Original Article
Are Nurses Prepared to Manage Cancer
Pain? A National Survey of Nurses’
Knowledge about Pain Control in Taiwan
Yeur-Hur Lai, RN, PhD, Mei-Ling Chen, RN, PhD, Li-Yun Tsai, RN, MS, Li-Hua Lo, RN, PhD, Ling-Ling Wei, RN, MS, Ming-Ying Hong, RN, MS,
Ling-Nu Hsiu, RN, MS, Shu-Tai Hsiao-Sheen, RN, MS, Shu-Ching Chen, RN, MS, Chin-Chiu Kao, RN, MS, Tsai-Wei Huang, RN, MS, Shu-Chen Chang, RN, MS, Li Chen, RN, BS, and Shu-Liu Guo, RN, MS
College of Nursing (Y-H.L., L-L.W.), Taipei Medical University, Taipei; Chang Gung University (M-L.C.), Tau-Yuan; Mackay Memorial Hospital (L-Y.T.), Taipei; National Cheng-Kung University (L-H.L.), Tainan; National Taiwan University Hospital (M-Y.H.); Chung-Gung Technology College of Health (S-C.Chen), Tau-Yuan; Kaohsing Chang Gung Memorial Hospital (L-N.H.),
Kaohsing; Cathay General Hospital (S-T.H-S., S-L.G.), Taipei; Wong-Fan General Hospital (C-C.K.), Taipei; Hung-Kuang Technology College (T-W.H.), Taichung; Changhua Christian Hospital (S-C.Chang), Changhua and Buddhist Tzuchi General Hospital (L.C.), Hualien, Taiwan
Abstract
Nurses play a crucial role in cancer pain control, but little is known about how well-prepared nurses are to manage cancer pain in Taiwan. The purpose of this study was to examine the level of knowledge about pain management among Taiwanese nurses with different background characteristics and to determine the predictor(s) of nurses’ pain management knowledge. Nurse subjects were recruited by a cross-sectional nationwide survey with stratified sampling from nine hospitals distributed in the four major geographic regions of Taiwan. The Nurses’ Knowledge and Attitudes Survey-Taiwanese version (NKAS-T) and a background information form were used to collect the data. Of 1900 surveys distributed, 1797 valid questionnaires (94.5%) were analyzed. The average correct response rate was 50.5%, with rates ranging from 7–86% for each survey question. Results from stepwise regression showed that nurses with higher mean correct answer scores had BS or higher degrees, had received pain education at professional conferences, had more prior hours of pain education, had longer clinical care experiences, and always worked with cancer patients. Nurses who worked in intensive care units, however, had significantly lower mean correct scores. The results strongly suggest an urgent need to strengthen pain education in Taiwan. The results also provide the direction for developing pain education. J Pain Symptom Manage 2003;26:1016–1025.
쑖
2003 U.S. Cancer Pain Relief Committee. Published by Elsevier Inc. All rights reserved.Key Words
Pain, knowledge, attitudes, education
Address reprint requests to: Yeur-Hur Lai, RN, PhD,
Col-lege of Nursing, Taipei Medical University, 250 Wu-Hsing Street, Taipei 110, Taiwan.
Accepted for publication: March 14, 2003.
쑖2003 U.S. Cancer Pain Relief Committee 0885-3924/03/$–see front matter Published by Elsevier Inc. All rights reserved. doi:10.1016/S0885-3924(03)00330-0
Introduction
Cancer has been the leading cause of death in Taiwan since 1982,1 with pain recognized
as one of the most severe problems for these patients. Pain is experienced by 30.9–85% of cancer patients in Taiwan.2–4The data strongly suggest that cancer pain has not been well man-aged in Taiwan and that problems related to ineffective pain control should be examined.
In the United States (U.S.), health care pro-fessionals’ lack of accurate pain knowledge and inappropriate attitudes toward cancer pain and use of analgesics have been recognized as major barriers to managing pain.5In particular, nurses play a critical role in pain management because they deliver direct patient care on a 24-hour basis. Unfortunately, results from stud-ies in the U.S.6–14 and several other coun-tries7,15,16reveal that nurses’ lack of knowledge about pain is a common problem in pain man-agement. The problem may influence nurses’ sequential inferences and clinical decision-making on pain control. Therefore, it is im-portant to identify how well nurses are prepared to manage cancer pain.
Assessment of nurses’ level of pain man-agement knowledge can provide information about the distribution of different aspects of knowledge about pain management and also be used as the basis for developing appropriate pain management education for nurses who work with cancer patients. Although a few studies have explored student nurses’ or nurses’ beliefs and knowledge about pain in Taiwan,17–19these studies focused on particular groups of nurses with relatively small sample sizes. This lack of data and generalizability fails to represent the level of nurses’ knowledge about pain man-agement in Taiwan. In addition, cancer patients are widely distributed among different hospital settings. Therefore, nurses in different work set-tings may have opportunities to care for cancer patients. Insufficient data, however, prevent knowing whether there are knowledge differ-ences among nurses working in different set-tings. Even if such differences in pain management knowledge exist, do they stem from different demographic characteristics and educational background? Do these factors pre-dict nurses’ pain knowledge level?
As part of a larger pain management project in Taiwan, therefore, the present study focused on analyzing nurses’ pain knowledge. The spe-cific aims of this study were to 1) identify the level of knowledge about pain management among Taiwanese nurses, 2) examine nurses’
pain management knowledge according to their background characteristics (level of nurs-ing education, frequency of carnurs-ing for cancer patients, work setting, prior pain education, hours of pain education, sources of pain educa-tion), and 3) determine predictor(s) of nurses’ pain knowledge using the variables found to be significant in Aim 2.
Methods
Sample and Setting
A nationwide survey of Taiwanese nurses’ knowledge about pain management was con-ducted. In order to study a representative sample, nurses were recruited based on two cri-teria: hospital category level and geographic distribution. In Taiwan, hospitals are catego-rized by the number of hospital beds; level of advanced treatments, preparation for teaching, training, and research. The majority of cancer patients in Taiwan are treated at medical cen-ters (the top level or most advanced hospitals) and regional-level hospitals. Nurses who work in hospitals at these two levels generally have many more opportunities to care for cancer patients than nurses working at other types of hospitals. We, therefore, targeted hospitals at these two levels. Targeted settings for data col-lection were medical wards, surgical wards, on-cology wards, medical-surgical mixed wards, intensive care units, and emergency rooms.
The sample surveyed included nurses working at hospitals located in northern, central, south-ern, and eastern Taiwan. To account for differ-ences in hospital distributions among these four major geographic areas, we recruited nurses from four hospitals in Taipei (two medical cen-ters, two regional-level hospitals), two hospitals in central Taiwan (one of each type of hospital), two hospitals in southern Taiwan (one of each type), and one hospital from eastern Taiwan.
Instruments
The instruments used in this study include the Nurses’ Knowledge and Attitude Survey (NKAS)20and a background information form. The NKAS has been widely used in assessing nurses’ knowledge and attitude towards pain, and has been found to be reliable.16,20 The NKAS consists of 46 pain management-related items. The first section includes 37 items re-lated to pain assessment and management
knowledge; items 38 to 46 relate to nurses’ opin-ions about the adequacy of pain control in their clinical settings. For the purposes of this study, we used only the items in the first section to examine nurses’ knowledge about pain. In addi-tion, the NKAS was translated and back-trans-lated between English and Chinese based on principles of instrument translation across dif-ferent languages.21 To account for potential cross-country differences in managing cancer pain, five pain experts (two anesthesiologists, one oncologist, two master’s-prepared oncol-ogy nurses) verified the content validity (includ-ing appropriateness of the content and clarity of the wording) of the NKAS Taiwanese version (NKAS-T) for use in Taiwan.
Because some medications are not widely used in most hospitals in Taiwan, however, the assessment of nurses’ knowledge about drugs that are mentioned in these items may not re-flect their knowledge about pain management. As suggested by four of the five pain experts, therefore, two items of the original NKAS were not included in the current study. These two items were “Research shows that promethazine (Phenergan) is a reliable potentiator of opi-oids,” and “Which of the following drugs are useful for treatment of cancer pain? (ibupro-fen, hydromorphone, amitriptyline).” Among the remaining 35 items, Items 36 and 37 were case studies with two sub-items. Therefore, in total, 37 knowledge questions were assessed in the current study. Each correctly scored item was assigned a score of 1. Incorrectly answered items or those not answered were assigned a score of 0. Total scores were summed and ranged from 0 to 37. Correct answer rates were calculated by dividing the total number of cor-rectly answered items by the total number of items (37). Cronbach’s alpha for the NKAS-T in previous studies was 0.8217 and 0.70,19 and 0.70 in the current study.
We used a background information form to record nurses’ age, formal nursing education (professional nursing high school diploma, junior nursing college level, and BS or higher degree in nursing), length of clinical care expe-rience (months), work setting (medical, surgi-cal, oncology, mixed medical-surgisurgi-cal, intensive care or emergency room), prior experience caring for cancer patients (Yes/No), frequency of caring for cancer patients, prior pain manage-ment education (Yes/No), total hours of prior
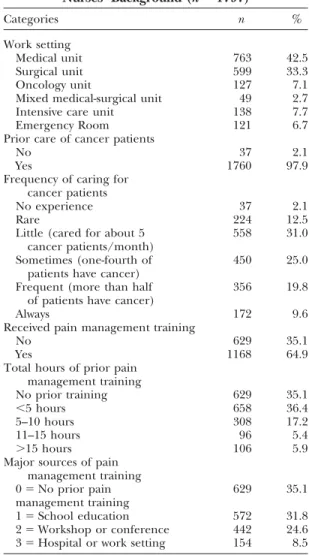
pain management education (No classes, ⬍5 hours, 6–10 hours, 11–15 hours, ⬎15 hours), and major source of prior pain management education (SeeTable 1for details).
These instruments were delivered as self-ad-ministered questionnaires to nurse subjects (n⫽ 1900) recruited from the nine hospitals mentioned above. A cover letter introducing the purpose of the study was included. To in-crease the reliability of answers, the ques-tionnaires were anonymous and confidential. Anonymity was particularly important to ensure that pain knowledge scores would not be used to evaluate nurses in each data-collection setting, and to increase the nurses’ willingness to answer the questionnaire.
Procedures
After hospitals and settings were chosen, the evaluation from the Institutional Review Board
Table 1 Nurses’ Background (n⫽ 1797) Categories n % Work setting Medical unit 763 42.5 Surgical unit 599 33.3 Oncology unit 127 7.1
Mixed medical-surgical unit 49 2.7
Intensive care unit 138 7.7
Emergency Room 121 6.7
Prior care of cancer patients
No 37 2.1
Yes 1760 97.9
Frequency of caring for cancer patients
No experience 37 2.1
Rare 224 12.5
Little (cared for about 5 558 31.0 cancer patients/month)
Sometimes (one-fourth of 450 25.0 patients have cancer)
Frequent (more than half 356 19.8 of patients have cancer)
Always 172 9.6
Received pain management training
No 629 35.1
Yes 1168 64.9
Total hours of prior pain management training No prior training 629 35.1 ⬍5 hours 658 36.4 5–10 hours 308 17.2 11–15 hours 96 5.4 ⬎15 hours 106 5.9
Major sources of pain management training
0⫽ No prior pain 629 35.1
management training
1⫽ School education 572 31.8
2⫽ Workshop or conference 442 24.6 3⫽ Hospital or work setting 154 8.5
(IRB) in each data collection hospital was fur-ther processed before data collection. After the approval from the IRB, the principal investiga-tor met with nurse representatives from the dif-ferent settings at each hospital to explain the questionnaires and procedures of data collec-tion. The self-administered questionnaires were disseminated to each selected setting through its representative. Nurses at these settings were invited to participate in the study. The impor-tance and purposes of this study were stated on the first page of the questionnaire, and fur-ther explained by the representative at each setting. All nurses voluntarily and anonymously participated in this study. Nurses were asked to answer the pain knowledge questions without discussion during a meeting called specifically to fill out the surveys. Nurses who were off duty on the day of the surveys were asked to answer the questionnaires on their next day back at work. Nurses who answered the questionnaire received a small gift for their participation.
Data Analysis
Knowledge scores for each item in the NKAS-T were calculated by giving “1” for correct an-swers and “0” for incorrect anan-swers, adding the total, and calculating the mean scores for total pain knowledge. The percentages of correct an-swers for total scores received and for each item were also calculated. T-test and analysis of vari-ance (ANOVA) were used to compare the dif-ferences of nurses’ knowledge according to various demographic groups, including formal nursing education, length of clinical care expe-rience, prior cancer care expeexpe-rience, working setting, prior pain education, hours of pain edu-cation and major sources of pain eduedu-cation (SeeTable 1for details). Age was not chosen as a variable because it is highly correlated to length of clinical care experience (r⫽ 0.92, P⫽ 0.000), and age may only reflect the length of nurses’ clinical working experience. Stepwise regression was further applied to identify the predictors of nurses’ pain knowledge by using demographic and background variables found to be significant from the above analysis.
Results
Nurses’ Background in Cancer Care
and Pain Management
Of 1,900 questionnaires sent out to the 9 hospitals, 1,797 valid questionnaires were re-ceived, indicating a 94.6% response rate. Of
the remaining 103 questionnaires, 55 were miss-ing and the other 48 contained too many unan-swered items. Results are based on analysis of the 1,797 valid questionnaires. Responding nurses’ ages ranged from 18 to 50 years, with the mean age of 25.0 (SD⫽ 4.0). The average length of working in nursing was 47.7 months (SD⫽ 45.3), with arange of 1 to364 months and a mode of 31 months. Most respondents (84%) received their nursing education at the junior college level. Some respondents (n⫽ 260, 14.5%) had a BS or higher degree in nursing. Very few (1.5%) had attended three-year nurs-ing diploma programs at professional high schools (individuals with either junior college preparation or a BS degree in nursing are quali-fied to take the national RN examination). The majority of respondents worked in either medi-cal or surgimedi-cal inpatient wards (75.8%), and almost all nurses had prior cancer care experi-ence (97.9%) (Table 1). Almost one-third of respondents (29.4%) reported that they fre-quently or always cared for cancer patients.
Regarding pain management training, a large proportion of responding nurses (35.1%) had no prior pain management training. The remaining nurses (64.9%) had various hours of prior pain management training (Table 1). Among the nurses with prior pain education, the majority received less than 5 hours of pain education.
Nurses’ Pain Knowledge
Among the 37 pain knowledge questions as-sessed, the mean number of correctly answered questions was 18.52 (SD⫽ 4.61), with a range of 6 to 34 items correctly answered. The correct answer rate for the entire scale, on average, was 50.5%. The correct answer rates for each item were further analyzed and are listed inTable 2 as items receiving less than a 50% correct answer rate and those receiving more than 80% of correct answers. Several items received a very low percentage of correct answers. One case study item (Item 36b) received only a 7% cor-rect answer rate, and another case study item (Item 37b) also had a very low correct answer rate (18%). Ten items had a correct answer rate lower than 30%, eight items had a correct answer rate between 30% to 50%, and only six items had more than an 80% correct answer rate (Table 2).
Table 2
Distribution of Nurses’ Knowledge about Pain (n⫽ 1797)
Correct Answer
Item Number Item Content Rate %
Items receiving less than 50% correct answer rate
36B Case Study: Andrew… first day following abdominal surgery. …, he smiles at you … 7 He rates his pain as 8… your assessment is made two hours after he received
morphine 2 mg IV. Half-hourly pain ratings following the injection ranged from 6 to 8, and he had no clinically significant respiratory depression,… His physician’s order for analgesia is “morphine IV 1–3 mg q1h PRN pain relief.” The action you will take at this time is…
34 The percentage of patients who over-report the amount of pain. 10 35 How likely will opioid addiction occur as a result of treating pain with 12
opioid analgesics?
28 … The likelihood of the patient developing clinically significant respiratory depression 16 (with opioid treatment).
8 Respiratory depression rarely occurs in patients who have been receiving opioids over 17 a period of months.
37B Case Study: Andrew… first day following abdominal surgery. He is lying quietly in bed 18 and grimaces as he turns in bed…He rates his pain as 8 … Your assessment
is made two hours after he received morphine 2 mg IV. Half-hourly pain ratings following the injection ranged from 6 to 8, and he had no clinically significant respiratory
depression,… His physician’s order for analgesia is “morphine IV 1–3 mg q1h PRN pain relief.” The action you will take at this time is…
11 The usual duration of action of meperidine (Demerol) IM is 4–5 hours. 24 36A Case Study: Andrew… first day following abdominal surgery. He smiles at you … 24
rates his pain as 8… your assessment of Andrew’s pain is …
23 The recommended route of administration of opioid analgesics to patients with prolonged 24 cancer-related pain is…
7 Non-drug interventions are very effective for mild-moderate pain control but are rarely 29 helpful for more severe pain.
24 Recommended route of administration of opioid analgesics to patients with brief, 30 severe pain of sudden onset, e.g. trauma or postoperative pain, is…
4 Patients may sleep in spite of severe pain. 33
14 Beyond a certain dosage of strong opioids, increases in dosage will not increase pain relief. 34 9 Aspirin 650 mg PO is approximately equal in analgesic effect to meperidine (Demerol) 41
50 mg PO.
30 The most likely explanation for why a patient with pain would request increased doses 44 of pain medication is…
27 Analgesics for post-operative pain should initially be give… 47 37A Case Study: Andrew… first day following abdominal surgery. He is lying quietly in bed 47
and grimaces as he turns in bed… He rates his pain as 8 …your assessment of Andrew’s pain is…
6 Aspirin and other nonsteroidal anti-inflammatory agents are not effective analgesics 48 for bone pain caused by metastases.
Items receiving more than 80% correct answer rate
16 The patient with pain should be encouraged to endure as much pain as possible 82 before resorting to a pain relief measure.
33 Which of the following describes the best approach for cultural considerations in 82 caring for patients in pain:
19 After the initial recommended dose of opioid analgesic, subsequent doses are adjusted 84 in accordance with the individual patient’s response.
32 The most accurate judge of the intensity of the patient’s pain is the patient. 84 5 Comparable stimuli in different people produce the same intensity of pain. 85 1 Observable changes in vital signs must be relied upon to verify a patient’s statement 86
that he has severe pain.
The knowledge scores were further analyzed by nurses’ background characteristics using t-test, ANOVA, and Pearson’s correlation. Signifi-cant differences in nurses’ pain knowledge were found among subgroups in all background vari-ables except prior experience in caring for
cancer patients. In other words, there was no difference in pain knowledge between nurses with or without experience in caring for cancer patients. However, nurses who had always cared for cancer patients (n⫽ 172) had significantly higher pain knowledge than the remaining
nurses (n⫽ 1625) with lower frequencies of caring for cancer patients; the mean pain knowledge scores (SD) were 22.37 (5.14) and 18.11 (4.36), respectively (t⫽ ⫺11.96, P ⫽ 0.000). Nurses’ pain knowledge was positively correlated to length of clinical nursing care expe-rience (in months) (r⫽ 0.18, P ⫽ 0.000). Nurses with a BS or higher level of education (Master’s degree) had significantly higher pain knowledge scores (M⫽ 21.68, SD ⫽ 4.83, correct answer rate⫽ 58.6%) than nurses with junior college education (M⫽ 18.00, SD ⫽ 4.35), and nurses with diploma (M⫽ 16.5, SD ⫽ 4.37)(F ⫽ 79.2, P⫽ 0.000). In particular, nurses with master’s degree preparation had the highest mean pain knowledge score (M⫽ 27.00, SD ⫽ 5.85) and the highest correct answer rate (73.0%).
Knowledge differences were also found among nurses working in different types of settings (F⫽ 18.4, P ⫽ 0.000). The results of ANOVA with post hoc Scheffe’s analysis re-vealed that nurses working in oncology units and emergency rooms had the highest (M⫽ 21.49, SD ⫽ 4.21, 58.1% correct answers) and second highest (M⫽ 20.12, SD ⫽ 6.63, 54.4% correct answers) mean knowledge scores compared to nurses working in other settings. Nurses working in intensive care units had the lowest scores of all (M⫽ 17.04, SD ⫽ 4.24), with a correct answer rate of only 46.1%.
Prior pain management training also had an impact on nurses’ pain knowledge. Nurses who had received pain management education (at school, conferences, or on-site at hospitals) had, on average, significantly higher mean knowledge scores than those without prior pain education; mean scores (SD) were 19.30 (4.72) and 17.06 (4.03), respectively (t⫽ ⫺ 10.1, P⫽ 0.000).
Pain knowledge scores were further com-pared across the three major sources of learn-ing and no prior pain education by uslearn-ing ANOVA and Scheffe’s post hoc examination. The results showed that nurses without any prior pain education had the lowest scores. Nurses who received pain education from pro-fessional pain management conferences or workshops had significantly higher pain knowl-edge scores (M⫽ 21.05, SD ⫽ 5.09, 56.9% cor-rect answers) than nurses who received pain education from school (M⫽ 18.11, SD ⫽ 4.14), hospital on-site continuing education courses
(M⫽ 18.70, SD ⫽ 4.10), or had no prior pain education at all (M⫽ 17.06, SD ⫽ 4.03) (F⫽ 75.0, P ⫽ 0.000).
Pain knowledge scores were also compared among nurses who received different hours of pain education by using ANOVA and Scheffe’s post hoc test. Significant differences were re-vealed in the knowledge scores among nurses having different amounts of hours in pain edu-cation (F⫽ 53.0, P ⫽ 0.000). Mean pain knowl-edge scores descended from high to low, corresponding to the level (hours) of pain man-agement training received by nurses. Those re-ceiving more than 15 hours of pain education scored M⫽ 22.77 (SD ⫽ 5.14, correct answer rate⫽ 61.5%), 10 to 15 hours education scored M⫽ 20.98 (SD ⫽ 5.21), 5 to 10 hours educa-tion scored M⫽ 19.32 (SD ⫽ 4.94), less than 5 hours education scored M⫽ 18.48, (SD ⫽ 4.11) and nurses with no prior pain education scored M⫽ 17.06 (SD ⫽ 4.03, correct answer rate⫽ 46.1%).
One of the study’s purposes was to identify predictors of nurses’ pain management knowl-edge. Significant variables from the previous t-test, ANOVA, or bivariate correlation were used as independent variables in stepwise regression to predict nurses’ pain management knowl-edge. The results showed that predictors of pain management knowledge were having received more hours of pain management, source of pain management from professional confer-ences, always caring for cancer patients, having more clinical care experience (months in clini-cal care), having a BS degree or higher, and not working in intensive care unit (ICU). These variables explained 24.2% of variances of nurses’ pain knowledge.
Discussion
This study provides important information about the level of nurses’ pain knowledge across Taiwan. In general, the results revealed that nurses’ knowledge about pain in Taiwan is far from optimal. Among the 37 pain questions examined, the mean score for correctly an-swered items was 18.8 (50.5% correct answer rate). Although the instrument used in our study may differ somewhat from those used in previous research,8,9,13,22,23our results still show that nurses in Taiwan have relatively low correct
answer rates compared to nurses in the U.S.8,9,11,13,22,23 However, the correct answer rate is similar to that for nurses from other countries, such as Japan,7 Greece,16 and Fin-land.24The less than optimal pain management knowledge in Taiwanese nurses, compared to those in the U.S., may be related to the lack of attention given to pain education in Taiwan in the past. Only with the advent of the hospice movement in Taiwan during the past 10 years has pain control begun to receive attention.
Among the 37 items surveyed, 18 did not even receive half the correct answer rate. Further analysis of items showed four major areas of knowledge deficit: 1) lack of analytic and inte-gration abilities in making clinical pain judg-ments (as reflected in items related to the case studies), 2) questioning patients’ report of pain, 3) lack of knowledge and over-concern about possibilities of developing addiction and respi-ratory depression, and 4) lack of general knowl-edge about the use of analgesics.
Two case studies (representing four items) were assessed in the current study. The item that received the lowest correct answer rate (Table 2, Item 36B) is from one case study. In that item, a patient reports his pain (with a smile) as “8” on a 0 to 10 numerical scale. Surprisingly, only 7% of nurse respondents correctly answered the morphine dosage for the patient (PRN, give as needed), and only 24% of nurses correctly rated the pain intensity as “8” in accord with the pa-tient’s report (Table 2, Item 36A).
In the other case study, a very similar pain scenario was presented except the patient’s po-sition and expression were different (patient is lying quietly in bed and grimaces as he turns in bed). Interestingly, compared to the previous case study, more than twice as many nurses (18%) correctly answered the question about the patient’s morphine dose, though the cor-rect answer rate was still very low. Furthermore, compared to the previous case study scenario, almost double the number of nurses (47%) cor-rectly rated the pain intensity “8” as the patient’s self-report. In contrast, compare these results to an independent item (Table 2, Item 32): “The most accurate judge of the intensity of the pa-tient’s pain is the patient;” surprisingly, 84% of nurses correctly answered the latter item. Our results are similar to and may be best explained by Ferrell et al.’s finding25that 91% of nurses
stated that asking patients was the most fre-quently used method to know patients’ pain intensity; however, only 45% of nurses actually thought asking patients was the best strategy for determining patients’ pain intensity. Taken to-gether, these results indicate that nurses’ clini-cal reasoning about pain is complicated and may be heavily influenced by patients’ expression, position, conditions surrounding the pain expe-rience, and even personal pain experiences.26,27 Our results also reflect potential problems with nurses’ abilities to apply pain knowledge and analyze complicated pain situations. The results further suggest that nurses need more training in analyzing and integrating data from clinical pain assessment.
Another critical issue was raised regarding the item about patients’ over-reporting of pain (Table 2, item 34). Particular attention should be paid to this issue because nurses who believe that patients are over-reporting their pain may be less likely to apply the most appropriate pain management strategies. Regarding the item of over-reporting pain, the correct answer is less than 10%. In our study, only 10.1% of nurse respondents correctly answered Item 34. In other words, most nurses (89.1%) incorrectly believed that more than 10% of patients over-report their pain. Compared to nurses in Western countries,7 a greater percentage of Taiwanese nurses seem to identify patients as over-reporting pain. Inter-estingly, however, our results are very similar to findings about Japanese nurses,7 only 9.7% of whom believe that less than 10% of patients over-report their pain. We wonder if nurses in Asia share similar cultural values or attitudes toward pain that influence how they identify patients’ pain intensity. How cultural values or circumstances shape nurses’ attitudes, values, or knowledge about pain have not yet been explored, and should be further examined to understand pain management problems in Asian countries. The high percentage of nurses who believed that patients’ over-report pain may also explain why the majority rated pa-tients’ pain intensity lower than the papa-tients’ self-report of 8 in the case studies. If nurses lack sufficient and accurate knowledge about pain, they may be easily influenced by factors sur-rounding a patient’s pain situation or their own personal factors, and make pain management decisions based on inaccurate assumptions.28
These factors were not examined in the present study and merit further in-depth research.
Similar to previous studies,10,12,13,29,30 knowl-edge deficits were found in the use of anal-gesics, particularly in equianalgesic dosing, duration of analgesic treatment, and opioid pharmacology. However, compared to nurses in Western countries,7,14,30more nurses (88%) in Taiwan are concerned about addiction (Item 35). Furthermore, similar to a previous study on elderly patients’ pain,3184% of nurses in our study had exaggerated concern about opioid-related respiratory depression (Item 28). To close these pain knowledge gaps, nurse educa-tors in Taiwan should use our results as well as guidelines and well-developed programs, such as American Pain Society or pain resources nurses training, to train nurses, particularly in the use of analgesics.
The regression analysis revealed that pre-dictors of more correct pain knowledge were having a BS or higher degree, more hours of pain education, more experience (time) in clin-ical care, having always cared for cancer pa-tients, and pain education from professional conferences. However, having worked in an ICU negatively predicted nurses’ correct pain knowledge. Some important issues are raised by the regression results. First, similar to previous studies,15 our results strongly support the im-portance and usefulness of nursing and pain education in improving nurses’ knowledge about pain management, though the relatively high knowledge scores found among BS- or MS-prepared nurses are still far from the ideal. Sec-ondly, nurses who received pain education from professional conferences had the highest pain knowledge scores of all educational sources ex-amined. A large number (n⫽ 629; 35.1%) of nurses had not received any pain education. Of those nurses with prior pain education, the majority received only 5 hours or less training. Taken together, these findings further raise important educational issues in Taiwan. First, pain education has not yet been emphasized and generalized across formal nursing educa-tion. Second, total hours of pain education may not be sufficient to prepare nurses to deal with complicated clinical pain problems. Third, al-though mean pain knowledge scores differed significantly among pain education groups, in-cluding hours of pain education received, sources of pain management training and levels
of nursing education, these differences may not have clinical significance in pain manage-ment since they were relatively small. This small difference in scores further suggests that the contents of pain management courses are not sufficiently comprehensive for clinical rele-vance in pain management. Finally, this last issue, if true, suggests that there are not enough pain experts or nurse educators to provide com-prehensive pain education in Taiwan. This lack of sufficient and well-trained pain educators may decrease the effectiveness of delivering and disseminating the most critical and accurate knowledge about pain management.
Similar to a previous study,9 nurses working in oncology wards had relatively higher pain knowledge levels than nurses in other settings. This finding may reflect that pain management is generally recognized as an important clinical issue in oncology wards in Taiwan. Compared to other types of clinical settings, therefore, nurses on oncology wards may discuss relatively more pain-related issues continuing education and clinical case conferences. These discussions may increase oncology nurses’ pain manage-ment knowledge. Interestingly, nurses working in emergency rooms had similar pain knowl-edge levels, which may be because pain is a major problem in both units. In contrast, nurses working in the ICU had the lowest scores in pain knowledge. It’s difficult to explain why ICU nurses had the lowest pain knowledge scores compared to nurses working in other settings, though similar findings were found in a comparison of pain knowledge between hos-pice and ICU nurses.32Perhaps ICU patients are too sick to express their pain problems, which ICU nurses may perceive as indicating they have little or no pain. Another possibility is that pain control may not be as high a priority in the ICU, where the main goal is saving patients’ lives. Taken together, the results suggest that pain management concepts need to be strengthened across different clinical settings. In particular, the pain management knowledge of ICU nurses could be effectively improved by offering them more pain education and clini-cal case discussion guided by experienced pain experts, oncology nurses or physicians.
Although this study provides important infor-mation about nurses’ pain knowledge and iden-tifies factors that predict such knowledge, a few limitations still exist. First, the factors predicting
nurses’ pain knowledge explained only 24.2% of the variance. Other factors that influence nurses’ pain knowledge are not yet known. Some factors that might be examined include cultural values or attitudes toward pain, per-sonal pain experiences, clinical observations, experience taking care of patients with pain, clinical teaching about pain, habitual pain management procedures used in clinical set-tings, and influence of other health care provid-ers, for example, physicians.
The lack of appropriate pain management knowledge among physicians is known to be a major barrier to pain control in Taiwan.33 Be-cause of the close professional interaction between physicians and nurses, physicians’ knowledge about pain may be a major factor influencing nurses’ pain knowledge. Future re-search should examine in depth the sources and factors contributing to pain knowledge. Furthermore, nurse educators play an im-portant role in motivating students to learn about pain, yet nursing faculty themselves need more knowledge about pain management.34 Our findings suggest the necessity of examining pain knowledge of nurse faculty and clinical educators in Taiwan.
Our study, the first nationwide survey of nurses’ pain knowledge in Taiwan, provides im-portant information about knowledge deficits in pain management among Taiwanese nurses. These findings provide a clear blueprint for what Taiwanese nurses need to learn about pain management. Although our nurse subjects were all volunteers, the high response rate (94.6%) suggests that nurses in Taiwan recognize and support the meaning and importance of pain management as a critical nursing care issue to be improved. Therefore, development and test-ing of a nationwide nurses’ traintest-ing program in pain management is urgently needed to in-crease and disseminate pain education and knowledge in Taiwan.
Acknowledgments
The authors would like to express their grati-tude to the nurses who participated in the study and to Ms. Claire Baldwin for her English edit-ing of this manuscript. This study was partially supported by the National Science Council in Taiwan (NSC88-2314-B-038-107).
References
1. Department of Health, the Executive Yuan. Health and vital statistics in the Republic of China 1999. Taipei, Republic of China: Department of Health, Executive Yuan, 2000.
2. Ger LP, Ho ST, Wan JJ, et al. The prevalence and severity of cancer pain: a study of newly-diag-nosed cancer patients in Taiwan. J Pain Symptom Manage 1998;15:285–293.
3. Lai YL. Continuous hospice care for cancer pa-tients: three years experience. Taiwan Med J 1994;93: S98–S101.
4. Chiu TY. Pain control in terminal cancer pa-tients. Formosan J Med 1997;1:198–208.
5. U. S. Department of Health and Human Services. Management of cancer pain. Quick reference guide for clinicians, No.9. AHCPR Publication No. 94-0592. Rockville, MD. Agency for Health Care Policy and Research, U.S. Department of Health and Human Services, 1994.
6. Ryan P, Vortherms R, Ward S. Cancer pain: knowledge, attitudes of pharmacological manage-ment. J Ger Nurs 1994;20:7–16.
7. McCaffery M, Ferrell BR. Nurses’ knowledge about cancer pain: a survey of five countries. J Pain Symptom Manage 1995;10:356–367.
8. O’Brien S, Dalton JA, Konsler G, et al. The knowledge and attitudes of experienced oncology nurses regarding the management of cancer-related pain. Oncol Nurs Forum 1996;23:515–521.
9. Clarke EB, French B, Bilodeau ML, et al. Pain management knowledge, attitudes and clinical prac-tice: the impact of nurses’ characteristics and educa-tion. J Pain Symptom Manage 1996;11:18–31. 10. Ferrell BR, McCaffery M. Nurses’ knowledge about equianalgesia and opioid dosing. Cancer Nurs 1997;20:201–212.
11. McCaffery M, Ferrell BR. Nurses’ knowledge of pain assessment and management: how much prog-ress have we made? J Pain Symptom Manage 1997;14:175–188.
12. McMillan SC, Tittle M, Hagan S, et al. Knowledge and attitudes of nurses in veterans hospitals about pain management in patients with cancer. Oncol Nurs Forum 2000;27:1415–1423.
13. Glajchen M, Bookbinder M. Knowledge and per-ceived competence of home care nurses in pain man-agement: a national survey. J Pain Symptom Manage 2001;21:307–316.
14. Kubecka KE, Simon JM, Boettcher JH. Pain man-agement knowledge of hospital-based nurses in a rural Appalachian area. J Adv Nurs 1996;23:861–867. 15. Brunier G, Carson MG, Harrison DE. What do nurses know and believe about patients with pain? Results of a hospital survey. J Pain Symptom Manage 1995;10:436–445.
16. Tafas CA, Patiraki E, McDonald DD, et al. Testing an instrument measuring Greek nurses’ knowledge and attitudes regarding pain. Cancer Nurs 2002; 25:8–13.
17. Lai YH, Chen SC, Chang LI, et al. Beliefs about and knowledge of cancer pain and narcotic analge-sics and related factors in undergraduate student nurses. New Taipei J Nurs 2000;2(2):5–15.
18. Hsiu LN, Chang YP, Chen SH, et al. Beliefs about cancer pain and opioid analgesics and related factors among nurses. Chang Gung Nurs 2001;12:200–207. 19. Lai YH, Tsai LY, Chang TY, et al. Knowledge about cancer pain management among nurses in northern Taiwan. J Oncol Nurs 2002;2:1–16. 20. Ferrell BR, Grant M, Ritchey KJ, et al. The pain resource nurse training program: a unique approach to pain management. J Pain Symptom Manage 1993; 8:549–556.
21. Marin G, Marin BV. Research with Hispanic pop-ulations. Applied social research methods series, vol. 23. Newbury Park, CA: Sage, 1991.
22. Hollen CJ, Hollen CW, Stolte K. Hospice and hospital oncology unit nurses: a comparative survey of knowledge and attitudes about cancer pain. Oncol Nurs Forum 2000;27:1593–1598.
23. Pederson C, Parran L. Bone marrow transplant nurses’ knowledge, beliefs, and attitudes regarding pain management. Oncol Nurs Forum 1997;24: 1563–1571.
24. Salantera S, Lauri S, Salmi TT, et al. Nurses’ knowledge about pharmacological and nonpharma-cological pain management in Children. J Pain Symp-tom Manage 1999;18:289–299.
25. Ferrell BR, Eberts MT, McCaffery M, et al. Clini-cal decision making and pain. Cancer Nurs 1991;14: 289–297.
26. Holm K, Cohen F, Dudas S, et al. Effect of per-sonal pain experience on pain assessment. Image J Nurs Sch 1989;21(2):72–75.
27. Wessman AC, McDonald DD. Nurses’ personal pain experiences and their pain management knowledge. J Contin Educ Nurs 1999;30:152–157. 28. Paice JA, Mahon SM, Faut-Callahan M. Factors associated with adequate pain control in hopitalized postsurgical patients diagnosed with cancer. Cancer Nurs 1991;14:298–305.
29. Sheidler VR, McGuire DB, Grossman SA, et al. Analgesic decision-making skills of nurses. Oncol Nurs Forum 1992;19:1531–1534.
30. Furstenberg CT, Ahles TA, Whedon MB, et al. Knowledge and attitudes of health-care providers toward cancer pain management: a comparison of physicians, nurses, and pharmacists in the state of New Hampshire. J Pain Symptom Manage 1998;15:335– 349.
31. Closs SJ. Pain and elderly patients: a survey of nurses’ knowledge and experiences. J Adv Nurs 1996; 23:237–242.
32. Fothergill-Bourbonnais F, Wilson-Barnett J. A comparative study of intensive therapy unit and hos-pice nurses’ knowledge on pain management. J Adv Nurs 1992;17:362–372.
33. Ger LP, Ho ST, Wang JJ. Physicians’ knowledge and attitudes toward the use of analgesics for cancer pain management: a survey of two medical centers in Taiwan. J Pain Symptom Manage 2000;20:335–344. 34. Ferrell BR, McGuire DB, Donovan MI. Knowl-edge and beliefs regarding pain in a sample of nurs-ing faculty. J Prof Nurs 1993;979–988.