The Assessment of Air Pollution Exposure and Paracetamol Use
Related to Children Allergic Disease: A Population-Based Cohort
Study in Taiwan
Wen-Chao Ho, Meng-Hung Lin, Kang-Chih Fan, Tsung-Ta Wu, Hui-Chuan Kao, Pau-Chung Chen,
Trong-Neng Wu, Fung-Chang Sung, Ruey-Shiung Lin
In Taiwan, there are nearly 70 % people living in the urban areas which have more
serious air pollution year by year. It causes that the prevalence of children allergic
disease increases every year. Recently, there are many studies showing that air
pollution is a significant risk factor to cause allergic disease. In Taiwan, paracetamol
is the most common drug to decrease pain, because paracetamol causes less stomach
irritation than aspirin. But there are some studies showing that paracetamol is a risk
factor of allergic disease. The objective of this study is to assess air pollutants
exposure and paracetamol use related to children allergic disease. There were two
databases used in this study: 1) Longitudinal Health Insurance Database 2005
(LHID2005) and 2) Environmental Protection Agency (EPA) air monitoring database.
Geographic Information Systems (GIS) was used in estimating air pollution exposure.
Paracetamol use and children allergic disease records were collected by LHID2005.
Furthermore, we used cox proportion regression models to estimate the relationship
between air pollution, paracetamol use and children allergic disease. The results
showed that air pollution and paracetamol use individually increased the risk of
children allergic disease. Furthermore, patients who were using paracetamol and
exposed to air pollution had more serious effects on children allergic disease. It is
necessary to protect children from the adverse effects of air pollution, especially
considering the potential interaction with paracetamol use.
Keywords: Children allergic disease; Paracetamol; Air pollution; Longitudinal Health
Introduction
Asthma is an important issue in public health. In allergic diseases, asthma, allergic
rhinitis and eczema are related with air pollution exposure in early life. In Taiwan, air
pollution is very serious and the incidence of allergic diseases increases year by year.
It causes huge burden of medical expenses. Therefore, how to verify the
epidemiological risk factors for asthma may be especially important. The air pollution
exposure will increase the amount of inflammatory substances in the human
respiratory tract and increase the risk of asthma and respiratory diseases. Recent
studies indicated that paracetamol drug usage will also cause respiratory tract
inflammation, and induce asthma and respiratory diseases.
Objective
The objective of this study was to investigate the effect of air pollution exposure
and paracetamol drug usage in early life (before one year old) on asthma incidence
during childhood.
Methods
This study was a retrospective cohort study. Children who were born form 2000 to
2004 and exposed to air pollution and postnatal paracetamol drug usage before one
year old was followed up to ages 7-11. This study collected the children’s asthma data
and assessed their residence code thought primary health care outpatient visit location
by Longitudinal Health Insurance Database 2005 (LHID2005). We estimated air
pollutants concentration by Geographic Information Systems (GIS) with air quality
monitoring stations in Taipei. Furthermore we used the nearest 12 monitoring stations
to calculate every district’s air pollutants concentration in Taipei by Inverse Distance Weighting (IDW). At last, we recorded children’s paracetamol usage in exposure
period by LHID 2005.
we used Cox Proportional Hazard Regression Models and adjusted gender, antibiotic,
household income, temperature and relative humidity.
Result
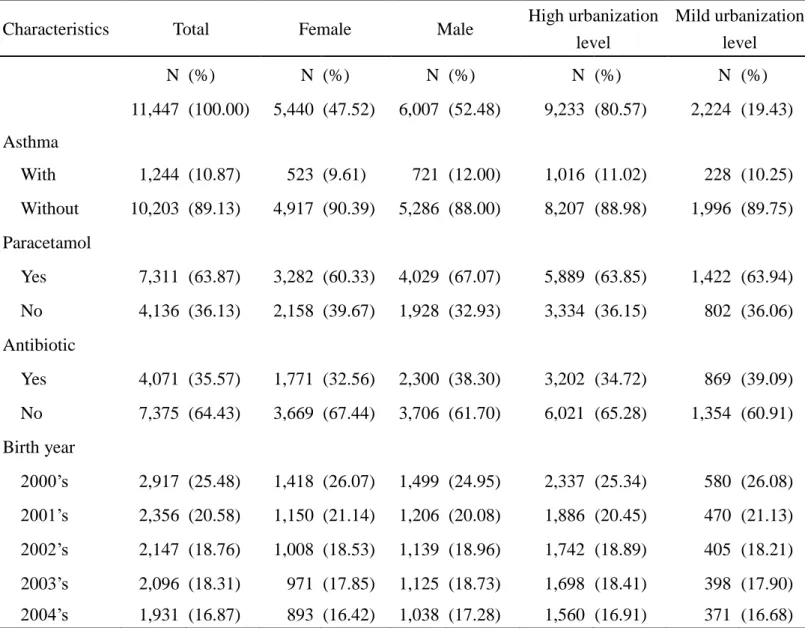
Table 1 showed the demographic variables in this study. There were 10.87%
children developing asthma. More than 60% children had paracetamol exposure in our
study in Taipei. Table 2 showed the Spearman's rank correlation coefficient between
air pollutants. There was high positive correlation coefficient between PM10 and PM2.5.
In addition, there was negative correlation between O3 and other air pollutants. The
effect of air pollutants and paracetamol use on developing asthma showed in table 3
The significant interaction effect was found between PM10 and paracetamol, and
PM2.5 and paracetamol. There was higher risk of children having both paracetamol
use and air pollution exposure. Two pollutants model showed that PM2.5 was
significantly related to asthma only among children with paracetamol use after
adjusting O3 and CO (Table 5).
Discussion and Conclusion
In our finding, air pollution and paracetamol use were both related to children
asthma in Taipei. Furthermore, PM10 and PM2.5 have more consistent results.
Paracetamol use also has significant interaction effect with PM10 and PM2.5 on
developing asthma. The strengths of this study are having complete and
comprehensive drug usage record through LHID 2005. Our subjects are more than
10,000 children. LHID2005 is based on the all population in Taiwan. It may reduce
the possibility of selection bias. However our limitation includes no other
environmental factors like dust, pollen and second hand cigarette exposure in children
early life. Because there aren’t collected in LHID and no national survey data.
In conclusion, children early life exposed to air pollutants and paracetamol will
Avoiding exposure to air pollution during paracetamol use can be important. Wearing
masks in order to reduce air pollution damage to the respiratory tract of children and
Table 1. Characteristic of study population with asthma in Taipei.
Characteristics Total Female Male High urbanization level Mild urbanization level N (%) N (%) N (%) N (%) N (%) 11,447 (100.00) 5,440 (47.52) 6,007 (52.48) 9,233 (80.57) 2,224 (19.43) Asthma With 1,244 (10.87) 523 (9.61) 721 (12.00) 1,016 (11.02) 228 (10.25) Without 10,203 (89.13) 4,917 (90.39) 5,286 (88.00) 8,207 (88.98) 1,996 (89.75) Paracetamol Yes 7,311 (63.87) 3,282 (60.33) 4,029 (67.07) 5,889 (63.85) 1,422 (63.94) No 4,136 (36.13) 2,158 (39.67) 1,928 (32.93) 3,334 (36.15) 802 (36.06) Antibiotic Yes 4,071 (35.57) 1,771 (32.56) 2,300 (38.30) 3,202 (34.72) 869 (39.09) No 7,375 (64.43) 3,669 (67.44) 3,706 (61.70) 6,021 (65.28) 1,354 (60.91) Birth year 2000’s 2,917 (25.48) 1,418 (26.07) 1,499 (24.95) 2,337 (25.34) 580 (26.08) 2001’s 2,356 (20.58) 1,150 (21.14) 1,206 (20.08) 1,886 (20.45) 470 (21.13) 2002’s 2,147 (18.76) 1,008 (18.53) 1,139 (18.96) 1,742 (18.89) 405 (18.21) 2003’s 2,096 (18.31) 971 (17.85) 1,125 (18.73) 1,698 (18.41) 398 (17.90) 2004’s 1,931 (16.87) 893 (16.42) 1,038 (17.28) 1,560 (16.91) 371 (16.68)
Table 2. Correlation coefficients of ambient air pollutants average concentration during exposure period.
PM10 PM2.5 NO NO2 NOX O3 CO SO2 RH Temp PM10 1 0.87 0.49 0.72 0.62 -0.61 0.20 0.66 -0.20 -0.01 PM2.5 1 0.24 0.59 0.41 -0.14 0.11 0.65 -0.32 0.07 NO 1 0.78 0.93 -0.63 0.36 0.18 0.45 0.13 NO2 1 0.92 -0.64 0.36 0.49 0.17 0.26 NOX 1 -0.69 0.41 0.34 0.33 0.19 O3 1 -0.27 -0.16 -0.53 -0.29 CO 1 -0.04 0.10 0.32 SO2 1 -0.21 0.15 RH 1 -0.14 Temp 1
Temp:temperature ; RH:relative humidity ; All P-value < 0.001
Table 3. The hazard ratios and interaction term between air pollution and drug use for asthma children in Taipei.
Pollutant
Model 1 (Main Effect) Model 2
Air pollutants β p-value Paracetamol β p-value p-value for
Interaction term PM10 1.02 (1.00-1.03) 0.015 0.05 1.23 (1.09-1.39) 0.209 <0.001 0.03 PM2.5 1.01 (0.98-1.04) 0.008 0.64 1.24 (1.09-1.40) 0.211 <0.001 0.02 NO 1.01 (1.00-1.02) 0.010 0.03 1.23 (1.09-1.40) 0.211 <0.001 0.41 NO2 1.02 (0.99-1.05) 0.018 0.20 1.24 (1.10-1.40) 0.213 <0.001 0.10 NOx 1.01 (1.00-1.02) 0.008 0.04 1.24 (1.09-1.40) 0.211 <0.001 0.26 O3 1.04 (1.01-1.08) 0.040 0.02 1.23 (1.09-1.39) 0.206 0.001 0.29 CO 1.10 (0.98-1.23) 0.091 0.12 1.23 (1.09-1.39) 0.209 <0.001 0.99 SO2 1.12 (1.01-1.24) 0.113 0.03 1.23 (1.09-1.39) 0.206 0.001 0.15 Model 1: Without interaction term and adjusted sex, temperature, relative humidity, antibiotic and birth year. Model 2: With interaction term
Table 4. Adjusted association between air pollution (per unit in exposure period) and drug use for asthma children: single-pollutant models in Taipei.
Pollutant
Drug exposure (Adjusted HR, 95% CI)
All cases With Paracetamol Without Paracetamol PM10 1.02 (1.00-1.03) 1.02 (1.01-1.04) 1.00 (0.97-1.03) PM2.5 1.01 (0.99-1.04) 1.03 (0.99-1.07) 0.96 (0.91-1.02) NO 1.01 (1.00-1.02) 1.01 (1.00-1.02) 1.01 (0.99-1.03) NO2 1.02 (0.995-1.05) 1.03 (0.998-1.06) 1.00 (0.96-1.05) NOx 1.01 (1.00-1.02) 1.01 (1.00-1.02) 1.01 (0.99-1.02) O3 1.04 (1.01-1.08) 1.03 (0.99-1.07) 1.06 (0.997-1.13) CO 1.11 (0.99-1.24) 1.13 (0.99-1.28) 1.04 (0.82-1.31) SO2 1.12 (1.02-1.24) 1.13 (1.00-1.28) 1.07 (0.89-1.29)
All models adjusted sex, temperature, relative humidity, antibiotic and birth year.
Table 5. Adjusted association between air pollution (per unit in exposure period) and drug use for asthma children: two-pollutant models for PM2.5 in Taipei.
Pollutant Drug exposure (Adjusted HR, 95% CI)
All cases With Paracetamol Without Paracetamol PM2.5 With NO 0.996 (0.97-1.02) 1.02 (0.98-1.05) 0.95 (0.91-1.00) PM2.5 With NO2 0.99 (0.95-1.03) 1.01 (0.97-1.06) 0.94 (0.87-1.00) PM2.5 With NOx 0.99 (0.96-1.02) 1.01 (0.98-1.05) 0.94 (0.89-0.997) PM2.5 With O3 1.03 (0.99-1.06) 1.05 (1.01-1.09) 0.98 (0.92-1.04) PM2.5 With CO 1.01 (0.98-1.04) 1.03 (1.00-1.06) 0.96 (0.92-1.01) PM2.5 With SO2 0.99 (0.96-1.02) 1.01 (0.97-1.06) 0.94 (0.89-1.00) All models adjusted sex, temperature, relative humidity, antibiotic and birth year.