Association
between
17-HSD8
Polymorphisms
and
1Kawasaki Disease among Han Chinese Children in Taiwan
23
Shih-Yin Chen a,b,Ying-Ju Lin a,b,Jeng Sheng Chang d,Yu-Chuen Huang a,b,Jim 4
Jinn-Chyuan Sheu a,b,Yao-Yuan, Hsieh b,c,Lei Wan a,b, Fuu-Jen Tsai d-f,* 5
6
a
Genetics Center, Department of Medical Research, China Medical University 7
Hospital, Taichung, Taiwan. 8
b
Graduate Institute of Chinese Medical Science, China Medical University, Taichung, 9
Taiwan. 10
c
Division of Infertility Clinic, Hsieh Yao-Yuan Womens’ Hospital, Taichung, Taiwan. 11
d
Department of Pediatrics, China Medical University Hospital, Taichung, Taiwan. 12
e
Department of Medical Research, China Medical University Hospital, Taichung, 13
Taiwan. 14
f
Department of Medical Genetics, China Medical University Hospital, Taichung, 15
Taiwan. 16
17
Correspondence: F. J. Tsai, MD, PhD, Department of Medical Research, China 18
Medical University Hospital, No. 2 Yuh Der Road, Taichung, Taiwan. E-mail: 19
20
SY Chen, Ph.D., and YJ Lin, Ph.D. are joint first authors and equal contribution in 21
this study. 22
23
ABSTRACT: Kawasaki Disease (KD) is considered infectious, with immunologic 24
expressions caused by genetic susceptibility of individuals. The 17-hydroxysteroid 25
dehydrogenase type 8 (17-HSD8) enzymes are involved in the biosynthesis of 26
estrogens and androgens and regulate immune responses through modulation of the 27
hormone in mammals. The objective of this study was to clarify the relationship 28
between 17-HSD8 gene single nucleotide polymorphisms (SNPs) and the
29
pathogenesis of KD. We investigated association between 17-HSD8 SNPs (rs421446,
30
rs213213) and KD in Taiwanese children. Genotyping analysis involved 93 KD 31
patients and 680 unrelated healthy children. Our findings indicated frequency of A 32
allele in polymorphisms rs421446 was markedly higher among patient (43.3%) than 33
in controls the group (34.0%; p=0.032). Children with the A allele at rs421446 SNP 34
may show higher risk of developing KD, particularly in whom with AA homozygous 35
genotype. Also, from comparison of haplotype frequencies between case and control, 36
children with AC haplotype appeared more “at-risk” for Kawasaki disease 37
progression (p=0.022). Our results suggest that rs421446 polymorphism and the 38
haplotypes in 17-HSD8 gene are associated with the risk of KD in Taiwanese 39 children. 40 41 RUNNING TITLE: 42 17-HSD8 SNPs and KD 43 44 INTRODUCTION 45
Kawasaki disease (KD) is an acute febrile vasculitic syndrome of early childhood who 46
present with fever, rash, conjunctival injection, cervical lymphadenitis, inflammation 47
of the lips and oral cavity, and erythema and edema of the hands and feet1. The first 48
cases were identified among Japanese Children in the 19672. Cardiac sequela, such as 49
coronary artery lesions (CAL), is one of the most important aspects of this disease3. 50
Cause of the disease is a syndrome of unknown etiology, generally believed to be an 51
infectious agent, host immune dysregulation, and genetic susceptibility4,5. Moreover, 52
KD is overrepresented in Asian children, with gender differences observed: i.e., more 53
often in boys (ratio of about 1.5:1)6,7. Annual incidence of KD in Taiwan is estimated 54
to be 69/100,000 children, the third highest in the world after Japan and Korea8,9. 55
The immune response is characterized by the accumulation and expansion of 56
T-helper 1 (Th1) lymphocytes and increased amounts of several proinflammatory 57
cytokines, such as interferon-(IFN-), tumor necrosis factor-(TNF-) and sex 58
hormones10-13. Sex hormonal action on the immune system is thought to account for 59
gender differences in immune capability, dispelling the notion that sex steroid 60
hormones exclusively affect sexrelated endocrinologic functions14. Among vertebrates, 61
the levels of sex steroids within tissues are regulated by a variety of steroidogenic 62
enzymes. The 17-hydroxysteroid dehydrogenases (17-HSDs) enzymes catalyze the 63
oxidoreduction of hydroxyl/keto groups of androgens and estrogens15 and they are 64
involved in the biosynthesis of estrogens and androgens and modulation of their 65
hormone action in steroidogenic as well as in peripheral tissues in mammals16. 66
Multiple types of 17-HSDs (named types 1–12) have been cloned and have been 67
shown to be expressed in several human and animal tissues15,17,18. The type 8 68
17-HSD has been recently identified. It is also known as the product of the Ke 6 69
gene, which is found in the human leukocyte antigen region19. 70
As well know, KD is thought to be an infectious disease with immunologic 71
expressions and maybe caused by the genetic susceptible individuals. In this study, we 72
hypothesized that 17-HSD8 genetic variants in the 3’UTR confer KD susceptibility.
73
We examined and compared 17-HSD8 genotype distribution in a group of
74
Taiwanese KD patients and a non-KD control group. An attempt was also made to 75
clarify the association between 17-HSD8 and KD severity.
77
MATERIALS AND METHODS 78
Study Population 79
We enrolled 93 patients from the Department of Pediatrics at China Medical 80
University Hospital from 1998 to 2005. All met the criteria proposed by the Japanese 81
Kawasaki Disease Research Committee (Research Committee on Kawasaki Disease). 82
Patients were treated with intravenous immunoglobulin (IVIG; 2 g/kg infused over 83
8-12 h) and oral aspirin (80-100 mg/kg/day). Echocardiographs were obtained by the 84
pediatric cardiologist before or within two weeks of IVIG administration. CAL were 85
diagnosed from echocardiograms, using criteria proposed by the Japanese Kawasaki 86
Disease Research Committee: coronary arteries were classified as abnormal if internal 87
lumen diameter was > 3 mm in a child younger than 5 years or > 4 mm in those older 88
than 5 years, if the internal diameter of a segment measured ≥ 1.5 times that of an 89
adjacent segment, or if the coronary lumen was clearly irregular. We also studied 680 90
gender-age-matched unrelated healthy children to serve as a control group. All blood 91
samples were drawn before IVIG therapy in KD patient groups; 680 control samples 92
had no prior history of KD and were tested in parallel with patient samples. The ethics 93
committee of China Medical University Hospital’s Institutional Review Board 94
approved the study, with written informed consent from parents of all subjects 95
(DMR97-IRB-246). 96
97
SNP selection 98
17-HSD8 SNPs genotypes information was downloaded in December 2008
99
from the HapMap CHB + JPT population. HapMap genotypes were analyzed within 100
Haploview and Tag SNPs were selected using the Tagger function by applying the 101
following additional criteria: (i) a threshold minor allele frequency (MAF) in the 102
HapMap CHB + JPT population of 0.05 for”tag SNPs”; and (ii) probe/primers that 103
pass the qualification as recommended by the manufacturer (Applied Biosystems), to 104
ensure a high genotyping success rate. Two polymorphisms met the criteria and were 105
selected, including SNP rs421446 (A/G) and rs213213 (C/T) in 3’UTR of 17-HSD8
106
gene (Figure 1). 107
108
Genomic DNA Extraction and Genotyping of 17-HSD8 Polymorphisms 109
Genomic DNA was extracted from peripheral blood leukocytes according to standard 110
protocols (Genomic DNA kit; Qiagen, Valencia, CA, USA). Genotypes of SNPs 111
rs421446 and rs213213 at chromosome positions 6:33174783 and 6:33183730 in 112
3’UTR of 17-HSD8 (Figure 1) gene were identified by high-throughput
113
matrix-assisted laser desorption ionization time-of-flight (MALDI-TOF) mass 114
spectrometry. A detailed description of the procedures is presented by Lin et al, 115 200920. 116 117 Statistical analysis 118
Hardy-Weinberg equilibrium was tested for each marker using χ2-test. Chi-squaretest 119
or Fisher’s exact tests determined statistically significant differences in 120
allele/genotype frequencies between case and control groups. Allelic frequencies were 121
expressed as percentage of aggregate alleles. Haplotype combination at rs421446 and 122
rs213213 in 17-HSD8 gene was estimated using Haploview version4.1 based on 123
accelerated EM algorithm21. Intergroup differences in haplotype frequency were 124
assessed by χ2-test. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were 125
obtained by logistic regression to define association between 17-HSD8
126
alleles/genotypes/haplotypes and KD susceptibility. All data were analyzed with SPSS 127
Version 15.0 software (SPSS Inc., Chicago, IL, USA), p value < 0.05 considered 128
statistically significant. 129
Results 131
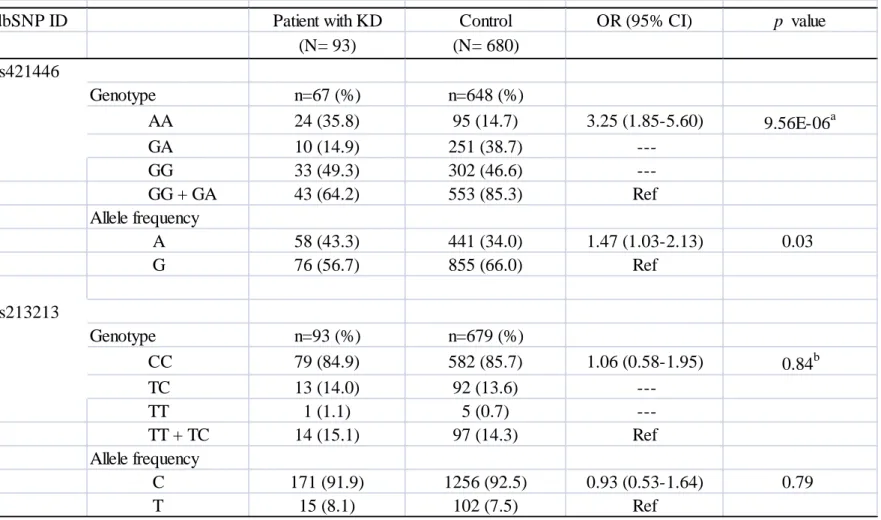
Table 1 plots genotypic and allelic frequencies of rs421446 and rs213213, A allele 132
frequencies at rs421446 polymorphism in KD patients and controls are 43.3% (58/134) 133
and 34% (441/1296), respectively. G allele frequencies in KD patients and controls 134
are 56.7% (76/134) and 66% (855/1296), respectively. When we compared 135
frequencies between case and control groups, results showed A allele frequency in 136
rs421446 polymorphism significantly higher in the patient group (43.3%) than in the 137
control group (34%; p = 0.032, OR = 1.47; 95% CI = 1.03-2.13). Therefore, children 138
with A allele may have higher risk of developing KD. Significant difference in 139
genotype frequency was also found in KD patients and controls (p = 9.557E-06), but 140
none in rs213213 SNP. 141
Haplotype frequencies were estimated using the rs421446 and rs213213 SNPs 142
(Table 2). Three haplotypes of the 17-HSD8 were present in the study population.
143
The GC and AC were the common haplotypes both in KD patients (56.3% and 35.6%, 144
respectively) and health control (65.0% and 27.5%, respectively) groups. Data 145
indicated that compared with haplotype frequencies between groups, children with 146
AC haplotype appeared to be a significant “at-risk” haplotype for KD progression (p 147
= 0.022, OR = 1.46; 95% CI = 1.05-2.01). In addition, the GC haplotype appeared a 148
significant “protective” haplotype compared with other haplotypes (p = 0.021, OR = 149
0.7; 95% CI = 0.51-0.95) (Table 2). 150
In addition, we analyzed whether certain rs421446 and rs213213 haplotypes are 151
associated with development of coronary artery lesions (CAL) in the KD patients 152
(Table 3). Compared with haplotype frequencies in KD patients with/without CAL, 153
GC and AC were common haplotypes both in the KD patients with (65.0% and 30.0%, 154
respectively) and without CAL (51.5% and 39.0%, respectively). Data also indicated 155
that KD patients with GC haplotype seem to develop CAL (65.0%) more often, but 156
the difference was not statistically significant. 157
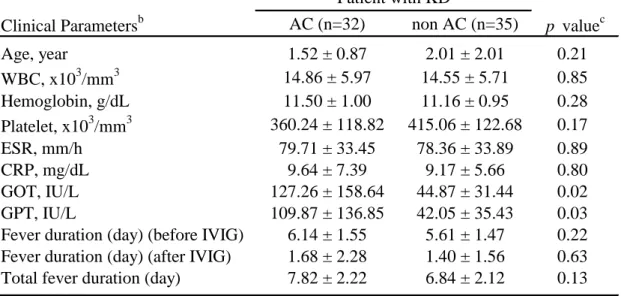
Furthermore, we compared the association between clinical parameters and 158
diplotypes with/without haplotype AC in 17-HSD8 gene (Table 4). The results
159
showed that higher level of glutamate oxaloacetate transaminase (GOT) was observed 160
in KD patients with AC haplotype compared with non AC haplotype (p = 0.022). 161
Likewise, glutamate pyruvate transaminase (GPT) level in KD patients with AC 162
haplotype was statistically significant higher than patients with non AC haplotype (p 163 = 0.03). 164 165 DISCUSSION 166
Currently, KD is viewed as an infectious disease with immunologic expressions 167
caused by genetic susceptibility of individuals4. Polymorphic gene sequences of 168
cytokines definitely involved in pathogenesis of KD are potential markers of disease 169
susceptibility: e.g., tumor necrosis factor-α, Interleukin-1, 10, and 1822-25. 170
This study focused on the variant of 17-HSD8 3'UTR genetic polymorphisms
171
(rs421446 and rs213213) previously investigated for biosynthesis of estrogens and 172
androgens in mammals16. Our data linked the correlation between KD and rs421446 173
of 17-HSD8 polymorphism, and AA homozygous genotype frequency in KD
174
patients was significantly higher than in controls (Table 1). However, the call rate of 175
rs421446 in KD patients was a little bit low. Therefore, we used TaqMan assay 176
(Applied Biosystems) for validating 10% of all samples and got the concordant results. 177
Since rs421446 is located in the promoter region (-176) of 17-HSD8 gene. Previous
178
report indicated that sequences from -260 to -75 of 17-HSD8 promoter region are
179
required for full transcriptional activity26. This suggests that the SNP rs421446 located 180
in the important region of 17-HSD8 gene promoter and may be contributed the
181
different KD develop risk with different transcriptional activity. In addition, our 182
results also indicated haplotypes of 17-HSD8 gene play a significant role in creating
183
susceptibility to KD in the Taiwanese population. Table 2 shows the AC haplotype 184
present in an estimated 35.6% of KD patients. AC haplotype appeared a susceptibility 185
factor for developing KD in our cohort. We also observed individuals with AC 186
haplotype seemed more “at-risk” for Kawasaki disease progression (OR: 1.46, 95% 187
CI: 1.05-2.01; p = 0.022). Briefly, these haplotypes may be involved in a potential 188
role of 17-HSD8 gene in KD pathogenesis, although the precise mechanism remains
189
undetermined. 190
Since inflammation is believed to play a role in pathogenesis of cardiovascular 191
events, measuring inflammation markers has been proposed to enhance prediction of 192
risk of these events27. And several studies suggest that C-reactive protein (CRP) level 193
evaluation may provide a useful method of assessing risk of cardiovascular disease in 194
apparently healthy persons28,29. In our study, high level of CRP (> 5 mg/dL) was 195
observed both in KD patients with/without AC haplotype. We also found total fever 196
duration in KD patients with AC haplotype elongated compared with non AC 197
haplotype, though the difference was not significant (Table 3). In addition, GOT and 198
GPT levels in KD patients with AC haplotype were statistically significant higher 199
than patients with non AC haplotype (p = 0.022 and 0.03, respectively) (Table 4). 200
Previous study indicated that liver function impairment is common in acute stage of 201
KD patients30. Briefly, our data indicated individuals with AC haplotype appeared to 202
be a significant “at-risk” haplotype for Kawasaki disease progression maybe due to 203
the retardations observed in clinical parameters of GOT and GTP which compared 204
with non AC haplotype. 205
Previously study indicated that CAL will be occurred in about 25% of KD 206
patients without therapy, and death may result from coronary artery aneurysm (CAA) 207
rupture or thrombosis, myocardial infarction, or myocarditis3. In this study, we 208
observed 29.9% (20/67) of KD patients with CAL and we analyzed the relationship 209
between rs421446 and rs213213 polymorphisms and CAL development in the KD 210
patients. Our data showed that compared with the KD CAL (-) patients, the KD 211
patients with GC haplotype seem to have higher frequency of CAL (65.0%), though 212
the difference was not significant (Table 3). 213
Our data provide a new information of rs421446 and rs213213 SNPs in disease 214
progression of KD patients which may have important implications in the 215
development of strategies for the prevention, diagnosis and treatment of KD. In 216
conclusion, our study showed variant genotype distribution of 17-HSD8 gene
217
between controls and KD patients. And data also suggested that 17-HSD8 gene
218
(rs421446 and rs213213) SNPs may be the underlying cause of KD; polymorphism 219
revealed by this study warrants further investigation. 220
221
Acknowledgements: This work was supported by China Medical University 222
(CMU98-N1-18), China Medical University Hospital (DMR-98-042 and 223
DMR-98-144), National Science Council in Taiwan (NSC 98-2314-B-039-004-MY2) 224
and Asia University (CMU-asia-05) in Taiwan. 225
REFERENCES 227
1 Taubert KA, Shulman ST (1999) Kawasaki disease. Am Fam Physician 59, 228
3093-102, 3107-8. 229
2 Kawasaki T (1967) Acute febrile mucocutaneous syndrome with lymphoid 230
involvement with specific desquamation of the fingers and toes in children. 231
Arerugi 16, 178-222.
232
3 Pahlavan PS, Niroomand F (2006) Coronary artery aneurysm: a review. Clin 233
Cardiol 29, 439-43.
234
4 Wang CL, Wu YT, Liu CA, et al (2005) Kawasaki disease: infection, immunity and 235
genetics. Pediatr Infect Dis J 24, 998-1004. 236
5 Tse SM, Silverman ED, McCrindle BW, Yeung RS
(
2002)
Early treatment with 237intravenous immunoglobulin in patients with Kawasaki disease. J Pediatr 140, 238
450-5. 239
6 Burns JC, Glode MP
(
2004)
Kawasaki syndrome. Lancet 364, 533–44. 2407 Juan CC, Hwang B, Lee PC, et al
(
2007)
The clinical manifestations and risk 241factors of a delayed diagnosis of Kawasaki disease. J Chin Med Assoc 70, 374-9. 242
8 Chang LY, Chang IS, Lu CY, et al
(
2004)
Epidemiologic features of Kawasaki 243disease in Taiwan, 1996-2002. Pediatrics 114, e678-82. 244
9 Park YW, Han JW, Park IS, et al
(
2005)
Epidemiologic picture of Kawasaki disease 245in Korea, 2000-2002. Pediatr Int 47, 382-7. 246
10 Sugerman PB, Savage NW, Walsh LJ, et al
(
2002)
The pathogenesis of oral lichen 247planus. Crit Rev Oral Biol Med 13, 350-65. 248
11 Simark Mattsson C, Jontell M, Bergenholtz G, et al
(
1998)
Distribution of 249interferon-gamma mRNA-positive cell in oral lichen planus lesions. J Oral Pathol 250
Med 27, 483-8.
251
12 Simark-Mattsson C, Bergenholtz G, Jontell M, et al
(
1999)
Distribution of 252interleukin-2-4-10, tumor necrosis factor-alpha and transforming growth 253
factor-beta mRNA in oral lichen planus. Arch Oral Biol 44, 499-507. 254
13 Strober W, Kelsall B, Fuss I, et al
(
1997)
Reciprocal IFN-gamma and TGF-beta 255responses regulate the occurrence of mucosal inflammation. Immunol Today 18, 256
61-4. 257
14 Ahmed SA, Hissong BD, Verthelyi D, et al
(
1999)
Gender and risk of 258autoimmune diseases: possible role of estrogenic compounds. Environ Health 259
Perspect 107, 681-6.
260
15 Mindnich R, Müller G, Adamski J
(
2004)
The role of 17betahydroxysteroid 261dehydrogenases. Mol Cell Endocrinol 218, 7–20. 262
16 Pletnev VZ, Duax WL
(
2005)
Rational proteomics IV: modeling the primary 263function of the mammalian 17beta-hydroxysteroid dehydrogenase type 8. J Steroid 264
Biochem Mol Biol 94, 327-35.
265
17 Luu-The V
(
2001)
Analysis and characteristics of multiple types of human 26617beta-hydroxysteroid dehydrogenase. J Steroid Biochem Mol Biol 76, 143–151. 267
18 Peltoketo H, Luu-The V, Simard J, Adamski J
(
1999)
17beta-hydroxysteroid 268dehydrogenase (HSD)/17-ketosteroid reductase (KSR) family; nomenclature and 269
main characteristics of the 17HSD/KSR enzymes. J Mol Endocrinol 23, 1-11. 270
19 Kikuti YY, Tamiya G, Ando A, et al
(
1997)
Physical mapping 220 kb centromeric 271of the human MHC and DNA sequence analysis of the 43-kb segment including 272
the RING1, HKE6, and HKE4 genes. Genomics 42, 422-35. 273
20 Lin YJ, Wan L, Wu JY, et al
(
2009)
HLA-E gene polymorphism associated with 274susceptibility to Kawasaki disease and formation of coronary artery aneurysms. 275
Arthritis Rheum 60, 604-10.
276
21 Barrett JC, Fry B, Maller J, Daly MJ et al
(
2005)
Haploview: analysis and 277visualization of LD and haplotype maps. Bioinformatics 21, 263-5. 278
22 Quasney MW, Bronstein DE, Cantor RM, et al
(
2001)
Increased frequency of 279alleles associated with elevated tumor necrosis factor-α levels in children with 280
Kawasaki disease. Pediatr Res 49, 686-90. 281
23 Wu SF, Chang JS, Wan L, et al
(
2005)
Association of IL-1Ra gene polymorphism, 282but no association of IL-1ß and IL-4 gene polymorphisms, with Kawasaki disease. 283
J Clin Lab Anal 19, 99-102.
284
24 Jin HS, Kim HB, Kim BS, et al
(
2007)
The IL-10 (-627 A/C) promoter 285polymorphism may be associated with coronary aneurysms and low serum albumin 286
in Korean children with Kawasaki disease. Pediatr Res 61, 584-7. 287
25 Chen SY, Wan L, Huang YC, et al
(
2009)
Interleukin-18 gene 105A/C genetic 288polymorphism is associated with the susceptibility of Kawasaki disease. J Clin Lab 289
Anal 23, 71-6.
290
26 Villar J, Celay J, Alonso MM, et al (2007) Transcriptional regulation of the human 291
type 8 17beta-hydroxysteroid dehydrogenase gene by C/EBP. J Steroid Biochem 292
Mol Biol 105, 131-9.
293
27 Ridker PM, Hennekens CH, Buring JE, Rifai N
(
2000)
C-reactive protein and 294other markers of inflammation in the prediction of cardiovascular disease in 295
women. N Engl J Med 342, 836-43. 296
28 Ridker PM, Rifai N, Clearfield M, et al
(
2001)
Measurement of C-reactive protein 297for the targeting of statin therapy in the primary prevention of acute coronary 298
events. N Engl J Med 344, 1959-65. 299
29 Visser M, Bouter LM, McQuillan GM, et al (1999) Elevated C-reactive protein 300
levels in overweight and obese adults. JAMA 282, 2131-5. 301
30 Eladawy M, Dominguez SR, Anderson MS, Glodé MP (2011) Abnormal liver 302
panel in acute kawasaki disease. Pediatr Infect Dis J 30,141-4. 303
Table 1 Genotypic and allelic frequencies of 17-HSD8 gene genetic polymorphism in KD patients and controls.
dbSNP ID Patient with KD Control OR (95% CI) p value
(N= 93) (N= 680) rs421446 Genotype n=67 (%) n=648 (%) AA 24 (35.8) 95 (14.7) 3.25 (1.85-5.60) 9.56E-06a GA 10 (14.9) 251 (38.7) GG 33 (49.3) 302 (46.6) GG + GA 43 (64.2) 553 (85.3) Ref Allele frequency A 58 (43.3) 441 (34.0) 1.47 (1.03-2.13) 0.03 G 76 (56.7) 855 (66.0) Ref rs213213 Genotype n=93 (%) n=679 (%) CC 79 (84.9) 582 (85.7) 1.06 (0.58-1.95) 0.84b TC 13 (14.0) 92 (13.6) TT 1 (1.1) 5 (0.7) TT + TC 14 (15.1) 97 (14.3) Ref Allele frequency C 171 (91.9) 1256 (92.5) 0.93 (0.53-1.64) 0.79 T 15 (8.1) 102 (7.5) Ref
CI, confidence interval; OR, odds ratio.
a
Compared with rs421446 AA and AG+GG genotype.
b
Table 2 Distribution of 17-HSD8 gene haplotype frequencies in patients with KD
and controls.
Haplotypea Patient with KD (%)b Control (%) OR (95% CI) p value
(n= 67) (n= 648)
GC 56.3% 65.0% 0.70 (0.51-0.95) 0.02
AC 35.6% 27.5% 1.46 (1,05-2.01) 0.02
AT 6.5% 6.6% 0.99 (0.53-1.83) 0.99
CI, confidence interval; OR, odds ratio.
a
Order of single nucleotide polymorphisms comprising the 17-HSD8 gene
haplotypes: rs421446 and rs213213.
b
Percentages may not sum to 100% because of the presence of the presence of rare haplotypes (<5%) not presented here.
Table 3 Distribution of 17-HSD8 SNPs (rs421446, rs213213) frequencies in KD
patients with/without coronary artery lesions (CAL).
Haplotypea
CAL (+) (n=20) CAL (-) (n= 47) OR (95% CI) p value
GC 65.0% 51.5% 1.75 (0.93-3.31) 0.08
AC 30.0% 39.0% 0.67 (0.35-1.29) 0.23
AT 0.6% 9.2% 0.06 (0.00-19.04) 0.45
Patient with KD (%)b KD CAL(+) vs KD CAL (-)
CI, confidence interval; OR, odds ratio; KD CAL(+)/CAL(-), KD patients with/without CAL.
a
Order of single nucleotide polymorphisms comprising the 17-HSD8 SNPs
haplotypes: rs421446 and rs213213.
b
Percentages may not sum to 100% because of the presence of the presence of rare haplotypes not presented here.
Table 4 Association between 17-HSD8 gene diplotypesa and clinical parameters in KD patients.
Clinical Parametersb AC (n=32) non AC (n=35) p valuec
Age, year 1.52 ± 0.87 2.01 ± 2.01 0.21 WBC, x103/mm3 14.86 ± 5.97 14.55 ± 5.71 0.85 Hemoglobin, g/dL 11.50 ± 1.00 11.16 ± 0.95 0.28 Platelet, x103/mm3 360.24 ± 118.82 415.06 ± 122.68 0.17 ESR, mm/h 79.71 ± 33.45 78.36 ± 33.89 0.89 CRP, mg/dL 9.64 ± 7.39 9.17 ± 5.66 0.80 GOT, IU/L 127.26 ± 158.64 44.87 ± 31.44 0.02 GPT, IU/L 109.87 ± 136.85 42.05 ± 35.43 0.03
Fever duration (day) (before IVIG) 6.14 ± 1.55 5.61 ± 1.47 0.22 Fever duration (day) (after IVIG) 1.68 ± 2.28 1.40 ± 1.56 0.63 Total fever duration (day) 7.82 ± 2.22 6.84 ± 2.12 0.13
Patient with KD
a
17-HSD8 3'UTR diplotypes contain haplotype AC.
b
Data for each group are expressed as mean ± SD.
c