Corresponding author: Chia-Hua Kuo, Ph.D., Laboratory of Exercise Biochemistry, Taipei Physical Education College, 101, Sec. 2, Jhongcheng Rd., Shihlin District, Taipei City 11153, Taiwan, Republic of China. Tel: +886-2-28718288 ext. 5101, Fax: +886-2-28753383, E-mail: [email protected]
Received: January 19, 2009; Revised: September 24, 2009; Accepted: October 7, 2009.
2010 by The Chinese Physiological Society. ISSN : 0304-4920. http://www.cps.org.tw
Effects of One-Year Swimming Training on
Blood Pressure and Insulin Sensitivity in Mild
Hypertensive Young Patients
Hsiu-Hua Chen1, Yi-Liang Chen1, Chih-Yang Huang2, 3, Shin-Da Lee4, Shih-Chang Chen1, and Chia-Hua Kuo1
1Laboratory of Exercise Biochemistry, Taipei Physical Education College, Taipei 2Graduate Institute of Basic Science, China Medical University, Taichung 3Department of Health and Nutrition Biotechnology, Asia University, Taichung
and
4Graduate Institute of Physical Therapy, China Medical University, Taichung Taiwan, Republic of China
Abstract
Swimming is a lifestyle intervention recommended by many clinicians in the prevention and treatment of hypertension. Yet, not all studies have agreed that swimming training can reduce blood pressure (BP). Inclusion of normotensive subjects could be a confounder for discrepancies among studies. In this one-year longitudinal study, long-term effects of swimming training on BP were investigated in 7 mild hypertensive patients (systolic BP (SBP) > 140 mmHg) and 16 normotensive controls. At baseline, these subjects (aged 21.5 ± 0.1 years) did not participate in any form of sport training activity for the previous 3 months before enrollment into the training program. The training distance progressed from 0 (baseline) to 7 kilometers per week. BP and the homeostasis model assessment for insulin resistance (HOMA-IR) were determined under fasted condition at baseline and 48 h after the last swimming bout. The hypertensive patients displayed significantly greater HOMA-IR than age-matched normotensive controls. When data of all subjects were pooled, plasma glucose concentration was only slightly lowered after training, but weight, height, body mass index, SBP, diastolic BP (DBP) and HOMA-IR values were not significantly altered. However, when observation was restricted to the hypertensive patients, swimming training significantly lowered SBP by ~17 mmHg, concurrent with 41% reduction in HOMA-IR. Intriguingly, SBP in the normotensive subjects was elevated by ~ 6 mmHg after training. Conclusions: The present study found normalization rather than universal reduction effect of swimming training on BP. Furthermore, the BP-lowering effect of training in hypertensive patients appears to be associated with improvement in insulin sensitivity.
Key Words: glucose tolerance, hypertension, insulin resistance, insulin sensitivity, HOMA-IR, systolic BP, diastolic BP, exercise training
Introduction
Individuals with high blood pressure in early lifetime have greater chances to develop hypertension in later adulthood (7). Swimming is a recommended training mode in the prevention of development of
hypertension, which is largely based on evidence from studies using other forms of aerobic exercise (10). Few studies have determined specifically intervention effects of long-term swimming training on resting BP. One early study performed in middle-aged hypertensive subjects with 10-week swimming
training has reported only 2% drop in BP which cannot be considered an impressive outcome by clinicians and patients (29). Another study reported significantly elevations in BP for normotensive women after swimming training (8). However, intervention studies using other modes of exercise training to reduce BP have also generated inconsistent results (8, 9, 14, 17). In contrary, most epidemiological evidences have consistently shown the benefit of exercise train-ing on BP (2). One possibility that may account for this discrepancy can be the inclusion of normoten-sive subjects.
Insulin resistance has been proposed as a patho-genic origin in the development of hypertension (1, 21, 27, 28). Interventions that increase insulin sensi-tivity can lower BP supports this causal relationship (30). Increasing physical activity is generally known as an effective intervention for enhancing insulin sensitivity (13). Previous reports have suggested that the homeostasis model assessment of insulin resis-tance (HOMA-IR) serves as an important factor in the etiology of hypertension for both adults and children (16, 21). In this study, we evaluated one-year swim-ming training effect on BP with inclusion of 7 mild hypertensive patients and 16 normotensive age-matched subjects. Their HOMA-IR and weight status were also recorded before and 48 h after the last swimming bout.
Materials and Methods Human Subjects
A total of 23 young participants with an average age of 21.5 ± 0.1 years, including 7 mild hypertensive patients and 16 normotensive age-matched subjects, voluntarily enrolled in this one-year swimming training. Subjects were initially screened according to their basic swimming capability. All subjects were capable of swimming for more than 800 meters. This study was approved by the institutional ethical com-mittee and the subjects gave informed consents.
Intervention
These subjects remained sedentary for at least 3 months before beginning of the intervention. Swim-ming training started from the first year of college and the swimming distance progressively increased from 0 to 7 kilometers.
Measurements
All measurements were performed before and 1 year after the swimming training, 48 h following the last swimming bout and under fasted condition in the
morning. Measurements consisted of anthropometric assessments (height, weight), glucose, insulin and BP determination. Systolic (first phase) and diastolic (fifth phase) BP were measured by auscultation with a mercury column sphygmomanometer in the seated position after a 5-min rest period. The mean of 2 determinations was used for BP measurement before blood sample collection.
Plasma glucose and insulin were measured with-in 3 h followwith-ing sample collection (15). Glucose concentration was determined using the method of glucose oxidase. Insulin was determined using the method of ELISA with a commercial kit (Diagnostic Systems Laboratories, Inc. Webster, TX, USA). In-sulin resistance was determined according to the HOMA-IR as the product of fasting plasma glucose (mM) and insulin (µU/ml) divided by the constant 22.5 (3).
Statistical Analysis
Paired t test was used to determine the mean differences between baseline and post-training values on all metabolic and anthropometric variables. Two-way ANOVA with repeated measurements was used to determine the interactive effects of initial BP and time on all variables. Fisher post-hoc test was used to compare mean differences between groups. Pearson correlation was used to determine the association between baseline and the magnitude of change on metabolic variables. A level of P < 0.05 was con-sidered significant on all tests, and all values are ex-pressed as means ± standard errors (SE).
Table 1. Characteristics of subjects
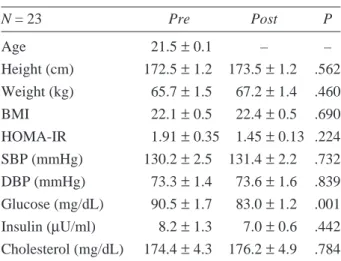
N = 23 Pre Post P Age 21.5± 0.1 – – Height (cm) 172.5± 1.2 173.5 ± 1.2 .562 Weight (kg) 65.7± 1.5 67.2± 1.4 .460 BMI 22.1± 0.5 22.4± 0.5 .690 HOMA-IR 1.91± 0.35 1.45 ± 0.13 .224 SBP (mmHg) 130.2± 2.5 131.4 ± 2.2 .732 DBP (mmHg) 73.3± 1.4 73.6± 1.6 .839 Glucose (mg/dL) 90.5± 1.7 83.0± 1.2 .001 Insulin (µU/ml) 8.2± 1.3 7.0± 0.6 .442 Cholesterol (mg/dL) 174.4± 4.3 176.2 ± 4.9 .784
P, probability of type I error for the difference between
initial value and post-training value. Abbreviations: BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure, HOMA-IR, homeostasis model assessment for insulin resistance.
Results
Table 1 shows anthropometric and metabolic variables at baseline and following one year of swimming training with inclusion of all subjects. Weight, height, BMI, DBP and HOMA-IR values were not significantly altered with the one-year swimming training. Fasting plasma glucose level was slightly reduced after training (P < 0.05). Blood pressure data are shown in Fig. 1 (SBP) and Fig. 2
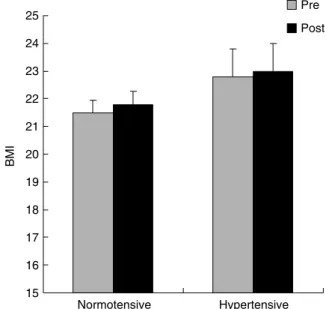
(DBP). Body mass index (BMI) was not affected by swimming training for both normotensive subjects and hypertensive patients (Fig. 3). HOMA-IR data are shown in Fig. 4. SBP, DBP and HOMA-IR in the hypertensive group were significantly greater than those in the normotensive group (P < 0.05). Swim-ming training significantly lowered SBP and HOMA-IR in the hypertensive group (P < 0.05). However, for the normotensive subjects, SBP was significantly elevated from 124 to 130 mmHg (P < 0.05).
Fig. 3. BMI after one-year swimming training.
25 24 23 22 21 20 19 18 17 16 15 Normotensive Hypertensive BMI Pre Post 160 150 140 130 120 110 100 Normotensive Hypertensive SBP (mmHg) Pre Post † * †
Fig. 1. Systolic BP after one-year swimming training. *Signifi-cance against normotensive control; †Significance against Pre. 85 80 75 70 65 60 55 50 DBP (mmHg) Pre Post * * Normotensive Hypertensive
Fig. 2. Diastolic BP after one-year swimming training. *Sig-nificance against normotensive control.
3 2.5 2 1.5 1 0.5 1 Normotensive Hypertensive HOMA-IR Pre Post * †
Fig. 4. HOMA-IR after one-year swimming training. *Signifi-cance against normotensive control; †Significance against Pre.
Discussion
Swimming is a recommended intervention in the prevention and treatment of hypertension. How-ever, previous studies reported inconsistent results on positive training effects of swimming on resting BP (8, 29). In the study, we found a significant BP lower-ing effect of swimmlower-ing trainlower-ing for mild hypertensive young patients. However, swimming training slightly elevated SBP in the normotensive subjects. Such opposing trend towards normal values of BP brought no significant change in BP by training when data from all subjects were pooled. Thus, the present study demonstrates a normalization effect, rather than a reduction effect, of swimming training on resting BP. Such a finding might explain the inconsistent results of swimming training on resting BP from previous studies (8, 9, 14, 17), and reconfirms the benefit of exercise training on suppressing eccentric BP towards normal. One factor that is causally linked with hy-pertension is the weight status (9, 24). In this study, the mean BMI of the subjects was not altered by swimming training in the hypertensive subjects. This indicates that the training effect on BP reduction was not associated with changes in weight status for this cohort. This is not surprising sine it has been pre-viously found in young adults that the percentages of the variance of BP that could be explained by BMI were less than 15% (33). Other factors, such as in-creases in muscle mass (5), could be involved with the change of BP by swimming training in the study. This might be due to changes in body composition rather than weight fluctuation (22, 23).
Hypertension is a part of insulin resistance syndromes in humans (27). In the study, we also found that the training effect on HOMA-IR was highly correlated with their initial values. HOMA-IR is a surrogate measure of insulin resistance (4) based on glucose-insulin feedback system in the homeostatic state (overnight fasting) (31). Intervention that en-hances insulin sensitivity can alleviate hypertension, whereas hypertensive medicine could not reverse insulin resistance (27). This highlights a causal relationship between BP and insulin resistance. The fact that the training effect on insulin sensitivity oc-curred without altering weight status is consistent with a previous study reported for younger ages (25). The similar trend in the relationships between training effect on BP and HOMA-IR and their initial values suggests a possibility that the beneficial effect of swimming training could be mediated by increased responsiveness in endothelium-dependent vasodila-tion, which is highly associated with insulin sensitivity (34). Type 2 diabetes patients are characterized by a significantly blunted vasodilator response to insulin as well as an attenuated effect of insulin in decreasing
vascular resistance (18, 28). Furthermore, increased protein glycation (formation of advanced glycation end products) due to hyperglycemia is increasingly recognized to be linked with insulin resistance. Modification of endogenous proteins could lead to non-specific inflammatory responses, which in turn increase oxidative stress and cause vasculature damage (32). As a result, endothelial dysfunction and reduced capillary density in periphery develop (11), and thus contributes to increased blood pressure. Although the training effect on reducing HOMA-IR has been confirmed in numerous studies (20, 25, 26), the additional knowledge provided by this study is that the swimming training effect is more pronounced for individuals with initially lower insulin sensitivity in this young cohort.
The present study found that swimming training significantly increased SBP in normotensive subjects. One possibility accounting for increased BP in nor-motensive subjects is the normal training effect on in-creasing plasma volume. An acute bout of exercise can increase plasma volume within a day (12) which might improve hypotension for those initially low BP subjects but not for normotensive individuals. Low plasma volume is generally known as a major cause of hypotension (19). The plasma volume expansion phenomenon of training is related to increase in al-bumin synthesis (6) which leads to greater water re-tention in circulation. Furthermore, the exercise mode appears to be important for the BP lowering effect of exercise training. Cox et al. (8) have found that, re-lative to walking, regular swimming significantly elevates BP in previously sedentary, normotensive subjects.
In conclusion, previous studies have reported inconsistent findings with regard to swimming training effect on resting BP. This discrepancy could be due to inclusion of normotensive subjects based on the current finding that an elevated BP with training re-stricted only to the normotensive young subjects, whereas hypertensive subjects exhibited an opposing change. The results of the study demonstrate that long-term swimming training can normalize BP and HOMA-IR towards norm for young adults. The benefit of swimming training on resting BP is, thus, recon-firmed in the study.
Acknowledgments
This study is partly sponsored by the grant from National Science Council, grant number NSC 96-2413-H-154-003-MY3.
References
Skeletal muscle blood flow: a possible link between insulin resis-tance and blood pressure. Hypertension 21: 129-135, 1993. 2. Bjorntorp, P. Effects of physical training on blood pressure in
hypertension. Eur. Heart J. 8: 71-79, 1987.
3. Bonora, E., Formentini, G., Calcaterra, F., Lombardi, S., Marini, F., Zenari, L., Saggiani, F., Poli, M., Perbellini, S., Raffaelli, A., Cacciatori, V., Santi, L., Targher, G., Bonadonna, R. and Muggeo, M. HOMA-estimated insulin resistance is an independent predictor of cardiovascular disease in type 2 diabetic subjects: prospective data from the Verona Diabetes Complications Study. Diabetes Care 25: 1135-1141, 2002.
4. Bonora, E., Targher, G., Alberiche, M., Bonadonna, R.C., Saggiani, F., Zenere, M.B., Monauni, T. and Muggeo, M. Homeostasis model assessment closely mirrors the glucose clamp technique in the assessment of insulin sensitivity: studies in subjects with various degrees of glucose tolerance and insulin sensitivity. Diabetes Care 23: 57-63, 2000.
5. Chen, C.H., Liu, Y.F., Lee, S.D., Lee, W.C., Tsai, Y.L., Hou, C.W., Huang, C.Y. and Kuo, C.H. Altitude hypoxia increases glucose uptake in human heart. High Alt. Med. Biol. 10: 83-86, 2009. 6. Convertino, V.A., Greenleaf, J.E. and Bernauer, E.M. Role of
thermal and exercise factors in the mechanism of hypervolemia. J. Appl. Physiol. 48: 657-664, 1980.
7. Cook, N.R., Gillman, M.W., Rosner, B.A., Taylor, J.O. and Hennekens, C.H. Prediction of young adult blood pressure from childhood blood pressure, height, and weight. J. Clin. Epidemiol. 50: 571-579, 1997.
8. Cox, K.L., Burke, V., Beilin, L.J., Grove, J.R., Blanksby, B.A. and Puddey, I.B. Blood pressure rise with swimming versus walking in older women: The sedentary women exercise adherence trial 2 (SWEAT 2). J. Hypertens. 24: 307-314, 2006.
9. Cox, K.L., Puddey, I.B., Morton, A.R., Burke, V., Beilin, L.J. and McAleer, M. Exercise and weight control in sedentary overweight men: effects on clinic and ambulatory blood pressure. J. Hypertens. 14: 779-790, 1996.
10. Fagard, R.H. Exercise is good for your blood pressure: Effect of endurance training and resistance training. Clin. Exp. Pharmacol. Physiol. 33: 853-856, 2006.
11. Frisbee, J.C. Hypertension-independent microvascular rarefaction in the obese Zucker rat model of the metabolic syndrome. Micro-circulation 12: 383-392, 2005.
12. Gillen, C.M., Lee, R., Mack, G.W., Tomaselli, C.M., Nishiyasu, T. and Nadel, E.R. Plasma volume expansion in humans after a single intense exercise protocol. J. Appl. Physiol. 71: 1914-1920, 1991. 13. Hamburg, N.M., McMackin, C.J., Huang, A.L., Shenouda, S.M., Widlansky, M.E., Schulz, E., Gokce, N., Ruderman, N.B., Keaney, J.F., Jr. and Vita, J.A. Physical inactivity rapidly induces insulin resistance and microvascular dysfunction in healthy volunteers. Arterioscler. Thromb. Vasc. Biol. 27: 2650-2656, 2007. 14. Hansen, H.S., Froberg, K., Hyldebrandt, N. and Nielsen, J.R. A
controlled study of eight months of physical training and reduction of blood pressure in children: the Odense schoolchild study. Brit, Med. J. 682-685, 1991.
15. Hsu, T.H., Lee, S.D., Fang, C.L., Lee, J.P., Chen, F.T., Huang, Y.J., Chen, Y.L., Liu, T.C. and Kuo, C.H. Age-dependent increase in insulinemia under glucose challenge is suppressed in early middle-aged females. Chinese J. Physiol. 51: 263-268, 2008. 16. Kanauchi, M., Yamano, S., Kanauchi, K. and Saito, Y.
Homeosta-sis model assessment of insulin reHomeosta-sistance, quantitative insulin sensitivity check index, and oral glucose insulin sensitivity index in nonobese, nondiabetic subjects with high-normal blood pressure. J. Clin. Endocrinol. Metab. 88: 3444-3446, 2003.
17. Kelley, G.A., Kelley, K.S. and Tran, Z.V. The effects of exercise
on resting blood pressure in children and adolescents: a meta-analysis of randomized controlled trials. Prev. Cardiol. 6: 8-16, 2003.
18. Laakso, M., Edelman, S.V., Brechtel, G. and Baron, A.D. Impaired insulin-mediated skeletal muscle blood flow in patients with NIDDM. Diabetes 41: 1076-1083, 1992.
19. Laederach-Hofmann, K., Weidmann, P. and Ferrari, P. Hypov-olemia contributes to the pathogenesis of orthostatic hypotension in patients with diabetes mellitus. Am. J. Med. 106: 50-58, 1999. 20. Lai, Y.C., Chen, C.Y. and Kuo, C.H. Exercise and type 2 diabetes.
Adapt. Med. 1: 1-16, 2009.
21. Lissner, L., Bengtsson, C., Lapidus, L., Kristjansson, K. and Wedel, H. Fasting insulin in relation to subsequent blood pressure changes and hypertension in women. Hypertension 20: 797-801, 1992. 22. Liu, T.C., Kuo, C.H. and Wang, P.S. Exercise and testosterone.
Adapt. Med. 1: 24-29, 2009.
23. Liu, T.C., Liu, Y.Y., Lee, S.D., Huang, C.Y., Chien, K.Y., Cheng, I.S., Lin, C.Y. and Kuo, C.H. Effects of short-term detraining on measures of obesity and glucose tolerance in elite athletes. J. Sports Sci. 26: 919-925, 2008.
24. Miyamatsu, N., Kadowaki, T., Okamura, T., Hayakawa, T., Kita, Y., Okayama, A., Nakamura, Y., Oki, I. and Ueshima, H. Different effects of blood pressure on mortality from stroke subtypes depend-ing on BMI levels: a 19-year cohort study in the Japanese general population-NIPPON DATA80. J. Hum. Hypertens. 19: 285-291, 2005.
25. Nassis, G.P., Papantakou, K., Skenderi, K., Triandafillopoulou, M., Kavouras, S.A., Yannakoulia, M., Chrousos, G.P. and Sidossis, L.S. Aerobic exercise training improves insulin sensitivity without changes in body weight, body fat, adiponectin, and inflammatory markers in overweight and obese girls. Metabolism 54: 1472-1479, 2005.
26. O’Donovan, G., Kearney, E., Nevill, A., Woolf-May, K. and Bird, S. The effects of 24 weeks of moderate- or high-intensity exercise on insulin resistance. Eur. J. Appl. Physiol. 95: 522-528, 2005. 27. Reaven, G.M. Role of insulin resistance in human disease.
Dia-betes 37: 1595-1607, 1988.
28. Skarfors, E.T., Lithell, H.O. and Selinus, I. Risk factors for the development of hypertension: a 10-year longitudinal study in middle-aged men. J. Hypertens. 9: 217-223, 1991.
29. Tanaka, H., Bassett, D.R., Howley, E.T., Thompson, D.L., Ashraf, M. and Rawson, F.L. Swimming training lowers the resting blood pressure in individuals with hypertension. J. Hypertens. 15: 651-657, 1997.
30. Usui, I., Fujisaka, S., Yamazaki, K., Takano, A., Murakami, S., Yamazaki, Y., Urakaze, M., Hachiya, H., Takata, M., Senda, S., Iwata, M., Satoh, A., Sasaoka, T., Ak, N.D., Temaru, R. and Kobayashi, M. Telmisartan reduced blood pressure and HOMA-IR with increasing plasma leptin level in hypertensive and type 2 diabetic patients. Diabetes Res. Clin. Pract. 77: 210-214, 2007. 31. van Haeften, T.W. Glucose tolerance, insulin sensitivity, and the
homeostasis model assessment method. Diabetes Care 21: 673-674, 1998.
32. Vasdev, S., Gill, V. and Singal, P. Role of advanced glycation end products in hypertension and atherosclerosis: therapeutic im-plications. Cell. Biochem. Biophys. 49: 48-63, 2007.
33. Vinck, W.J., Vlietinck, R. and Fagard, R.H. The contribution of genes, environment and of body mass to blood pressure variance in young adult males. J. Hum. Hypertens. 13: 191-197, 1999. 34. Wendelhag, I., Fagerberg, B., Hulthe, J., Bokemark, L. and
Wikstrand, J. Endothelium-dependent flow-mediated vasodilatation, insulin resistance and the metabolic syndrome in 60-year-old men. J. Intern. Med. 252: 305-313, 2002.