It is the result of a revision process based on the ICIDH. In particular, it moves away from a “consequences of disease" classification, which focuses on the impacts of disease or other adverse health conditions as
a result of having impairment, to a “components of health" classification that identifies the constituents of health (WHO, 2001, p.4). Theoretically, the lCF is also regarded as the biopsychosocial model of disability in that it is based on an integration of the medical model, which assumes that an abnormality exists in the disabled individual 's body, caused directly by the impairment (Thomas, 2002),
362 成長與茁壯
and the social model, which defines disability as socially created, rather than a biological determination (Oliver, 2004). Such integration gives the ICF great potential to understand disability from diverse perspectives, including physical, psychological and social aspects, in order to achieve a holistic approach. To date, a large number of countries, including Taiwan, have expressed interest in the need for the application of the ICF framework in government policies or clinical practlce.
A brief review of the International Classification of
Functioning
,
Disability and Health
The ICF comprises two main parts: part one contains
“
functioning and disability" and part two includes“
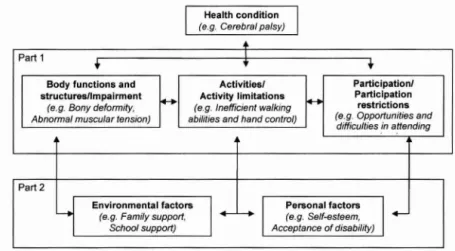
contextual Factors." Specifically,part one addresses issues that are more directly related to an individual's health condition. It is further divided into three components: 1. body functions and structures, which refers to the physiological and anatomical aspects of the body; 2. activity, which means execution of a task or action by an individual; and 3. participation, which connotes involvement by the individual in life situations (WHO, 2001). Although these three components (body functions and structures, activity and participation) are all named by a neutral or positive term, with the idea of introducing the components of health and reducing the undesirable impressions that negative terms
Exploring Cerebral Palsy from the lntcrnational Classification of Functioning.
Disability and Health Framework 363
may have, they can also be applied in a negative way (i.e. impairme肘, activity Iimitation and participation restriction, respectively). This helps us to describe the multi-dimensional situations of real life experience, rather than paying attention solely to the negative aspects as a result of having disability (Ueda & Okawa, 2003).
Part two is made up by two contextual factors: environmental and personal factors. According to WHO (2001), environmental factors refer to the physical, social and attitudinal environments where an individual conducts hislher lives. Personal factors refer to other individual's attributes
,
apart 企om those directly related to health conditions, as discussed earlier, such as gender, age, social background, individual psychological assets, experience etc. Although these two contextual factors are not related to an individual's health condition straightforwardly, they may influence the individual 's perception of hislher health condition (e.g. acceptance of disability or past experience)。r have an effect upon the outcomes of his/her health condition and quality of life (e.g. age, habit or others' support). Figure 1 shows a schematic representation of the ICF model and the examples, which are written in italics, relate to cerebral palsy (CP).
364 成長與茁壯
Environmenlal faclol$
(e.g. Family suppo付,
School support)
Pe悶。 nal facl。用
(e.g. Self.司steem, Acceptance of disability)
Figure 1: The ICF model and its application in children with CP (adapted from WHO, 2001, p.18)
Within this framework, functioning is seen as an interaction between an individual's internal condition and his/her external context.
Disability is not only the consequence of a health condition, but also
determined by the environmental factors surrounding a person and
influenced by an individual's characteristics. Therefore, it is essential to explore disability by adopting an ecological view, which pays attention to the person-environment interaction, and a coherent view, in which the biological, individual and social perspectives are considered (Simeonsson et 泣,2003, van der Ploeg, van der Beek, van der Woude
Exploring Cerebral Palsy from the lnternational Classification of Functioning,
Disability and Health Framework 365
Cerebral palsy
Cerebral palsy is generally defined as a disorder of movement and posture caused by a non旬progressive defect or lesion in the immature brain (8ax, 1964; Schenker, Coster & Parush, 2005). It tends to occur in utero or during or shortly after birth (Odding, Roebroeck & Stam, 2006; Qiu, Paneth, Lorenz & Collins, 2003; 8eckung & Hagberg, 2002). When affected, it causes disturbance of voluntary motor control and movement disorder in one or more limbs and, frequently, in the trunk (Stanley, 81air & Alberman, 2000; Olney & Wright, 1994). Although such a definition of CP is widely accepted and used, it has been criticised as
“
an umbrella term," a term of convenience applied to a broad range of non-progressive,
but often changing,
motor impairment syndromes which are secondary to lesions in the immature brain (Kennes et 泣, 2002; Nordmark, Hagglund & Lagergr凹, 200Ia). In addition, it is argued that this definition regards CP as a heterogeneous condition in terms of etiology, types and severity of impairments (Bax, Goldstein, Rosenbaum, Leviton & Paneth, 2005; Becher, 2002; Miller, 1998).As is the title of this article, the following introduction of CP is organized according to the themes in the ICF model, namely health condition, body functions and structures, activities, participation, environmental factors and personal factors. This format aims to provide
366 成長與茁壯
a holistic approach to understanding cerebral palsy. Additional旬, it can also belp to exemplify the advantage of adopting the lCF model as a theoretical framework.
1. The health condition of cerebral palsy
In order to describe the effects of CP more clearly, clinically there are three ways of classifying cerebral palsy (Stanley et al., 2000). The flfSt classification is based on the outcome of motor impairment. This classification describes the severity of motor impairment usually in terms of minimal, moderate or severely affected motor impairment.
However
,
because of the heterogeneous nature of CP, it is not easy to develop a generally accepted standardised method of classifying the severity of motor impairment much more finely (Nordmark, Hagglund& Lagergren, 2001b; Ostensjo, Carlberg & Vollestad, 2003).
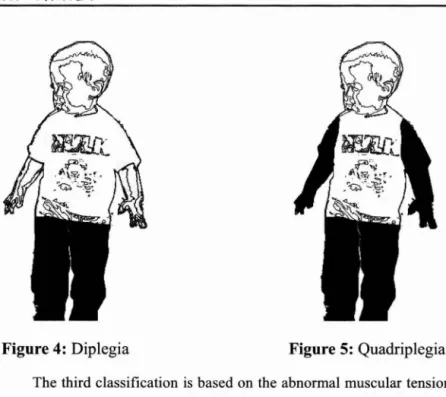
The second classification is based on the area of the body showing impairment. ln this topographic classification, four terms are frequently used to describe the distribution of abnormal muscular tension:
monoplegia, hemiplegia, diplegia and quadriplegia (Stanley et 此, 2000;
Olney & Wright, 1994). Monoplegia is one type of CP involving only one limb. However, this condition is rare (Mine缸, 1956). Hemiplegia is another kind of CP in which one side of the body is affected relatively more than the contralateral part. The upper limb tends to be more severely affected than the lower (see Figure 2 and Figure 3). Diplegia is when the botb lower extremities are involved but have little effect of
Exploring Cerebral Palsy from the Intcmational Classification of Functioning,
Disability and Health Framework 367
the upper extremities (see Figure 4). Quadriplegia means all four limbs are involved and the lower extremities are atIected more severely than the upper (see Figure 5). Although this topographic classification appears clear in describing the area of the body with impairment, in practice it is not always easy to apply. In particular, with the body growing gradually and central nervous systems developing, the clinical syndrome of cerebral palsy may vary greatly (Best, 2009).
368 成長與茁壯
Figure 4: Diplegia Figure 5: Quadriplegia The third classification is based on the abnormal muscular tension resulting from different brain lesions. This classification includes spastic, athetoid and ataxic types. Spasticity is usually described as clasp-knife phenomenon and defined as an increased stretch ref1ex when the spastic muscles are passively stretched at a particular speed (Miller, 1998). It stems from an involvement of the motor cortex or white matter pr叮叮tions to and from the cortical sensorimotor areas of the brain. Abnormalities in ref1exes are obvious in this type.
Additionally, spasticity may cause exaggerated deep tendon ref1exes and clonus in some digital joints. These often lead to poor control of voluntary movements (Stanley et al., 2000; Levitt, 2004).Under this
Exploring Ccrebral Palsy from the Intemational Classification of Functioning,
Disability and Health Framework 369
classification, spasticity is the most common type with more than 70% of CP (Odding et al., 2006; Becher, 2002; Surveillance of Cerebral Palsy in Europe, 2002). The athetoid type connotes an involvement of the basal ganglia and results in an unsteady and fluctuating muscle tones. Fluctuations in muscle tones cause difficulties for these children to maintain their postural stability. Therefore
,
purposeless,
uncontrollable movements are apparent, which are likely to happen when the children are at rest. These involuntary movements may be slow or fast, may be writhing, jerky, swiping or un-patterned and may change greatly with the children's development (Stanley et 址, 2000). Some children are unable to support their weight on their feet and so
need to continually draw their feet up and out, which is called “athetoid dance" (Levitt, 2004). The cerebellar lesion causes ataxia, a distribution in the coordination of voluntary movements (Olney & Wright, 1994). Difficulties in balance and coordination are the characteristic features when children start to sit, stand or walk. AIso, children of this type commonly walk with a wide-based gait, combined with a mild intention tremor. They tend to have hypotone and ine宜iciency of fine motor control (Levitt, 2004; Miller, 1998). Although this classification is popularly applied based on the predominant form, it is found that different types of abnormal muscular tension can coexist and may change over time within an individua1.
370 成長與茁壯
lntemationally, most studies show a preva1ence of CP at around 1.5 to 2.5 per 1000 live birtl>s (Odding et al., 2006; Nordmark et al.,
2001 b; Bottos, Granato, Allibrio, Gioachin & Puato, 1999; Liu, Li, Lin & Li, 1999). Low birth weight remains the predominant risk factor for cerebra1 pa1sy. The preva1ence of CP increases with decreasing birth weight (Blickstein, 2003; Lawson & Badawi, 2003; Ansari, Sheikh,
Akhdar & Moutaery, 2001). Despite the dramatic decrease in perinata1
morta1ity in deve10ped countries during the 1980s and the remarkab1e
advances in obstetric and perinata1 care, the preva1ence of cerebra1 pa1sy has not declined. lnstead, some evidence shows that improved surviva1 rates for 10w birth weight babies may cause a higher risk to an increase in the number of chi1dren with neurodeve1opmenta1 prob1ems (Best, 2009; Ansari et al., 2001). Even though, with better 1iving conditions and improvements in health care, most chi1dren with CP can
expect to survive to adulthood, particu1arly in deve10ped countries (B1air, Watson, Badawi & Stan1ey, 2001).
2. Body functions and structures
Motor impairment is usually the primary prerequisite for the diagnosis of cerebra1 pa1sy. The effect of having CP, however, is like1y to extend beyond motor prob1ems. Chi1dren with CP frequently a1so
have associated disorders, such as cognitive and 1eaming disabilities,
speech and 1anguage difficulties
,
auditory impairments,
visua1 abnormalities, epilepsy and behaviour and emotional disorders.Exploring Cerebral Palsy from the Intcmational Classification of Functioning, Disability and Health Framework 371
(Koman, Smith & Shit, 2004; Beckung & Hagberg, 2002; Parkes, Dolk, Hill & Pattenden, 2001; Pharoah, Cooke, Johnson, King & Mutch,1998). When the extent and severity of motor impairment increase, the likelihood and severity of associated impairments tend to increase (Stanley et al., 2000). However, many studies have reported that about 35~50 % of children with CP have normal to greater intellectual capacity (e.g. Nordmark et al., 2001a; Kennes et al., 2002;
Pharoah et al., 1998).
Development of musculoskeletal system in individuals with CP is also influenced by abnormal muscle tone and involuntary movement control. Therefore, there are secondary complications which usually OCCUT. Many adults or adolescents with CP have secondary impairments in body functions and structures, such as joint pain or skeletal
deformity (Andersson & Mattsson, 2001). Of these, scoliosis is the most commonly associated with cerebral palsy (Bottos, Feliciangeli, Sciuto, Gericke & Vianello, 2001). It usually starts in childhood and
continues to worsen in adulthood. According to Williamson (2003), the prevalence of scoliosis in adults with CP is estimated at 60 ~ 70%.
Scoliosis may lead to pain, aggravated motor dysfunction, compromised pulmonary function and difficulties in walking and sitting or standing in an upright position. For those children who do not walk
,
hip dislocation is a prevalent complication because of spasticity and an incorrect range of motion around the hip joint. According to Knapp and
372 成長與茁壯
Cortes (2002), the incidence of hip displacement ranges from 25% to 75%. lt usually causes pain, pressure sores, difficulties with perineal hygiene and instability in the sitting and standing positions.
3.
Activity performance and limitationsDue to abnorrnal muscle tone and involuntary movement control, the activity perforrnance of individuals with CP is usually compromised. Although the motor function and activity perforrnance among individuals with CP vary greatly, there are several activity limitations associated with CP that are commonly discussed, including walking problems and inefficient hand control.
According to the sequence of motor development, the ability to sit unsupported develops in the children with typical development within 12 months and the ability to walk independently starts within 24 months (Chambers & Sugden, 2006). However, these abilities are usually delayed for children with CP because such abilities require the maturation of neurological postural reactions and enough postural stability through trunk and pelvic control (Haywood & Getchell, 2005). They can also be absent for some children who are more severely atTected by CP. Palisano, Copeland and Galuppi (2007) surveyed 156 adolescents with CP, ranging in age from 11.6 to 17.7 years, and report that 22% of participants are transported by a wheelchair or power wheelchair and are unable to ambulate. ln a study, involving 167 children with CP, Nordmark et al (2001 b) find that 16% of the
Exploring Cerebral Palsy from the lnternational Classification of Functioning,
Disability and Health Framework 373
participating children are unable to walk at the age of 6.8 years. In
addition
,
many studies have found that most individuals with CPrequire a walking aid or use a wheeled device, in particular when
outdoors (e.g. Schenker et al., 2006; Bechung & Hagberg, 2002). Individuals with CP expend greater energy during walking than
other non-disabled people (Johnson, Moore, Quinn & Smith, 2004;
Mattsson & Andersson; 1997). This may lead to their walking ability
deteriorating in adulthood. According to the study of 此-1urphy,此-101ner
& Lankasky (1995), which inc1udes 101 adults with CP between the
ages of 19 and 74 years, about 75% of the participants have to stop
walking and change to wheelchairs by the time they are around 25
years old because of fatigue and inefficiency of ambulation, although
there are some participants who lose their walking ability at around 45 years old due to joint pain. Data from a study (Bottos et al, 2001),
including 72 adults with CP, shows that 44.8% of the participants
dramatically decline or lose their independent walking or other forms
of locomotion between 20 and 40 years. Their reasons for the loss
inc1ude incorrect surgery, bone fracture due to a fall and physiological
bum-out syndrome, which means that the physical function deteriorates
as a consequence of its overuse and being overburned (Pimm, 1992).
Due to the deterioration of their walking ability, a high percentage of
individuals with CP count on wheeled devices for transportation in adulthood.
374 成長與茁壯
The hand function of those with CP is often atfected by abnormal
muscular tension and reflex movement, asymmetric movement pattem
(e.g. shoulder forward flexion with elbow and wrist extension) and poor postural control (Hanna et al., 2003). Many children have difficulties in reaching
,
grasping,
releasing or manipulating objects because ofdeficient hand-eye function, lack of coordination of movement
sequences and sensory deficits in areas of stereognosis and two-point discrimination (Eliasson & Gordon, 2000). Problems in manual dexterity are the main reason contributing to difficulties in the activities of daily living. As a result, only a few of adults with CP are able to perform daily tasks unassisted and many of them require physical assistance in self-care and daily activities. Turk, Geremski, Rosenbaum and Weber (1997) surveyed 63 women with CP, who range in age from 20 to 74 years old, and report that 38% are independent in carrying out daily routines whereas 16% require great assistance in such activities as eating, bathing, dressing, grooming and toileting. In a study of 156 adolescents with CP (Palisano et al., 2007), 37% of the participants perform activities by themselves, 35% need physical assistance at times throughout the day, particularly in the area of personal care and mobility, and 28% depend profoundly on others' assistance. Data from a study which includes 149 adolescents and young adults with CP shows that 45% of the participants are categorised as being independent in the activities of daily living, 18% require assistance with some daily
Exploring Cerebral Palsy from thc lnternational Classification of Functioning, Disability and Health Framework 375
living tasks, and 37% need maximum assistance in their daily routines (Cathels & Reddihough, 1993). Many studies on children with CP have suggested that the severity of cerebral palsy, cognitive impairment and age are important factors that are highly related to these children's functioning and activity performance (e.g. Voorman et al., 2006; Liptak et al., 2001).
4. Participation opportunities and restrictions
The inf1uence of CP is long-term, multidimensional and wide-ranging. It also has inevitable effects on these children 's participation opportunities. Although nearly half of individuals with CP have the same intellectual capacity as their peers with typical development or are mildly affected by CP, the problems in motor functioning and management of activities of daily living create difficulties in the fulfilment of independence and negatively affect their choices of social activities (Ostensjo et al., 2003; Beckung & Hagberg, 2002). It has been found that children with CP rely more on their parents' care and have fewer outdoor activities or friends (Bailey & Wolery
,
1992). AIso,
many parents of children with CP are more protective of their own children and are faced with long-term and ongoing responsibilities for looking after them. The parents then tend to become isolated and distant from their friends (Attwood & Thomson,
376 成長與茁壯
participate in activities with their peers and leam social skills. Many of them live in an environment oriented towards their homes, even after adulthood (Lawlor, Mihaylov, Welsh, Jarvis & Colver, 2006; Baker & Donelly
,
2001).During school going a阱, these children are likely to have difficulties in being involved in campus life and face such situations as low academic perfOIτnance, exclusion from some curriculum or activities, difficulties in developing an equal relationship with their non-disabled peers and being rejected by some school staff (Simeonsson, Carlson, Huntington, McMillen & Brent, 2001). Some studies have found that the severity of cerebral palsy, cognitive performance and epilepsy are important factors influencing school
integration and social communication ofpupils with CP (Schenker et al., 2006).
Although participation opportunities vary from individual to individual, an adverse social participation has been found for adolescents and adults with CP. In general, these individuals demonstrate a lower rate of college education, employment, social
integration and rely more on their family members for their living arrangement (Michelsen, Uldall, Kejs & Madsen, 2005; Andersson & Mattsson, 2001). Their choice of community and leisure activities is restricted due to various reasons. These include the individuals' physical challenges and disability awareness
,
poor support from others,
Exploring Ccrcbral Palsy from thc International Classification of Functionin皂,
Disability and Health Framcwork 377
time pressure, transportation problems, limited accessibility to public spaces, lack of information, expensive program cost, and so on (Rimmer, Riley, Wang, Rauworth & Jurkowski, 2004).
5. Environmental factors
According to the ICF model, environmental factors encompass the physical, social and attitudinal environment where individuals conduct their lives. Although these environmental factors are extemal to the individuals, they can positively or negatively affect the individuals' participation in society, capacity to perform activities and perceptions of outcomes of their health conditions. World Health Organization (2001) makes a distinction between the physical environment and the social and attitudinal environment. The physical environment is defined as animate and inanimate elements of the natural environment, and components of the built environment, whereas the social and attitudinal environment refers to the observable consequences of customs,
practices, ideologies, values, norms, factual beliefs and religious beliefs which affect the individuals' behaviour and sociallife at alllevels, from interpersonal relationships and community associations to political, economic and legal structures (WHO, 2001, p.182 and p.190).
Several studies explore the influence of environmental factors in the home context. For example, in a study involving 326 participants, Stark (2001) finds that there are several physical environmental barriers
378 成長與茁壯
at home, ranging from uneven surfaces or steps, inappropriate fumiture height and layout to narrow domestic space and unpleasant temperature or atmospheric condition. These environmental barriers are likely to cause the participants difficulties in performing daily tasks and personal care. Assistive devices, architectural modifications and personal assistance are reported as useful solutions to overcome the environmental barriers. Beresford and Oldman (2002) find that the lack of domestic space is a major factor for most families of children with disability. It may cause difficulties for these children to caπY out their daily activities independently and further restrict the children 's opportunities to make their own decisions about where and how they move about at home. Many children accordingly have to depend on their family members' care. Similarly, in a study of 153 community-dwelling wheelchair users, Hoening, Landerman, Shipp and George (2003) indicate that mobility limitations and environmental barriers are likely to impede the participants' willingness and opportunities to participate in activities both within the home and outside the home. Based on data from a series of 12 home interviews, Cook, Brotherson, Weigel-Garrey and Mize (1996) suggest that many physical barriers that children with disabilities encounter at home can be removed by making some relatively simple and inexpensive modifications, such as locating mirrors properly, lowering the bed or widening the doors. The children then are more able to exercise choice
Exploring Cerebral Palsy from the lntemational Classification of Functioning, Disability and Health Framework 379
in participation in family activities in the manner they want.
Parents' support and other family members' assistance have long been viewed as the strongest social and attitudinal environmental facilitators. According to Attwood and Thomson (1997), most parents of children with disability view their support as an important resource for their children's welfare. As a result, they are likely to pay more attention to their children 's development and have a higher emotional involvement in the issues sUITounding th凹 childrenthan other parents of non-disabled children. Consequently, these parents tend to become isolated as they spend a substantial amount of time looking after or accompanying their children. Dale (1996) identifies two different models that have been put forward to explore parents' reactions to their children's disabilities. The first is the pathological model which emphasises the stress and difficulties that parents of children with disabilities can experience. For example, data from a study involving 78 mothers of children with CP
,
Barlow,
Cullen-Powell and Cheshire (2006) find that the participating mothers have a higher level of stress and anxiety than other mothers whose children are developing typically: 26% and 11.7% of the participating mothers are at moderate and high risk of clinically anxious mood (compared with population female norms of l3% and 跳, respectively) and 19.5% of them are at moderate risk of clinically depressed mood (compared with norms of 4%). In a survey of 62 mothers and 22 fathers of children with CP,
380 成長與茁壯
Wanamaker and Glenwich (1998) report that the level of stress of caring for their children that the parents perceive is related both to their perception of the severity of their children's disability and also to their satisfaction with the social support they receive.
The second model discussed by Dale is the stress and coping model, which focuses on parents' coping strategies to manage the stress and challenges that result from their children's disabilities. In a study of 20 families caring for children with severe disabilities, Beresford (1994) finds that parental affection and sense of responsibility, as well as a desire to restrict the impact of the disability on their children 's lives and improve their children's happiness, are strong motivating factors for parents to cope with the stressful daily events that they face. Read (2000), who interviewed 12 mothers of teenagers with disabilities, indicates that in order to increase their children 's sense of well-being and quality of life
,
parents of children with disabilities,
in particular mothers, are often involved in the long-term and all-encompassing nature of caring work. For example, they provide ongoing physical care of their children, deal with their children's emotional issues, andactively mediate between their children and other individuals,
organizations or systems, such as teachers, schools and education systems. Therefore, they usually play a pivotal role in their children's lives and become a strong supporter for their children both at home and in the outside world.
Exploring Cerebral Palsy from the International Classification of Functioning, Disability and Health Framework 38)
Other studies draw attention to the influence of environmental factors in the school context. Architectural barriers, such as inaccessible transportation or buildings, are frequently reported as hindrances for pupils with disabilities to accessibility and participation in school. For example
,
in a study involving a series of focus group meetings of 15 pupils with disabilities and their parents, Pivik, McComas and Laflamme (2002) identified several environmental barriers on campus, such as heavy doors, narrow corridors, a lack of elevators, steep ramps, poorly designed lockers as wel1 as inaccessible playground and recreational areas. As a result of these barriers, the pupils with disabilities are likely to have less social contact with their peers, be excluded from some lessons or outdoor activities and have difficulties in exercising their choice and control in the manner that their peers do. Temporal aspects of the school environment may also be disadvantageous for these pupils. Hemmingson and Borell (2002) point out that the school routines for using different classrooms for different classes often become a challenge for pupils with physical disabilities. Without enough time in breaks, the pupils cannot transfer to a different classroom on time or by themselves,
especially if that classroom is located on a different floor or in another building. As a result, the pupils' leaming opportunities are likely to be restricted. Assistive devices, building adaptations and alterations, extra leaming support, personal assistance, or support from teachers or peers are reported as382 成長與茁壯
resources for these pupils to overcome the physical and temporal aspects of school environmental barriers. They can also help the pupils to increase their school participation and the quality of schooling.
However, other studies have found that pupils with CP are likely to be rejected by their peers or school staff and have problems in relationships with their peers or teachers. 1n addition, some studies show that pupils with disabilities are likely to be teased or bullied and suffer verbal abuse from their peers. For example, Connors and Stalker (2003) interviewed 26 school-going children with disabilities and report that a higher proportion of the participants have the experience of being bullied at school. Most of these children then develop strategies or get support from their parents or teachers to deal with it so
that bullying does not recur. However, a few of them view bullying as a
part of their daily lives. Pivik et al (2002) find that pupils with disabilities encounter a wide range of attitudinal barriers from their peers or sometimes from their teachers. According to the participating pupils' perception
,
some people do this intentionally. For example,
they isolate, are prejudiced against, physically bully or address the pupils with disabilities in a devaluing way (e.g. stupid person). However, some of the others' behaviours are unintentional,
mainly due to their lack of knowledge or misunderstanding about the children's disability. Based on the experience of these participants with disabilities,
increasing opportunities to talk about their disabilities with their peersExploring Cerebral Palsy from the lntemational Classification of Functioning, Disability and Health Framework 383
or teachers are helpful strategies to increase their social interaction and change others' negative attitudes towards them (Pivik et al., 2002; Low 1996). Moreover, a supportive school atmosphere, where they are accepted with respect and their different needs are valued, is particularly highlighted by most pupils with disabilities as an important social and attitudinal environmental facilitator (Simeonsson et al., 2001; Mihaylov, Jarvis, Clover & Beresford, 2004).
6. Other personal factors
Many studies have suggested that children with CP are likely to have adverse psychological development
,
such as lower self-esteem or self-confidence, and emotional problems, such as frustration, stress or helplessness as a result of their functional limitations and lower attainment of independence. For example, Anderson and Clarke (1982) find that adolescents with CP tend to show signs of unhappiness or depression, have lower self-confidence and self-esteem, and frequently wo的 abouttheir lack of skills. Quinn (1998) and Cogher, Savage and Smith (1992) indicate that, because of their impairments, children with CP may perceive themselves as different and inadequate. Such a perception further lowers their self-esteem and causes embarrassment or sense of inferiority. Appleton, Minchen, Ellis and Elliott (1994) find that lower academic and athletics performance as well as unsatisfactory physical appearance are the main reasons influencing these children's384 成長與茁壯
sense of se1f. Consequently, they are 1ike1y to view themse1ves as 1ess competent than their non-disab1ed peers. Scholtes
,
Vermeer and Meek (2002) point out that repeated fai1ure in these chi1dr凹 's day-to-day lives and socia1 re1ationship prob1ems have a negative effect on these chi1dren's deve1opment. Some chi1dren may withdraw themse1ves from interaction with others in order to avoid being hurt whereas some may overestimate their competencies as a means of se1f-defence.lt is, however, important to note that results from some studies a1so suggest that there is no difference between the 1eve1 of se1f-esteem of chi1dren or ado1escents with CP and that of chi1dren with typica1 deve1opment. For examp1e, in a study of 110 chi1dren with CP, whose ages ranged from 9 to 13 years old, Schuenge1 et a1 (2006) find that,
although these participants have a significantly 10wer perceived competence in motor domain, their results in globa1 se1f-worth and perceived competence in other domains, such as socia1 skills, physica1 appearance and scho1astic performance, are positive and appropriate to their deve1opmenta1 stage. Manue1, Ba1krishnan, Camacho, Smith and Koman (2003) surveyed 50 pre-ado1escents and ado1escents with CP,
ranges in age from 9 to 18 years old, and report that, although 30% of participants score be10w a cut-off point for 10w se1f-esteem, the average score of se1f-esteem of the all participants are comparab1e to samp1es of healthy ado1escents. Data from 101 ado1escents with physica1 disabilities aged 11-16 years old (Stevens et al., 1996) show that the
Exploring Cerebral Palsy 命om the Intemational Classification of Functioning,
Disability and Health Framework 385
participants have the same level of self-esteem as those without disabilities. Although these studies do not exclude the possibility that their participants may be defensive and so reluctant to admit their
unfavourable characteristics, they mainly interpret their results as
indicating that these children appear resilient against the challenges that
are posed to them. As these children have psychological resilience, they
are able to accept their disability and also maintain a positive
self-worth and perceived competence.
Conclusions
Throughout this article
,
reference has been made to the explorationof the multidimensional aspects of cerebral palsy, based on the WHO 's
lntemational Classification of Functioning, Disability and Health. The
information provided is holistic and relatively straightforward, so that
various areas relating to the individuals with CP are addressed and,
accordingly, person-centered, which is desirable in current
rehabilitation climate as well as special education area. ln addition, CP,
one of the frequent causes of severe disabling conditions in childhood,
is a lifelong condition, which affects a1most every aspect of the life of
an individual with CP, from the time of birth. People with CP are likely
to place a heavy demand on their families as well as the medical
,
386 成長與茁壯
complex and wide-ranging needs cannot be met by only a single model of disability, neither the medical nor the social one. Therefore, the ICF,
which integrates the medical model and the social model, can help researchers, clinical practitioners and educators to consider dimensions of disability stemming from CP.
References
Anderson, E. M., & Clarke, L. (1982). Disability in adolescence.
London: Methuen.
Andersson, C., & Mattsson, E. (2001). Adults with cerebra1 pa1sy: a survey describing prob1ems, needs, and resources with special emphasis on 1ocomotion. Developmental medicine and child neurology, 43, 76-82.
Ansari, S. A., Sheikh, A., Akhdar, F., & Moutaery, K. M. (2001).
Towards improving care in cerebral palsy. Disability and rehabilitation, 23(13),592-595.
Appleton, P., Minch凹, P., Ellis, N., & Elliott, C. (1994). The self-concept of young people with spina bifida: a population-based study. Deve/opmenta/ medicine and child neurology
,
36,
198-215.Attwood, R., & Thomson, D. (1997). Parental values and care for the child with special needs. ln G. Lindsay & D. Thompson (Eds.), 均lues into practice in special education (pp. 121-l35). London: David Fulton.
Exploring Cerebral Palsy from the lnternational Classification of Functioning, Disability and Health Framework 387
Bail句, D. 且,& Wolery, M. (1992). Teaching infants and preschoolers
with disabilities (2nd ed.). New York Oxford: Maxwell
Macmillan lnternational.
Baker, K., & Donelly, M. (2001). The social experiences of children with disability and the inf1uence of environment: a framework for intervention. Disαbility and socie紗', 16(1) , 71-85.
Barlow, J. H., Cullen-Powell, L. A., & Cheshire, A. (2006).
Psychological well-being among mothers of children with cerebral
palsy. Early child development αnd care, 176(3-4),421-428.
Bax, M., Goldstein, M., Rosenbaum, P., Leviton, A., & Paneth, N.
(2005). Proposed definition and classification of cerebral palsy,
April 2005. Developmental medicine and child neurology, 47(8),
571-576.
Bax ,此1.C. O. (1964). Terminology and classification of cerebral palsy.
Developmental medicine and child neurology, 6, 295-297.
Becher, 1. G. (2002). Pediatric rehabilitation in children with cerebral
palsy: general management, classification of motor disorders.
Journal ofprosthetics and orthotics, 14(4), 143-149.
Beckung, E., & Hagberg, G. (2002). Neuroimpairments, activity
limitations, and participation restrictions in children with cerebral
palsy. Developmental medicine and child neurology, 44(5),
388 成長與茁丹士
Beresford, B. (1994). Positively parents: caring for a severely disabled child. York: SPRU.
Beresford, B., & Oldman, C. (2002). Housing matters: national evidence relating to disabled children and their housing. Bristol: The Policy Press.
Best, S. J. (2009). Cerebral palsy. In M. G. Broadwin, F. W. Siu, J. Howard & E. R. Broadwin (Eds.), Medical, psychosocial and vocational aspects
0/
disability (3rd ed., pp. 305-318). Athens, GA: Elliott & Fitzpatrick.Blair, E., Watson, L., Badawi ,叭, & Stanley, F. J. (2001). Life expectancy among people with cerebral palsy in Westem Australia. Developmental medicine and child neurology, 的 (8) , 508-515.
Bottos, M., Feliciangeli, A., Sciuto, L., Gericke, c., & Vianello, A. (2001). Functional status of adults with cerebral palsy and implications for treatment of children. Developmental medicine
and child neurology, 的 (8) ,516-528
Bottos, M., Granato, T., Allibrio, G., Gioachin,仁, & Puato, M. L. P.
(1999). Prevalence of cerebral palsy in north-east Italy from 1965 to 1989. Developmental medicine and child neurology, 41(1), 26-39.
Cathels, B. A., & Reddihough, D. S. (1993). The health care of young adults with cerebral palsy. Medical journal
0/
Australia, 159, 444-446.Exploring Cercbral Palsy from the lnternational Classification of Functioning, Disability and Health Framework 389
Chambers, M., & Sugden, D. (2006). Early years movement skills:
description, diagnosis and intervention. London: Whurr.
Cogher, L., Savage, E., & Smith, M. F. (1992). Cerebral palsy: the
child and young person. London: Chapman & Hall Medical.
Connors, C., & Stalker, K. (2003). The views and experiences of
disabled children and their siblings: a positive outlook. London:
Jessica Kingsley Publishers.
Cook, C., Brotherson, M., Weigel-Garrey,仁,& Mize, 1. (1996). Homes to support the se1f-determination of children. In D. Sands & M.
Wehmeyer (Eds.)
,
Selj三determination across the life span:independence and choice 戶rpeople with disabilities (pp. 91-110).
Ba1timore: Paul Brookers.
Dah1, T. H. (2002). Intemational classification of functioning, disability
and health: an introduction and discussion of its potentia1 impact
on rehabilitation services and research. Journal 01 rehabilitation
medicine, 34(5),201 -204.
Da1e, N. (1996). Working with families of children with special needs:
partnership and practice. London: Routledge.
E1iasson, A. 仁,& Gordon , A. M. (2000). Impaired force coordination during object re1ease in children with hemiplegic cerebral palsy.
390 成長與茁壯
Hanna, S. 且,Law, M. c., Rosenbaum, P. L., King, G. A., Walker, S.且, Pollock, N., et al. (2003). Development of hand function among children with cerebral palsy: growth curve analysis for ages 16 to 70 months. Developmental medicine and child neurology, 45(7), 448-455.
Haywood, K. 悅, & Getchell, N. (2005). Life span motor development (4th ed.). Champaign, IL; Leeds, UK: Human Kinetics.
Hemmingson, H., & Borell, L. (2002). Environmental barriers in
mainstream schools. Child: care, health and development, 28(1), 57-63.
Hoenig, H., Landerman, L.氏, Shipp, K. M., & George, L. (2003).
Activity restriction among wheelchair users. Journal 01 the American geriatrics socie紗~51(9), 1244-1251.
Johnston, T. E., Moore, S. 丘, Quinn, L. T., & Smith, B. T. (2004). Energy cost of walking in children with cerebral palsy: relation to the Gross Motor Function Classi 日 cation System. Developmental medicine and child neurology, 46(1),34-38.
Kennes, J., Rosenbaum, P., Hanna, S. E., Walter, S., Russell,缸,Raina,
P., et al. (2002). Health status of school-aged children with cerebral palsy: information from a population-based sample. Developmental medicine and child neurology, 啊, 240-247.
Knapp, D. R., & Cortes, H. (2002). Untreated hip dislocation in cerebral palsy. Journal 01 pediatric orthopedics, 22(5), 668-671.
Exploring Cerebral Palsy from thc International Classification of Functioning, Disability and Health Framework 391
Koman, L. A., Smith, B. P., & Shit, J. S. (2004). Cerebral palsy. The lancet, 363(9421), 1619-1631.
Lawlor, K., Mihaylov, S., Welsh,旦, Jarv函,S., & Colver, A. (2006). A
qualitative study of the physical, social and attitudinal
environments influencing the participation of children with cerebral palsy in northeast England. Pediatric rehabilitation, 9(3), 219-228.
Lawson, R. D., & Badawi, N. (2003). Etiology of cerebral palsy. Hand clinics, 19(4),549-556.
Levitt, S. (2004). Treatment 01 cerebral palsy and motor delay (4th ed.). Oxford: Blackwell.
Lipt此, 0. S., O'Donnell, M., Conaway, M., Chuml間, W. 仁,Worley, 0., Henderson, R. 仁, et al. (2001). Health status of children with moderate to severe cerebral palsy. Developmental medicine and child neurology, 43(6), 364-370.
Liu, J.-M., Li, S., Lin,見, & Li, Z. (1999). Prevalence of cerebral palsy in China. lnternational journal 01 epidemiology, 28, 949-954. Low, J. (1996). Negotiating identities, negotiating environments: an
interpretation of the experiences of students with disabilities.
Disability and Socie紗" 11(2),235-248.
Manuel, J. C., Balkrishnan, R., Camacho, F., Smith, B. P., & Koman, L. A. (2003). Factors associated with self-esteem in pre-adolescents and adolescents with cerebral palsy. Journal 01 adolescent health,
392 成長與茁壯
32(6),456-458.
Mattsson, E., & Andersson, C. (1997). Oxygen cost, walking speed, and perceived exertion in children with cerebral palsy when walking with anterior and posterior walkers. Developmental medicine and child neurology, 39, 671-676.
Michels凹, S. 1., Uldall, P., Kejs, A. M. T., & Madsen, M. (2005).
Education and employment prospects in cerebral palsy.
Developmental medicine and child neuroiogy, 47(8), 511-517.
Mihaylov, S. 1., Jarvis, S. N., Clover, A. 且, & Beresford, B. (2004). ldentification and description of environmental factors that
influence participation of children with cerebral palsy.
Developmental medicine and child neurology, 46(5), 299-304.
Miller, 0. (1998). Cerebral palsies: an overview. In 0. Miller & 0. D. Clark (Eds.), The cerebral palsies . causes, consequences, and
management (pp. 1-35). Boston; Oxford: Butterworth-Heinemann.
Minear, W. L. (1956). A classification of cerebral palsy. Pediatrics, 18, 841-852.
Murphy, K. P., Molner, 0. E., & Lankasky, K. (1995). Medical and functional status of adults with cerebral palsy. Developmental
medicine and child neurology, 37, 1075-1084.
Nordmark, E., Hagglund, 0., & Lagergren, J. (2001a). Cerebral palsy in
southem Sweden l. Prevalence and clinical features. Acta
Exploring Cercbral Palsy from the lnternational Classi 日 cation of Functioning,
Disability and Health Framework 393
Nordmark, E., Hagglund, 0., & Lagergren, J. (2001b). Cerebral palsy in southem Sweden ll. Gross motor function and disabilities. Acta
Paediatrica, 90(11), 1277-1282.
Odding ,且,Roebroeck, M. E., & Stam, H. J. (2006). The epidemiology of cerebral palsy: lncidence, impairrnents and risk factors.
Disability and rehabilitation, 28(4), 183-191.
0liver, M. (2004). lf 1 had a hammer: the social model in action. ln 1. Swain, S. French, C. Bames &
c.
Thomas (Eds.), Disabling barriers . enabling environments (2 ed., pp. 7-12). London: Sage. Oln句, S. J.,&
Wright, M. (1994). Cerebral palsy. In S. K. Campbell(Ed.), Physical therapy for children (pp. 489-523). Philadelphia: W.B. Saunders company.
Ostensjo, S., Carlberg, E. B., & Vollestad , N. K. (2003). Everyday functioning in young children with cerebral palsy: functional skills, caregiver assistance, and modifications of the environment. Devel中menta/medicine and child neurology, 45( 1 0), 603-612.
Palisano, R. J., Copeland, W. P., & Galup阱,B. E. (2007). Performance of physical activities by adolescents with cerebral palsy. Physica/ therapy, 87(1), 77-87.
Parkes, J., Dolk, H., Hill, N., & Pattenden, S. (2001). Cerebral palsy in Northem lreland: 1981 ?3. Paediatric and perinatal epidemi%gy,
J 5(3), 278-286.
394 成長與茁壯
(1998). Epidemiology of cerebral palsy in England and Scotland,
1984-9. Archives of disease in childhood. Fetal and neonatal
edition, 79, F21-F25.
Pimm, P. (1992). Cerebral palsy: a non progressive disorder?
Educational and child psychology, 9,27-33.
Pivik, J., McComas, J., & Laflamme, M. (2002). 8arriers and
facilitators to inclusive education. Exceptional children, 69( 1),
97-107.
Qiu ,此, Paneth, N., Lorenz, 1.加1., & Col1ins, M. (2003). Labor and
delivery factors in brain damage, disabling cerebral palsy, and
neonatal death in low-birth-weight infants. American journal of
obstetrics and gynecology, 189, 1143-1149.
Quinn, P. (1998). Understanding disability: a lifespan approach.
California: Sage
Read, J. (2000). Disability, the family and society: Iistening to mothers. 8uckingham: Open University.
Rimmer, J. H., Riley, 且, Wang, E., Rauworth, A., & Jurkowski, J.
(2004). Physical activity participation among persons with
disabilities: barriers and facilitators. American journal of
preventive medicine, 26(5),419-425.
Schenker, R., Cost仗, w., & Parush, S. (2005). Participation and activity perforrnance of students with cerebral palsy within the school environment. Disability and rehabilitation, 27(10), 539 - 552.
Exploring Cerebral Palsy from the lntemational Classi 位 cation of Functioning, Disability and Health Framework 395
Schenker, R., Cost仗,帆, & Parush, S. (2006). Persona1 assistance,
adaptations and participation in students with cerebra1 pa1sy mainstreamed in e1ementary schoo1s. Disability and rehabilitation,
28(17),1061-1069.
Scholt郎,紋, Vermeer, A.,
&
Meek, G. (2002). Measuring perceived competence and socia1 acceptance in chi1dren with cerebra1 pa1sy.European Journal 01 Special Needs Education, J 7( 1), 77-87. Schuenge1, C., Voorman, J., Sto1k, J., Dallmeijer, A., Vermeer, A., &
Becher, J. (2006). Se1f-worth, perceived competence, and behaviour prob1ems in chi1dren with cerebra1 pa1sy. Disability and rehabilitation, 28(20), 1251-1258.
Simeonsson, R. 1., Carlson, D., Huntington, G. S., McMillen, J. S., & Brent, J. L. (2001). Students with disabilities: a nationa1 survey of participation in schoo1 activities. Disability and rehabilitation,
23(2),49-63.
Simeonsson, R. J., Leonardi, M., Lollar, D., Bjorck-Akesson, E.,
Hollenweger, J., & Martinuzzi, A. (2003). App1ying the Intemationa1 C1assification of Functioning, Disabi1ity and Health (ICF) to measure chi1dhood disabi1ity. Disability and rehabilitation, 46(11-12), 602-610.
Stan1ey,且, B1air, E., & A1berman, E. (2000). Cerebral palsies:
epidemiology and causal pathways. London: Mac Keith.
396 成長與茁壯
environmental barriers in the United States. Disability and society, 16(1),37-49.
Stevens, S. E., Steele, C. A., Jutai, J. W., Kalni肘,1.叭, Bortolussi, J. A.,
& Bigg缸, W. D. (1996). Adolescents with physical disabilities: some psychosocial aspects of health. Journal 01 adolescent heal的, 19(2),157-164.
Surveillance of Cerebral Palsy in Europe (ECPE). (2002). Prevalence and characteristics of children with cerebral palsy in Europe Developmental medicine and child neurology, 44, 633-640. Thomas, C. (2002). Disability theory: key ideas, issues and thinkers. ln
C. Barn間, M. Oliver & L. Barton (Eds.), Disability studies today
(pp. 38-57). Cambridge: Polity Press in association with Blackwell Publishers.
Turk, M. A., Geremski, C. A., Rosenbaum, P. F., & Weber, R. J. (1997).
The health status of women with cerebral palsy. Archives 01
physical medicine and rehabilitation, 78(Sup 5), sI0-sI7.
Ueda, S., & Okawa, Y. (2003). The subjective dimension offunctioning
and disability: what is it and what is it for? Disability and rehabilitation, 25(11-12), 596-601.
Van der Ploeg, H. P., van der Beek, A. J., van der Woude, L. H. 叭,&
van Mechelen, W. (2004). Physical activity for people with a disability: a conceptual model. Sports Medicine, 34(10),639-649. Voorrnan, J. 悅, Dallmeijer, A. J., Schuen闕,仁, Knol, D. L.,
Exploring Cerebral Palsy from the Intemational Classification of functionin皂,
Disability and Health framework 397
Lankhorst, G. J., & Becher, 1. G. (2006). Activities and
participation of 9- to 13-year-old children with cerebral palsy.
Clinical rehabilitation, 20(11), 937-948
Wanamaker, C. E., & Glenwick, D. S. (1998). Stress, coping, and perceptions of child behavior in parents of preschoolers with
cerebral palsy. Rehabilitation psychology, 的(4) , 207-312.
Williamson, J. B. (2003). Management of the spine in cerebral palsy.
Current orthopaedics
,
17(2),
117-123.World Health Organization. (1980). lnternational classification of
impairments, disabilities and handicaps: a manual of classification
relating to the consequences of disease. Geneva: WHO.
World Health Organization. (2001). Jnternational classification
01
βmctioni嗯" disability and health. Geneva: World Health