Haptic Virtual Reality Pinch Task for Chronic Hemiparesis
Shuya Chen1, Shih-Ching Yeh2*, Margaret McLaughlin3, Albert Rizzo4, Carolee Winstein51Department of Physical Therapy, China Medical University, Taichung 404, Taiwan
sychen@mail.cmu.edu.tw
2Department of Computer Science and Information Engineering, National Central University, Taoyuan 320, Taiwan
shihchiy@csie.ncu.edu.tw
3Annenburg School for Communication and Integrated Media Systems Center, University of Southern California, Los Angeles,
CA, 90089, USA mmclaugh@usc.edu
4Institute for Creative Technologies, University of Southern California, Los Angeles, CA, 90089, USA
arizzo@usc.edu
5Division of Biokinesiology and Physical Therapy at the School of Dentistry, University of Southern California, Los Angeles,
CA, 90033, USA winstein@usc.edu
Abstract. Incorporating the virtual reality technology into stroke rehabilitation has been proved to be effective in
improving upper extremity function for stroke survivors. However, without haptic feedback, the recovery of pinch skill will not be sufficient for daily activities. Pinch skill is an important component for hand manipulation. Impaired pinch skill affects dexterity function after stroke. This study aimed to develop a haptic virtual reality pinch task and to investigate its feasibility and effectiveness for chronic hemiparesis. The pinch task in the virtual environment was accomplished by coordinating two PHANTOM devices that provide haptic feedback. Participants grasped and lifted a virtual cube within 30 seconds for 10 trials. Cube size, cube mass and lift height were systematically varied. The participant poststroke attempted an average of 38 trials per session with a 60% success rate and without complaint of fatigue or pain. After training, the participant poststroke decreased the total time. However, the peak pinch force did not change. The results suggest that the haptic virtual reality pinch task was feasible for chronic hemiparesis. Further investigation is warranted to better understand the pinch force regulation using hepatic feedback.
Keywords: haptic, virtual reality, pinch, hemiparesis
1 Introduction
Pinch, the squeezing movement between the thumb and a finger, is one the important skills of upper extremity in performing daily activities . After stroke, around 60%of the patients encountered difficulties in regaining their upper extremity functions in six month . While many patients poststroke regain most of the reaching and grasp capabilities for their upper extremity function after rehabilitation, recovery of the pinch skill remains incomplete for most of the patients . Impaired pinch skill significantly affects dexterity function for stroke survivors, leading to higher dependency of daily activities and poor quality of life . With considerable amount of practice , the regained pinch capability would significantly improve the upper extremity function after stroke.
To restore poststroke functional ability, task-oriented training is one of the dominant approaches for motor control and relearning . The characteristics of task-oriented training program should be challenge, adaptable, repetitive, interesting and meaningful. One recent technology, virtual reality, has been shown to be beneficial for the enhancement of hand function poststroke , because game-like exercises are motivating and allow therapists to easily modify training parameters . The application of virtual reality is a form of task-oriented training. With the principle of task-oriented training in mind, re-acquisition of meaningful pinch function after stroke should focus on not only its range of motion, but also its use of appropriate force to generate object perception. However, most of the research about restoring pinch skill after stroke has been focusing on the kinematic control; very few studies examined pinch force modulation. This study aimed to develop a haptic virtual reality pinch task and to investigate its feasibility and effectiveness for chronic hemiparesis.
2 Methods & Materials
2.1 Participants
One participant with poststroke hemiparesis was recruited based on the following criteria: (1) more than 18 years of age, (2) stroke at least 1 month prior, (3) Mini-Mental Status Exam score ≥ 24, (4) no significant range of motion limitations in the hemiparetic upper extremity, (5) ability to perform the haptic virtual reality pinch task. One control participant was chosen to match with the poststroke participant’s age, tested hand, and total time on the pinch task.
2.2 Haptic Virtual Reality Pinch Task
The pinch task was one of four upper extremity virtual reality-based tasks from our pilot project . To develop the pinch task in virtual environment with force feedback, there were two PHANToM devices (SensAble Technologies Inc., Woburn, MA) placed perpendicular to each other for the pinch movement ( and in the Figure 1) and reconfigured to provide hepatic feedback for the pinch task. Haptic feedback was provided for the thumb and index finger through the PHANToM devices, so that the participants felt they were lifting a real cube with mass. Each trial was configured using eight parameters: cube width (20–40 mm), cube height (20–40 mm), cube length (20–40 mm), mass (50–150 gw), dynamic friction (0.5–1.0), static friction (0.5–1.0), stiffness (0.5–1.0), and lift height (20–80 mm). However, dynamic friction, static friction, and stiffness were not used eventually because they were not working well in our pilot study.
Figure 1. Arrangement of two PHANToM devices. Two PHANToM devices were placed perpendicular to each other for the
pinch movement
2.3 Testing Procedure
Participants sat in front of the computer screen with their tested thumb and index finger attached to the PHANTOM devices (Figure 1). Before the trials, the 7-cm distance between the thumb and index finger were positioned and calibrated to reconfigure the metrics in the virtual environment (Figure 2). An experienced physical or occupational therapist worked with the participants. The responsibility of the therapist was to choose appropriate practice blocks and task parameters for participants.
Participants were asked to successfully pick the virtual cube up from the floor, lift it to a specified height, and place it back on the floor without dropping (Figure 3). A maximum of 30 seconds was allowed for each trial. There were 10 trials per block. Cube size, cube mass and lift height could be systematically varied according to the participant’s capability level. The number of successful hit and total time on the task were provided as performance feedback after each block. When the participants successfully complete one block of test, they would hear the clapping sound immediately after the block. Both participants practiced the pinch task for 15 minutes over three weeks for 12 training sessions.
1
Figure 2. Calibration in order to reconfigure the metrics in the virtual environment
Figure 3. The display of actual training
2.4 Outcome Measures
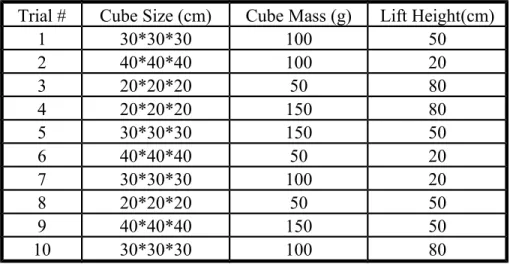
A preset benchmark block of the pinch task (Table 1) and the behavioral assessments including the Fugl-Meyer Assessment (FMA) and the Box and Block test (B&B) were conducted pre- and post- training to evaluate the effectiveness of the haptic virtual reality system. Total time on the task and the peak pinch force on the benchmark block were further calculated.
Trial #
Cube Size (cm)
Cube Mass (g)
Lift Height(cm)
1
30*30*30
100
50
2
40*40*40
100
20
3
20*20*20
50
80
4
20*20*20
150
80
5
30*30*30
150
50
6
40*40*40
50
20
7
30*30*30
100
20
8
20*20*20
50
50
9
40*40*40
150
50
10
30*30*30
100
80
3 Results & Discussion
3.1 Demographic Data
The participant poststroke was dominant hand affected. When the participant poststroke came for the training, he was in his chronic stage after stroke (Table 2).
Table 2. Demographic data of study participants
Age (y)
Sex
Dominant Hand
Tested Hand
Time after Stroke (m)
Stroke
59
Male
Right
Right
24
Control
60
Female
Right
Right
3.2 Training Performance
Given that the duration of training time was arranged to be matched between both participants, the participant poststroke was able to complete 11 training sessions with the haptic virtual reality pinch task (Table 3). The average training time per session was 12.4 minutes for the participant poststroke whereas it was 15.9 minutes for the control participant. The participant poststroke attempted an average of 38 trials per session with a 60% success rate and without complaint of fatigue or pain. Eventhough the total time was fluctuating throughout the sessions; there was a tendency of decreasing the average time, indicating an improvement of pinch skill of the affected hand (Figure 4).
Table 3. Overall training performance
Training
Days
Training Time
(hrs)*
Blocks
Completed
Trials
Completed
Successful
Trials
Success Rate
(%)
Stroke
11
2.28
48
415
250
60.24
Control
8
2.12
134
1260
1252
99.37
Figure 4. The performance time across sessions
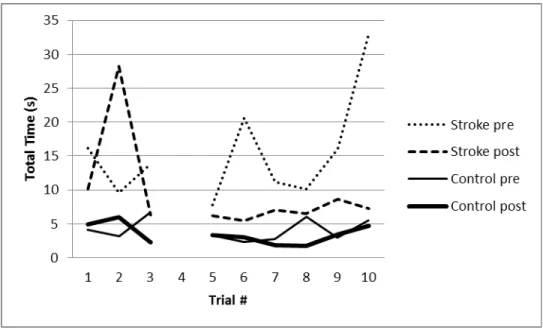
3.3 Training Effect – Total Time on Task
The benchmark block was the probe trial to examine the training effect. The trial 4 was eliminated due to unpredictable programming problems. Within the same block, the total time per trial and the total time per block were longer for the participant poststroke compared to the control participant (blue line vs green line; red line vs purple line in Figure 5). After training, the participant poststroke reduced the total time per trial on the benchmark block (blue line vs red line in Figure 5), except the trial 2. The virtual cube of the trial 2 was 40cm3 with 100gm, and the goal for this trial was to life the cube up to the 20cm height. Although the target height was not difficult to reach, the first biggest cube size in the benchmark block might be the reason of poor pinch performance.
Figure 5. Total time for each trial on the benchmark block pre- and post- training
* Trial 4 was eliminated due to programming problems
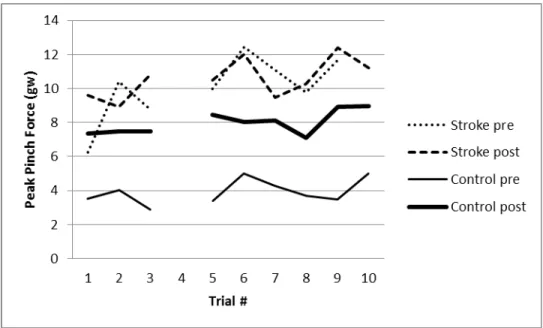
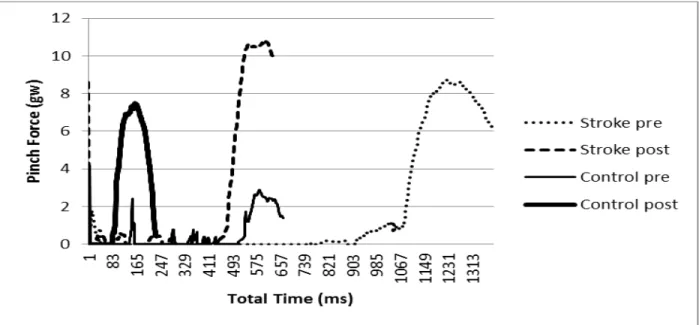
Peak pinch force in the benchmark block shows in Figure 6. Pre-training peak pinch force was greater for the participant poststroke than the control participant. After training, the participant poststroke used a higher grip force for most of the trials (5 out of 9 trials) in the benchmark block while the control participant used a higher grip force for all trails. However, the higher grip force did not reach the significant level for the participant poststroke. The tendency of using a higher grip force for lifting the virtual cube may be associated with the concomitant increased lifting speed evidenced by shorter total time per trial. The findings suggest that the participant poststroke could perform a haptic virtual reality pinch task and improve speed of performance with practice without a significant change in peak force modulation. An example trial (Trial 3) of peak pinch force on the benchmark pre and post training for both participants was shown in Figure 7. The total time post-training for the hemiparetic participant became shorter to the extent very close to the total time for the control participant at the pre-training (the end of red line vs the end of green line in Figure 7). This finding suggests that there was a potential of recovery with appropriate training within a short period of training.
Figure 6. Peak pinch force for each trial in the benchmark block pre- and post- training
Figure 7. An example (t3) of peak pinch force on the benchmark pre and post training for both participants
3.5 Training Effect – Behavioral Measures
As for the behavior performance, the participant poststroke improved on the score of the Fugl-Meyer Assessment (FMA) and the completed time on the benchmark block (Table 4). The results suggest the effectiveness of the haptic virtual reality pinch task for stroke rehabilitation.
Table 4. Behavior and virtual reality performance data pre-post training
FMA
B&B
Total Time on BM (ms) (9 trials)*
Pre
Post
Pre
Post
Pre
Post
Stroke
48
55
17
17
138.37
85.88
Control
36.94
31.42
FMA: Fugl-Meyer Assessment; B&B: Box and Block test; BM: Benchmark block. * Trial 4 was not included in calculating total time on BM.
4 Conclusions
Post-stroke participant could perform a haptic virtual reality pinch task and improve speed of performance with practice. A lack of explicit feedback regarding force during task performance may explain the similar peak force after training. Further investigation is warranted to better understand the effect of pinch force regulation during haptic virtual reality training for people poststroke.
5 Acknowledgements
This study was supported by the Interdisciplinary Study of Neuroplasticity and Stroke Rehabilitation (ISNSR), an NIH Exploratory Center for Interdisciplinary Research (Grant # P20 RR20700-01) and the Integrated Media Systems Center, an NSF Engineering Research Center (Cooperative Agreement # EEC-9529152), both at the University of Southern California.
References
1. Blennerhassett, J.M., L.M. Carey, and T.A. Matyas, Grip force regulation during pinch grip lifts under somatosensory guidance: comparison between people with stroke and healthy controls. Arch Phys Med Rehabil, 2006. 87(3): p. 418-29.
2. Blennerhassett, J.M., T.A. Matyas, and L.M. Carey, Impaired discrimination of surface friction contributes to pinch grip deficit after stroke. Neurorehabil Neural Repair, 2007. 21(3): p. 263-72.
3. Mayo, N.E., et al., Activity, participation, and quality of life 6 months poststroke. Arch Phys Med Rehabil, 2002. 83(8): p. 1035-42.
4. Broeks, J.G., et al., The long-term outcome of arm function after stroke: results of a follow-up study. Disability and Rehabilitation, 1999. 21(8): p. 357-64.
5. Faria-Fortini, I., et al., Upper Extremity Function in Stroke Subjects: Relationships between the International Classification of Functioning, Disability, and Health Domains. J Hand Ther, 2011.
6. Kleim, J.A. and T.A. Jones, Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. J Speech Lang Hear Res, 2008. 51(1): p. S225-39.
7. Winstein, C.J. and S.L. Wolf, Task-oriented training to promote upper extremity recovery, in Stroke Recovery & Rehabilitation, J. Stein, et al., Editors. 2009, Demos Medical Publishing: New York. p. 267-290.
8. Wade, E. and C.J. Winstein, Virtual reality and robotics for stroke rehabilitation: where do we go from here? Top Stroke Rehabil, 2011. 18(6): p. 685-700.
9. Merians, A.S., et al., Virtual reality-augmented rehabilitation for patients following stroke. Phys Ther, 2002. 82(9): p. 898-915.
10. Crosbie, J., et al., Development of a virtual reality system for the rehabilitation of the upper limb after stroke. Stud Health Technol Inform, 2005. 117: p. 218-22.
11. Stewart, J.C., et al., Intervention to enhance skilled arm and hand movements after stroke: A feasibility study using a new virtual reality system. J Neuroeng Rehabil, 2007. 4: p. 21.
12. Stewart, J.C., et al., Training reach movements in individuals with hemiparesis: effect of a virtual environment. J Neurol Phys Ther, 2007. 31(4): p. 192.
13. Fugl-Meyer, A.R., et al., The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand J Rehabil Med, 1975. 7(1): p. 13-31.
14. Desrosiers, J., et al., Validation of the Box and Block Test as a measure of dexterity of elderly people: reliability, validity, and norms studies. Arch Phys Med Rehabil, 1994. 75(7): p. 751-5.


![TraditionalMLCalgorithmsmainlytacklethebatchMLCproblem,wheretheinputdataarepresentedinabatch[24,28].Nevertheless,inmanyMLCapplicationssuchase-mailcategorization[22],multi-labelexamplesarriveasastream.Onlineanalysisistherefore dimensionreducermotivatedbyma](data:image/gif;base64,R0lGODlhAQABAIAAAP///wAAACH5BAEAAAAALAAAAAABAAEAAAICRAEAOw==)