Reporters: B101099139 李佳駺 B101099047 黃冠閔 B101099101 曾士剛 Cerebrovasc Dis 2006; 22-225-230 IF:2.723 1
Antiphospholipid antibodies Autoantibodies
Thrombo-occlusive events (IgG isotype)
◦ Cerebrovascular system (most)
aCL↑, stroke patients under 40 years old aCL↑, future stoke↑
Not yet established as an independent risk
factor for ischemic strokes
Case-control study was set up to determine
the association between aCL and ischemic stroke among Taiwanese
Ischemic stroke patients First-ever ischemic stroke < 48 hr onset > 40 years old No cancer No connective tissue disease 1996-1999, Shin Kong WHS Memorial Hospital, Neurological wards
Response rate = 96.5% (n=273)
Pregnancy,systemic lupus erythematosus, transient ischemic attack, venous thrombosis and peripheral vessel thrombosis
Control: outpatients (n=181)
◦ Other than stroke (nonspecific symptoms)
Headache
Musculoskeletal pain
Peripheral vestibulopathy Parkinson’s disease
◦ No cancer or connective tissue disease
Serum specimens centrifuged and frozen ELISA
IgG aCL (GPL) and IgM aCL (MPL) levels:
• Negative(<10GPL <7.5MPL), low positive(10-20GPL 7.5-15MPL), high positive(>20GPL >15MPL)
Demographics and vascular risk factor
◦ X2 test: categorical variables
◦ Two sample t test: continuous variables
Odds ratios:
◦ Stroke risk: high positive aCL vs normal/low
positive aCL
Adjustment (logistic regression):
◦ Model I : not adjusted ◦ Model II : age, sex
◦ Model III : age, sex, smoking, history of deseases
Table 1. Characteristics of the study
participants
T test
There are significant differences in the
proportion of gender, cigarette smoking, hypertension, DM, LVH, A-fib, and
hyperlipidemia between the control group and ischemic stroke patient
* * * * * * * 15
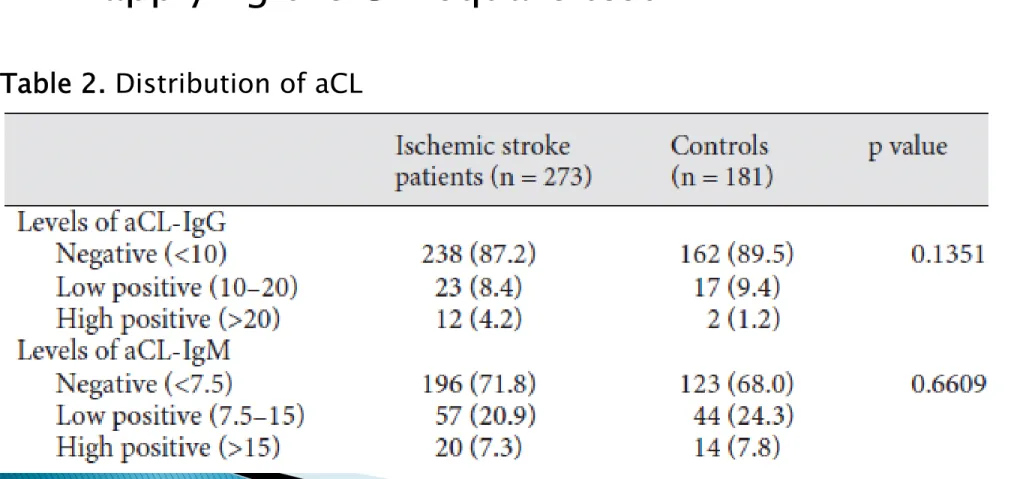
No significant difference between mean
aCL-IgG aCL-IgM is observed applying two sample t test
After stratifying mean aCL-Igs into three
groups, no significant difference is observed applying the Chi square test
Table 2. Distribution of aCL
Determine whether or not subject with high
level of aCL-Igs is more likely to develop ischemic stroke
Blood aCL-IgG>20GPL and aCL-IgM>15MPL
is the cut off point
Ischemic
Stroke
Control
IgG>20
12
2
IgG 20
261
179
OR=
ଵଶൈଵଽ Calculation of 95% CI, taking aCL-IgG as an
example
CI of OR is between 0.091 to 18.595, which
includes 1
Unable to justified that high blood aCL-IgG is
a risk factor for ischemic stroke
Method for calculation for 95% CI is the same
for aCL-IgM
95% CI of aCL-IgM also contains 1, therefore
high aCL-IgM present in blood is not a significant risk factor of ischemic stroke
As previously mentioned, there is significant
different the ratio of gender, smoking status…between the two group
Even age is not significantly different between
two group, it’s widely accepted that advanced age is a risk factor for ischemic stroke
In order to avoid interference, two model is
constructed in order to eliminate these factors
Model 1: Unadjusted
Model 2: Adjusted by age and sex
Model 3:adjusted by age, sex, smoking, and
history of hypertension, DM, A-fib, LVH, and hyperlipidemia
Method for adjustment: Adjusted Logistic
Regression
Framingha m Study
Unadjusted OR can be expressed as:
ln(OR)=β0+βaCL
In the formula above, βaCL represent the effect
of high blood aCL on the risk of developing ischemic stroke
If the CI of βaCL contains 0,calculated OR
( β0+βaCL)is statistically insignificant compare
to the OR ( β0) that did not consider aCL as a
risk factor
In the form of null hypothesis:
H
0: β
0= β
0+ β
aCLβ
aCL= 0
H
1: β
0β
0+β
aCLβ
aCL0
When the CI of β
aCLcontains 0,H
0 In the case of considering smoking status as
a risk factor
Unadjusted formula of OR:
ln(OR)=β0+βaCL
After considering smoking status, formula is
transformed into :
ln(OR)=β’0+β’aCL+β’smoke
The β’aCL in the second formula is the effect
of high blood aCL on the risk of developing ischemic stroke under identical smoking
status
β’aCL and β’smoke have their own CI
If the CI of β’aCL contain 0,no significant
effect of high blood aCL is associate with the risk of developing ischemic stroke under
identical smoking status
OR formula for Model 1:
ln(OR)=β0+βaCL
OR formula for Model 2:
ln(OR)=β’
0+β’aCL+β’age+β’sex
OR formula for Model 3:
ln(OR)=β’’0+β’’aCL+β’’age+β’’sex+…+β’’hyperlipidemi
a
Note: aCL-IgM and aCL-IgG is calculated separately
From Model 2, the 95% CI of β’aCL contains 0
(CI of β’
age and β’sex is unknown)
95% CI of β’’aCL derived from Model 3 (only for
gG) doesn’t contain 0, which imply under identical status (age, sex, smoking status), subject with high aCL-IgG present in blood have a higher odds ratio for developing
The definition above is based on the reviews
of past research (as the following table), and the further Discussions will also compare with this table.
Model I: Unadjusted
Model II: Adjusted by age and sex
Model III: Adjusted by age, sex, smoking,
hypertension, diabetes, atrial fibrillation, left ventricular hypertrophy and hyperlipidemia
Studies of stroke victims under 40 years of
age have found that the studied antibodies are associated with incident ischemic stroke.
Several investigations have provided
conflicting Results with respect to the
significance of elevated aCL levels in older patients.
Table 4. Prevalence of a higher titer of aCL IgG
in non-Asians and Asians
The Framingham study reported that high
aCL levels predict the occurrence of an incident of ischemic stoke.
The Framingham study adjusted for age, prior
Given the fact that multivariate analysis is a
more precise estimation that univariate analysis.
After adjustment for age, sex, smoking,
hypertension, diabetes, atrial fibrillation, left ventricular hypertrophy and hyperlipidemia, ischemic stroke patients aged over 40 years compared to controls. A fivefold increase in stroke risk was also observed.
The Results of this study suggest that
elevated titer of aCL IgG (>20 GPL) is
associated with first-ever ischemic stroke in Taiwanese patients aged over 40 years.
High positive aCL titer is related to ischemic
stroke after adjustment for conventional
cerebrovascular risk factors, indicating that it is probably an independent risk factor for
A separate analysis has demonstrated that
aCL is associated with cerebral stroke and
myocardial infarction, but not with deep vein thrombosis.
37 李碩堯
Q:本篇只有在model III才看到各組間的顯著差異,
model I和model II都沒有看到,那為什麼還要把 model II放進來呢?
A:那是一開始作者的研究順序,原本是想要探討性
別之間的影響,調整之後發現還是沒有顯著差異, 故才進行了第三個model來排除更多risk factor
69謝蓁 Q:為什麼一開始有提到aCL IgM,可是之後的討論 卻只在討論aCL IgG了? A:會把aCL IgM放進來是因為之前別人的實驗都有 個別在探討IgM和IgG的isotype,只是本篇文章最 後都只發現到aCL IgG比較和疾病有相關性所以到 最後就只在探討這部分。其實也和前人的結果符合, 就是aCl IgG 的level對於疾病的影響比較aCL IgM 來的明顯
132李易軒 Q:請問第27頁,238是指人數,旁邊為什麼會有百 分比呢? A:那個並不是百分比,而是標準差,下面的項目才 是百分比。 43
118劉郁欣
Q:為什麼cancer 和connective tissue diseases不
像其他risk factor一樣等到最後再用logistic regression去掉?
A:Cancer 和 connective tissue diseases和其他
risk factor 不一樣,他們是直接影響了aCL的濃度, 所以既然已經知道他們的直接相關性了就直接排除。
老師:覺得本篇論文有什麼可以改進? 士剛:我覺得控制組選得很有爭議,因為沒辦法完 全說有這些疾病的患者,並不會引響此次統計的結 果,而實驗組,若是能一開始就排除心血管因子, 雖然可能有些難度,但是這樣討論就更具意義。 佳駺+冠閔:本篇的IgM和IgG的level是個別探討 的,可以深入探討IgM和IgG的level在同一個病人 上的不同的組合和疾病的相關性(考慮到IgM 和 IgG之間是有可能會有一些相互關係,也可以探討) 45
135劉冠宏
Q:有沒有可能這樣的做法在調整之後,實際上沒有
相關的risk factor也變成有相關?
A:任何的實驗都有可能出現偽陽性的情況,唯有加