Increase the risk of intellectual disability
in children with scabies
A nationwide population-based cohort study
Jui-Ming Liu, MD
a,b,c, Ren-Jun Hsu, PhD
c,d,e, Fung-Wei Chang, MD
f, Chia-Lun Yeh, MD
a,g,
Chun-Fa Huang, PhD
h,i, Shu-Ting Chang, MD
j, Nan-Chang Chiu, MD
k,l, Hung-Yang Chang, MD
k,l,
Hsin Chi, MD
k,l, Chien-Yu Lin, MD
m,n,∗Abstract
Scabies is a common and distressing disease caused by the mite Sarcoptes scabiei var. hominis. Psychiatric disorder in childhood is an important disease and easily neglected. There are several similarities in scabies and psychiatric disorders in childhood (PDC). Both of them may present with pruritus. They are relatively common in patients with lower socioeconomic status and crowded
environment. Furthermore, immune-mediated inflammatory processes play a role in the pathophysiology in both diseases. An
association between scabies and psychiatric disorders may exist. This nationwide population-based cohort study utilized data from the National Health Insurance Research Database to investigate the relationship between scabies and PDC. A total of 2137 children
with scabies were identified as the study group and 8548 age- and sex-matched children were selected as the control group. A total
of 607 (5.68%) children developed PDC during the 7-year follow-up period. The overall incidences of PDC are similar but patients with scabies had a higher risk of developing intellectual disability (ID) (scabies group vs control group: 1.3% vs 0.6%, adjusted hazard ratio:
2.04 and 95% confidence interval: 1.25–3.32). The immune-mediated inflammatory processes of both diseases were reviewed and
may contribute to the 104% increased risk of interleukin in patients with scabies. We suggest a more comprehensive management in treating patients with scabies or ID. Early and comprehensive treatment of scabies and other risk factors may decrease the risk of subsequent ID. When we approach patients with ID, concurrent evaluation of scabies and other risk factors may contribute to successful management.
Abbreviations:ADHD= attention deficit hyperactivity disorder, aHR = adjusted hazard ratio, CI = confidence interval, ICD-9-CM = The International Classification of Diseases, Ninth Revision, Clinical Modification, ID = intellectual disability, IL = interleukin, Editor: Angelo Valerio Marzano.
J-ML and R-JH contributed equally to the article.
Institutional review board statement and data sharing statement: This study was approved by the Institutional Review Board of the Tri-Service General Hospital, Taipei, Taiwan (approval number: TSGHIRB NO. B-105-06). Written consent from study patients was not obtained because all information potentially identifying any individual patient was encrypted. The data regulations of the patients’ confidentiality were guaranteed by the Bureau of National Health Insurance and Institutional Review Board of Tri-Service General Hospital. The raw data is encrypted and release or share is prohibited.
Biostatistics statement: The statistical methods and results were reviewed by C-LY, Institute of Bioinformatics and System Biology, National Chiao Tung University, Hsinchu, Taiwan.
Language certificate: Our manuscript has been edited for English language, grammar, punctuation, and spelling by Enago, the editing brand of Crimson Interactive Pvt, Ltd.
Foundation: None declared.
Funding/support: The work was supported by grants from the Ministry of Health and Welfare (10510) and Taoyuan General Hospital, Ministry of Health and Welfare (10533), Taoyuan General Hospital, Ministry of Health and Welfare (PYT10601), the Ministry of Science and Technology Taiwan (MOST 104-2320-B-016-012-MY3) in the analysis and interpretation of data. The current implications and conclusions do not represent the opinions of the Bureau of National Health Insurance, the Department of Health, or the National Health Research Institute.
The authors have no conflicts of interest to disclose.
a
Division of Urology, Department of Surgery, Taoyuan General Hospital, Ministry of Health and Welfare, Taoyuan,b
Department of Medicine, National Yang-Ming University,c
Graduate Institute of Life Sciences,d
Biobank Management Center of the Tri-Service General Hospital,e
Department of Pathology and Graduate Institute of Pathology and Parasitology,fDepartment of Obstetrics & Gynecology, Tri-Service General Hospital, National Defense Medical Center,gInstitute of Bioinformatics and System Biology, National Chiao Tung University, Hsinchu,h
School of Chinese Medicine, College of Chinese Medicine, China Medical University,i
Department of Nursing, College of Medical and Health Science, Asia University,jDepartment of Pediatrics, BinKun Women’s and Children’s Hospital, Taoyuan,kDepartment of Pediatrics, MacKay Children’s Hospital, Taipei,l
Department of Medicine, MacKay Medical College, New Taipei City,m
Department of Pediatrics and Infectious Disease, Hsinchu MacKay Memorial Hospital, Hsinchu, Taiwan,n
Division of Infection and Pathway Medicine, College of Medicine and Veterinary Medicine, the University of Edinburgh, Edinburgh, United Kingdom.
∗
Correspondence: Chien-Yu Lin, Department of Pediatrics and Infectious Disease, Hsinchu MacKay Memorial Hospital, No. 690, Sec. 2, Guangfu Road, Hsinchu 300, Taiwan (e-mail: [email protected])
Copyright© 2017 the Author(s). Published by Wolters Kluwer Health, Inc.
This is an open access article distributed under the terms of the Creative Commons Attribution-Non Commercial-No Derivatives License 4.0 (CCBY-NC-ND), where it is permissible to download and share the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal.
Medicine (2017) 96:23(e7108)
Received: 11 December 2016 / Received infinal form: 12 May 2017 / Accepted: 16 May 2017 http://dx.doi.org/10.1097/MD.0000000000007108
Observational Study
Medicine
LHID2000 = Longitudinal Health Insurance Database 2000, NHIRD = National Health Insurance Research Database, OCD =
obsessive-compulsive disorder, PDC= psychiatric disorders in childhood.
Keywords:childhood psychiatric disorder, children, intellectual disability, mental disorder, mental health, National Health Insurance Research Database, scabies
1. Introduction
Scabies is a common and distressing disease caused by the mite
Sarcoptes scabiei var. hominis.[1] The disease burden is
substantial and affects between 0.2% and 71.4% of the general
population depending on the region.[1–3] Scabies is most
prevalent during early childhood with a peak age between 5
and 9 years old.[3]The skin lesions are intensely pruritic, and a
scabies infection can profoundly impair the individual’s quality of life. The pruritus is more severe at night, and thus, sleep disturbance and inattention are common in children with scabies.
In addition, an infestation ofS. scabiei var. hominis will induce
immune-mediated inflammatory reactions, and some systemic
diseases have been associated with scabies.[4–6] However, the
precise mechanism and long-term consequences of a scabies infection remain largely unclear.
At least 1 in 10 children have a psychiatric disorder.[7,8]
However, psychiatric disorders in childhood (PDC) are difficult
to diagnose and are underestimated worldwide.[8] Various
diseases, including neurologic and developmental diseases, may present as psychiatry disorders, the manifestations of which
may initially be occult.[9]In addition, the environmental, family
education status, and socioeconomic factors have a huge impact on the clinical manifestation of the affected individual. Moreover, inattention, sleep disturbance, and somatic complaints are
common in children.[10,11]Although advances in the
understand-ing of psychiatric disorders (e.g., the roles of neurotransmitters and cytokines in the pathophysiology of psychiatric disorders) have been made, the diagnosis of PDC remains a challenge for
both pediatricians and psychiatrists.[12]
There are several similarities for both diseases and an association between these 2 diseases may exist. For example, both diseases may
present as pruritus, inattention, and sleep disturbances.[1,13]
Pruritus is one of the most common somatic symptoms and can lead to the diagnosis of several psychiatric disorders. In addition, both scabies and PDC are prevalent in patients with a lower
socioeconomic status.[14–16]Third, immune-mediated in
flamma-tion plays a role in the underlying pathophysiology.[5,12] The
association between scabies and PDC has not been previously reported in the literature. Therefore, we hypothesized that there was an association between an infection with scabies and PDC.
Specifically, an infection with scabies during childhood may
increase the subsequent risk of psychiatric disorders in adolescents. We conducted the nationwide population-based cohort study to investigate the relationship between scabies and PDC.
2. Materials and methods 2.1. Database
This large-scale study utilized data from the National Health Insurance Research Database (NHIRD) of Taiwan, which was a unique public health and medical insurance system. The National Health Insurance program was launched in 1995 and covered 99.9% of the 23 million residents of Taiwan by the end of
2013.[17] The NHIRD includes all data for persons seeking
medical aid, including demographic data, medical records, and medical procedures. We used the Longitudinal Health Insurance Database 2000 (LHID2000), which consists of a sub-dataset of the NHIRD-comprised data from 1 million people randomly selected from the larger NHIRD in 2000 and representative of the
nationwide population.[18]
2.2. Study subjects
The study subjects were chosen from LHID2000 and the study period was between January 2000 and December 2013. This
study was divided into 2 stages: first, recruiting patients with
newly diagnosed scabies and matched controls, and second, the follow-up of newly developed PDC. The diagnoses of the patients
were sorted according to The International Classification of
Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)
system.[19]The patients newly diagnosed with scabies
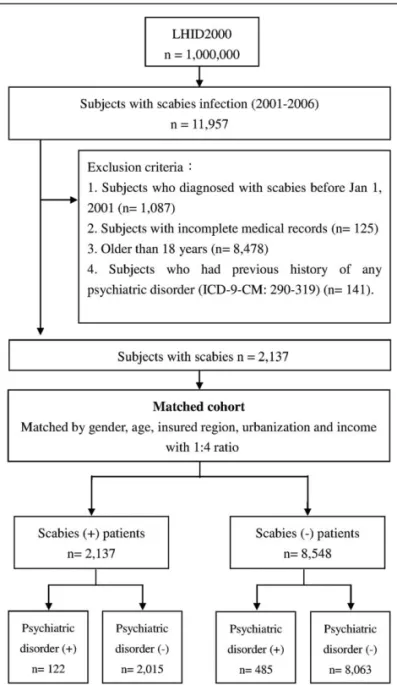
(ICD-9-CM: 133.0) by licensed doctors between 2001 and 2006 were enrolled in this study (Fig. 1). The exclusion criteria consisted of patients who were diagnosed with scabies before January 1, 2001
(n=1087); patients with missing medical records (n=125);
patients older than 18 years (n=8478); and patients with history
of scabies or any PDC (n=141). Finally, a total of 2137 patients
with a scabies infection were enrolled as the scabies groups. Patients without scabies were enrolled by randomly matching patients by gender, age, insured region, and urbanization to the scabies group at a ratio of 1:4 as the control group. Specifically,
the nonscabies control group patients were matched by age (0–2,
3–5, 6–12, and 13–18 years), gender, and index year of the scabies diagnoses of the patients in the scabies group. A total of 8548 subjects were enrolled in the nonscabies control group. Subjects who had a previous psychiatric history (ICD-9-CM:
290–319) were excluded from both the study and control groups.
A total of 10,685 subjects were enrolled in the study, including 2137 study subjects in the scabies group and 8548 study subjects in the nonscabies control group. We tracked each subject over a 7-year period starting with their index date to determine which subjects were diagnosed with PDC, based on the Diagnostic and
Statistical Manual of Mental Disorders, Fifth Edition,[20]which
included attention deficit hyperactivity disorder (ADHD)
(ICD-9-CM:314), autism spectrum disorder (ICD-9-CM: 299), anxiety CM: 300 except 300.3, 300.4), schizophrenia (ICD-9-CM: 295), intellectual disability (ID) (ICD-9-(ICD-9-CM: 317–319), tic disorder (ICD-9-CM: 307.2), delayed development (ICD-9-CM: 315), obsessive–compulsive disorder (OCD) (ICD-9-CM: 300.3), conductive disorder (ICD-9-CM: 312), disturbance of emotions specific to childhood and adolescence (ICD-9-CM: 313), psychic factors associated with diseases (ICD-9-CM: 316), eating disorder (ICD-9-CM: 307.5), stuttering (ICD-9-CM: 307.0), communication disorder CM: 307.9), enuresis (ICD-9-CM: 307.6), encopresis (ICD-9-(ICD-9-CM: 307.7, 787.6), and separation anxiety disorder (ICD-9-CM: 309.21) during the
follow-up period. Disturbance of emotions specific to childhood
and adolescence (ICD-9-CM: 313) comprised the different types of emotional disturbances in childhood and adolescence:
overanxious, misery and unhappiness, shyness, introverted disorders, and so on. Mental disturbances or psychic factors which were thought to have played a major part in the etiology of
physical conditions were classified in psychic factors associated
with diseases (ICD-9-CM: 316), such as psychogenic asthma, dermatitis, and gastric ulcer. Enuresis (ICD-9-CM: 307.6) was considered as physiological disorder before the age of 3 years and encopresis (ICD-9-CM: 307.7, 787.6) was regarded as
physio-logical disorder before the age of 4 years.[20]
The outcomes of this study included the number of patients
newly diagnosed with any PDC in each group. We also identified
and analyzed all the other medical diagnoses and procedures of the patients during the follow-up period. The diagnoses of PDC were made by psychiatrists on the basis of at least 1 admission or at least 2 consistent diagnoses in outpatient departments due to the diseases mentioned above. In addition, PDC was diagnosed by the psychiatrists according to a detailed clinical interviews and based on their experimental judgment with the aim of achieving diagnostic validity.
This study was approved by the Institutional Review Board of the Tri-Service General Hospital (approval number: TSGHIRB
NO. B-105-06.). As this was a retrospective study and all data was anonymous, the Institutional Review Board committee agreed with the authors that it was not necessary to obtain patient consent.
2.3. Adjustment of covariates
The covariates of the comorbidities selected in this study consisted of asthma 9-CM: 493), atopic dermatitis (ICD-9-CM: 691), allergic rhinitis (ICD-(ICD-9-CM: 477), and preterm labor (ICD-9-CM: 765.0, 765.1). Age was categorized into 4 age groups: 0 to 2, 3 to 5, 6 to 12, and 13 to 18 years. Urbanization was classified into 4 groups. The geographic areas of residency in Taiwan were divided into 4 regions: the northern, central, southern, and other regions (i.e., eastern and outlying islands). 2.4. Statistical analysis
We used SPSS software version 19.0 (SPSS Inc., Chicago, IL) for our statistical analysis and SQL Server 2008 (Microsoft Cooperation, New Mexico) for data management. A chi-square test was used to analyze the descriptive data including the demographic characteristics, age, geography, level of urbaniza-tion, and comorbidities between the scabies and nonscabies control group. The Cox proportional hazards regression models were performed to estimate the effects of risk factors on the
hazard ratio with an accompanying 95% confidence interval
(CI). All models were adjusted for the covariates (i.e., gender, age, income, geography, urbanization, and comorbidities) to calculate
the independent risks of individual diseases. A 2-sidedP<.05
was set as the determinant of statistical significance. 3. Results
From January 2001 to December 2006, 2137 children with a
scabies infection were identified from the LHID2000 database.
Another 8548 matched uninfected children were assigned to the control group, and a total of 10,685 patients were enrolled in our study (Fig. 1). The demographic and medical characteristics of both groups are shown in Table 1. Boys and school-aged children had a higher risk of scabies infection, but the difference was not statistically significant. Most patients were residents of northern Taiwan and urbanized areas. Higher comorbid asthma and atopic dermatitis were observed in scabies group (asthma: scabies
vs control groups: 14.8% vs 13%, P<.05; atopic dermatitis:
scabies vs control groups: 14.6% vs 8.6%,P<.001).
All enrolled children were tracked for 7 years to evaluate the incidence of psychiatric disorders, the results of which are summarized in Table 2. A total of 607 (5.68%) children developed a psychiatric disorder in the subsequent 7-year follow-up period. The risk of developing any kind of PDC is not different between scabies and control groups. Patients with scabies had higher risk of developing ID (adjusted hazard ratio [aHR]: 2.04;
95% CI: 1.25–3.32). The prevalence of anxiety, schizophrenia,
tic disorder, developmental delay, OCD, conductive disorder, emotional disorder, enuresis, ADHD, and autism was not
significantly different between these 2 groups according to the
results of the Cox risk regression analysis.
4. Discussion
Based on the clinical similarities in the presenting symptoms, socioeconomic status, immunopathology, and age at onset, we
Figure 1. Flowchart of recruitment of subjects from the 1 million random sample of the National Health Insurance Research Database from 2000 to 2006 in Taiwan.
hypothesized that an infection with scabies during childhood may increase the subsequent risk of psychiatric disorders in adolescents. We found there was no obvious difference in the overall incidence of PDC, but children with scabies had a higher risk of developing ID (aHR: 2.04; 95% CI: 1.25–3.32).
ID, used to be called mental retardation, is a neurodevelop-mental disorder characterized by limitations in intelligence and adaptive skills since the childhood. ID is associated with several risk factors, such as lower level of maternal education, maternal age of delivery, male sex, and lower birth weight, but the full-spectrum of the underpinning pathophysiology remains largely unclear. Comorbidities with genetic and metabolic diseases are
common in patients with ID. Immune-mediated inflammatory
processes also contribute to the pathophysiology of ID. In patients with ID, higher level of interleukin (IL)-6 and IL-10 were
observed.[21–23] Genetic abnormalities of IL-1 receptor among
patients with X-linked ID were reported.[24–26] Cytokines are
responsible for signaling and can affect
hypothalamic–pituitary–-adrenal axis and the function of glia in the developing brain.[12]
Exposure to external infection can predispose or increase the susceptibility of an individual to future mental illness via the
actions of cytokines and subsequent inflammatory cascades.[12]
Physical diseases can interfere with mental illness and altered
cytokine profiles are noted in both psychiatric disorders and
scabies (Table 3). In patients with anxiety, elevated levels of tumor necrosis factor a, IL-6, and IL-17 have been
reported.[27–29]In particular, decreased levels of 2, 4,
IL-5, interferon-g have been found in patients with anxiety.[29]In
children with ADHD, higher serum levels of IL-6 and IL-10 have
been detected.[30–32]Patients with scabies also exhibit increased
levels of IL-6, IL-10, and IL-17.[33–37] Based on similar
pathophysiologic underpinnings, an interaction between scabies and psychiatric disorders may occur. The exact mechanism between the association of scabies of ID was unknown but
elevated IL-6 and IL-10 were observed in both scabies and ID. Furthermore, both scabies and ID are thought to be more common in patients with a lower socioeconomic status and in
crowed environment according to previous reports.[14,16] Our
study found an 104% increased risk of ID in patients with scabies. Further studies are warranted to elucidate the entire mechanism and casual relationship.
The relationship between scabies and ID may be bidirectional. They share several abovementioned similarities in clinical risk factors and cytokines alterations thus an interaction between
scabies and ID may exist. However, the definite mechanism
remains largely unclear. Patients with ID may have poor skills of
care and are prone to be infected with scabies.[38]Lower maternal
education level is a risk factor of ID and an unsatisfied hygiene may increase the risk of scabies. Moreover, patients ID may have a longer stay in medical institutions, and scabies is relatively
common in some institutions.[1]Although our study confirms an
increased risk of ID in patients with scabies, the entire mechanism is complex and further studies are warranted. We suggest a more comprehensive management in treating patients with scabies or ID. Early and comprehensive treatment of scabies and other risk factors may decrease the risk of subsequent ID. When we approach patients with ID, concurrent evaluation of scabies infection and other risk factors may contribute to successful management.
There was no statistical difference of risk for all kinds of PDC between scabies and control group in our study, and underdiag-nosis of PDC may contribute to the phenomenon. The diagunderdiag-nosis of PDC is underestimated worldwide. Although at least half of all psychiatric disorders develop before adulthood according to the
Table 2
The association between scabies and PDC analyzed by Cox regression. Psychiatric disorders Scabies (N, %) Controls (N, %) Crude HR (95% CI) Adjusted HR (95% CI)∗ All kinds of PDC 122 (5.7%) 485 (5.7%) 1 (0.82–1.22) Anxiety 53 (2.5%) 190 (2.2%) 1.12 (0.82–1.51) Schizophrenia 4 (0.2%) 21 (0.2%) 0.76 (0.26–2.22) Intellectual disability 27 (1.3%) 48 (0.6%) 2.26 (1.41–3.62)† 2.04 (1.25–3.32)† Tic disorder 3 (0.1%) 26 (0.3%) 0.46 (0.14–1.52) Delayed development 18 (0.8%) 88 (1.0%) 0.82 (0.49–1.36) OCD 6 (0.3%) 12 (0.1%) 2 (0.75–5.33) Conductive disorder 4 (0.2%) 13 (0.2%) 1.23 (0.4–3.77) Emotional disorder 9 (0.4%) 34 (0.4%) 1.06 (0.51–2.21) Enuresis 4 (0.2%) 36 (0.4%) 0.44 (0.16–1.25) ADHD 32 (1.5%) 162 (1.9%) 0.79 (0.54–1.15) ASD 2 (0.1%) 13 (0.2%) 0.62 (0.14–2.73)
ADHD= attention deficit/hyperactivity disorder, ASD = autism spectrum disorder, HR = hazard ratio, OCD= obsessive-compulsive disorder, PDC = psychiatric disorders in childhood.
∗
Each variable was adjusted for every other variable.
†P <.05 for comparison between patients with 2 groups.
Bold values means a statistically significance in adjust HR.
Table 1
Demographic data in both scabies and control groups. Scabies (N, %) Controls (N, %) Variables 2137 (100%) 8548 (100%) P Gender 1 Female 817 (38.2%) 3268 (38.2%) Male 1320 (61.8%) 5280 (61.8%) Age 1 0–2 101 (4.7%) 404 (4.7%) 3–5 316 (14.8%) 1264 (14.8%) 6–12 775 (36.3%) 3100 (36.3%) 13–18 945 (44.2%) 3780 (44.2%) Geography <.001∗ North 1018 (47.6%) 4275 (50.0%) Central 326 (15.3%) 1690 (19.8%) South 604 (28.3%) 2367 (27.7%) Other 189 (8.8%) 216 (2.5%) Urbanization <.001∗ 1 (highest) 703 (32.9%) 3670 (42.9%) 2 599 (28.0%) 2326 (27.2%) 3 481 (22.5%) 1812 (21.2%) 4 (lowest) 354 (16.6%) 740 (8.7%) Comorbidity Asthma 317 (14.8%) 1108 (13.0%) <.05∗ Atopic dermatitis 311 (14.6%) 735 (8.6%) <.001∗ Allergic rhinitis 872 (40.8%) 3478 (40.7%) .922 Preterm 2 (0.1%) 7 (0.1%) .868 ∗ P<.05.
World Health Organization’s World Mental Health Survey Initiative, the reported prevalence varies according to the specific
region of study.[8,39,40]The clinical manifestations of PDC may
be vague and present as many physical illnesses. Variables including, family, school, socio-environmental, cultural factors, and study methodology will affect the occurrence and incidence of reported psychiatric disorders. Thus, the reported prevalence of PDC differs according to each area and study, some of which are summarized in Table 4. In Mexico, 37.9% of adolescents experienced some form of psychiatric disorder and 28.4% sought
medical services during the 8-year follow-up period.[39] The
overall prevalence of PDC was 19.9% and 29.7% in high-risk
groups in Brazil.[41]Among British children aged from 5 to 15
years old, 10% were estimated to have psychiatric disorders
during late 20th century.[7]In a recent meta-analysis investigating
the worldwide prevalence of mental disorders in children and adolescents, the global pooled prevalence of childhood
psychiat-ric disorders was 13.4%.[8] The variation of the reported
prevalence in different countries is significant.[8,39,41–43]
There-fore, it remains a challenge for pediatricians and psychiatrists to make a diagnosis in children. The incidence of all types of psychiatric disorders during the 7-year follow-up period in the present study was 5.68%. Compared with the 8-year incidence reported by Benjet et al in Mexico, they are quite different (37.9% vs 5.68%, 8-year incidence vs 7-year incidence). Anxiety
disorders and ADHD are the most common psychiatric disorders,
which is consistent with the results of most previous studies.[8,10]
Very few patients were diagnosed with tic disorders, OCD, conduction disorders, and emotional disorders; however, we believe that these incidences are underestimated.
The stigmatization of psychiatric disorders may decrease the
drive for patients and parents to seek medical assistance.[45,46]
This phenomenon is more evident in traditional conservative Chinese society as patients with psychiatric disorders will be labeled and rejected by their peers. Therefore, individuals who are suspected to have such diseases are more reluctant to seek medical assistance in Taiwan. In addition, doctors are more cautious when making such diagnoses for it may cause negative
effects on the patient’s personal medical insurance. Therefore, all
of these factors result in the underestimation of childhood psychiatric disorders.
4.1. Limitations
Our study is subject to several limitations. First, the diagnosis of NHIRD was categorized according to the ICD-9-CM code. The severity of scabies and psychiatric disorders may affect the risk and is not to be differentiated in the coding system. In addition, children with mild psychiatric disorders may not be recorded, and thus, the diagnosis is underestimated. Second, the onset of
Table 3
Comparison of cytokine alterations in patients with anxiety, ADHD, ID or scabies with healthy controls.
Reference IL1b IL1Ra IL2 IL4 IL5 IL6 IL8 IL10 IL17 TNF-a IFN-g hsCRP TGF-b Corti-sol Anxiety Vieira et al[29] ↓ ↓ ↓ ↓ ↑ ↑ ↓ – O’Donovan et al[28] ↑ – ↓ Glaus et al[27] – – – ADHD Segman et al[32] ↑ Oades[31] ↑ ↑ ↑ Donfrancesco et al[30] – – ↑ ↑ – – – ID Lehtimaki et al[22] ↑ Marek et al[23] ↑ Aureli et al[21] ↑ ↑ Scabies Mullins et al[36] ↑ ↓
Walton and Oprescu[37] ↑ ↑ ↑
Liu et al[34] ↑
Mounsey et al[35] ↑
Abd El-Aal et al[33] ↑
ADHD= attention deficit/hyperactivity disorder, hsCRP = high-sensitivity C-reactive protein, ID = intellectual disability, IFN-g = interferon-g, IL = interleukin, IL1Ra = interleukin 1 receptor agonist, TGF-b = transforming growth factorb, TNF-a = tumor necrosis factor a, TNFR1 = tumor necrosis factor receptor 1. “↑”: significantly higher level than healthy controls. “ ”: trend of higher cytokine level than healthy controls.“–”: no significant difference compared with health controls. “ ”: trend of lower cytokine level than healthy controls.
Table 4
Reported prevalence of PDC in different areas.
Reference Region Study period Age groups, y/o Any disease, % Anxiety, % ADHD, %
Meltzer et al[7] UK 1999 5–15 10 4 Costello et al[42] USA 1993–2000 9–13 13.3 2.4 0.9 Gau et al[43] Taiwan 1994–1997 13–15 14.8–20.3 3.1–9.2 3.3–7.5 Yang et al[44] China 2008 6–17 9.49 6.06 0.84 Salum et al[41] Brazil 7–14 26 3.7 10.9 Polanczyk et al[8] Meta-analysis 1985 –2006 4–18 13.4 6.5 3.4 Benjet et al[39] Mexico 2005 –2013 12–17 37.9 7 0
various psychiatric disorders is variable. For example, anxiety occurs earlier in life, and mood disorders emerge during late
adulthood.[8,13,39] Although a 7-year follow-up period is not
short, some prevalent psychiatric disorders do not reach the peak age of onset during this period. Furthermore, the NHIRD is representative of the general population with a broad coverage, but the detailed history and laboratory tests are
undistinguish-able. Therefore, it is difficult to reach a definite conclusion
regarding the casual pathophysiology between scabies and childhood psychiatric disorders. We found an increased risk of ID in patients with scabies but it’s impossible to validate the relationship and investigate the pathologic mechanism between these 2 diseases. However, we provided a possible clue and starting point for further studies. Further studies are warranted to elucidate the entire mechanism and casual relationship. More-over, some risk factors may contribute to the subsequent development of psychiatric disorders, such as childhood
adversity or maltreatment.[41,47]This information is not available
due to the limitations of the NHIRD. 5. Conclusion
In conclusion, physical illnesses could interact with psychiatric disorders. This nationwide population-based cohort study provides evidence indicating a possible relationship between scabies and psychiatric disorders during childhood. Although lack of association of scabies and all kinds of PDC was observed, a 104% increased risk of ID was found in children with scabies (aHR: 2.04). We suggest a more comprehensive management in treating patients with scabies or ID. Early and comprehensive treatment of scabies and other risk factors may decrease the risk of subsequent ID. When we approach patients with ID, concurrent evaluation of scabies and other risk factors may contribute to successful management.
References
[1] Chosidow O. Scabies. N Engl J Med 2006;354:1718–27.
[2] Romani L, Steer AC, Whitfeld MJ, et al. Prevalence of scabies and impetigo worldwide: a systematic review. Lancet Infect Dis 2015;15:960–7.
[3] Romani L, Koroivueta J, Steer AC, et al. Scabies and impetigo prevalence and risk factors in Fiji: a national survey. PLoS Negl Trop Dis 2015;9: e0003452.
[4] Chung SD, Wang KH, Huang CC, et al. Scabies increased the risk of chronic kidney disease: a 5-year follow-up study. J Eur Acad Dermatol Venereol 2014;28:286–92.
[5] Chen JY, Liu JM, Chang FW, et al. Scabies increased the risk and severity of COPD: a nationwide population-based study. Int J Chron Obstruct Pulmon Dis 2016;11:2171–8.
[6] Liu JM, Chiu FH, Lin CY, et al. Incidence of autoimmune diseases in patients with scabies: a nationwide population-based study in Taiwan. Rheumotol Int 2017;[Epub ahead of print].
[7] Meltzer H, Gatward R, Goodman R, et al. Mental health of children and adolescents in Great Britain. Int Rev Psychiatry 2003;15:185–7. [8] Polanczyk GV, Salum GA, Sugaya LS, et al. Annual research review: a
meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry 2015;56:345–65. [9] Erskine HE, Baxter AJ, Patton G, et al. The global coverage of prevalence
data for mental disorders in children and adolescents. Epidemiol Psychiatr Sci 2016;1–8. [Epub ahead of print].
[10] Baxter AJ, Scott KM, Vos T, et al. Global prevalence of anxiety disorders: a systematic review and meta-regression. Psychol Med 2013;43:897–910. [11] Bron TI, Bijlenga D, Verduijn J, et al. Prevalence of ADHD symptoms
across clinical stages of major depressive disorder. J Affect Disord 2016;197:29–35.
[12] Ratnayake U, Quinn T, Walker DW, et al. Cytokines and the neurodevelopmental basis of mental illness. Front Neurosci 2013;7:180. [13] Craske MG, Stein MB. Anxiety. Lancet 2016;388:3048–59.
[14] Bowen AC, Mahe A, Hay RJ, et al. The global epidemiology of impetigo: a systematic review of the population prevalence of impetigo and pyoderma. PLoS One 2015;10:e0136789.
[15] Heukelbach J, Feldmeier H. Scabies. Lancet 2006;367:1767–74. [16] Rutter M. Poverty and child mental health: natural experiments and
social causation. JAMA 2003;290:2063–4.
[17] Chang FW, Lee WY, Liu YP, et al. The relationship between economic conditions and postpartum depression in Taiwan: a nationwide population-based study. J Affect Disord 2016;204:174–9.
[18] National Health Insurance Institutes: National Health Insurance Research Database. 2016. http://nhird.nhri.org.tw/en/Data_Subsets. html# [Accessed on October 10, 2016].
[19] American Hospital Association; American Medical Record Association; Health Care Financing Administration; National Center for Health StatisticsICD-9-CM coding and reporting official guidelines. J Am Med Rec Assoc 1990;61(suppl):1–7.
[20] American Psychiatric AssociationDiagnostic and statistical manual of mental disorders. 5th edAuthor, Washington, DC:2013.
[21] Aureli A, Sebastiani P, Del Beato T, et al. Involvement of IL-6 and IL-1 receptor antagonist on intellectual disability. Immunol Lett 2014;162:124–31. [22] Lehtimaki KA, Liimatainen S, Peltola J, et al. The serum level of
interleukin-6 in patients with intellectual disability and refractory epilepsy. Epilepsy Res 2011;95:184–7.
[23] Marek D, Papin S, Ellefsen K, et al. Carriers of the fragile X mental retardation 1 (FMR1) premutation allele present with increased levels of cytokine IL-10. J Neuroinflammation 2012;9:238.
[24] Carrie A, Jun L, Bienvenu T, et al. A new member of the IL-1 receptor family highly expressed in hippocampus and involved in X-linked mental retardation. Nat Genet 1999;23:25–31.
[25] Jin H, Gardner RJ, Viswesvaraiah R, et al. Two novel members of the interleukin-1 receptor gene family, one deleted in Xp22.1-Xp21.3 mental retardation. Eur J Hum Genet 2000;8:87–94.
[26] Zhang YH, Huang BL, Niakan KK, et al. IL1RAPL1 is associated with mental retardation in patients with complex glycerol kinase deficiency who have deletions extending telomeric of DAX1. Hum Mutat 2004;24:273.
[27] Glaus J, Vandeleur CL, von Kanel R, et al. Associations between mood, anxiety or substance use disorders and inflammatory markers after adjustment for multiple covariates in a population-based study. J Psychiatr Res 2014;58:36–45.
[28] O’Donovan A, Hughes BM, Slavich GM, et al. Clinical anxiety, cortisol and interleukin-6: evidence for specificity in emotion-biology relation-ships. Brain Behav Immun 2010;24:1074–7.
[29] Vieira MMM, Ferreira TB, Pacheco PAF, et al. Enhanced Th17 phenotype in individuals with generalized anxiety disorder. J Neuro-immunol 2010;229:212–8.
[30] Donfrancesco R, Nativio P, Di Benedetto A, et al. Anti-Yo antibodies in children with ADHD:first results about serum cytokines. J Atten Disord 2016;[Epub ahead of print].
[31] Oades RD. An exploration of the associations of pregnancy and perinatal features with cytokines and tryptophan/kynurenine metabolism in children with attention-deficit hyperactivity disorder (ADHD). Atten Defic Hyperact Disord 2011;3:301–18.
[32] Segman RH, Meltzer A, Gross-Tsur V, et al. Preferential transmission of interleukin-1 receptor antagonist alleles in attention deficit hyperactivity disorder. Mol Psychiatry 2002;7:72–4.
[33] Abd El-Aal AA, Hassan MA, Gawdat HI, et al. Immunomodulatory impression of anti and pro-inflammatory cytokines in relation to humoral immunity in human scabies. Int J Immunopathol Pharmacol 2016;29:188–94.
[34] Liu X, Walton SF, Murray HC, et al. Crusted scabies is associated with increased IL-17 secretion by skin T cells. Parasite Immunol 2014;36:594–604. [35] Mounsey KE, Murray HC, Bielefeldt-Ohmann H, et al. Prospective study in a porcine model ofSarcoptes scabiei indicates the association of Th2 and Th17 pathways with the clinical severity of scabies. PLoS Negl Trop Dis 2015;9:e0003498.
[36] Mullins JS, Arlian LG, Morgan MS. Extracts ofSarcoptes scabiei De Geer downmodulate secretion of IL-8 by skin keratinocytes and fibroblasts and of GM-CSF by fibroblasts in the presence of proinflammatory cytokines. J Med Entomol 2009;46:845–51. [37] Walton SF, Oprescu FI. Immunology of scabies and translational
outcomes: identifying the missing links. Curr Opin Infect Dis 2013;26:116–22.
[38] American Psychiatric Association. Intellectual disability (intellectual developmental disorder). Diagnostic and Statistical Manual of Mental Disorders 5th ed. American Psychiatric Association, Arlington, VA:2013;33.
[39] Benjet C, Borges G, Mendez E, et al. Eight-year incidence of psychiatric disorders and service use from adolescence to early adulthood: longitudinal follow-up of the Mexican Adolescent Mental Health Survey. Eur Child Adolesc Psychiatry 2016;25:163–73.
[40] Kessler RC, Angermeyer M, Anthony JC, et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry 2007;6:168–76.
[41] Salum GA, Gadelha A, Pan PM, et al. High risk cohort study for psychiatric disorders in childhood: rationale, design, methods and preliminary results. Int J Methods Psychiatr Res 2015;24:58–73. [42] Costello EJ, Mustillo S, Erkanli A, et al. Prevalence and development of
psychiatric disorders in childhood and adolescence. Arch Gen Psychiatry 2003;60:837–44.
[43] Gau SS, Chong MY, Chen TH, et al. A 3-year panel study of mental disorders among adolescents in Taiwan. Am J Psychiatry 2005;162: 1344–50.
[44] Yang X, Jiang C, Pan W, et al. Prevalence of psychiatric disorders among children and adolescents in northeast China. PLoS One 2014;9: e111223.
[45] Hinshaw SP. The stigmatization of mental illness in children and parents: developmental issues, family concerns, and research needs. J Child Psychol Psychiatry 2005;46:714–34.
[46] Corrigan PW, Watson AC. Understanding the impact of stigma on people with mental illness. World Psychiatry 2002;1:16–20.
[47] Bjorkenstam E, Burstrom B, Vinnerljung B, et al. Childhood adversity and psychiatric disorder in young adulthood: An analysis of 107,704 Swedes. J Psychiatr Res 2016;77:67–75.