Association of Color Doppler Vascular ity Index and
Micr ovessel Density with Sur vival in Patients with Gastr ic
Cancer
Mini Abstr act
In order to evaluate the clinical usefulness of the color Doppler vascularity (CDVI) in patients with gastric cancer, seventy-nine gastric cancer patients were studied with microvessel density. Among them, tumors were sonographically visible in thirty-one patients. Vascular invasion and CDVI were independent prognostic factors. CDVI was also a good preoperative indicator of early death in stage III gastric cancer patients. Thus, CDVI may be helpful in selecting patients with gastric cancer for neoadjuvant chemotherapy and/or anti-angiogenic therapy.
Abstr act
Objective
The purpose of this study was to investigate the clinical usefulness of microvessel density (MVD) and an in vivo angiogenesis parameter, color Doppler vascularity
index (CDVI), in patients with gastric cancer.
Summar y Backgr ound Data
Many studies have reported a significant association between the degree of MVD-evaluated angiogenesis with the clinicopathologic factors and prognosis of patients with various solid tumors. All these studies were accomplished on tissue sections retrospectively obtained from surgical specimens. However, an “in vivo” method to
assess tumor angiogenesis for human malignancies is highly desirable for diagnostic purpose, treatment planning and follow-up. The CDVI is a new ultrasound parameter for evaluating in vivo angiogenesis, and has a good
correlation with status of lymph node metastasis in cervical carcinoma, and can predict distant metastasis and survival in colon cancer patients. Therefore, the CDVI may also be useful to assess in vivo angiogenesis in human gastric cancer.
Methods
A total of 79 patients with gastric cancer were enrolled in this study, and microvessel density was evaluated by using immunohistochemical staining of surgical specimens with anti-CD-34 antibody. Tumors were sonographically visible in thirty-one patients. The CDVI of each tumor was determined using transabdominal color Doppler ultrasound. The CDVI was defined as the ratio of the number of the colored pixels within a tumor section to the number of total pixels in that specific tumor section, and was calculated by using Encomate
software (Electronic Business Machine Co. Ltd., Taipei, Taiwan). Correlation between MVD, CDVI and clinicopathologic factors and patient survival was studied.
Results
The MVD was significantly correlated with vascular invasion by multiple linear regression analysis. Although the survival of patients with high MVD (>32) was significantly worse than those with low MVD (<32) by univariate analysis, vascular invasion was an independent prognostic factor by Cox proportional hazard model. There was a linear correlation between CDVI and MVD (r=0.495, p=0.005). Moreover, in patients with a high CDVI (> 11%), the survival rate was significantly lower than that in those with low CDVI (≦11%) (p=0.005). None of the patients with high CDVI (>11%) survived 2 years after curative resection. In addition to vascular invasion, the CDVI was another independent prognostic factor in the patients with stage III gastric cancer.
Conclusions
Vascular invasion was an important prognostic indicator in gastric cancer. The high CDVI was a good preoperative indicator of early death in stage III gastric cancer patients. Thus, the CDVI may be helpful in selecting patients with gastric cancer for neoadjuvant chemotherapy and/or anti-angiogenic therapy.
Introduction
Angiogenesis is a very complex phenomenon and essential for the growth of solid tumors measuring more than a few millimeters.1 It permits rapid tumor growth and potential presence of tumor metastasis.2,3 It is not easy to develop a single method capable of detecting such a complex biological phenomenon. At present the most widely used method to assess angiogenesis in human malignancies is the quantification of microvessel density (MVD) of tumors using specific markers for endothelial cells including factor VIII-related antigen, CD31 and CD34.4-11 These studies have reported an association between the degree of angiogenesis, and the clinicopathologic factors and prognosis of patients with various solid tumors, such as breast,4-6 lung,7 prostate,8 head and neck,9 and gastrointestinal cancer.10,11 All these studies were accomplished on tissue sections retrospectively obtained from surgical specimens. However, an “in vivo” method
to assess tumor angiogenesis for human malignancies is highly desirable for diagnostic purpose, treatment planning and follow-up.
With the current technique of color Doppler sonography, tumor vascularity can be assessed in vivo.12 The correlation of the color Doppler vascular signals with the angiographic and histologic findings has also been shown in tumors of various human organs.13,14 Incremental angiogenesis could be demonstrated in the tumorigenesis of ovarian and endometrial malignancies with color Doppler ultrasound.15,16 Vascularity index is a new ultrasound parameter for evaluating in vivo angiogenesis. Several reports has revealed that vascularity index could be used to differentiate the nature of neck lymph node17 and had a good correlation with status of lymph node metastasis in cervical carcinoma.18 Conventional transabdominal sonography has become increasingly important not only in
evaluating diseases of solid organ but also in diagnosis of the gastrointestinal diseases.19-21 Recently, we also found that color Doppler vascularity index (CDVI) can predict distant metastasis and survival in colon cancer patients.22 Therefore, the CDVI may also be used to assess in vivo angiogenesis in human gastric cancer. To investigate the clinical usefulness of the CDVI and MVD in gastric cancer, this study was conducted to elucidate the correlation between CDVI and MVD, and evaluate association between these two angiogenesis parameters and clinicopathological factors and survival in patients with sonographically visible gastric cancer.
Patients and Methods
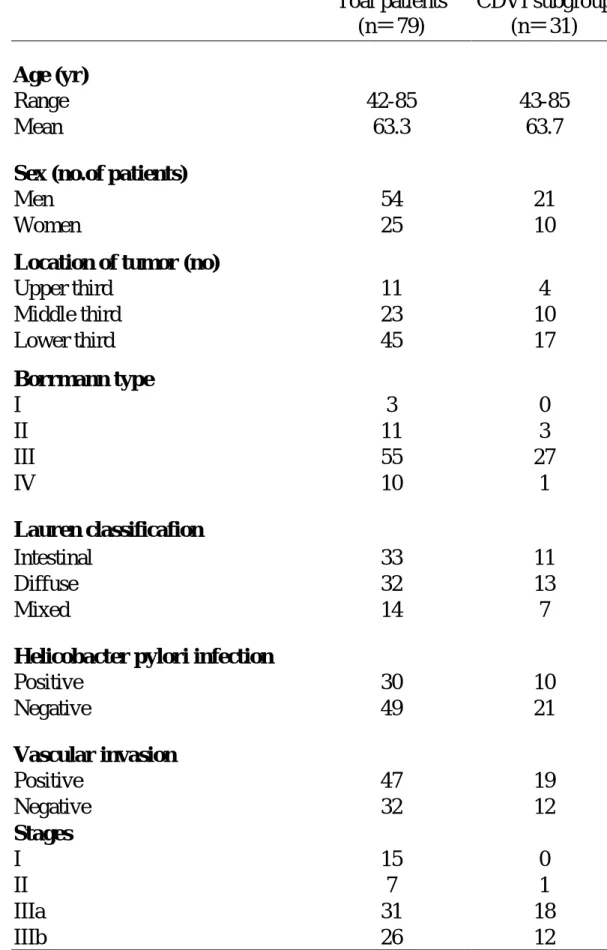
Patients. A total of 79 patients with gastric cancer, who had undergone radical gastrectomy at our institution from July 1995 to March 1999, were included in this study. They were all proved to have adenocarcinomas by panendoscopic biopsies. They were staged according to TNM system. Criteria for consideration as curative resection were the complete removal of a primary gastric tumor, D2 dissection of regional lymph nodes, and no macroscopic tumor being left behind. They had no detectable metastasis in liver, peritoneum and distant organ at the time of surgery. No other previous or concomitant primary cancer was present. Abdominal ultrasound was performed before operation to evaluate liver and other intraperitoneal metastases routinely without hydrogastric preparation after overnight fasting. The tumor mass of gastric cancer could be clearly delineated by trans-abdominal ultrasound in 31 patients (39%) who constituted a subpopulation of this study. These 31 patients ranged in age from 43 to 85 years (average age, 63.7 years); 21 were men and 10 were women. Clinicopathological characteristics were similar between original group and CDVI subgroup. All patients in CDVI subgroup had stage III disease except one whose disease was stage II (Table 1). No patient had received chemotherapy and radiotherapy before surgery. Clinicopathologic factors including age, sex, gross types of tumors (Borrmann classification), histologic types of tumors (Lauren classification), depth of tumor invasion, status of lymph node metastasis, vascular invasion, and Helicobacter pylori (H. pylori) infection documented with histologic findings were reviewed and stored in patients’ data base. Vascular invasion was considered to be definite only when tumor cells and red blood cells were noted together in an endothelium-lined vascular space or when tumor cells were found in an endothelium-lined vascular
space with a definite smooth muscle layer. The tissue were considered positive for H. pylori if faintly blue staining curved bacilli were seen in the mucus of crypts just adjacent to tumor using hematoxylin and eosin stain. The patients were followed up from 3 to 46 months after sugery. The follow-up intervals were calculated as survival intervals after surgery.
Sonographic Technique and Quantification of Vascular Density in Color Doppler Images17, 18, 22 . The scanner we used was a color Doppler ultrasound unit (HDI 3000 or 5000, Advanced Technology Laboratories, Bothell, WA) with a 2-5 MHz curved array or a 5-10 MHz linear array transducers. Settings of the color Doppler ultrasound were standardized for the highest sensitivity in the absence of apparent noise by using a medium wall filter, pulsed repetition frequency of 1000 Hz, color gain of 78-79%, moderate-to-long persistence, and a slow sweep technique. Under these conditions, the lowest possible measurable velocity was claimed below 5 cm/second. Focusing depth was set between 1.5 and 5 cm. Each tumor was scanned thoroughly and tangential scanning was made to avoid the intraluminal air interference as possible as we can. The color window was set to cover the whole tumor on the screen. The tumor of the gastric cancer was then scanned carefully in all directions and the tumor section with subjectively maximal color signals was captured and stored for later analysis. Each tumor was scanned three times, thus three tumor sections with maximal color signals were available for quantatitive analysis. After the examination, the previously stored images were retrieved and displayed on the monitor. The tumor margin was contoured using a cursor. Quantification of the vascular color signals within the demarcated tumor area was then automatically performed using the special software (Encomate, Electronic Business Machine Co., Ltd., Taiwan). The results were expressed as the "color
Doppler vascularity index (CDVI)" (the number of colored pixels within the tumor section /the number of total pixels in that particular tumor section) (Fig. 1). For each tumor, the mean of the CDVI of three representative tumor sections was used for statistical analysis.
Microvessel Staining and Evaluation. The paraffinized tumor blocks of 79 patients whose gastric cancers were stained for endothelial cell CD34 antigen using the labelled streptavidin-biotin after antigen retrieval (Fig. 2). Briefly, deparaffinized sections were heated in a pressure cooker. After endogenous peroxidase was blocked with 3% hydrogen peroxide in the section, each section was incubated with nonimmuned horse serum. The sections were incubated in anti-CD34 monoclonal antibody (Santa Crus, CA) at a dilution of 1:20, or the control nonimmune serum at 4 ℃ overnight. The sections were incubated with link antibodies followed by peroxidase conjugated streptavidin complex (LSAB kit, DAKO Corporation, Carpinteria, CA). The peroxidase activity was visualized with diaminobenzidine tetrahydroxychioride solution (DAB, DAKO corporation, Carpinteria, CA) as the substrate. The sections were lightly counterstained with hematoxylin. After screening the areas with intense neovascularized spots at low power field (100X), microvessels in the area with the highest number of discrete microvessels were counted in a 400X field. Three separate intense neovascularized areas were assessed, and the mean was calculated as microvessel density of each tumor evaluated.
Statistics. The relationship between MVD, CDVI and the various clinicopathologic factors was examined by chi-square test. One-way ANOVA was used to test the correlation among different TNM stages. Survival curves were calculated using the Kaplan-Meier method and analyzed by the log-rank test. The
CDVI and clinicopathologic variables influencing survival was assessed by the Cox proportional hazards model. The mode of recurrence was examined by Fisher exact test. Statistical significance was defined as p < 0.05.
Results
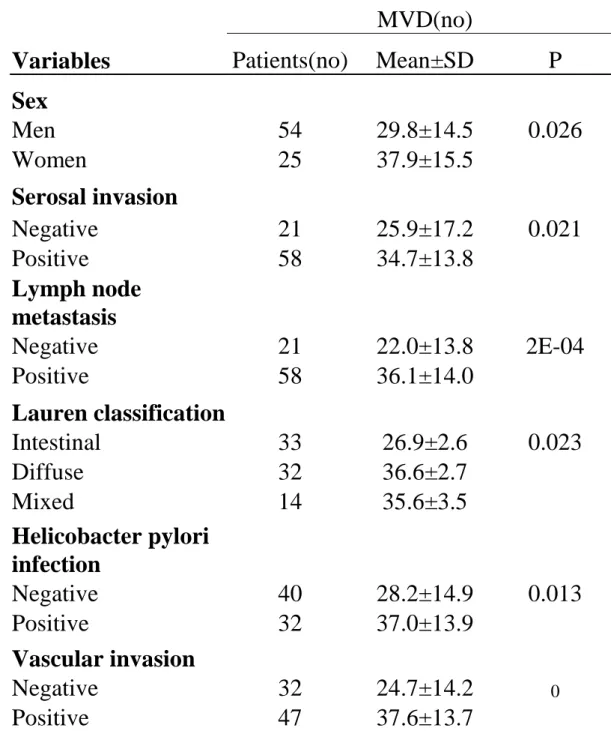
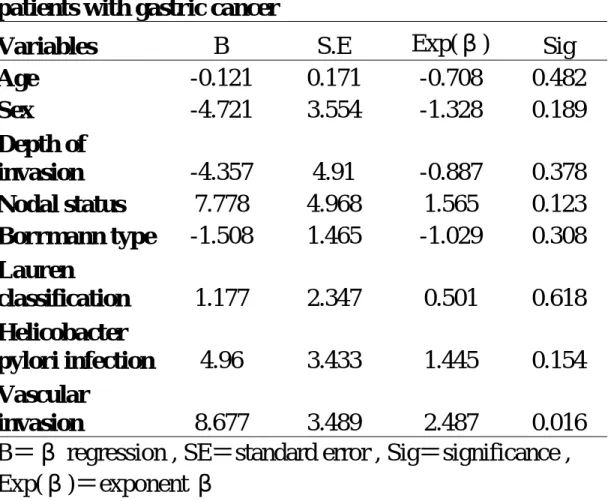
MVD of the total 79 patients ranged from 5 to 68 with a mean value of 32.4. Table 2 showed the correlation between MVD and various clinicopathologic factors. A significantly higher MVD was found in positive vascular invasion (p=0.000), depth of tumor invasion (p=0.021), diffuse type cancer (p=0.023) and positive Helicobacter pylori infection (p=0.013). However, multiple linear regression analysis showed only vascular invasion was significantly correlated with MVD (p=0.016) (Table 3). MVD of stage I gastric cancer was significantly lower than that of stage II and III (p=0.0007), and there was no significant difference among stage II, IIIa and IIIb. (Fig. 3) The outcome of the 79 patients was then analyzed. Since the mean MVD of these patients was 32.4; therefore, we classified them into two subgroups: group of MVD > 32 and group of MVD ≦ 32. The survival rates were calculated using the Kaplan-Meier method. The survival rate of the group with high MVD was significantly lower than that with low MVD (p=0.0002). The effects of variables presumably associated with patient survival were studied by multivariate analysis using Cox proportional hazards model. As a result, vascular invasion was the only independent prognostic factor in these 79 patients (Table 4). In CDVI subgroup, the CDVI of the sonographically visible gastric cancers ranged from 1.0% to 30% with a mean value of 11.4%. There was a linear correlation between CDVI and MVD (r=0.495, p=0.005) (Fig. 4). The CDVI in the patients with vascular invasion was significantly higher than in those without vascular invasion (p=0.026). The CDVI of diffuse type gastric cancer was significantly higher than that of intestinal type (p=0.034). There was no significant correlation between CDVI and other clinicopathological factors such as age sex, Borrmann types, Helicobacter pylori infection, and tumor size.
The prognosis of the 31 patients who had sonographically visible gastric cancer was then analyzed. Since the mean MVD of these patients was 33.5; therefore, we classified them into two subgroups: group of MVD > 34 and group of MVD ≦ 34. The mean CDVI of these patients was 11.4%. Accordingly, the patients were divided into two subgroups: group of high CDVI (> 11%) and group of low CDVI (≦ 11%). The survival rates were calculated using the Kaplan-Meier method. The survival rate of the group with high CDVI was significantly (p=0.005) lower than that with low CDVI and MVD was also the case (p=0.0493)(Fig. 5). There was an intriguing finding that none of the stage III patients with the CDVI > 11% survived beyond 2 years after curative resection.
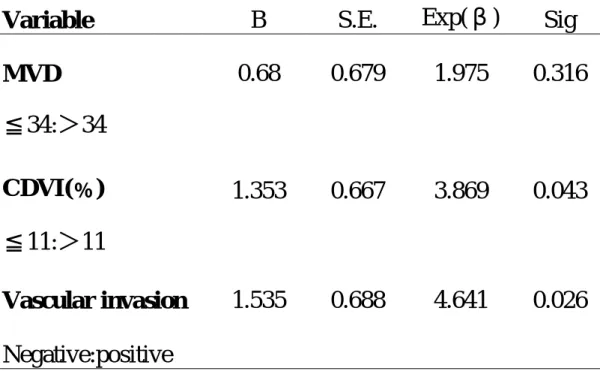
Simultaneous consideration of the effects of variables including vascular invasion, CDVI, and MVD on patients’ survival was studied by multivariate analysis using Cox proportional hazards model. As a result, vascular invasion and CDVI were independent prognostic factors (Table 5).
Discussion
In this study, MVD of gastric cancer was correlated with tumor differentiation, tumor invasion depth, lymph node metastasis, and vascular invasion. However, vascular invasion was found to be an independent prognostic factor in original group and CDVI subgroup. The CDVI was statistically significantly correlated with MVD though the correlation between these two parameters was not strong. In addition to vascular invasion, the CDVI was an independent prognostic factor in CDVI subgroup.
Current ultrasound technology is not capable of detecting tumor neovascularization itself (approximately 15 µm or less in diameter), which was usually demonstrated immunohistochemically23. The color Doppler signals seen within tumor represented the larger and functional vessels (approximately 100µm or more in diameter), possibly intratumoral arterioles, venules, and arteriole-vanule shunting23,24, in which blood flow ran. Although there was a loose linear correlation between CDVI and MVD in this study, we hypothesized that the more neovascularization existed, the more supplying intratumoral arterioles and draining venules was present. The distribution of angiogenesis in a tumor is usually uneven and heterogenous, and MVD, the microvessel count in a tiny portion of tumor, may be not sufficient to represent the global tumor angiogenesis. Recently, Maniotis et al25 reported that aggressive melanoma cells generate non-endothelial cell-lined channels delineated by extracellular matrix, and these “vasculogenic mimicry” channels that are undetectable in MVD assay link directly to larger normal vessels. Thus, CDVI, by quantitatively depicting the density of the larger supplying arterioles and draining venules, can better reflect global vascularization of a tumor.
Liotta et al26,27 developed a tumor perfusion study with C57BL/6J male mice, and they found that the tumor vessel size and density are important determinants of the size of tumor cell clumps and concentration of effluent tumor cells released into the circulation and developed distant metastasis28. Therefore, increased density of larger vessels that can be evaluated with CDVI may facilitate distant metastases by allowing the intravasation and transportation of larger cancer cell clumps. In our previous study, colon cancer patients with high CDVI has higher incidence of distant metastasis after curative resection and poorer prognosis than patients with low CDVI22. This in vivo observation in human is in line with Liotta’s in mice. As
a result, CDVI can better reflect the tumor invasiveness, metastasis and prognosis. This may be the reason why high CDVI can predict early death in patients with stage III gastric cancer.
Currently, MVD is widely employed for assessing angiogenesis in human solid cancers 10,11,29-32. In fact, more than 70% of the studies found a significant association between MVD and clinical outcome of the patients. Sixty percent of the studies in which a multivariate analysis was performed demonstrated that MVD is an independent prognostic factor 33. In the present study, higher MVD was correlated with positive vascular invasion, depth of tumor invasion, positve lymph node metastasis, diffuse type cancer and positive Helicobacter pylori infection. Vascular invasion was the only factor that significantly correlated with MVD in multivariate analysis, and was also an independent prognostic factor. However, MVD was not an independent prognostic factor. Vascular invasion is a well-known factor for hematogenous metastasis and also an independently prognostic factor in gastric cancer 34-39. Local shedding of cancer cells into the tumor vascular stream that can commence at the onset of angiogenesis, is quantitatively related to the
surface area of intratumoral vessels 26,40. The CDVI as a measure of global vascularity of the tumor might better reflect the surface area of intratumoral vessels. In present study, the patients with vascular invasion had significantly higher CDVI than those without. Poor prognosis of high CDVI patients may be related with hematogenous spreading for high frequency of vascular invasion.
The majority of the patients with early gastric cancer can be cured by surgery. Unfortunately, the most gastric cancer patients had advanced disease in Taiwan. The prognosis of patients with advanced gastric cancer, who have undergone curative gastrectomy, is still poor. It may depend on the biological nature of the resected tumor itself, as no grossly detectable residual tumors have been left behind after surgery. Unfortunately, there is currently still no definite place for adjuvant chemotherapy in resected gastric cancer, outside the setting of a clinical trial 41. One of the major clinical problems is we don’t know how to select high-risk patients who can really benefit from chemotherapy or other modality of treatment. Therefore, selecting out a subset of patients from this group who may have a worse prognosis may be clinically useful, and future studies using new compounds and regimens, focusing on high-risk groups of patients may offer the best chance of demonstrating a definite role for adjuvant chemotherapy in this disease.
There is little doubt that the current staging system of gastric cancer still lumps together molecularly distinct diseases with distinct clinical phenotypes. The majority of human solid tumors are heterogeneous diseases, made up of multiple cell clones with diverse biological aggressiveness. It seems clear that stage III gastric cancers at least are heterogeneously angiogenic diseases, and this angiogenic heterogeneity was associated with diverse angiogenic tumor clones 42, activation of oncogenes 43,44, downregulation of tumor suppressor genes 45,
immunogenecity 46,47, and ability to metastatize. Therefore, the CDVI could be considered to represent the summation effect of complex biological processes of tumor vascularization, progression, and metastasis in gastric cancer, and was an excellent prognostic indicator to select out patients who might suffer from early death in stage III gastric cancer patients after curative gastrectomy. The results of initial studies of neoadjuvant chemotherapy in resectable advanced gastric cancer are encouraging 48,49. Thus, the preoperative CDVI in advanced gastric cancer patients may help to identify patients for appropriate neoadjuvant therapy. Other than chemotherapy, different types of antiangiogenic compounds have been developed and shown to inhibit angiogenesis and the growth of some tumors in preclinical trials and a few compounds are further down the clinical road 50-52. Such agents may be valuable in the adjuvant and/or neoadjuvant therapy of advanced gastric cancer patients with high CDVI tumors.
References
1. Folkman J., Long D., Becker F. Growth and metastasis of tumor in organ culture. Cancer; 16: 453-457, 1963.
2. Folkman J. What is the evidence that tumors are angiogenesis dependent? J. Natl. Cancer Inst., 82: 4-6, 1990.
3. Bicknell R., Harris AL. Novel growth regulatory factors and tumor angiogenesis. Eur. J. Cancer , 27: 781-784, 1991.
4. Weidner N., Semple S.F., Welch W.R., Folkman J., et al. Tumor angiogenesis and metastasis-correlation in invasive breast carcinoma. N. Engl. J. Med., 324: 1-8, 1991.
5. Weidner N., Folkman J., Pozza F., et al. Tumor angiogenesis: a new significant and independent prognostic indicator in early stage breast carcinoma. J. Natl. Cancer Inst., 84:1875-1887, 1992.
6. Toi M., Kashitani J., Tominaga T. Tumor angiogenesis is an independent prognostic indicator in primary breast carcinoma. Int. J. Cancer, 55: 371-374, 1993.
7. Macchiiarini P., Fontanini G., Hardin MJ., et al. Relation of neovasculatue to metastasis of non-small-cell lung cancer. Lancet, 340: 145-146, 1992.
8. Weidner N., Carrol P.R., Flax J., blumenfeld W., Folkman J. Tumor angiogenesis correlates with metastasis in invasive prostate carcinoma. Am. J. Pathol., 143: 401-409, 1993.
9. Gasparini G., Weidner N., Maluta S., et al. Intratumoral microvessel density and p53 protein: correlation with metastasis in head-and-neck squamous-cell carcinoma. Int. J. Cancer, 55: 739-744, 1993.
10. Saclarides T.J., Speziale N.J., Drab E., et al. Tumor angiogenesis and rectal carcinoma. Dis. Colon Rectum, 37: 921-926, 1994.
11. FrankR.E., Saclarides T.J., Leurgans S., Speziale N.J., Drab E.A., Rubin D.B. Tumor angiogenesis as a predictor of recurrence and survival in patients with node-negative colon cancer. Ann. Surg., 222: 695-699, 1995.
12. Dock W., Grabenwoger F., Metz V., Eibenberger K., Farres M.T. Tumor vascularization: assessment with duplex sonography. Radiology, 181: 241-244, 1991.
13. Taylor K.J.W., Ramos I., Carter D., Morse S.S., Snower D., Fortune K. Correlation of Doppler US tumor signals with neovascular morphologic features. Radiology, 166: 57-62, 1988.
14. Newman J.S., Bree R.L., Rubin J.M. Prostate cancer: diagnosis with color Doppler sonography with histologic correlation of each biopsy site. Radiology, 195: 86-90, 1995.
15. Wu C.C., Lee C.N., Chen T.M., Shyu M.K., Hsieh C.Y., Chen C.Y., et al. Incremental angiogenesis assessed by color Doppler ultrasound in the tumorigenesis of ovarian neoplasm. Cancer, 73: 1251-1256, 1994.
16. Cheng W.F., Chen T.M., Chen C.A., Wu C.C., Huang K.T., Hsieh C.Y., et al. Clinical application of intratumoral blood flow study in patients with endometrial carcinoma. Cancer, 82: 1881-1886, 1998.
17. Wu C.H., Hsu M.M., Chang Y.L., Hsieh F.J. Vascular pathology of malignant cervical lymphadenopathy. Cancer, 83: 1189-1196, 1998.
18. Cheng W.F., Lee C.N., Chu J.S., Chen C.A., Chen T.M., Shau W.Y., Hsieh C.Y., Hsieh FJ. Vascularity index as a novel parameter for the in vivo assessment of angiogenesis in patients with cervical carcinoma. Cancer,
85:651-7, 1999.
19. Bluth E.I., Merrit C.R.B., Sullivan M.A. Ultrasonic evaluation of the stomach, small bowel, and colon. Radiology, 677-680, 1979.
20. Fakhry Jr., Berk R.N. The “target” pattern: characteristic sonographic feature of stomach and bowel abnormalities. A.J.R., 137: 969-972, 1981.
21. Rapaccini GL, Aliotta A, Pompili M, Grattagliano A, Anti M, Merlino B, Gambassi G. Gastric wall thickness in normal and neoplastic subjects: a prospective study performed by abdominal ultrasound. Gastrointestinal Radiol 1988; 13: 197-9.
22. Chen CN, Cheng YM, Liang JT, Lee PH, Hsieh FJ, Yuan RH, Wang SM, Chang MF, Chang KJ. Color Doppler vascularity index can predict distant metastasis and survival in colon cancer patients. Cancer Res 2000; 60: 2892-2897.
23. Fleischer A.C., Wojcicki W.E., Donnelly E.F., Pickens D.R., Thirsk G., Thurman G.B., Hellerqvist C.G. Quantified color Doppler sonography of tumor vascularity in an animal model. J. Ultrasound Med., 18: 547-551, 1999. 24. Lassau N, Paturel-Asselin C, Guinebretiere J-M, Leclere J, Koscielny S,
Roche A, Chouaib S, Peronneau P. Invest Radiol 1999; 34: 194-198.
25. Folberg R, Hendrix MJC, Maniotis AJ. Vasculogenic mimicry and tumor angiogenesis. Am J Pathol 2000; 156: 361-381.
26. Liotta L., Kleinerman J., Saldel G. Quantitative relationships of intravascular tumor cells, tumor vessel, and pulmonary metastases following tumor implantation. Cancer Res., 34: 997-1004, 1974.
27. Liotta L.A., Kleinerman J., Saidel G.M. The significance of hematogenous tumor cell clumps in the metastatic process. Cancer Res., 36: 889-894, 1976.
28. Fidler I.J. The relationship of embolic homogeneity, number, size and viability to the incidence of experimental metastasis. Euro. J. Cancer, 9: 223, 1973. 29. Meada K, Chung YS, Takatsuka S, Ogawa Y, Sawada T, Yamashita Y, Onoda
N, Kato Y, Nitta A, Arimoto Y, Kondo Y, Sowa M. Tumor angiogenesis as a predictor of recurrence in gastric carcinoma. J Clin Oncol 1995; 13: 477-481. 30. Tanigawa N, Amaya H, Matsumura M, Shimomatsuya T, Horiuchi T,
Muraoka R, Iki M. Extent of tumor vascularization correlates with prognosis and hematogenous metastasis in gastric carcinomas. Cancer Res 1996; 56: 2671-2676.
31. Takebayashi Y., Akiyama S.I., Yamada K., Akiba S., Aikou T. Angiogenesis as an unfavorable prognostic factor in human colorectal carcinoma. Cancer, 78: 226-31, 1996.
32. Bossi P., Viale G., Lee A.K.C., Alfano R.H., Coggi G., Bosari S. Angiogenesis in colorectal tumors: microvessel quantification in adenomas and carcinomas with clinicopathologic correlations. Cancer Res., 55: 5049-5053, 1995.
33. Gasparini G. Prognostic and predictive value of intra-tumoral microvessel density in human solid tumors. In: Bicknell R, Lewis CE, Ferrara N. Tumor angiogenesis. New York: Oxford University Press Inc; 1997. P.29-44.
34. Okada M, Kojima S, Murakami M, Fuchigami T, Tsuneyoshi Y, Omaet and Iwashita A. Human gastric carcinoma: prognosis in relation to macroscopic and microscopic features of the primary tumor. J Natl Cancer Inst 1983; 71: 275-279.
35. Ribeiro MM, Seoxas M, Sobrinho-Simoes M. Prognosis in gastric carcinoma. The preeminence of staging and futility of histological classification. Dig Dis
Pathol 1988; 1: 51-68.
36. Korenaga D, Haraguchi M, Okamura T, Baba H, Saito A, Sugimachi K. DNA ploidy and tumor invasion in human gastric cancer. Arch Surg 1989; 14: 314-318.
37. Gabbert HE, Meier S, Gerharz CD, Hommel G. Incidence and prognostic significance of vascular invasion in 529 gastric cancer patients. Int J Cancer 1991; 49: 203-207.
38. Setala LP, Kosma VM, Marin S, Lipponen PK, Eskelinen MJ, Syrjanen KJ. Alhava EM. Prognostic factors in gastric cancer: the value of vascular invasion, mitotic rate and lymphoplasmacytic infiltration. Br J Cancer 1996; 74: 766-772.
39. Maehara Y, Tomoda M, Hasuda S, Kabashima A, Tokunaga E, Kakeji Y, Sugimachi K. Prognostic value of p53 protein expression for patients with gastric cancer – a multivariate analysis. Br J Cancer 1999; 79: 1255-1261. 40. Liotta L.A., Steeg P.S., Stetler-Stevenson W.G. Cancer metastasis and
angiogenesis: an imbalance of positive and negative regulation. Cell, 64: 327-336, 1991.
41. Ellis P, Cunningham D. Adjuvant and neoadjuvant chemotherapy. In: Sugimura T, Sasako M. Gastric cancer. New York: Oxford University Press Inc; 1997. P.283-290.
42. Folkman J. Angiogenesis in cancer, vascular, rheumatoid and other disease. Nat Med 1995; 1: 27-31.
43. Mitsuhashi R, Bayko L, Shirasawa S, Sasazuki T, Kerbel R. Mutant ras upregulates VEGF/PVF expression: implications for induction and inhibition of tumor angiogenesis. Cancer Res 1995; 55: 4575-4580.
44. Mazure N, Chen E, Yeh P, Laderoute K, Giaccia A. Oncogenic transformation and hypoxia synergistically act to modulate vascular endothelial growth factor expression. Cancer Res 1996; 56: 3436-3440.
45. Dameron KM, Volpert OV, Tainsky MA, Bouck N. Control of angiogenesis in fibroblasts by p53 regulation of thrombospondin-1. Science 1994; 265: 1582-1584.
46. Camusssi G, Montrucchio G, Lupia E, Soldi R, Comoglio PM, Bussolino F. Angiogenesis induced in vivo by hepatocyte growth factor is mediated by platelet-activating factor synthesis from macrophage. J Immunol 1997; 158: 1302-1309.
47. Carlos TM, Harlen JM. Leukocyte-endothelial adhesion molecules. Blood 1994; 84: 2068-2101.
48. Ajani JA, Majer RJ, Ota DM, et al. Preoperative and postoperative combination chemotherapy for potentially resectable gastric carcinoma. J Natl Cancer Inst 1993; 85: 1839-1844.
49. Findlay M, Cunningham D, Norman A, et al. A phase II study in advanced gastric cancer using epirubicin and cisplatin in combination with continuous infusion 5-fluorouracil (ECF). Ann Oncol 1994; 5: 609-616.
50. Ingber D., Fujita T., Kishimoto S., et al. Synthetic analogues offumagillin that inhibit angiogenesis and suppress tumor growth. Nature, 384: 555-557, 1990. 51. Griffioen AW, Molema G. Angiogenesis: potentials for pharmacologic
intervention in treatment of cancer, cardiovascular diseases, and chronic inflammation. Pharmacol Review 2000; 52: 237-268.
52. Kerbel RS. Tumor angiogenesis: past, present and the near future. Carcinogenesis 2000; 21: 505-515.
Legends of figures
Figure 1. Color Doppler vascularity index assessment within the gastric cancer. The color window was set to cover the whole tumor on the screen and stored for later quantitative analysis (A). The tumor margin was contoured using a cursor (B). Quantification of the vascular color signals within the demarcated tumor was then automatically executed by special software called Encomate (Electronic Business Machine Co., Ltd., Taiwan). The results were expressed as the "color Doppler vascularity index" (the number of colored pixels within the tumor section /the number of total pixels in that particular tumor section) (C). Figure 2. Immunohistochemical staining for CD-34 in gastric cancer tissues (original magnification × 400). Microvessels are represented by brown clusters, which stand out sharply from other tissues.
Figure 3. Correlation between microvessel counts and TNM stages Figure 4. Correlation between MVD and CDVI
Figure 5. Survival curves of patients with high color Doppler vascularity index (> 11%) and that with low color Doppler vascularity index (≦ 11%).
Table 1 Char acter istics of patients studied
Toal patients
(n=79)
CDVI subgroup
(n=31)
Age (yr )
Range
42-85
43-85
Mean
63.3
63.7
Sex (no.of patients)
Men
54
21
Women
25
10
Location of tumor (no)
Upper third
11
4
Middle third
23
10
Lower third
45
17
Bor r mann type
I
3
0
II
11
3
III
55
27
IV
10
1
Laur en classificafion
Intestinal
33
11
Diffuse
32
13
Mixed
14
7
Helicobacter pylor i infection
Positive
30
10
Negative
49
21
Vascular invasion
Positive
47
19
Negative
32
12
Stages
I
15
0
II
7
1
IIIa
31
18
IIIb
26
12
Table 2 Cor r elation between clinicopathologic factor s and
MVD
MVD(no)
Var iables
Patients(no)
Mean±SD
P
Sex
Men
54
29.8±14.5
0.026
Women
25
37.9±15.5
Ser osal invasion
Negative
21
25.9±17.2
0.021
Positive
58
34.7±13.8
Lymph node
metastasis
Negative
21
22.0±13.8
2E-04
Positive
58
36.1±14.0
Laur en classification
Intestinal
33
26.9±2.6
0.023
Diffuse
32
36.6±2.7
Mixed
14
35.6±3.5
Helicobacter pylor i
infection
Negative
40
28.2±14.9
0.013
Positive
32
37.0±13.9
Vascular invasion
Negative
32
24.7±14.2
0Positive
47
37.6±13.7
Table 3 Relationship between MVD and the
clinicopathologic factor s by multivar iate analysis in 79
patients with gastr ic cancer
Var iables
B
S.E
Exp(β)
Sig
Age
-0.121
0.171
-0.708
0.482
Sex
-4.721
3.554
-1.328
0.189
Depth of
invasion
-4.357
4.91
-0.887
0.378
Nodal status
7.778
4.968
1.565
0.123
Bor r mann type
-1.508
1.465
-1.029
0.308
Laur en
classification
1.177
2.347
0.501
0.618
Helicobacter
pylor i infection
4.96
3.433
1.445
0.154
Vascular
invasion
8.677
3.489
2.487
0.016
B=β regression , SE=standard error , Sig=significance ,
Exp(β)=exponent β
Table 4 Clinicopathologic factor s affecting sur vival r ate by
multiple linear r egr ession analysis in 79 patients with
gastr ic cancer who under went r esection
Var iables
B
S.E
Exp(β)
Sig
Age
0.014
0.019
1.014
0.44
Sex
-0.322
0.394
0.725
0.41
Male vs female
Ser osal invasion
1.535
0.831
4.639
0.05
Negative vs Positive
Lymph node
metastasis
0.59
0.682
1.804
0.39
Negative vs Positive
Laur en classification
0.118
0.273
1.126
0.66
Intestinal vs diffuse
Helicobacter pylor i
infection
0.58
0.414
1.786
0.16
Negative vs Positive
Vascular invasion
1.31
0.556
3.705
0.018
Negative vs Positive
MVD
0.019
0.014
1.02
0.16
≦32 vs>32
B=β r egr ession coefficient , SE=standar d er r or , Sig=significance ,
Table 5 Clinicopathologic factor s affecting over all sur vival
r ate deter mined by Cox pr opor tional hazar d model in
stage III patients
Var iable
B
S.E.
Exp(β)
Sig
MVD
0.68
0.679
1.975
0.316
≦34:>34
CDVI(﹪)
1.353
0.667
3.869
0.043
≦11:>11
Vascular invasion
1.535
0.688
4.641
0.026
Negative:positive
Figure 3 0 10 20 30 40 50 60
stage I stage II stage IIIa stage IIIb
MVD Figure 4 10 20 30 40 50 60 MVD 0 5 10 15 20 25 30 CDVI (%) r=0.495 p=0.005
Figure 5 0 10 20 30 40 0 .0 0 .2 0 .4 0 .6 0 .8 1 .0 10.7% (n=14) 60.9% (n=17) p=0.0493
Months after surgery MVD<34 MVD>34 0 10 20 30 40 0 .0 0 .2 0 .4 0 .6 0 .8 1 .0 64.2% (n=16) 0% (n=15)
Months after surgery CDVI<11%
CDVI>11%