中國醫藥大學機構典藏 China Medical University Repository, Taiwan:Item 310903500/41376
142
0
0
全文
(2)
(3) 中文摘要 聽力損傷是常見的感覺系統障礙之一,耳蝸缺血則是導致聽力損傷的重要因素。 因為耳蝸代謝旺盛,需要許多能量來維持正常功能;但其血液供應只來自迷路動脈, 易受到影響而造成缺血性病變。已知許多聽力疾患與耳蝸缺血有關,如老化、噪音 性聽損等。本論文在於建立一個可逆式耳蝸缺血動物模式,並配合開發耳蝸缺血的 體外模式以完整地探討耳蝸缺血時內耳細胞變化,有助於了解耳蝸缺血相關聽力病 變之可能機轉,藉此平臺探尋耳蝸缺血與常見耳毒性的交互作用,並進而探尋對缺 血性耳蝸病變可能有效的治療方式。 首先完成對天竺鼠迷路動脈解剖構造的探索,並建立耳蝸可逆性缺血的動物模式 (第二章),以及確認天竺鼠迷路動脈暫時性缺血時間與劑量的反應(第三章)。在瞭解 動物耳蝸缺氧的組織形態變化後,進而探討動物耳蝸在高壓純氧下的變化(第四 章),以作為未來進一步研究的基礎。在與耳毒性與生物能量的交互作用研究上,首 先建立一個動物耳蝸粒線體功能障礙的動物模式,在此模式下顯示耳蝸對醣胺類抗 生素的耳毒性會增加(第五章);最後經由上述建立的動物耳蝸缺血模式,顯示暫時 性耳蝸缺血也會明顯增加對醣胺類抗生素的耳毒性,接下來利用HEI-OC1耳蝸細胞 株進一步探討缺血與醣胺類抗生素時耳蝸細胞死亡的分子機制(第六章)。最後總結 本系列缺血性耳蝸病變的研究,並檢討如何應用本模式下探尋可能有助於治療這類 疾病的方式,以作為未來臨床應用的基礎(第七章)。. 關鍵詞:耳蝸缺血、動物模式、體外模式、耳毒性、治療策略. i.
(4) Abstract The cochlea is a highly metabolic organ and requires much energy to maintain the normal physiologic function. However, it is an end-artery organ and mainly supplied by the labyrinthine artery, which is a branch of anterior inferior cerebellar artery (AICA). Therefore, the cochlea is sensitive to disturbance of blood flow. Cochlear ischemia has been implicated to be the causative factor in various hearing disorders such as noise induced hearing loss, presbyacusis, or sudden deafness. The first aim of this thesis is to establish an animal model of reversible cochlear ischemia after the detailed exploration of the inner ear circulation. The interaction of aminoglycoside ototoxicity and bioenergetic deficiency of cochlea is then explored. In addition, the in vivo model in coordination with in vitro cochlear ischemia model will provide a new approach to the investigation of the cellular and molecular mechanisms in cochlear ischemia. In this thesis, the detailed exploration of the inner ear circulation in guinea pigs was completed, followed by the establishment of a reversible cochlear ischemia model in guinea pigs (chapter 2). The time courses and dose responses of cochlear ischemia in guinea pigs were shown in chapter 3. The effects of hyperbaric oxygen on guinea pig cochlea were investigated and demonstrated in chapter 4, which could provide the basis for future researches in therapeutic applications. This thesis also established an animal model of acute cochlear mitochondrial dysfunction to elucidate the interaction of aminoglycoside ototoxicity with bioenergetic deficiency (chapter 5). Increased aminoglycoside ototoxic susceptibility was depicted in the impaired bioenergetic deficiency of acute cochlear mitochondrial dysfunction and ischemia-reperfusion injuries. The molecular mechanisms after the interaction of aminoglycoside and hypoxia/ischemia was investigated via the in vitro model using HEI-OC1 cochlear cell line and described in chapter 6. Finally, previous researches on the therapeutic purposes for cochlear ischemic damage were reviewed in chapter 7. The potential therapeutic opportunities for the ischemia-related hearing losses were raised. By virtue of the in vitro and in vivo model, some evidence-based therapeutic strategies may be identified, which may be useful in clinical applications. Keywords: cochlear ischemia, animal model, in vitro model, ototoxicity, therapeutic strategy. ii.
(5) 致謝 回首五年前正要由而立跨入不惑之際帶著期待與興奮的心情進入臨醫所,繼續追 求對科學的不惑;時間匆匆飛逝,在電腦鍵盤上終於要敲下致謝的同時,臨醫所博 士班的學業即將劃下一個句點。這幾年來,在工作、生活和學業的多重交會下,構 成一個令人難忘的焠煉修行的經驗。從對於基礎研究朦朦朧朧的憧憬,研究計畫的 請教與研擬,進行實驗時的挫折與寂寞,獲得結果的喜悅與滿足,到最後論文的修 飾與漫漫等待,這一連串的過程中,感謝許多貴人的相助,才能達到最後的目標。 就如巴西著名作家鮑羅科爾賀(Paulo Coelho)在他的名著『牧羊少年的奇幻之旅』曾 藉著引領猶太人祖先亞伯拉罕的撒冷王麥基洗德一再地描述一個”Maktub”的天命觀 念:「每個人在他們年輕的時候,都知道自己的天命,那時候每件事都清晰不昧, 每件事都有可能…這一股神秘力量會說服人們,讓人們相信…引導你去完成你的天 命。它能淬煉你的精神、砥礪你的願力,因為這是這個星球最偉大的真理;不管你 是誰…只要你真心渴望一樣東西,就『放手去做』,因為渴望是源自天地之心; 那就是你來到這世間的任務」在這五年中這個”Maktub”的信念也不斷地催促著我去 完成屬於自己的”Maktub”。 最要感謝的是我的指導老師蔡銘修教授,從 12 年前來到中國附醫後,就從蔡老師 翩翩君子的身教與言教中,得到莫大的啟發;甚至蔡老師親自帶領我三次遠赴日本 拜山求藝,自古以來,常吟詠的是劉備三顧茅廬拜請軍師出山,卻少聽到三次帶著 晚輩拜門入山;終於讓我得以進入日本東北大學研修,接受一個完整日式內耳研究 的基本訓練,並進而作為我在臨醫所延續研究的基礎。也要感謝高銘欽教授與林清 淵教授,高老師與林老師淵博的學識、嚴謹的治學態度及敏銳的洞察力,在向這兩 位老師的請益中,對研究計畫精確中肯的批評,就如武林明師,一點就找出可能的 破綻,進而修正研究方向。更要感謝解剖學科蔡孟宏老師、魏一華老師及吳慶祥教 授在實驗技術上的指導與支持,林振文教授在蛋白質體學和生物資訊學上的啟發, 微生物學科賴志河老師對於實驗的全力幫忙、論文寫作的指導以及投稿經驗的分 享,能夠與這樣聰明、熱心與誠實的學者一起學習研究,實在是一個莫大的幸福。 最後要感謝麻醉部動物實驗空間的分享及黃久珍博士在動物實驗的指導,林慧娟小 姐在組織切片上的協助,以及摯友鄭元凱醫師這些年來的同行與鼓勵,更要感謝中 國附醫醫研部支持研究案(DMR96-121, DMR99-046)及中國醫大與臺大醫學院研究合 作案(CMU97-069,CMU98-NTU-13),除了經費的支援外,更是對於研究理念的認可、 贊同與鼓勵。 論文底定,心中如釋重負,在臨醫所的求學過程,此刻更覺歷歷在目,然而,最 令人難忘的是同學間的切磋勉勵,更因此締結成了生活上的好友。最後,感謝所有 家人的支持,由於他們的體諒與辛勞,吾人方能得以在此求學過程中無後顧之憂, 順利完成學業,謹此獻上我最高的敬意與感謝。. iii.
(6) Contents 中文摘要 ............................................................................................................................. i Abstract.............................................................................................................................. ii 致謝.................................................................................................................................... iii Contents ............................................................................................................................ iv Original papers................................................................................................................ vii Abbreviations ................................................................................................................. viii Chapter 1 Introduction......................................................................................................1 1.1 Background ...............................................................................................................1 1.1.1 Epidemiology of hearing loss……………………………..………………………1 1.1.2 Peculiar anatomy of cochlea……………………………..………………...…...1 1.1.3 Ischemia-related hearing loss…………………………………………………...2 1.2 Clinical revelance and specific aims .........................................................................2 Chapter 2 Animal models of selective cochlear ischemia ...............................................4 2.1 Animals......................................................................................................................4 2.2 Methods.....................................................................................................................4 2.2.1 Animal model of cochlear ischemia………………………………………….… 4 2.2.1.1 Previous animals models of cochlear ischemia ..............................................4 2.2.1.2 Anatomical exploration to labyrinthine artery via ventral approach..............5 2.2.1.3 Using microclamp to produce cochlear ischemia via ventral approach.........6 2.2.2 Verification of the effect of labyrinthine artery occlusion……………….……….6 2.2.2.1 Cochlear blood flow (CBF) monitoring with laser Doppler equipment ........6 2.2.2.2 Auditory testing ..............................................................................................7 2.2.2.3 Cardiac perfusion with trypan blue ................................................................7 2.3 Results .......................................................................................................................8 2.3.1 Cochlear blood flow during temporary occlusion of labyrinthine artery……..…8 2.3.2 Gait and hearing disturbance after disrupting labyrinthine artery…………........8 2.3.3 Effect of microclamps to occlude labyrinthine artery………………………..…8 2.4 Conclusion.................................................................................................................9 2.5 Figures.....................................................................................................................10 Chapter 3 Chronic cochlear changes after transient cochlear ischemia.....................19 3.1 Background .............................................................................................................19 3.2 Materials and methods ............................................................................................20 3.2.1 Surgical procedures…………………………………………………………….20 3.2.2 Hearing test………………………………………………………..………..…21 3.2.3 Surface preparation of the cochlea and the hair cell–counting procedure…….22 3.2.4 Histopathological examination…………………………………………………23 3.2.5 Experimental groups ..………………………………………............................23 3.2.6 Statistical analysis………………………………………………………………23 3.3 Results .....................................................................................................................24 3.3.1 Time/dose responses in ABR threshold shifts caused by cochlear ischemia….24 3.3.2 Hair cell loss……………………………………………………………………24 3.3.3 Histopathological analysis………………………………………………………25 3.4 Comments and conclusion ......................................................................................25 Conclusion……………………………………………………………………………29 . iv.
(7) 3.5 Figures.....................................................................................................................30 Chapter 4 Effect of hyperbaric oxygen on guinea pig’s cochlea..................................35 4.1 Background .............................................................................................................35 4.1.1 Therapeutic implications of cochlear ischemia…………………………………35 4.1.2 Role of hyperbaric oxygen therapy in inner ear diseases………...…....….…...37 4.2 Materials and Methods ............................................................................................38 4.2.1 Animals…………………………………………………………………………38 4.2.2 HBOT Model……………..……………………………………………………38 4.2.3 Otoscopic Evaluation…………………………………………………………..39 4.2.4 Auditory Test……………………………………………………………………40 4.2.5 Immunohistochemistry…………………………………………………………40 4.2.5.1 Preparation of Specimens. ............................................................................40 4.2.5.2 Immunohistochemistry. ................................................................................41 4.2.5.3 Semi-quantitative morphometric analysis. ...................................................41 4.2.5.4 Immunofluorescence labeling. .....................................................................42 4.2.5.5 In Situ Detection of Nuclear DNA Fragmentation .......................................42 4.2.6 Statistical Analysis ………………...…...…………....….……………….........43 4.3 Results .....................................................................................................................43 4.3.1 Animal behavior during HBOT and otoscopic findings after HBOT……....…43 4.3.2 ABR measurements before and after HBOT…………………………………..44 4.3.3 Immunohistochemical analysis of NOS in cochleae…………………………..44 4.3.4 TUNEL assay of cochleae after HBOT………………………………………..45 4.4 Comments and conclusion ......................................................................................45 Conclusion……………………………………………………………………………49 4.5 Figures.....................................................................................................................50 Chapter 5 Increased aminoglycoside ototoxicity in acute cochlear mitochondrial dysfunction—interaction of kanamycin to 3-nitropropionic acid ..........................57 5.1 Background .............................................................................................................57 5.2 Materials and Methods ............................................................................................59 5.2.1 Animals…………………………………………………………………………59 5.2.2 Animal treatment………………………………………………………………60 5.2.3 Auditory brainstem response (ABR) .................................................................60 5.2.4 Hair cell counting………………………………………………………………61 5.2.5 Statistical analysis………………………………………………………………61 5.3 Results .....................................................................................................................62 5.3.1 ABR measurements…………………………………………………………….62 5.3.2 Histological analysis..................................................................................…....62 5.4 Comments and conclusion ......................................................................................63 Conclusion……………………………………………………………………………67 5.5 Figures and table .....................................................................................................68 Chapter 6 Transient ischemia/hypoxia may enhance aminoglycoside ototoxicity.....73 6.1 Background .............................................................................................................74 6.2 Materials and methods ............................................................................................77 6.2.1 Animals, medications, reagents and antibodies………………………………..77 6.2.2 In vivo study……………………………………………………………………78 6.2.2.1 Surgical procedures ......................................................................................78 v.
(8) 6.2.2.2 Hearing test...................................................................................................79 6.2.2.3 Surface preparation of cochlea and hair cell counting. ................................80 6.2.2.4 Histopathological examination.....................................................................80 6.2.2.5 Grouping.......................................................................................................81 6.2.3 Tracking gentamicin uptake using fluorescence gentamicin……………………81 6.2.4 In situ detection of nuclear DNA fragmentation in vivo……………………..……82 6.2.5 In vitro study……………………………………………………………………83 6.2.5.1 Cell culture ...................................................................................................83 6.2.5.2 Hypoxia of cultured HEI-OC1 cells .............................................................83 6.2.5.3 MTT assay ....................................................................................................84 6.2.5.4 Quantification of apoptosis by flow cytometry ............................................84 6.2.5.5 Determination of the mitochondrial membrane potential ............................85 6.2.5.6 Measurements of ROS..................................................................................85 6.2.5.7 Detection of Ca2+ concentrations..................................................................86 6.2.5.8 Western blot analysis....................................................................................86 6.2.5.9 Determination of caspase activity ................................................................86 6.2.6 Statistics analysis………………………………………………………………87 6.3 Results .....................................................................................................................87 6.3.1 Transient ischemia increases the gentamicin-induced ABR threshold shifts….87 6.3.2 Increased hair cell loss after interaction of gentamicin and ischemia………….88 6.3.3 Histological analysis after combination of gentamicin and transient ischemia.88 6.3.4 Enhanced gentamicin uptake after transient cochlear ischemia……………….88 6.3.5 TUNEL stain in vivo….…………....................................................................................…89 6.3.6 Gentamicin-induced cell apoptosis in HEI-OC1 cells.......................................89 6.3.7 Gentamicin caused mitochondrial dysfunction in HEI-OC1 cells……………..90 6.3.8 Gentamicin caused ER stress, Ca2+ release and calpain activity……………….90 6.4 Comments and conclusion ......................................................................................91 Conclusion…………………………………………………………………..….……97 6.5 Figures.....................................................................................................................99 Chapter 7 Further clinical implications and conclusion ............................................113 References .......................................................................................................................116 Appendix.........................................................................................................................130 . vi.
(9) Original papers This dissertation is mostly based on the following papers, which will be properly referred in the subsequent chapters 2 to 7. 1. Lin CD, Oshima T, Oda K, Yamauchi D, Tsai MH, Kobayashi T*. Ototoxic interaction of kanamycin and 3-nitropropionic acid. Acta Oto-Laryngologica (SCI, 2009 IF:0.984) 2008; 128:1280-5 (In chapter 5). 2. Lin CD, Wei IH, Tsai MH, Kao MC, Lai CH, Hsu CJ, Oshima T, Tsai MH*. Changes in guinea pig cochlea after transient cochlear ischemia. NeuroReport (SCI, 2009 IF: 1.805) 2010; 21:968-75 (In chapters 2, 3). This paper was selected as the cover story for the print in NeuroReport 2010, Volume 21, Issue 15.. 3. Lin CD, Wei IH, Lai CH, Hsia TC, Kao MC, Tsai MH, Wu CH, Tsai MH*. Hyperbaric oxygen upregulates cochlear constitutive nitric oxide synthase. BMC Neuroscience (SCI, 2009 IF: 2.744) 2011; 12:21 e1-e10. (In chapter 4). This paper was selected as the image highlight as featured image for BMC Neuroscience homepage in February 2011.. 4. Lin CD, Kao MC, Tsai MH, Lai CH, Wei IH, Tsai MH, Tang CH, Lin CW, Hsu CJ, Lin CY*. Transient ischemia/hypoxia enhances gentamicin ototoxicity via caspase-dependent cell death pathway. Laboratory Investigation (SCI, 2009 IF: 4.602, ranking 7/71) 2011, accepted. (In chapter 6). vii.
(10) Abbreviations: 3-NP: 3-nitropropionic acid; ABR: auditory brainstem response; AG: aminoglycoside; AICA: anterior inferior cerebellar artery; ATA: atmosphere absolute, atm abs.; BBB: blood-brain barrier; BLB:. blood-labyrinthine barrier; CAP: common action potential;. CBF: cochlear blood flow; cNOS: constitutive form of NOS; CTM: Chinese traditional medicine; DAB: 3,3’-diaminobenzidine; dB: decibel; DFX: Desferrioxamine; DPOAE: distortion product of otoacoustic emission; EDTA: ethylenediamine tetra-acetic acid; EGCG: Epigallocatechin gallate; EGF: epidermal growth factor; eNOS: endothelial NOS; FHC: ferritin heavy chain; GDNF: glial-cell-derived neurotrophic factor; GM: gentamicin; HBO: hyperbaric oxygen; HBOT: hyperbaric oxygen therapy; HC: hair cell; HEI-OC1: House Ear Institute-organ of Corti 1; i.m.: intramuscular; i.p.: intraperitoneal; IGF: insulin-like growth factor; IHC: inner hair cell; iNOS: inducible form of NOS; IR: ischemia/reperfusion; KM: kanamycin; MMP: mitochondrial membrane potential; Mn-SOD:. mitochondrial. superoxide. dismutase;. MTT:. 3-(4,. 5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide; NBA: normobaric air; NGS: normal goat serum; NHS: normal horse serum; NMDA: N-methyl-D-aspartate; nNOS: neuronal NOS; NO: nitric oxide; NOS: nitric oxide synthase; OD: optical density; OC: organ of Corti; OHC: outer hair cell; PBS: phosphate-buffered saline; PFA: paraformaldehyde;. PI:. propidium. iodide;. POD:. post-operative. day;. PS:. phosphatidylserine; rhEPO: recombinant human erythropoietin; RNS: reactive nitrogen species; ROS: reactive oxygen species; RWM: round window membrane; RWN: round window niche; S.E.: standard error; SG: spiral ganglion; SGN: spiral ganglion neuron; SL: spiral ligament; SOD: sodium dismutase; SPL: sound pressure level; SSHL: sudden sensorineural hearing loss; SV: stria vascularis; TBS: Tris-buffered solution; TUNEL: terminal deoxynucleotidyl transferase (TdT)-mediated deoxyuridine triphosphate (dUTP)-biotin nick end labeling.. viii.
(11) Chapter 1 Introduction 1.1 Background 1.1.1 Epidemiology of hearing loss It is known that more than 70 million people suffer from severe hearing disturbances worldwide (Tekin et al., 2001). On the basis of this incidence, hearing loss can be regarded as one of the most frequent neurosensory diseases of the human being. Bilateral severe sensorineural hearing loss occurs in about every 752 births in Taiwan (Lin et al., 2002). The incidence of hearing loss increases significantly after 60 years of age. In the elderly, the progressive deterioration of auditory sensitivity associated with the aging process is known as “presbycusis”. Approximately 23% of the population between 65 and 75 years of age, and 40% of the population older than 75 years of age are affected by this condition (Seidman et al., 2004). It was estimated in 1993 that 7% of the population was 65 years or older and this number was 9.2% in 2003, 10.6% in 200 and is expected to be nearly 20% in 2030 (Department of Household Registration, 2010). Multiple factors contribute to the hearing loss, including genetic factors, degeneration, trauma, inflammation, vascular insufficiency. Hypoxia and ischemia has been postulated to be essential pathogenic factors in the clinicopathogenesis of hearing loss (Mazurek et al., 2008; Mazurek et al., 2006).. 1.1.2 Peculiar anatomy of cochlea Normal hearing relies on the integrity of cochlear function which is dependent upon the maintenance of a delicate homeostatic environment. The cochlea plays a key role in converting the mechanical sound energy into electrical potential and sensory inputs. It comprised essentially of two components, the organ of Corti and the stria vascularis. The organ of Corti is an organ of high metabolic activity. The processes of high-energy consumption are involved in the activation of ion pump in the stria vascularis to the maintenance of electrochemical gradient between perilymph and endolymph and tuning of the basilar membrane by the outer hair cells (Brass and Kemp, 1993). However, it is an 1.
(12) end-artery organ and mainly supplied by the labyrinthine artery, which is a branch of anterior inferior cerebellar artery (AICA) (Nakashima et al., 2003). Therefore, the cochlea is sensitive to disturbance of blood flow.. 1.1.3 Ischemia-related hearing loss Perturbations in the inner ear microcirculation have been considered to be one of the factors implicated in the pathophysiology of various kinds of sensorineural hearing loss (Nakashima et al., 2003). Clinical and experimental studies have shown that hearing disorders, including presbycusis (Riva et al., 2005; Riva et al., 2007), noise-induced hearing loss (Lamm and Arnold, 1996; Scheibe et al., 1990), sudden deafness (Yamasoba et al., 1993; Kim et al., 1999), endolymphatic drops (Larsen et al., 1988; Yazawa et al., 1998; Yamamoto et al., 1991) are related to alterations in the blood flow of inner ear.. 1.2 Clinical revelance and specific aims Giving the complexity of cell death pathway in cochlea (Jiang et al., 2006), an intervention in the early stages of ischemia may be a promising approach to the prevention of ischemia-related hearing loss in clinical setting. Therefore, we propose to investigate the role of oxidative stress and its time response in the inner ear following ischemia change both in vitro and in vivo. The in vitro method is feasible to study the molecular changes and the in vivo method is more relevant to clinical situation. The further clarification of the change of oxidative stress in cochlear ischemia will increase our understanding of the complexity of ischemia-related hearing loss and may offer additional possibilities to protect against hearing loss related to ischemia such as noise induced hearing loss, sudden deafness or presbycusis. Specific aims: 1. Establishment of an animal model of reversible cochlear ischemia, which is more relevant to clinical situations. Through this model, we can get more understanding to the complicated molecular mechanisms of cell death after cochlear ischemia, which may be applied to our understanding of other ischemia-associated hearing loss such as 2.
(13) presbycusis, noise induced hearing loss or sudden deafness. 2. Building-up an in vitro model of cochlear ischemia which is more feasible to cellular investigation. Such in vitro model could also provide an in vitro system for drug screening. 3. Investigation of the interaction of cochlear ischemia with common ototoxic agents such as aminoglycosides in order to elucidate the complicated interaction between ischemia and aminoglycoside, plus cytotoxic mechanisms they may induce within cochlea that potentiate ischemia or aminoglycoside ototoxicity into cytotoxic phenomenon. These results should aid the understanding of the interacting mechanism and potential preventive strategy against aminoglycoside ototoxicity. These results may provide us more implications for the treatments of other ischemia-associated hearing loss such as presbycusis, noise induced hearing loss or sudden deafness in human.. 3.
(14) Chapter 2 Animal models of selective cochlear ischemia 2.1 Animals Adult albino guinea pigs were used for this study. Guinea pigs have been proved to be a reliable animal model for hearing loss, in which a robust pathological response to aminoglycoside induced cochlear damage could be elicited. In addition, the historic role of guinea pigs in cochlear research is based on the easy surgical access to its cochlea, and well characterized cochlear anatomy and physiology (Forge and Schacht, 2000).. 2.2 Methods 2.2.1 Animal model of cochlear ischemia 2.2.1.1 Previous animals models of cochlear ischemia There have been several methods to produce cochlear ischemia in animals: (1) ventral approach via the auditory bulla cavity(Kimura and Perlman, 1958; Perlman et al., 1959); (2) skull base approach (Tabuchi et al., 1998; Kusakari et al., 1981); (3) vertebral artery occlusion (Hata et al., 1993; Fujita et al., 2007) and (4) occipital craniotomy approach (Mom et al., 1997; Short et al., 1985). These methods are able to induce complete and reversible anoxia without any additional microvascular damage. In addition to these mechanical methods, other methods, e.g. the photochemical AICA occlusion method (Asai et al., 1996) or the ferromagnetic thrombosis method (Schweinfurth and Cacace, 2000; Scheibe et al., 1997) have been also reported. To induce reversible local anoxia, however, the mechanical occlusion is superior to these methods in which large interindividual differences are seen in the degree of ischemia. The inner ear is principally supplied by the labyrinthine artery, which is a branch of anterior inferior cerebellar approach (AICA). The labyrinthine artery is the target artery to be occluded, rather than the AICA because there are many anastomoses among the cerebellar arteries and occlusion of AICA alone cannot ensure complete ischemia in the cochlea (Ren et al., 1995). 4.
(15) 2.2.1.2 Anatomical exploration to labyrinthine artery via ventral approach In this study, we plan to use the ventral approach to occlude the labyrinthine artery because the esophagus and trachea will not exposed in this method (which have to be exposed by the method of vertebral artery occlusion and skull base approach) and ventral approach also offers a easier way for long-term observation (which is difficult in the other approaches). The surgical approach to the labyrinthine artery of anterior inferior cerebellar artery was ventral through the tympanic bulla cavity (Kimura & Perlman, 1958; Perlman et al., 1959). The animal was in supine position after anesthesia was setup by intramuscular injection of mixtures of zoletil (30 mg/kg) and xylazine (10 mg/kg). This allows non-ventilator dependent oxygenation and a maintenance dose, 25% of the initial dose, was injected i.m. every 60 min to maintain constant blood levels. The animal was placed in a supine position with head holder apparatus. The cervical hair was shaved and skin was disinfected with 75% alcohol. A submental incision about 2-3 centimeters of skin incision was made medial to mandibular edge. The submandibular gland was separated to expose the digastric muscle and the paracondylar process. After the digastric muscle was separated from the fractured paracondylar process, the tympanic bulla was exposed. The anterior wall of tympanic bulla was opened by Rongeur to expose the cochlear turns. The drilling was then started on the petrous bone, medial to the basal turn and anterior to the intracranial opening of the cochlear aqueduct and the inferior petrosal sinus (Fig 2.1) (Kimura & Perlman, 1958). The dura and the inferior petrosal sinus were protected from damage by a piece of thin silastic sheeting. The drill was stopped at about 2mm anterior to internal auditory meatus. Through the drill hole, the labyrinthine branch of AICA was visible under the dura. The dura was excised and opened wide so that the labyrinthine branch of AICA was fully exposed for further research purpose. The serial figures are summarized in Fig. 2.2.. 5.
(16) 2.2.1.3 Using microclamp to produce cochlear ischemia via ventral approach In order to produce reversible cochlear ischemia, a microclamps (S&T Micro Clamps B-2, No. 00398-02) was used. According to the manufacturer’s manual, the B-2 microclamps is recommended for vessel diameter at around 0.5mm to 1.5mm at which the clamp pressure is at about 5 to 15g/mm2. The labyrinthine artery was further clamped by this microclamps. The morphology of labyrinthine artery was observed under microscopy. After releasing the microclamps, the labyrinthine artery was noted to reperfuse immediately after the release of the clamp (Fig. 2.3).. 2.2.2 Verification of the effect of labyrinthine artery occlusion 2.2.2.1 Cochlear blood flow (CBF) monitoring with laser Doppler equipment CBF was assessed from the velocity measurements of a Perimed PF 4001 laser Doppler equipment _HeNe, wave-length 632.8 nm, probe PF418rB500-0. The laser probe was applied to the second cochlear turns (Fig. 2.3). The CBF signal coming from the velocimeter system was continuously recorded before, during and after clamping using the series input of a PC computer. Two generical remarks about laser Doppler velocimetry must be kept in mind. First, this equipment only provides a relative evaluation of CBF in percentage of a reference flow. Second, the output of the laser Doppler velocimeter resulted from the combination of true CBF and spurious contributions from more superficial vessels in the bony wall of the cochlea or at its surface. These contributions were not expected to vary when the labyrinthine artery was clamped, so that 0% signal could never be reached even for a complete cochlear ischemia with 0% CBF. Nevertheless, the residual signal could be assessed at the end of the experiment after complete section of the eighth nerve bundle, including the arterial supply. The percentage of CBF corresponding to really complete ischemia was ascertained by this last measurement. Throughout flow measurements, a green Wratten filter was placed 6.
(17) on the microscope lighting in order to allow visual control without interference with the detection of red laser light.. 2.2.2.2 Auditory testing The hearing status of all animals is evaluated with tone burst ABR. The sound delivery tubes are inserted into the external ear canal during the ABR measurement. These tubes had custom adapters attached for curved insertion into the external ear canal. Different frequencies (1, 2, 4, 8 kHz) will be checked. For the ABR measurement, the guinea pigs are anesthetized with the mixture of xylazine and Zoletil intramuscularly injected before the steel needle electrodes are subdermally inserted in the ipsilateral and contralateral retro-auricular region as reference electrode and active electrode and in the neck as the ground electrode. The auditory stimuli are band-passed filtered (30-3000 Hz), amplified and averaged for 12.7 milliseconds after stimulus. An average of 512 responses is recorded and the visual detection threshold is determined by attenuating stimulus intensities by 20-dB increments from the maximal output level at each frequency until the waveform is lost, then raised by 10-dB increments until the waveform re-appeared, and then approached by 5-dB increments until the waveform is reestablished. At the threshold intensity, at least two sequences of recordings are made to verify the reproducibility of the ABR responses.. 2.2.2.3 Cardiac perfusion with trypan blue The animals were deeply anesthetized by the i.p. administration of an excessive dose of pentobarbital sodium (50 mg/kg). They were perfused intracardially with physiological saline containing 0.1% heparin followed by 0.3% trypan blue in 0.1M phosphate buffer (pH 7.4). The cochleae were removed and dissected to expose the organ of Corti and modiolus.. 7.
(18) 2.3 Results 2.3.1 Cochlear blood flow during temporary occlusion of labyrinthine artery Laser dopplerometry was used to verify the blood flow in the cochlea. The laser probe was applied to the cochlear turn and external compression of the labyrinthine artery was done by microspatula. The baseline of the cochlear blood flow was significantly decreased after the external compression of the labyrinthine artery. Return of the blood flow was demonstrated after the release of the compression. The cochlear blood flow was slightly higher than the baseline after the release the compression. Reperfusion was shown in Fig. 2.4. 2.3.2 Gait disturbance and elevated auditory threshold after disrupting labyrinthine artery Permanent occlusion of the labyrinthine artery was performed by the suction cauterization method. After the suction cauterization of the labyrinthine artery, the animals exhibited significant gait deviation and spontaneous nystagmus (Fig. 2.5). The ABR threshold also was significantly elevated (Fig. 2.6). The sham surgery itself will not cause ABR threshold shifts (Fig. 2.7).. 2.3.3 Effect of microclamps to occlude labyrinthine artery The labyrinthine artery was further clamped by this microclamps. After the microclamps was applied to the labyrinthine artery, the cochlear function was monitored with click ABR at 120dB sound pressure level (SPL) at least every 3 minutes. Compared with the pre-operative apparent ABR waveform, persistent loss of ABR waveform could be depicted as the microclamps was successfully occluded the labyrinthine branch of AICA (Fig. 2.8). The occlusion effect of the labyrinthine artery by this microclamps was verified by intracardiac perfusion of 3% trypan blue. The cochlea of the control ear was stained by trypan blue while the cochlea of the operated ear was not (Fig. 2.9). 8.
(19) 2.4 Conclusion The surgical approach to the labyrinthine artery in guinea pigs is feasible by way of ventral approach as described by Kimura et al (Kimura & Perlman, 1958). Through this approach, the animal model of precise cochlear infarct or ischemia could be made. In this study, the effect of labyrinthine artery occlusion was verified by ABR threshold shifts, gait disturbance and morphological changes. ABR threshold shifts happened immediately after the application of the microclamps and restored after the release of the microclamp. However, the sham surgery itself will not cause ABR threshold shifts. This provides the basis for further reversible model of cochlear ischemia. 9.
(20) 2.5 Figures. Figure 2.1 Diagrammatic sketch (A) of the surgical approach to left labyrinthine branch of anterior inferior cerebellar artery (AICA) modified from the Kimura et al (Kimura & Perlman, 1958). Red cross indicates the occlusion point by the microclamps. A 3x2mm fenestrum was made medial to the cochlear basal turn (B).. 10.
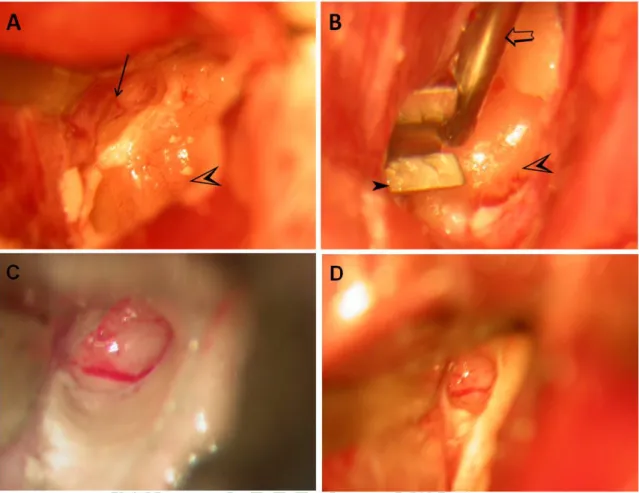
(21) Figure 2.2 Surgical procedures of the ventral approach to the exploration of labyrinthine artery. A. supine position for op; B. exposure of tympanic bulla; C. opening the tympanic bulla to exposure the cochlea; D. drilling medial to basal turn of cochlea to expose the labyrinthine artery (arrow).. 11.
(22) Figure 2.3 Application of laser probe for measurement of cochlear blood flow. A. Exposure of labyrinthine artery (arrow) and cochlear turns (empty arrowhead) via ventral approach. B. The microclamps (filled arrowhead) was applied to occlude the labyrinthine artery. The cochlear blood flow was monitored by laser Doppler with the probe (empty arrow) near the cochlear turn (empty arrowhead). Compared with the pre-clamped view (C), no significant morphologic change of labyrinthine artery was observed after the application of the microclamps (D).. 12.
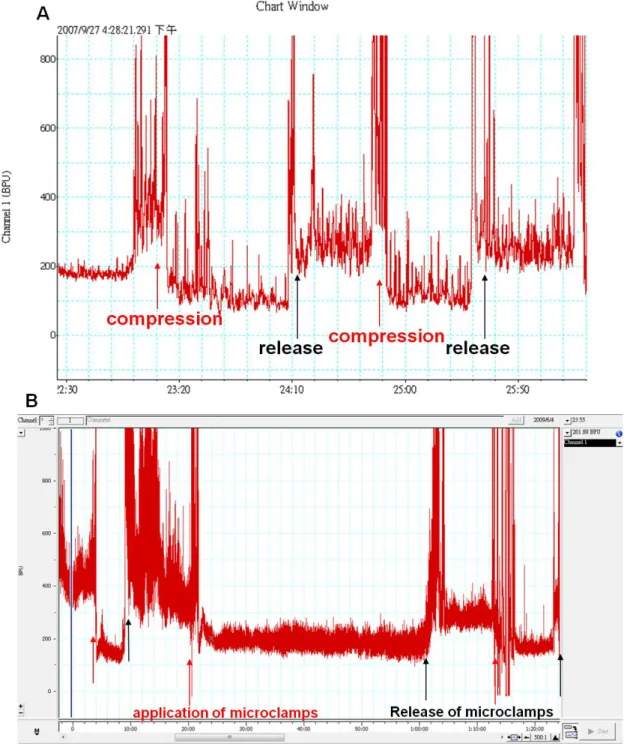
(23) Figure 2.4 Measurement of the cochlear blood flow by laser dopplerometry. A. Reduction of cochlear blood flow was recorded immediately after compression of the labyrinthine artery (red arrow); however, return of cochlear blood flow was depicted immediately after release of the external compression (black arrow). Hyperperfusion of the cochlea was observed immediately after the release. B. Persistence reduction of cochlear blood flow was observation in the 40-min microclamped period. Similar hyperperfusion of the cochlea was observed after the release of the microclamps.. 13.
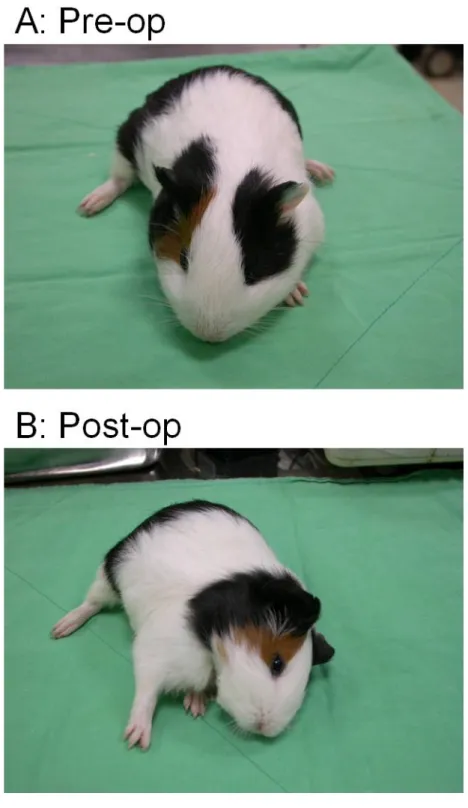
(24) Figure 2.5 Alterations of gait control before and after disruption of labyrinthine artery. A. Normal gait before op; B. Deviated gait to the left side was observed after cauterization of left labyrinthine artery.. 14.
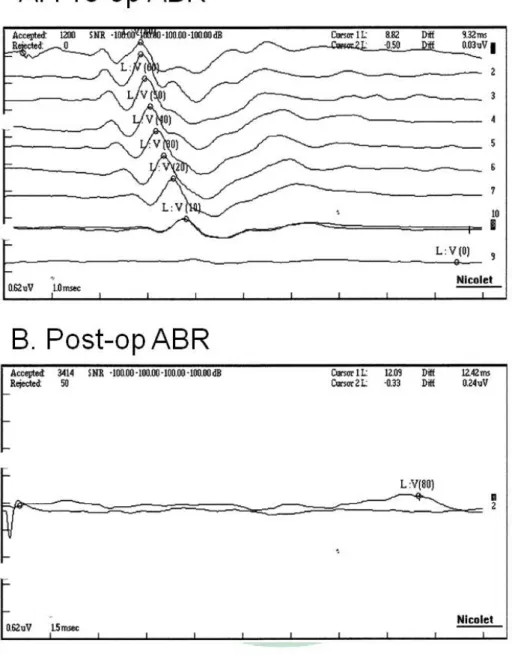
(25) Figure 2.6 ABR threshold changes before and after the disruption of labyrinthine artery. A. Normal ABR before op. B. ABR threshold > 80dB SPL after suction cauterization of labyrinthine artery. Stimulation sound: short tone burst at 8k Hz.. 15.
(26) Figure 2.7 Hearing level in sham surgery. Compared with the ABR waveform and auditory level before the surgery (A), no obvious auditory threshold shifts was noted 4 days after the surgery (B). Stimulation sound: short tone burst at 8 kHz.. 16.
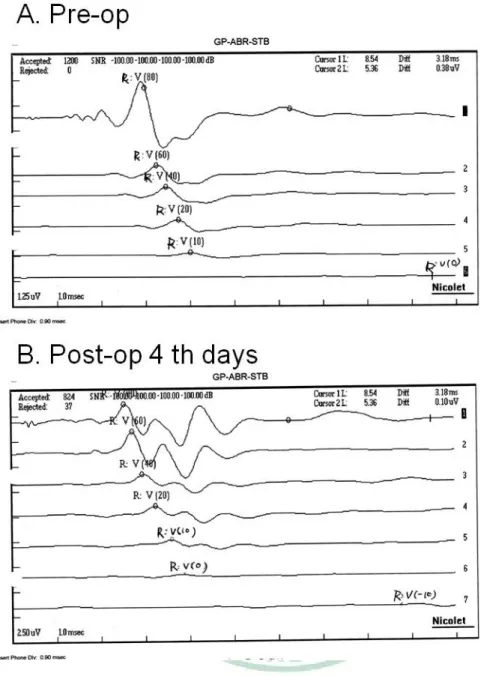
(27) Figure 2.8 Serial changes of ABR waveform during the clamping procedure. A. Before surgery, an apparent ABR waveform was recorded (top) (☆). After the microclamps was applied (←), the ABR waveform disappeared. b. The ABR waveform reappeared (★) when the microclamps was released (↔). The ABR waveform did, however, disappear again when the microclamps was reapplied (←). Stimulating sound: click at 80 dB HL, which is comparable to 120 dB SPL.. 17.
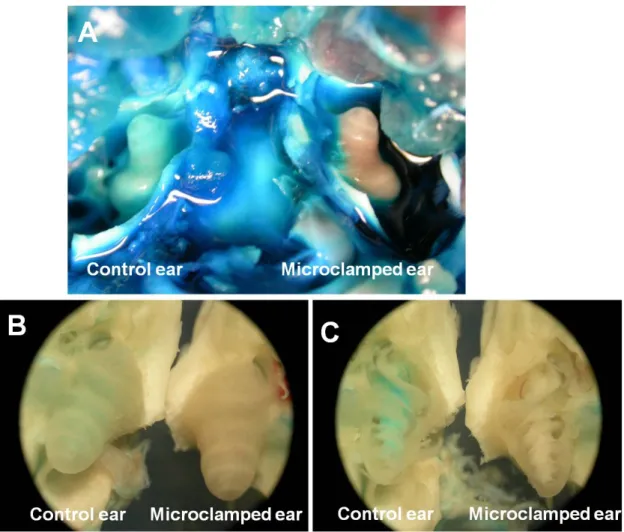
(28) Figure 2.9 Verification of the occlusion effect by the microclamps. After trypan blue perfusion, blue stain over the cochlear bony wall was noted in the control ear, but not in the microclamped ear (A, B). In the control ear, the cochlea was stained in the cochlear wall, modiolus and stria vascularis. However, in the clamped ear, the cochlear wall, modiolus and stria vascularis was free of trypan blue (C).. 18.
(29) Chapter 3 Chronic cochlear changes after transient cochlear ischemia ABSTRACT Perturbation of cochlear microcirculation is a major cause of hearing impairment. Previous studies examined the short-term (≤ 7 days) effect of cochlear ischemia. This study characterized the long-term (4 weeks) functional and morphological changes caused by transient ischemia that was induced in the adult guinea pig cochleae by clamping the labyrinthine artery for 0.25–3 h. Notably, treatments ≥ 1 h increased auditory brainstem response thresholds and caused loss of high-frequency hearing, basal-turn hair cells, and spiral ganglions. The time for functional recovery of the cochleae after ischemia may be up to 30 min. The extent of the functional and morphological changes depended on the ischemia period, and the changes progressed in intensity from the apical to the basal turn in an orderly fashion.. 3.1 Background The cochlea is a metabolically active organ that requires a substantial amount of energy to maintain its normal physiological function. Because it is an end-artery organ, mainly supplied by the labyrinthine artery (a branch of the anterior inferior cerebellar artery, AICA) (Nakashima et al., 2003), it is sensitive to blood flow disturbances. Disturbance of the cochlear microcirculation causes local hypoxia, which may result in common otologic disorders, such as noise-induced (Henderson et al., 2006), or sudden sensorineural hearing loss (SSHL) (Nagahara et al., 1983). Although there have been many attempts to characterize how ischemia causes cochlear damage, no definitive animal model to induce ischemia exists. Previous attempts to induce cochlear ischemia included occluding the bilateral vertebral arteries (Maetani et al., 2003) and compressing the neurovascular bundles in the internal auditory canals via either an skull base approach (Kusakari et al., 1981) or occipital approach (Tsuji et al., 2002). Post-operation observation periods were, however, relatively short (1 week at most 19.
(30) (Tsuji et al., 2002). Because the post-operative observation times of the experimental animals used in these studies were limited, a full evaluation of the effects of the ischemia treatments was not possible. Changes in hearing caused by common cochlear ischemia-induced disorders, e.g., SSHL, may evolve over a relatively long period of time after the initial acute insult. Early intervention may aid the recovery process in SSHL patients (Byl, Jr., 1984). Yet for SSHL patients, their hearing may continue to improve for 1 month after treatment cessation (Wilkins, Jr. et al., 1987). Therefore, a study incorporating a long observation period is needed to better understand the functional and morphological cochlear changes caused by ischemia, which is the purpose of this study.. 3.2 Materials and methods Adult albino guinea pigs between the ages of 2 and 4 months (body weight, 350–550 g) were used. The use and care of animals in this study were approved by the Institutional Animal Care and Use Committee of the China Medical University (permission number: 97-60-N). Animals were anesthetized by intramuscular injection of a mixture of Zoletil (30 mg/kg) and xylazine (10 mg/kg), which allowed for non–ventilator dependent oxygenation. A maintenance dose, 50% of the initial dose, was injected intramuscularly every 60 min thereafter. After sedation, atropine (0.05 mg/kg) and chloramphenicol (400 mg/kg) were given intramuscularly. For surgical accessibility and convenience, only the left ear was treated, but to avoid acoustical crossover from the cochlea of the right ear during auditory brainstem response (ABR) measurements, the latter was surgically destroyed.. 3.2.1 Surgical procedures After an animal had been anesthetized, the cervical hair was shaved. It was placed in the prone position, and 1% xylocaine was injected into the posterior auricular area of the right ear. The skin and subcutaneous myofascial plane of the ear were dissected to expose the mastoid bulla, which was then opened so that the cochlea could be directly destroyed by needle penetration and disruption. 20.
(31) The ventral-approach procedure to the labyrinthine artery has been described (Perlman et al., 1959). Electrodes were inserted subcutaneously into the left mastoid (anode), right mastoid (cathode), and the back (ground), and an earphone was inserted into the left ear canal to monitor the ABR perioperatively. The animal was then placed in the supine position. The skin over the ventral neck was disinfected with 75% alcohol and draped with aseptic dressings. A submental incision ~2–3 centimeters in length was made medially to the mandibular edge. The submandibular gland was separated to expose the digastric muscle and the paracondylar process. Separation of the digastric muscle from the fractured paracondylar process exposed the tympanic bulla. The anterior wall of the tympanic bulla was opened using a rongeur so that the basal cochlear turns were visible. Drilling started at the petrous bone, continued medially to the basal turn and anteriorly to the inferior petrosal sinus. The dura and the inferior petrosal sinus were protected during drilling by placing a thin Silastic sheet over them. A fenestration ~1.5 × 3.0 mm was made at the base of the skull, so that the labyrinthine artery was visible under the dura. The dura was excised, and the area opened so that the labyrinthine artery was fully exposed. The labyrinthine artery was closed with V1 microclamps] (#00396-01, S&T Microsurgical Instruments, USA), and cochlear function was thereafter monitored by click ABR at a 120-dB sound pressure level (SPL) at least every 3 min. Compared with the pre-operative apparent ABR waveform, persistent absence of the ABR waveform indicated that the microclamps had successfully occluded the labyrinthine artery (Fig. 2.8).. 3.2.2 Hearing test Tone burst ABR pre-operative and serial post-operative hearing tests were performed in a sound attenuated room. The pure tone bursts were generated with the amplitude specified by a real-time programmable attenuator (IHC Smart EP version 3.97, USA) with ER2 insert earphone, with stimulus frequency at 1, 2, 4, 8, 16 and 24 kHz (0.2ms rise/fall time and 1ms flat segment) with maximal output level 125, 123, 111, 117, 98 and 96dB SPL. The click/tone bursts were produced by IHS high frequency transducer in a 21.
(32) closed acoustic system through the sound delivery system. Responses for 1024 sweeps were averaged at each intensity level around the threshold in 5 dB SPL steps. Threshold was defined as the lowest intensity at which a clear waveform was visible upon inspection of an evoked trace. At least two sequences of recordings were made at the threshold intensity to verify the reproducibility of the ABR responses. Each ABR threshold was compared with the pre-operative threshold, which served as the baseline measurement. For the sham operation (sham-op) and the treatment groups (described below), serial ABR measurements were performed pre-operatively, immediately after the operation (PODi), 1 and 3 days after the operation (POD1d, 3d,) and 1, 2, 3, and 4 weeks after the operation (POD1w, 2w, 3w, 4w).. 3.2.3 Surface preparation of the cochlea and the hair cell–counting procedure At the end of the study, the animals were deeply anesthetized and then sacrificed by decapitation. The left cochleae were fixed with 4% paraformaldehyde in 0.1 M phosphate-buffered saline (PBS) by perilymphatic perfusion and then immersed in 4% paraformaldehyde in 0.1 M PBS for 1 day. The bony modiolus with the organ of Corti was carefully detached at the base of the cochlea following removal of the bony capsule, lateral wall, and tectorial membrane. After permeabilization with 0.3% Triton X-100 in PBS for 10 min, the tissues were incubated at room temperature with rhodamine-coupled phalloidin (Molecular Probes, Eugene, OR, USA) diluted 1:200 with PBS for 30 min. After the tissues were rinsed with PBS, strips of the organ of Corti were divided into the four turns, which were mounted on glass slides and examined with a fluorescence microscope (Model Leitz DM RBE; Leica, Wetzlar, Germany) to count the number of hair cells (HCs) present at each cochlear turn, thereby determining the extent of HC loss. For each group of animals, the mean losses of inner HCs (IHCs) and at each row of outer HCs (OHCs) in each group were calculated.. 22.
(33) 3.2.4 Histopathological examination Cochlear sectioning along the paramodiolar axis was done followed by hematoxylin/eosin staining. After fixation as described above, the cochleae were decalcified by immersion in 10% ethylenediamine tetra-acetic acid (EDTA) (in 0.1M PBS, pH 7.4) for 4 weeks, with gentle stirring at 4°C. The cochleae were then dehydrated, embedded in paraffin, and serially sectioned (4 μm thick) parallel to the modiolar axis. The sections were plated for hematoxylin/eosin staining and examined under a high-power light microscope.. 3.2.5 Experimental groups The animals were divided into the following groups. (1) Control (n = 6): No surgery. (2) Sham operation (n = 6): The animals received surgery as described above until the step at which the labyrinthine artery was exposed. Although the overlying dura was excised, the labyrinthine artery was fully exposed only momentarily, and then the wound was closed. (3) Treatment groups: The animals received surgery as described above until the step at which the labyrinthine artery was exposed. The labyrinthine artery was then temporarily occluded with microclamps for 15 or 30 min or for 1, 2, or 3 h (6 animals per subgroup). Then the microclamps was released, and the wounds were closed. During the time that the arteries were occluded, the effects that clamping had on hearing were monitored by serial click ABR at 120-dB SPL. In each group of 6 sacrificed animals, 4 cochleae were prepared for cochlear surface preparation and HC counting. The cochleae of the other two animals were sectioned along paramodiolar axis and stained with hematoxylin/eosin.. 3.2.6 Statistical analysis The ABR threshold shifts and the percentages of HC loss between the control and the sham-op group, and between the control and each of the treatment groups were analyzed using the non-parametrical Mann-Whitney U-test contained in the SPSS program (version 13.0 for Windows, SPSS Inc., USA). A p value of <0.05 was considered statistically 23.
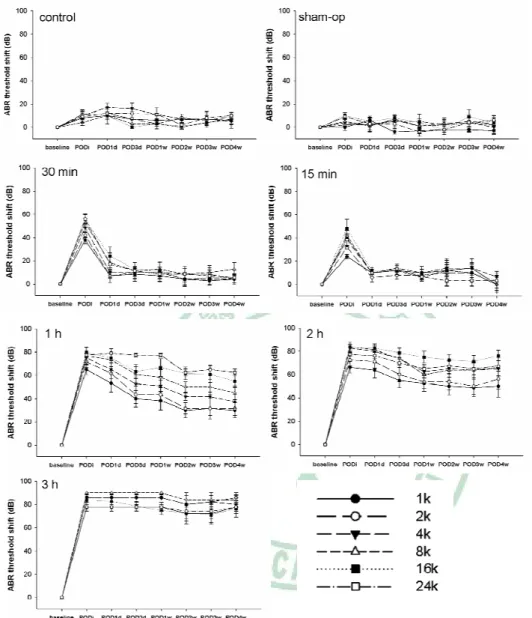
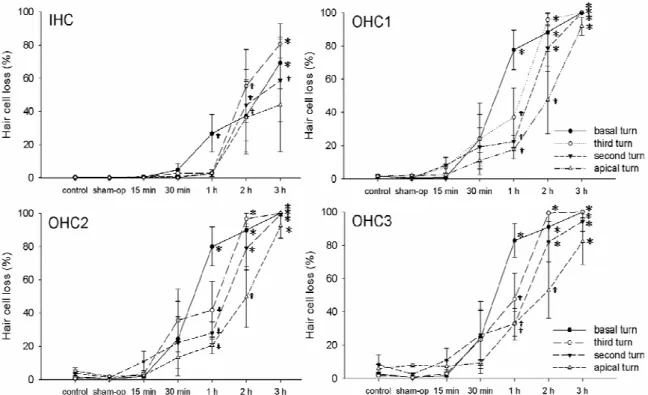
(34) significant.. 3.3 Results 3.3.1 Time and dose responses in ABR threshold shifts caused by cochlear ischemia The serial ABR threshold shifts found after transient cochlear ischemia of different durations are depicted in Fig. 2. No significant ABR threshold shifts were noted for the control group or the sham-op group. When the labyrinthine artery was clamped off for 15 or 30 min, marked ABR threshold shifts occurred but returned to pre-operative levels within 3 days. Persistent ABR threshold shifts were noted for the groups treated for ≥1 h. For the 1-h ischemia group, threshold shifts associated with higher frequencies (8–24 kHz) were larger than those associated with lower frequencies (1–4 kHz). More-severe threshold shifts were noted for the 2-h treatment group, and for this group, threshold changes were also larger for the high-frequency region than for the lower-frequency region. After a 3-h treatment period, the ABR threshold shift nearly approached the maximum stimulation level. In Fig. 3, we summarize the mean ABR threshold shifts for each group taken from the ABR audiograms recorded 4 weeks after treatment. No significant differences were found for the control group, the sham-op group, and the 15- and 30-min ischemia groups. For the 1-h treatment group, marked ABR threshold shifts that decreased as the frequencies increased were found. Severe ABR threshold shifts were noted for the 2-h treatment group, and profound ABR threshold shifts were found for the 3-h treatment group.. 3.3.2 Hair cell loss The amount of OHCs lost increased as the ischemia duration increased, but OHC loss did not increase significantly until the ischemia period was ≥1 h. OHC loss was more severe in the basal turn than in the apical turn. The amount of IHCs lost did not increase significantly until the animals were treated for at least 1 h, and for these animals, the loss was more severe in the basal turn than in the apical turn. The loss of IHC in the upper 24.
(35) turns was not significant until ischemia was ≥2 h (Fig. 4). There was a loss of HCs, especially the OHCs, 4 weeks after the 2-h ischemia (Fig. 5). The OHCs of the basal turn were nearly completely absent 4 weeks after the 2-h ischemia, although residual HCs were still present in the upper turns (Fig. 5).. 3.3.3 Histopathological analysis The morphology of spiral ganglion neurons (SGNs) were grossly normal 4 weeks after a 30-min ischemia treatment (Fig. 6A, B). SGN loss was, however, apparent after 1 h of ischemia (Fig. 6C) and became more severe as the treatment period increased (Fig. 6D). The gross architecture of the organ of Corti remained intact 4 weeks after the 30-min treatment (Fig. 6B). When ischemia lasted ≥1 h, however, hair cells had flattened and there was progressive loss of SGNs (Fig. 6C, D).. 3.4 Comments and conclusion Several different approaches have been developed to study the effects of transient cochlear ischemia in different animals. The occipital approach, during which the neurovascular bundles in the internal auditory canal are exposed by occipital craniotomy before being temporarily occluded, has been used in guinea pig (Tsuji et al., 2002), gerbil (Mom et al., 1997), and rabbit (Morawski et al., 2006). The skull base approach involves transient compression of the neurovascular component in the internal auditory canal after surgically entering through the base of the skull. This method has been used in gerbils (Ren et al., 1995) and guinea pigs (Kusakari et al., 1981). The ventral approach, during which the labyrinthine artery just medial to the cochlear turns is accessed through the auditory bulla cavity (Perlman et al., 1959), has been used in guinea pigs. The hindbrain approach for which, because of the peculiar anatomy of posterior brain circulation in gerbils, transient cochlear ischemia is achieved by compressing the bilateral vertebral artery (Maetani et al., 2003). Although the guinea pig labyrinthine artery originates from the AICA, and only it supplies blood to the cochlea, marked variations exist in the anastomoses and the branching pattern of the AICA. Therefore, attempts to produce 25.
(36) cochlear ischemia by compressing the AICA is unreliable and should not be used in guinea pigs (Ren et al., 1993). The various surgical approaches have different limitations and applications when used with different species. For example, the hindbrain approach to occlude the bilateral vertebral artery produces reversible and consistent cochlear ischemia in gerbils but can be used only with gerbils because of their peculiar posterior brain circulation. When bilateral vertebral artery occlusion was used in guinea pigs, the results were inconsistent (Randolf et al., 1990). Bilateral occlusion of the vertebral artery for ≥1 h may also damage the brainstem vital nuclei, thereby limiting the ischemia period. The esophagus and pharynx must be removed when the skull base approach is used. Therefore, longer observation periods of > 1 d may not be feasible. A relatively long observation period (1 week) after transient cochlear ischemia was possible when the occipital approach was used (Tsuji et al., 2002). In the study reported herein, we used the ventral approach to expose the labyrinthine artery. The surgical field was accessed through the auditory bulla, which limited brain damage. The pharynx and trachea were also preserved. The guinea pigs survived for a relatively long period of time (4 weeks) after their operations, so that observation over a period of weeks was possible. A possible drawback to the ventral approach is that the operative field is very narrow. We could not continuously and directly monitor the ischemia induced by the microclamps using an instrument such as a laser dopplerometry. When we placed a probe of laser dopplerometry at the basal turn of the cochlea and attempted to continuously monitor the ischemia, decreased cochlear blood flow was observed (Fig. 2.4). However, cerebrospinal fluid that leaked from the fenestrum at the base of the skull interfered with the continuous measurement of cochlear blood flow and made the measurements variable and inconsistent. Therefore, we monitored the occlusions by serial ABR. The cochlea has a very low oxidative reserve and is very sensitive to interruption of the blood supply; the electrical activity of the cochlea disappears within seconds when the blood supply is interrupted (Perlman et al., 1959). Serial ABR monitoring has been widely used during skull base surgery and during operations on lesions in the cerebellopontine area, e.g., 26.
(37) vestibular schwannoma surgery (Legatt, 2002). Once the cochlear blood flow is interrupted, the entire ABR waveform disappears (Legatt, 2002). In contrast, when the damage is localized to the auditory nerve or the central auditory pathways in the brainstem or mesencephalon, the classic ABR waveforms may instead be altered: late ABR waveforms (e.g., waveforms III–V) may disappear, whereas early ABR waveforms, (e.g., waveforms I and/or II) remain visible (Legatt, 2002). In this study, when the microclamps were successfully applied to the labyrinthine artery, the ABR waveforms completely disappeared but rapidly reappeared when the microclamps were removed (Fig. 2.8). These observations suggest that the ABR waveform disappeared when cochlear blood flow was interrupted. In our preliminary studies, we verified the occlusion effect produced by the microclamps using intracardiac perfusion with 3% trypan blue. Trypan blue did not perfuse into the microclamped cochlea but did perfuse into the control cochlea. Therefore, we believe that the microclamps successfully and reversibly occluded the arterial blood supply to the guinea pig cochlea. The ABR threshold shifts returned to pre-operative levels when cochlear ischemia was induced for ≤ 30 min. Partial recovery of ABR threshold shifts occurred if cochlear ischemia was induced for ≥ 1 h, and poor ABR recovery occurred if cochlear ischemia was ≥3 h (Fig. 2, 3). As defined by Perlman and colleagues(Perlman et al., 1959), the revival time is the maximum duration of ischemia after which auditory responses can fully return. The revival time of the guinea pig cochlea after transient ischemia may therefore be up to 30 min. The recovery of ABR threshold shifts after shorter periods of cochlear ischemia (≤ 30 min) occurred within 3 days. ABR recovery from the 1-h ischemia did, however, seem to progress up to 2 weeks, which is a time period similar to the clinical course of SSHL. It has been proposed that ischemic damage possibly contributes to SSHL (Nagahara et al., 1983). Most patients with SSHL spontaneously recover, although some continue to suffer from variable degrees of hearing loss (Byl, Jr., 1984). The time between the initial insult and when treatment begins is a major prognostic indicator of hearing recovery from SSHL. Early intervention aids in recovery. The longer patients wait before beginning medical treatment after the onset of SSHL, the 27.
(38) poorer the recovery (Byl, Jr., 1984). The hearing status in a substantial number of SSHL patients does, however, improve long after the cessation of treatment (Wilkins, Jr. et al., 1987), possibly because of the long recuperation potential, as shown in this study. Our results also showed that ABR threshold shifts were associated more with the high-frequency range than with the low-frequency range. These observations were confirmed by morphological examination of the cochlear surface preparation and the numbers of HCs that were stained with phalloidin. The basal turn HCs seemed to be more susceptible to ischemic damage than were the upper turn HCs. These observations had been found in previous cochlear ischemia studies that used guinea pigs (Perlman et al., 1959) and gerbils (Maetani et al., 2003). The basal portion of the cochlea has a greater rate of oxygen consumption than does the upper apical portion (Mizukoshi and Daly, 1967). Conversely, the energy reserve of the organ of Corti, especially glycogen, follows an inverse base-to-apex distribution—more glycogen is found in the apical turns than in the basal turns (Thalmann et al., 1972). A base-to-apex gradient of differential intrinsic susceptibility to free radicals has also been reported (Sha et al., 2001). Free radicals and reactive oxygen species are common products of ischemia-reperfusion injuries. The HCs in the basal turns are more vulnerable to free-radical damage than are those in the apical turns (Sha et al., 2001). These observations could explain why the apical turn tolerates ischemic damage better than the basal turn does. In addition to the intrinsic base-to-apical differential susceptibility to ischemia, this study also showed that guinea pig OHCs were more vulnerable to ischemia than were the IHCs. After 4 weeks, minimal OHC loss occurred when ischemia lasted 15 min, but OHC loss in each cochlear turn was apparent after a 1-h ischemia treatment. Mild loss of IHCs was found after a 30-min ischemia treatment, and significant basal-turn IHC loss was found 4 weeks after a 1-h treatment (Fig. 3.3). In guinea pigs, OHCs may be more vulnerable to ischemia-reperfusion injury than are IHCs (Perlman et al., 1959; Tabuchi et al., 2002). In addition to ischemic damage, OHCs in guinea pigs are more vulnerable to other kinds of cochlear injuries, such as aminoglycoside ototoxicity(Suzuki et al., 2008). With the longer periods of ischemia, both IHCs and OHCs may be affected. Early IHC 28.
(39) loss rather than OHC loss after cochlear ischemia may occur in other species, as IHC loss occurs more readily in gerbils when their cochleae are subjected to ischemia-reperfusion by occlusion of the bilateral vertebral artery (Maetani et al., 2003). Comparatively, more OHC loss after ischemic injury was found for guinea pigs when a similar surgical approach was used to perturb the bilateral vertebral artery (Olszewski et al., 2003). Glucocorticoids possess protective effects against cochlear ischemic damage to guinea pig OHCs (Tabuchi et al., 2006) and gerbil IHCs (Maetani et al., 2009). Therefore, the susceptibility differences of IHCs and OHCs to ischemia may reflect a species difference. We also found that SGNs were damaged 4 weeks after induced transient ischemia. In addition to direct injury produced by ischemia, secondary SGN loss occurs after HC loss, especially IHC loss (Bae et al., 2008). External insults such as noise trauma, aminoglycoside ototoxicity, or cochlear ischemia could induce excessive glutamate release from IHCs into synaptic clefts. A large glutamate concentration causes SGN cell death(Steinbach and Lutz, 2007). In this study, hair cell loss was not apparent unless the animals were treated for 1 h or longer. In the 30-min ischemia group, mild OHC loss was found, whereas IHCs remained relatively unaffected. Additionally, SGN loss was not apparent unless the animals were treated for 1 h, and the morphology of the SGNs remained relatively intact in the 30-min ischemia group. The loss of the SGNs paralleled the loss of IHCs.. Conclusion Orderly functional and cellular changes in the cochlea were found depending on the duration of ischemia. A base-to-apex gradient of ischemia susceptibility seemed to exist. HCs and SGNs were most vulnerable to ischemia. The loss of SGNs paralleled the loss of IHCs. The revival time for guinea pig cochlea after transient ischemia may be up to 30 min.. 29.
(40) 3.5 Figures. Figure 3.1 Serial ABR threshold shifts after different periods of transient cochlear ischemia induced by microclamps. No significant ABR threshold shifts were noted in the control and sham-op groups. Transient ABR threshold shifts were found for the 15- and 30-min ischemia groups. Progressive partial recovery of the ABR threshold shifts was found for the 1-h ischemia group. X-axis indicates the timing for serial ABR measurement, from baseline, PODi, POD1d, 3d, 1w, 2w, 3w, and 4w. The abbreviations PODi, POD1d, 3d, 1w, 2w, 3w, and 4w are defined in Materials and Methods. The value with error bar in each point indicates mean ± standard error (S.E.). 30.
(41) Figure 3.2 ABR threshold shifts 4 weeks after cochlear ischemia treatments of different durations. Compared with the control group, no significant threshold shifts were noted for the sham-op group or when ischemia lasted ≤30 min (p > 0.05) but significant ABR threshold shifts were found when ischemia lasted ≥1 h (*, p < 0.001). A decline-type audiogram was found for the 1 h treatment. The ABR threshold shifts were more severe for the 2 h treatment. The value with error bar in each point indicates mean ± standard error (S.E.).. 31.
(42) Figure 3.3 Hair cell loss induced by ischemia. Compared with the control group, OHC loss and IHC loss at the basal turn were significant when ischemia was ≥ 1 h. However, loss of IHCs in the upper turns was not significant unless ischemia was ≥ 2 h. The value with error bar in each point indicates mean ± standard error (S.E.). (†, p < 0.05; *, p < 0.001).. 32.
(43) Figure 3.4 Hair cell (HC) labeling with rhodamine-conjugated phalloidin in animals 4 weeks after 2 h ischemia. Complete loss of Inner HCs (IHC) and the three rows of outer HCs (OHC1, OHC2, OHC3) were depicted in the basal turn. Significant loss of HCs was present in the third turn. Some IHCs and OHCs were identifiable in the second and apical turns. Bar=20μm. 33.
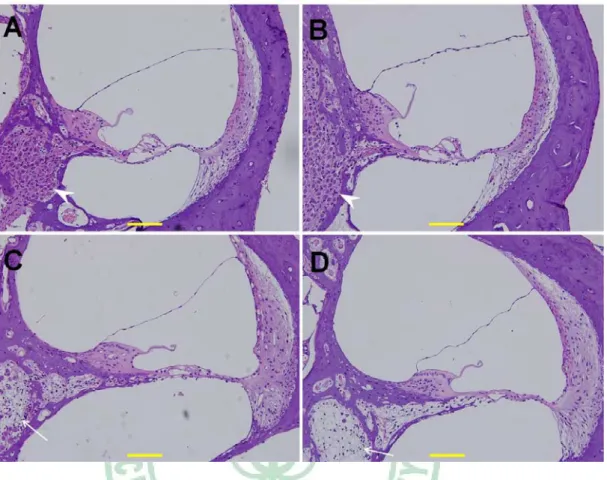
(44) Figure 3.5 Hematoxylin/eosin-stained cochlear sections. A. Normal cochlear section. B. A cochlear section taken 4 weeks after 30 min of ischemia. The architecture of the organ of Corti was intact, contained abundant spiral ganglion neurons (SGNs), and did not show significant spiral neuron loss (arrow head). C. Cochlear section taken 4 weeks after 1 h of ischemia. Apparent loss of SGN (arrow) and flattening of the organ of Corti were observed. D. Cochlear section taken 4 weeks after 2 h of ischemia. Severe loss of SGNs was accompanied by additional flattening of the organ of Corti. Bar=50μm. 34.
(45) Chapter 4 Effect of hyperbaric oxygen on guinea pig’s cochlea ABSTRACT Hyperbaric oxygen therapy (HBOT) is a known adjuvant for treating ischemia-related inner ear diseases. Few studies have yet to investigate the cellular changes that occur in inner ears after HBOT. Nitric oxide, which is synthesized by nitric oxide synthase (NOS), is an important signaling molecule in cochlear physiology and pathology. This study investigated the effects of hyperbaric oxygen on eardrum morphology, cochlear function and expression of NOS isoforms in cochlear substructures after repetitive HBOT in guinea pigs. Minor changes in the eardrum were observed after repetitive HBOT, which did not result in a significant hearing threshold shift by tone burst auditory brainstem responses (ABR). A differential effect of HBOT on the expression of NOS isoforms was identified. Upregulation of constitutive NOS (nNOS and eNOS) was found in the substructures of the cochlea after HBOT, but inducible NOS was not found in normal and HBOT animals, as shown by immunohistochemistry. There was no obvious DNA fragmentation present in this HBOT animal model. The present evidences indicated that the customary HBOT protocol may increase constitutive NOS expression but such upregulation did not cause cell death in the treated cochlea. The auditory morphology and function are consequently not changed through the protocol.. 4.1 Background 4.1.1 Therapeutic implications of cochlear ischemia Since 1998, there were several trials of chemical agents in the hope to prevent or alleviate cochlear damage from ischemia. These trials could be classified into two major groups: (1) pre-condition or protective effect, i.e., the treatment was given before the episode of ischemia. The aim is to prevent, amoleriate or protect cochlear damage from ischemia. 35.
數據

+7
相關文件
From the above- mentioned perspective, this research paper analyses Buddhist interaction in Taiwan and Hokkien; the ordination of Taiwanese Sangha in Kushan Mountain and, after the
臺大機構典藏NTUR (National Taiwan University 二 Repository, http://ntur.lib.ntu.edu.tw) 經驗與協助推 動臺灣學術機構典藏TAIR (Taiwan Academic Institutional Repository,
This article is for the founding of the modern centuries of Buddhist Studies in Taiwan, the mainland before 1949, the Republic of China period (1912~1949), and Taiwan from
Promote project learning, mathematical modeling, and problem-based learning to strengthen the ability to integrate and apply knowledge and skills, and make. calculated
Later, though, people learned that Copernicus was in fact telling the
After the SARS crisis in 2003, there is a huge and on-going reform in the post-graduate medical training program to improve the medical service in Taiwan. Our institute has
Estimated resident population by age and sex in statistical local areas, New South Wales, June 1990 (No. Canberra, Australian Capital
Consistent with the negative price of systematic volatility risk found by the option pricing studies, we see lower average raw returns, CAPM alphas, and FF-3 alphas with higher
