Clinical Toxicology (2009) 47, 161–168
Copyright © Informa UK, Ltd. ISSN: 1556-3650 print / 1556-9519 online DOI: 10.1080/15563650802077924
LCLT
ARTICLE
Common toxidromes of plant poisonings in Taiwan
Toxidromes of plant poisoningsTZENG JIH LIN1, LEWIS S. NELSON2, JIN LIAN TSAI3, DONG ZONG HUNG4, SHENG CHUAN HU5, HON MAN CHAN1, and JOU-FANG DENG6
1Department of Emergency, Kaohsiung Medical University Hospital and Department of Emergency Medicine, Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, and Faculty of Medicine, National Yang-Ming University, Taipei, Taiwan 2Department of Emergency Medicine, New York University School of Medicine, New York City Poison Control Center,
New York, USA
3Graduate Institute of Occupational Safety and Health, Kaohsiung Medical University, Kaohsiung, Taiwan
4Toxicology Center, China Medical University Hospital; Institute of Drug Safety, China Medical University, Taichung, Taiwan 5Department of Emergency Medicine, Buddhist Tzu Chi University and Buddhist Tzu Chi General Hospital, Hualien, Taiwan
6Division of Clinical Toxicology, Department of Internal Medicine, Taipei Veterans General Hospital and Faculty of Medicine, National Yang-Ming University, Taipei, Taiwan
Objective. To describe the toxidromes associated with plant poisonings in Taiwan. Methods. Retrospective review of acute single-plant exposures with clinical signs and symptoms reported between January 1987 and December 2006 by hospitals to the network of Taiwan Poison Control Centers. Recorded data included demographic data, intent of exposures, exposure routes, clinical findings, and therapeutic strategies. Results. There were 389 cases that met the criteria. Each case was placed into one of the expected toxidromes: anticholinergic, mucosal inflammation, gastroenteritis, acute multisystem organ failure, delayed multisystem organ failure, cholinergic, cardiac dysrhythmia, hepatotoxicity, dermatitis, seizures, and dyspnea. Anticholinergic poisoning was the most common toxidrome. Conclusion. Plant poisonings can be classified into recognizable toxicologic syndromes. These toxidromes may guide a clinician’s evaluation and management before a botanist can confirm the actual plant identity.
Keywords Plant; Epidemiology; Toxidrome; Poison control center
Introduction
Plant exposure is the seventh most commonly reported expo-sure to poison centers in the United States (1) and the third most frequent reported exposure to poison centers in the Ger-many (2). In Taiwan from 1985 to 1993, plant exposure was the 13th most common exposure leading to poison center contact (3). Most cases in Taiwan were unintentional and occurred in children under the age of 6 years. Because the concentration of toxin in most plants is low, intentional ingestions in adults, commonly with either suicidal intent or for abuse, are more likely to be associated with the develop-ment of signs and symptoms of poisoning.
The 23 million persons living in Taiwan are served by a network of four Poison Control Centers. We were interested in reviewing our plant exposure cases to determine the plants
most commonly linked to the development of specific clinical syndromes and how the patients were managed.
Methods
This study was performed with the support and acknowledg-ment of the Taiwan Departacknowledg-ment of Health. Prior to analyzing the data for this study, all patient-identifying data were removed to preserve confidentiality. We reviewed all expo-sures reported by healthcare providers to the four Poison Control Centers between January 1987 and December 2006. Only those cases with acute exposure to a single, identified plant, in which patients developed clinical signs and symp-toms were included. The toxicologists decided whether or not the signs and symptoms were related to the plant based on standard clinical findings and the known toxicologic proper-ties of the plant species. Cases involving consultations for information only, without exposures, were not included in this study. We recorded the name of the reporting hospital and identified the caller as a doctor, a nurse, or a pharmacist. We recorded demographic data, intent of exposure, exposure routes, clinical findings, and therapeutic strategies. The specific plant, quantity, and intent were based on the report of Received 22 October 2007; accepted 25 March 2008.
Address correspondence to Jou-Fang Deng, Division of Clinical Toxicology, Department of Internal Medicine, Taipei Veterans General Hospital, 201, Shih-pai Road, Section 2, Taipei, 11217 Taiwan. E-mail: [email protected]
Clinical Toxicology Downloaded from informahealthcare.com by Kaohsiung Medical University on 06/27/12
162
T.J. Lin et al.
the treating physician. Intent was either unintentionalexpo-sure (inadvertent, occupational, or herbal misuse) or inten-tional exposure (suicide, abuse, herbal errors, food or herbal adverse reaction). The clinical outcomes are based on the American Association of Poison Control Center National Poison Data System (1,3). We excluded cases of subacute (occurring repeatedly over several weeks or months) and chronic exposure (occurring repeatedly for many months or years), no clinical effect, possible causal effect, confirmed exposure with inadequate clinical information to determine its clinical outcome, unknown outcome, multiple plant expo-sure, or co-ingestants including alcohol (4).
Data analysis was performed using descriptive statistics. The signs and symptoms were then summarized according to the data recorded and adjudicated by the toxicologists. We classified our cases into one or more of the several recognized toxidromes derived from the plant poisoning literature (5).
Results
There were 1,414 cases related to plant poisoning during the 20-year period with 1,185 cases from the hospitals. There were 942 cases of acute exposure, of which 462 cases (49%) presented with signs and symptoms likely related to the exposure. After we excluded the cases with multiple plant exposure, or co-ingestants including alcohol, 389 cases remained. Of these, there were 182 males, 206 females, and 1 of unreported gender. The median age of the patients was 43 (range 0.5–83) years. There were 330 adults (85%), 25 children (<6 years), and 34 adolescents (7–18 years). Unin-tentional exposures accounted for 189 cases (49%; 147 adults, 42 adolescents and children), whereas intentional exposure accounted for 199 cases (51%; 182 adults, 17 ado-lescents and children); there was one case of unknown intent. Adults had more intentional exposures (55%), and the children and adolescents had more unintentional exposures (71%). The major route of exposure was oral (375 cases). There were 8 cases exposed by skin contact, 4 through the eyes, and 2 from unknown routes. There were 210 cases of mild toxicity, 153 cases of moderate toxicity, 23 cases of severe toxicity, and 3 deaths. The most common plants to which adults were exposed are mentioned in Table 1 (6–11). The most common plant exposures in children and adoles-cents are summarized in Table 2 (5–8,10,12,13). The tox-idromes, related plants, and patient outcomes are mentioned in Table 3 (5–53). The outcomes of the cases mostly were mild or moderate. Anticholinergic toxidrome was the most common and Datura spp. were the most frequently impli-cated plants. Twenty-nine patients with Datura poisoning were treated with physostigmine; no other antidote was administered. The three fatalities were due to Taxus
sumatrana (Miq.) de Laub. (two cases: hemolysis and
multi-ple organ failure; acute myocardial infarction) and Areca
catechu L (acute myocardial infarction).
Discussion
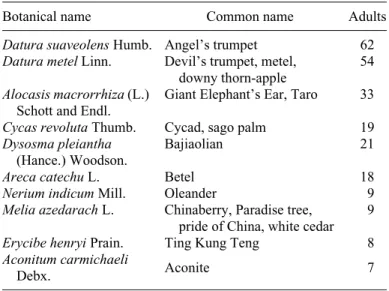
It is important to recognize clinical toxidromes associated with plant poisonings because typically the involved plant is not brought to the clinician by the patient (the plant may have been consumed completely or discarded). Often only the common name can be provided by the patient. Because a spe-cific plant often has several common names and because a common name may be applied to several unrelated plants, or be extended across an entire genus, the utility of this information Table 1. Ten most common poisonous plants in adults
Botanical name Common name Adults
Datura suaveolens Humb. Angel’s trumpet 62 Datura metel Linn. Devil’s trumpet, metel,
downy thorn-apple
54 Alocasis macrorrhiza (L.)
Schott and Endl.
Giant Elephant’s Ear, Taro 33 Cycas revoluta Thumb. Cycad, sago palm 19 Dysosma pleiantha
(Hance.) Woodson.
Bajiaolian 21
Areca catechu L. Betel 18
Nerium indicum Mill. Oleander 9
Melia azedarach L. Chinaberry, Paradise tree, pride of China, white cedar
9 Erycibe henryi Prain. Ting Kung Teng 8 Aconitum carmichaeli
Debx. Aconite 7
Table 2. Ten most common poisonous plants in adolescents and children
Botanical name Common name Children adolescents Total Alocasis
macrorrhiza (L.) Schott and Endl.
Giant Elephant’s Ear, Taro
4 7 11
Aleurites fordii Hemsl.
Tung Nut, Tung Oil Tree, Chinawood Oil Tree 0 7 7 Datura suaveolens Humb. Angel’s trumpet 2 4 6
Datura metel Linn. Devil’s trumpet, metel, downy thorn-apple 3 2 5 Cycas revoluta Thumb. Cycad, sago palm 1 4 5 Dieffenbachia spp. Dieffenbachia, Dumbcane 3 1 4
Lantana camara L. Lantana 2 1 3
Hura crepitans L. White cedar, sandbox tree
0 3 3
Areca catechu L. Betel 2 0 2
Clinical Toxicology Downloaded from informahealthcare.com by Kaohsiung Medical University on 06/27/12
163
Table 3. Toxidromes a nd ou tc omes of rela ted plants. To xidrom e T oxic me chanism B otanica l nam e Common n ame Toxin O utcome (No. patie
nts) Mechanism total (no. pt) Toxidrome total (no. pt) Mild Moderate Severe Fatal Anticholin erg ic P ar as ympa tholytic Datura suaveolens Humb. Ang el’s t rumpe t (6) A
tropine, scopolamine and other anticholinergic alkaloids (4, 13,
14) 15 47 5 0 67 136 Datura me tel Linn. Devil’s trumpet, metel, d o wny thorn -ap ple (5) 17 43 0 0 60 Datura tatula Linn. Purple Thorn Apple (15) 0 4 1 0 5 Solanum ac uleatissimum Ja cquin. De adly nightsha d e, p o tato (6) Solanine and anticholinergic alka loids (5, 17 ) 11 0 0 2 Solanum nigru m L. Black nightshade, pota to (6) 01 0 0 1 Solanum verbascifolium L. De adly nightsha d e, p o tato (6) 01 0 0 1 Mu cosal Inflammation M uco sal irritant Aloc asia macrorrhiza
(L.) Schott and Endl.
Giant Elephant’ s Ear, Taro ( 6 , 7) Calcium ox alate (4, 7, 17) 37 7 0 0 4 4 5 5 Dieffenbac hia ac ulata (Lodd .) Swe et. Die ffenba chia, D u mbcan e (6) 41 0 0 5 Dieffenbac hia am oena cv. ‘Bull’. Die ffenba chia, D u mbcan e (6) 40 0 0 4 Alocasia cucullata Schott & Endl. No 0 1 0 0 1 Caladium x hortulanun Birds ey. Caladium (6) 1 0 0 0 1 Gastro enteritis Gastrointestinal irritant Me lia azedarach L . Chinaberry, Paradise tree, prid e of China, w h ite cedar (6) Tetranortriterp en e (4, 18) 63 0 0 9 5 0 Aleu rites fordii Hemsl. Tung Nut, Tu ng Oil Tree , Chinaw ood O il Tre e (4, 11 ) Unknown (4, 11) 7 0 0 0 7 N a rcis sus tazetta var.c h inensis Daffodil, pap er white na rc is su s (6 ) Lyco rine a nd related ph ena n th ridin e (4) 51 0 0 6 Pac h yrrhizus ero sus Linn. No Rote none (4) 4 2 0 0 6 Derris trifoliata Lour. N o R ote none (19) 4 2 0 0 6 (Continue d )
Clinical Toxicology Downloaded from informahealthcare.com by Kaohsiung Medical University on 06/27/12
Table 3. (Co ntinued ) To xidrom e T oxic me chanism B otanica l nam e Common n ame Toxin O u
tcome (No. patie
nts) Mechanism total (no. pt) Toxidrome total (no. pt) Mild Moderate Severe Fatal Croton tigliu m L. Croton (9) P hobol este r (2 0) 3 1 0 0 4 Lantana camara L. Lantana (6) U nknown 1 2 0 0 3 Hura crepitans L. Wh ite ceda r (6), san dbox tree (12) Hurin (4) 3 0 0 0 3 Aloe ve ra L.var.chinensis 〈Haw .〉 Berger Aloe ve ra (6) B arbalo in (4) 2 0 0 0 2 Daphne genk wa Sieb. Et Zucc. Lilac daphne (5) M ezerein (21) 0 1 0 0 1 Ricinu s commu nis Linn. Castor bean (6) R icin (4) 0 1 0 0 1 Hippeastrum hyb ridum Hort. Amaryllis (5) L y co ri n e an d related ph en an th rid in e (4, 22) 10 0 0 1 Phy tolacca acinosa Ro xb. No Phytolacc atoxin (4) 10 0 0 1 Acute multisystem organ failure Cyanid e poisoning Cyc a s rev o luta Thumb . Cycad, sago palm (5) C yc asin and neoc ycasin (4, 23) 23 1 0 0 2 4 M a ni ho t e sc u le n ta Crantz . Cas sava (6), M anihot, ta pioca (9) Lina marin an d lotaustralin (4, 24, 25) 41 0 0 5 Hydrangea macrophylla (Thun b.) Se r. No Hydrangin (4 ) 1 0 0 0 1 Delay ed mu ltisystem organ failure Mitotic inhibitors Dysosma pleianth a (Hance .) W oodson. Bajiaolian (8) P odophyllotoxin (8) 36 1 2 0 2 1 Catharanthus rose us (L .) G. Doy. Rose periwinkle (6) V inca alka loids (4) 31 0 0 4 Cytotoxicity Tripterygium wil fo rdii Hook. f.
Lei Gong Ten
g (26) Unknown 3 2 0 0 5 Cholin erg ic P ar as ympa thomi metic Areca catec h u L. Betel (9) A recholine (9) 1 1 6 2 1 20 Erycibe henryi Pra in. Ting K ung Ten g (10) Tropan e a lkaloids (10) 44 0 0 8 Ca rdia c dysrhythmia cardiac glycoside Nerium indicum Mil l. O le ander (6) O leand rin and neriine (4, 27) 63 0 0 9 Cerbera m anghas L. pink-eye d c erb era , Sea Mang o (22, 28, 2 9 ) Cerberoside (22) 1 2 0 0 3 A d en iu m ob es um (For sk. ) B alf. Ex Ro em. E t Schult. No Conva llatoxin (30) 01 0 0 1 Digitalis purpure a L. Purple fox g love (9) D igitoxin (9 , 31) 0 1 0 0 1
Clinical Toxicology Downloaded from informahealthcare.com by Kaohsiung Medical University on 06/27/12
165
S o dium c h annel agonists Aco n itum carm ic haeli Debx . Aconite (6) A conitine and related alka loids (4, 32 ) 32 2 0 7 Rhodo dendron spp. Az alea (6 ) G rayanotox in s (4, 33) 01 0 0 1 S o dium a nd calc ium chan nel blo cker Taxus sumatra n a ( M iq.) de La ub. Yew (6) T axine alkaloids (4, 34–37) 00 0 2 2 Hepatotoxicity Hepatotox icity Lycopodium serratumThunb. var. longipetio
la tum*(38) No Unknown 6 1 0 0 7 15 Breynia officinalis Hemsl. Chi R Y un (39, 40) Unknown (39, 40) 21 1 0 4 C rin um asi a ti cu m L . ( 4 1 ) No Unknown 3 0 0 0 3 Poly gonum multifloru m Thunb.* (42) He Shou Wu (42) Unknown 1 0 0 0 1 Dermatitis Irrit ation o r Allergy Eupho rbia tirc u calli L. Penc il tree, Milkbush, Fing er tree, Rubber euphorbia (5) Diterpene esters (4 ) 60 0 0 6 1 4 Eupho rbia pulche rrima Willd. et. Klotz. Poinsettia, Christmas flower (5) Diterpene esters (4, 43) 20 0 0 2 Urtica thunbe rgian a sie b . (44) Nettle (44) Histamine, sero tonin, substa nce P, oxalic ac id a nd tartaric acid (44, 45) 20 0 0 2 Rhus vern iciflua Stok es. N o U nknown (4, 46) 2 0 0 0 2 Hedera helix L. Oakleaf ivy , Common iv y (4, 6, 9, 4 9 ) Hederin, falcarinol (4, 47) 10 0 0 1 Eupho rbia milii C h . des Moulins. Crow n of thorn s (6) D iterpene esters (4) 10 0 0 1 Conv ulsion/Se iz ure B
lock the inhibitory effe
cts of GABA Stryc hnos nuxv o mica L. § Strychnine (6) S tryc hnine (4, 48) 30 0 0 3 5 An a n tagonist of
pyridoxine and gastroin
testinal irritant Ginkgo biloba Linn . § Gink o (6) 4 -O - meth ylpyridoxne (4, 49, 50) 20 0 0 2 Dyspnea U nknown Saurop us And rogy nus (L .) Merr . Sauropus albicansAsin-A sin Chekor Manis (51) Unknown (51) 1 1 0 0 2 To tal num bers of patie nts 210 153 2 3 3 389 389 * Only mild signs and sy m p toms of gastroenteritis in our ca se series withou t hepatotoxicity recorded. § On ly mild sign s and symptoms of gastro enteriti s in ou
r case series without
seizures recorded.
Clinical Toxicology Downloaded from informahealthcare.com by Kaohsiung Medical University on 06/27/12
166
T.J. Lin et al.
is limited and possibly misleading. Healthcare providerssel-dom were able to identify the plants without the help of the Poison Control Centers or botanists.
In many situations, the emergency physician must manage a clinically ill patient before definitive identification of the plant is available. Typically, these patients are managed based on the clinical condition rather than on the knowledge of an exposure or suspicion of a toxin (5). We classified our clinically ill patients into one of the commonly described plant-related tox-idromes. Understanding this classification is particularly useful when the toxidrome manifested by the patient is not compati-ble with the common name of the plant described by the patient. Categorizing a patient’s clinical findings into one of these plant-related toxidromes may allow proper therapy to be administered despite specific insight into the exposure.
Anticholinergic syndrome was the most common encoun-tered plant poisoning in hospitals, accounting for 136 cases. Many plants may cause this syndrome, including plants of the genus Atropa, Brugmansia, Datura, Hyoscyamus, Solandra, and Solanum (5). In our adult patients, Datura suaveolens Humb. was the most commonly encountered and shown in Table 1.
Mucosal inflammation following plant exposure is caused commonly by the local irritation of calcium oxalate crystals that are released in proximity to the mucosa on chewing. In our study, 55 such cases were identified in Table 3 (5,8,18).
Alocasia macrorrhiza (L.) Schott and Endl. was the leading
plant poisoning in adolescents and children as shown in Table 2. Our patient who consumed the root of this plant pre-sented with signs and symptoms of calcium oxalate poison-ing with mucosal inflammation.
Gastrointestinal irritation (nausea, vomiting, diarrhea, or abdominal pain) occurred in 50 cases in our series due to 13 distinct species of plants noted in Table 3.
There were 30 cases of acute multisystem organ failure, caused mainly by plants that contain cyanogenic poisons.
Delayed multisystem organ failure occurred in 30 cases. Plants that contain colchicine-like mitotic inhibitors may induce gastrointestinal symptoms, abdominal pain, diarrhea, peripheral neuropathy, bone marrow suppression, and cardio-vascular collapse. Tripterygium wilfordii Hook. F., contain-ing an unidentified toxin, causes profuse vomitcontain-ing and diarrhea, leukopenia, renal failure, profound hypotension, shock, and cardiac toxicity (54).
Cholinergic symptoms may also develop in patients with plant poisoning. Erycibe henryi Prain. produces muscarinic clinical effects. Nicotinic clinical findings may be produced by betel nut, Areca catechu L. (10,11,55). There were 20 cases of poisoning by Erycibe henryi Prain. and 8 cases of
Areca catechu L. poisonings in our series (one of whom
died). Alkaloids in betel nut, such as arecoline, may play a contributing role in coronary artery vasoconstriction due to sympathomimetic effects on vessels with abnormal endothe-lium in a manner analogous to nicotine (55).
Cardiac toxicity may be due to effect of cardiac glycoside,
blocker. In our series, there were 24 cases of plant poisonings with cardiac toxicity. There were 8 cases of Aconitum
car-michaeli Debx. and Rhododendron spp. associated with
sodium channel agonists. These patients developed cardiac dysrhythmias in addition to burning in the mouth, salivation, vomiting, diarrhea, and a tingling sensation in the skin (5,33). There were two deaths caused by Taxus sumatrana (Miq.) de Laub., which results in sinus bradycardia, premature ventric-ular contractions, atrioventricventric-ular conduction defects, or ven-tricular tachydysrhythmias (5,35–38). In the two Taxus fatalities, one died from hemolysis and multiple organ failure and the other from acute myocardial infarction.
Breynia officinalis Hemsl., Lycopodium serratum Thunb.
var. longipetiolatum, Polygonum multiflorum Thunb., and
Cri-num asiaticum L. are reported to cause hepatotoxicity (39–43). Breynia officinalis Hemsl. resulted in hepatotoxicity in four
cases; the other plants caused mild gastrointestinal irritation. Dermatitis (allergic or irritant) is common after contact with certain plants. Ingestion of these same plants can often result in gastroenteritis. There were 14 cases manifesting matitis. Hedera helix L. usually causes allergic contact der-matitis (47). Both Urtica thunbergiana sieb. and Rhus
verniciflua Stokes. produced itching and contact dermatitis,
similar to other more widely reported species of the same genus (5,45–47).
In our case series, we had five patients poisoned by the
Strychnos nux-vomica L. and Ginkgo biloba Linn. Strychnine
interferes with the negative feedback function of glycine, resulting in excessive motor neuron activity (56,57). The tox-icity of Ginkgo biloba Linn. comes from 4-O-methylpyridox-ine, a competitive antagonist of pyridox4-O-methylpyridox-ine, which is needed for GABA synthesis (50,51). However, our cases had only mild gastrointestinal irritation without seizures.
Chronic use of Sauropus Androgynus (L.) Merr. has caused constrictive bronchiolitis obliterans (52). Our three cases were single exposures and none developed clinical toxicity.
Conclusions
Anticholinergic plants are the primary cause of clinical poi-soning from plants in adults, and mucosal irritants are prima-rily responsible for clinical effects in children following plant exposure. Plants produce predictable syndromes that can help clinicians in the absence of details about the specific exposure. If the plant implicated in an exposure cannot be specifically identified in a rapid fashion, the poisoning syndromes may help the clinician evaluate and manage the poisoned patients.
References
1. Lai MW, Klein-Schwartz W, Rodgers GC, Abrams JY, Haber DA, Bronstein AC, Wruk KM. 2005 Annual Report of the American Associ-ation of Poison Control Centers’ nAssoci-ational poisoning and exposure
data-Clinical Toxicology Downloaded from informahealthcare.com by Kaohsiung Medical University on 06/27/12
Clinical Toxicology vol. 47 no. 2 2009
Toxidromes of plant poisonings
167
2. Wolfle J, Kowalewski S. Epidemiology of ingestions in a regional poison control center over twenty years. Vet Hum Toxicol 1995; 37:367–368.
3. Yang CC, Wu JF, Ong HC, Hung SC, Kuo YP, Sa CH, Chen SS, Deng JF. Taiwan National Poison Center: epidemiologic data 1985–1993. J Toxicol Clin Toxicol 1996; 34:651–663.
4. Eaton DL, Klaassen CD. Principles of toxicology. In: Klaassen CD, ed. Casarett & Doull’s Toxicology: The Basic Science of Poisons. 6th ed. New York: McGraw-Hill; 2001: 14.
5. Nelson LS, Shih RD, Balick MJ, eds. Handbook of Poisonous and Inju-rious Plant. 2nd ed. New York, USA: Springer; 2007.
6. Russell AB. Poisonous Plants of North Carolina, Raleigh: North Carolina State University; 1996. http://www.ces.ncsu.edu/depts/hort/ consumer/poison/poison.htm. Accessed 16 January 2008.
7. Olson KR, Anderson IB, Benowitz NL, Blanc PD, Clark RF, Kearney TE, Osterloh JD, eds. Poisoning and Drug Overdose. 5th ed. New York, USA: The McGraw-Hill Companies, Inc.; 2007.
8. Lin TJ, Hung DZ, Hu WH, Yang DY, Wu TC, Deng JF. Calcium oxalate is the main toxic component in clinical presentations of alocasis macrorrhiza (L) Schott and Endl poisonings. Vet Hum Toxicol 1998; 40:93–95.
9. Kao WF, Hung DZ, Tsai WJ, Lin KP, Deng JF. Podophyllotoxin intox-ication: toxic effect of Bajiaolian in herbal therapeutics. Hum Exp Tox-icol 1992; 11:480–487.
10. Hoffman RS, Nelson LS, Howland MA, Lewin NA, Flomenbaum NE, Goldfrank LR, eds. Manual of toxicologic emergencies. New York, USA: The McGraw-Hill Compaines, Inc.; 2007.
11. Huang HH, Yen DH, Wu ML, Deng JF, Huang CL, Lee CH. Acute Erycibe henryi Prain ("Ting Kung Teng") poisoning. Clin Toxicol (Phila) 2006; 44:71–75.
12. Lin TJ, Hsu CL, Lee KH, Shiu LL, Deng JF. Two outbreaks of acute Tung Nut (Aleurites fordii) poisoning. J Toxicol Clin Toxicol 1996; 34:87–92.
13. Thumm EJ, Bayerl C, Goerdt S. [Allergic reaction after contact with Hura crepitans (sandbox tree)]. Hautarzt 2002; 53:192–195 (German). 14. Havelius U, Asman P. Accidental mydriasis from exposure to
Angel’s trumpet (Datura suaveolens). Acta Ophthalmol Scand 2002; 80:332–335.
15. Testa P, Fontanelli G. Acute poisoning with atropine-like alkaloids of Datura Metel. Clin Ter 1988; 125:203–211 (Italian).
16. Savela M. Lepidoptera and Some Life Forms, 12 April 2006. http:// www.ces.ncsu.edu/depts/hort/consumer/poison/poison.htm. Accessed 16 Januray 2008.
17. Towers RP. A case of poisoning by Solanum nigrum. Ir J Med Sci 1953; 6:77–80.
18. Pedaci L, Krenzelok EP, Jacobsen TD, Aronis J. Dieffenbachia species exposures: an evidence-based assessment of symptom presentation. Vet Hum Toxicol 1999; 41:335–338.
19. Kiat TK. Melia azedarach poisoning. Singapore Med J 1969; 10:24–28. 20. Yenesew A, Mushibe EK, Induli M, Derese S, Midiwo JO, Kabaru JM, Heydenreich M, Koch A, Peter MG. 7a-O-methyldeguelol, a modified rotenoid with an open ring-C, from the roots of Derris trifoliate. Phy-tochemistry 2005; 66:653–657.
21. Wedin GP, Neal JS, Everson GW, Krenzelok EP. Castor bean poison-ing. Am J Emerg Med 1986; 4:259–261.
22. Ronlan A, Wickberg B. The structure of mezerein, a major toxic princi-ple of Daphne mezereum L. Tetrahedron Lett 1970; 49:4261–4264. 23. Chiu NY, Chang KH, eds. The Illustrated Medicinal Plants of Taiwan.
4th ed. Taipei, Taiwan: SMC Publishing, Inc.; 1995 (Chinese). 24. Chang SS, Chan YL, Wu ML, Deng JF, Chiu T, Chen JC, Wang FL,
Tseng CP. Acute Cycas seed poisoning in Taiwan. J Toxicol Clin Toxi-col 2004; 42:49–54.
25. Padmaja G. Cyanide detoxification in cassava for food and feed uses. Crit Rev Food Sci Nutr 1995; 35:299–339.
26. Aregheore EM, Agunbiade OO. The toxic effects of cassava (manihot esculenta grantz) diets on humans: a review. Vet Hum Toxicol 1991; 33:274–275.
27. Zhang YG, Huang GZ, Wang HJ, Wu ZB, Xing SL. An experimen-tal pathological study of acute Lei Gong Teng (Tripterygium wilfordii Hook) intoxication in rats. Acta Acad Med Wuhan 1984; 4:75–81.
28. Shaw D, Pearn J. Oleander poisoning. Med J Aust 1979; 2:267–269. 29. Eddleston M, Persson H. Acute plant poisoning and antitoxin
antibod-ies. J Toxicol Clin Toxicol 2003; 41:309–315.
30. Radford DJ, Gillies AD, Hinds JA, Duffy P. Naturally occurring cardiac glycosides. Med J Aust 1986; 144:540–544.
31. Yamauchi T, Abe F. Cardiac glycosides and pregnanes from Adenium obesum (studies on the constituents of Adenium. I). Chem Pharm Bull (Tokyo) 1990; 38:669–672.
32. Lacassie E, Marquet P, Martin-Dupont S, Gaulier JM, Lachatre G. A non-fatal case of intoxication with foxglove, documented by means of liquid chromatography-electrospray-mass spectrometry. J Forensic Sci 2000; 45:1154–1158.
33. Chan TY, Tomlinson B, Tse LK, Chan JC, Chan WW, Critchley JA. Aconitine poisoning due to Chinese herbal medicines: a review. Vet Hum Toxicol 1994; 36:452–455.
34. Choi SH, Lee SW, Hong YS, Lim SI. Grayanotoxin poisoning from flower of Rhododendron mucronulatum in humans. Bull Environ Con-tam Toxicol 2007; 78:11–12.
35. Shen YC, Hsu SM, Lin YS, Cheng KC, Chien CT, Chou CH, Cheng YB. New bicyclic taxane diterpenoids from Taxus sumatrana. Chem Pharm Bull (Tokyo) 2005; 53:808–810.
36. Shen YC, Cheng KC, Lin YC, Cheng YB, Khalil AT, Guh JH, Chien CT, Teng CM, Chang YT. Three new taxane diterpenoids from Taxus sumatrana. J Nat Prod 2005; 68:90–93.
37. Shen YC, Wang SS, Pan YL, Lo KL, Chakraborty R, Chien CT, Kuo YH, Lin YC. New taxane diterpenoids from the leaves and twigs of Taxus sumatrana. J Nat Prod 2002; 65:1848–1852.
38. Shen YC, Pan YL, Lo KL, Wang SS, Chang YT, Wang LT, Lin YC. New taxane diterpenoids from Taiwanese Taxus sumatrana. Chem Pharm Bull (Tokyo) 2003; 51:867–869.
39. Horowitz RS, Feldhaus K, Dart RC, Stermitz FR, Beck JJ. The clinical spectrum of Jin Bu Huan toxicity. Arch Intern Med 1996; 156:899–903. 40. Lin TJ, Su CC, Lan CK, Jiang DD, Tsai JL, Tsai MS. Acute poisonings with Breynia officinalisan outbreak of hepatotoxicity. J Toxicol Clin Toxicol 2003; 41:591–594.
41. Lin TJ, Tsai MS, Chiou NM, Deng JF, Chiu NY. Hepatotoxicity caused by Breynia officinalis. Vet Hum Toxicol 2002; 44:87–88.
42. Chai B. Crinum asiaticum L cause hepatotoxicity – a case report. New Med Sci 1985; 5:253 (Chinese).
43. Cardenas A, Restrepo JC, Sierra F, Correa G. Acute hepatitis due to shen-min: a herbal product derived from Polygonum multiflorum. J Clin Gastroenterol 2006; 40:629–632.
44. Santucci B, Picardo M, Cristaudo A. Contact dermatitis from Euphorbia pulcherrima. Contact Dermatitis 1985; 12:285–286.
45. Youn NH, You DO, Lee YH, Park SD. Pathogenesis of Contact Urticaria Induced by Nettle (Urtica Thunbergiana). Korean J Dermatol 2003; 41:602–608 (Korean).
46. Fu HY, Chen SJ, Chen RF, Ding WH, Kuo-Huang LL, Huang RN. Identification of oxalic acid and tartaric acid as major persistent pain-inducing toxins in the stinging hairs of the nettle, Urtica thunbergiana. Ann Bot (Lond) 2006; 98:57–65.
47. Gladman AC. Toxicodendron dermatitis: poison ivy, oak, and sumac. Wilderness Environ Med 2006; 17:120–128.
48. Hausen BM, Brohan J, Konig WA, Faasch H, Hahn H, Bruhn G. Aller-gic and irritant contact dermatitis from falcarinol and didehydrofalcar-inol in common ivy (Hedera helix L.). Contact Dermatitis 1987; 17:1–9. 49. Shadnia S, Moiensadat M, Abdollahi M. A case of acute strychnine
poi-soning. Vet Hum Toxicol 2004; 46:76–79.
50. Kajiyama Y, Fujii K, Takeuchi H, Manabe Y. Ginkgo seed poisoning. Pediatrics 2002; 109:325–327.
51. Wada K, Ishigaki S, Ueda K, Sakata M, Haga M. An antivitamin B6, 4′-methoxypyridoxine, from the seed of Ginkgo biloba L. Chem Pharm Bull (Tokyo) 1985; 33:3555–3557.
Clinical Toxicology Downloaded from informahealthcare.com by Kaohsiung Medical University on 06/27/12
168
T.J. Lin et al.
52. Wang JS, Tseng HH, Lai RS, Hsu HK, Ger LP. Sauropus androgynus-con-strictive obliterative bronchitis/bronchiolitis–histopathological study of pneumonectomy and biopsy specimens with emphasis on the inflammatory process and disease progression. Histopathology 2000; 37:402–410. 53. Schildknecht H, Maurer. Die Struktur des Mezereins aus der Frucht des
Seidelbasts Daphne mezereum. Chemikerzeitung 1970; 94:894. 54. Chou WC, Wu CC, Yang PC, Lee YT. Hypovolemic shock and
mortal-ity after ingestion of Tripterygium wilfordii hook F.: a case report. Int J Cardiol 1995; 49:173–177.
55. Deng JF, Ger J, Tsai WJ, Kao WF, Yang CC. Acute toxicities of betel nut: rare but probably overlooked events. J Toxicol Clin Toxicol 2001; 39:355–360.
56. Snyder SH. Fifth Gaddum Memorial Lecture, University of Bristol, September 1974, The glycine synaptic receptor in the mammalian cen-tral nervous system. Br J Pharmacol 1975; 53:473–484.
57. Young AB, Snyder SH. The glycine synaptic receptor: evidence that strychnine binding is associated with the ionic conductance mechanism. Proc Natl Acad Sci USA 1974; 71:4002–4005.
Clinical Toxicology Downloaded from informahealthcare.com by Kaohsiung Medical University on 06/27/12