I
NTERESTING
I
MAGE
Focal Cerebral Hypermetabolism Due to Nonconvulsive Status
Epilepticus Mimicking Metastasis in Staging a Patient With Lung
Cancer by FDG PET/CT
Szu-Kuan Yang, MD,* Yu-Lin Pei, MD,* Chia-Hung Kao, MD,†‡ Jainn-Shiun Chiu, MD,§¶
and Guang-Uei Hung, MD§¶
Abstract: Here we report a case of a 77-year-old man referred for staging his
lung cancer by FDG PET/CT. In addition to the primary lung cancer, focal hypermetabolism was noted in right hemisphere of brain, which was initially considered as metastasis. However, there was no significantly morphologic abnormality on the coregistered CT image. Further MRI study revealed no evidence of tumor, metastasis, inflammation/infection, or infarction over the corresponding regions. The associated symptoms/signs included left limb weakness, mental confusion, and occasional right facial twitching. Electro-encephalography revealed typical findings of active epilepsy. A nonconvul-sive status epilepticus originating at right centroparietal area was finally concluded.
Key Words: epilepsy, lung cancer, FDG, PET/CT
(Clin Nucl Med 2011;36: 394 –396)
REFERENCES
1. Gupta NC, Nicholson P, Bloomfield SM. FDG-PET in the staging work-up of patients with suspected intracranial metastatic tumors. Ann Surg. 1999;230: 202–206.
2. Takalkar AM, El-Haddad G, Lilien DL, et al. Simultaneous demonstration of metabolic lesions consistent with Alzheimer disease and brain metastases on FDG-PET imaging. Clin Nucl Med. 2008;33:438 – 440.
3. Talanow R, Ruggieri P, Alexopoulos A, et al. PET manifestation in different types of pathology in epilepsy. Clin Nucl Med. 2009;34:670 – 674. 4. Coleman RE, Hoffman JM, Hanson MW, et al. Clinical application of PET for
the evaluation of brain tumors. J Nucl Med. 1991;32:616 – 622.
5. Meyer PT, Spetzger U, Mueller HD, et al. High F-18 FDG uptake in a low-grade supratentorial ganglioma: a positron emission tomography case report. Clin Nucl Med. 2000;25:694 – 647.
6. Lee BY, Newberg AB, Liebeskind DS, et al. FDG-PET findings in patients with suspected encephalitis. Clin Nucl Med. 2004;29:620 – 625.
7. Mascarenhas NB, Lam D, Lynch GR, et al. PET imaging of cerebral and pulmonary nocardia infection. Clin Nucl Med. 2006;31:131–133.
8. Fischman AJ, Thornton AF, Frosch MP, et al. FDG hypermetabolism associ-ated with inflammatory necrotic changes following radiation of meningioma.
J Nucl Med. 1997;38:1027–1029.
Received for publication July 2, 2010; revision accepted September 10, 2010. From the *Department of Neurology, Chang Bing Show Chwan Memorial
Hospital, Changhua, Taiwan; †Department of Nuclear Medicine and PET Center, China Medical University Hospital, Taichung, Taiwan; ‡School of Medicine, China Medical University, Taichung, Taiwan; §Department of Nuclear Medicine, Chang Bing Show Chwan Memorial Hospital, Changhua, Taiwan; and ¶Department of Biomedical Imaging and Radiological Science, China Medical University, Taichung, Taiwan.
Reprints: Guang-Uei Hung, MD, Department of Nuclear Medicine, Chang Bing Show Chwan Memorial Hospital, 6 Lukon Road, Lukong Town, Changhua Shien, Taiwan 505, Taiwan. E-mail: [email protected].
Copyright © 2011 by Lippincott Williams & Wilkins ISSN: 0363-9762/11/3605-0394
Clinical Nuclear Medicine • Volume 36, Number 5, May 2011
FIGURE 2. MRI of brain, shown here with
diffu-sion-weighted (A), FLAIR (B), T2-weighted (C), and T1-weighted with contrast enhancement (D), was performed for further evaluation. Mild hyper-intensity signal was noted in right parietal and occipital cerebral cortices on diffusion-weighted image, suggestive of ischemic change (A, arrows). Except for this, multifoci hypointensity signal le-sions were noted over left parietal lobe associated with peripheral white matter demyelination, con-sistent with old infarction changes (B–D, arrows). No definite evidence of indicating metastasis, pri-mary brain tumor, or inflammation/infection was demonstrated.
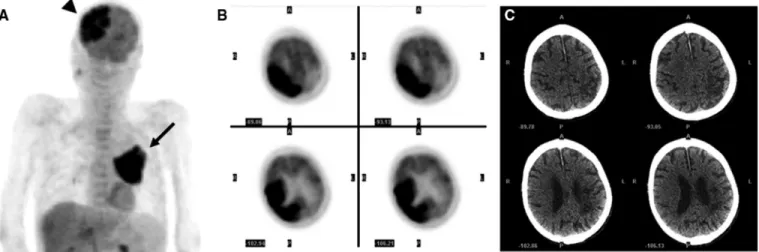
FIGURE 1. The presented case was of a 77-year-old man who had ever suffered from old cerebral infarction in left side of the
brain. He was referred for FDG PET/CT for whole-body staging due to a newly diagnosed squamous cell carcinoma of lung. A, The PET images (maximal intensity projection) revealed large hypermetabolic lesions in left upper lobe of lung, with a maxi-mum standard uptake value of 16.90 at 1 hour, consistent with the primary lung cancer (arrow). In addition, there were sig-nificantly hypermetabolic activities involving right hemisphere of brain (arrowhead), with a maximum standard uptake value of 15.85, which were initially considered as cerebral metastases of lung cancer.1,2B, The transaxial PET images localized the
hypermetabolic activities in right parieto-occipital cerebral cortices, basal ganglia, and thalamus. C, However, the coregistered CT images of PET/CT revealed no definitely morphologic abnormality on the corresponding regions of brain. In addition to metastasis, the differential diagnosis of focal cerebral hypermetabolism includes epilepsy,3primary brain tumor,4,5and
inflam-mation/infection.6 – 8
Clinical Nuclear Medicine • Volume 36, Number 5, May 2011 Focal Cerebral Hypermetabolism
FIGURE 3. The associated symptoms/signs of the patient included left limb weakness, mental confusion, and occasional right
facial twitching. Impressed by nonmalignant processes, neurologist was consulted and electroencephalography revealed sharp spike-wave with phase reversal at C4 and P4 positions, which were typical findings for active epilepsy with respect to epilepto-genic focus at right centroparietal lobe. Combining the findings of imaging studies, electroencephalography and clinical mani-festations, a “nonconvulsive status epilepticus” was finally concluded.
Yang et al Clinical Nuclear Medicine • Volume 36, Number 5, May 2011