Association between SRC-1 Gene Polymorphisms and Coronary Artery
Aneurysms Formation in Taiwanese Children with Kawasaki Disease
Yng-Tay Chen1, Wen-Lin Liao2, Ying-Ju Lin 1, 3, Shih-Yin Chen1, 3, Fuu-Jen Tsai1,2,4,*
1 Human Genetic Center, China Medical University Hospital, Taichung, Taiwan
2 Center for Personalized Medicine, China Medical University Hospital, Taichung, Taiwan 3 Graduate Institute of China Medical Science, China Medical University, Taichung, Taiwan. 4 Department of Biotechnology and Bioinformatics, Asia University, Taichung, Taiwan
Running title: SRC-1 and CAA in KD patients
YT Chen and WL Liao contributed equally to this paper. *Correspondence to:
Fuu-Jen Tsai
Human Genetic Center, China Medical University Hospital, 2 Yuh-Der Road, Taichung 40447, Taiwan.
Email: [email protected] 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Abstract
Kawasaki disease (KD) patients who experience a cardiovascular complication known as a coronary artery aneurysm (CAA) are at high risk of developing ischemic heart disease, which may lead to sudden death. The etiology of CAA in KD patients is unclear, and this study aims to clarify the relationship between steroid receptor coactivator-1 (SRC-1) gene polymorphisms and CAA pathogenesis. We investigated four SRC-1 gene polymorphisms (rs11894248, rs17791703, rs7572475, and rs9309308) and their correlation with KD with CAA susceptibility in 327 Taiwanese people (279 KD patients without CAA and 48 KD patients with CAA). The results indicated a statistically significant difference in genotype and allele frequency distributions at the SRC-1 4 SNPs between KD patients with and without CAA (p <0.01). Additionally, Smad3 gene polymorphism (rs12901071) is well known to be associated with KD patients. In our results, Smad3 SNP did not provide a statistically significant difference between KD patients with and without CAA. Our data show that SRC-1 polymorphisms may be the underlying cause of CAA; therefore, the polymorphisms examined in this study warrant further investigation.
Keywords: Kawasaki disease (KD), coronary artery aneurysm (CAA), steroid receptor
coactivator-1 (SRC-1) 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38
Introduction
Kawasaki disease (KD) is an acute, self-limited, and systemic vasculitis that is one of the leading inducers of heart disease in children (1-3). KD patients with cardiac complications, particularly those of the coronary artery, are known to suffer frequently from this syndrome, which develops in 15-25% of children diagnosed with KD who remain untreated (4, 5). KD patients with cardiovascular complications are at high risk of developing ischemic heart disease, which can lead to myocardial infarction and sudden death (5). Coronary artery aneurysm (CAA) develop in 25% of untreated patients and 3% to 5% of patients treated with intravenous immunoglobulin (IVIG) within the first 10 days of fever onset (6). The etiology of CAA in KD patients is unclear.
Transforming growth factor (TGF-) is a multifunctional peptide that regulates proliferation, differentiation, apoptosis, and migration in many cell types. TGF- induces transformation of cells of different lineages to myofibroblasts that mediate damage to the arterial wall. TGF- pathway genes, TGFB2, TGFBR2, and Smad3 genetic variants and their haplotypes are associated with KD susceptibility, CAA formation, aortic root dilatation, and intravenous immunoglobulin treatment response in different cohorts (7). Smad3 is a key signaling molecule in the pathway and was associated with both KD susceptibility and formation of CAA (7). The steroid receptor coactivator-1 (SRC-1) is a Smad3/4 transcriptional partner facilitating the functional link between Smad3 and p300/CBP and 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57
enhances TGF- medicated transcription (8). SRC-1 is a transcriptional coactivator and the first identified member of the p160 SRC gene family that includes SRC-2 and SRC-3 (9-11). These transcriptional coactivators interact with nuclear receptors in a ligand-binding dependent manner and recruit general coactivators such as cAMP-responsive element binding protein (CREB) binding protein (CBP) or p300 to the target gene promoter for activation of gene transcription (10, 11). SRC-1 is expressed in ECs, VSMCs, and neointima cells. SRC-1 expression in these cells facilitates estrogen/ER-mediated vasoprotection through the inhibition of neointima after a vascular injury (12).
In the present study, we examined 327 patients with a past history of Kawasaki disease, 48 of whom were Taiwanese children diagnosed with CAA. In a complication study, we investigated whether the identified gene polymorphisms were associated with CAA.
Materials and Methods
Patients and sample collection
We identified and enrolled 327 individuals into this study. All individuals attended the Department of Pediatrics, China Medical University Hospital in Taichung from 1998 to 2011 and fulfilled the diagnostic criteria for KD (13-17). Every patient underwent regular echocardiography examinations, beginning during the acute stage of KD at 2 months and 6 months after disease onset and once a year thereafter. A CAA was identified when either the 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76
right coronary artery or the left coronary artery showed a dilated diameter of 3 mm in children younger than 5 years or of 4 mm in children older than 5 years (18). The normal population was Han Chinese in Beijing (CHB) data from HapMap database (http://hapmap.ncbi.nlm.nih.gov/).
Genomic DNA extraction and genotyping
All blood samples were collected using venipuncture for genomic DNA isolation. Genomic DNA was extracted from peripheral blood leukocytes according to standard protocols (Genomic DNA kit; Qiagen, Valencia, CA, USA). We genotyped 4 SNPs in SRC-1 gene (rs11894248, rs17791703, rs7572475, and rs9309308) and 1 SNP in Smad3 gene (rs12901071). The primers and probes used to detect SNPs were from the ABI Assays-on Demand kit. Reactions were performed according to the manufacturer’s protocol. Briefly, PCR was performed in the presence of 2 TaqMan
Universal PCR Master Mix, assay mix and genomic DNA (15 ng). The probe for
fluorescence signal detection was from the ABI Prism 7900 Real Time PCR System. This study was approved by the Human Studies Committee of China Medical University Hospital, and informed consent was obtained from either the participants or their parents.
Statistical analysis
The allelic and genotype frequency distributions for the polymorphism of KD were determined through χ2 analysis using SPSS software (version 10.0, SPSS Inc. Chicago, 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95
Illinois, US). A P value of less than 0.05 was considered statistically significant. Allelic and genotype frequencies were expressed as percentages of the total number of alleles and genotypes. Odds ratios (OR) were calculated from allelic and genotype frequencies with a 95% confidence interval (95% CI). Adherence to the Hardy-Weinberg equilibrium constant was tested using a χ2 test with one degree of freedom.
Results
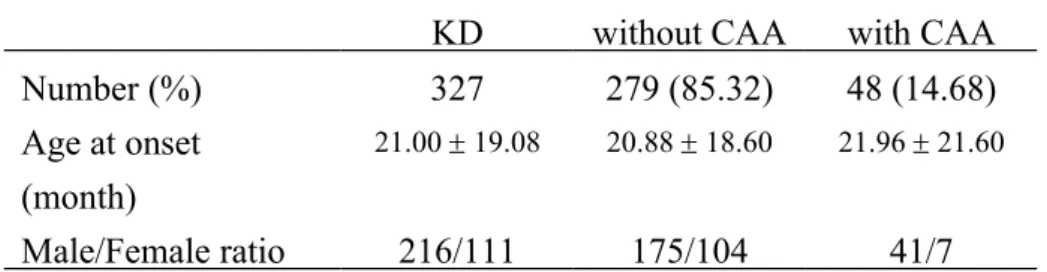
In this study, 327 KD patients, including 216 males and 111 females (Table 1), were analyzed. In total, 279 patients were without CAA (175 males and 104 females) and the mean age of the onset was 20.88 ± 18.60 months. Forty-eight patients suffered from CAA (41 males and 7 females) and the mean age of onset was 21.96 21.60 months. Adjuvant therapy was administered according to individual considerations.
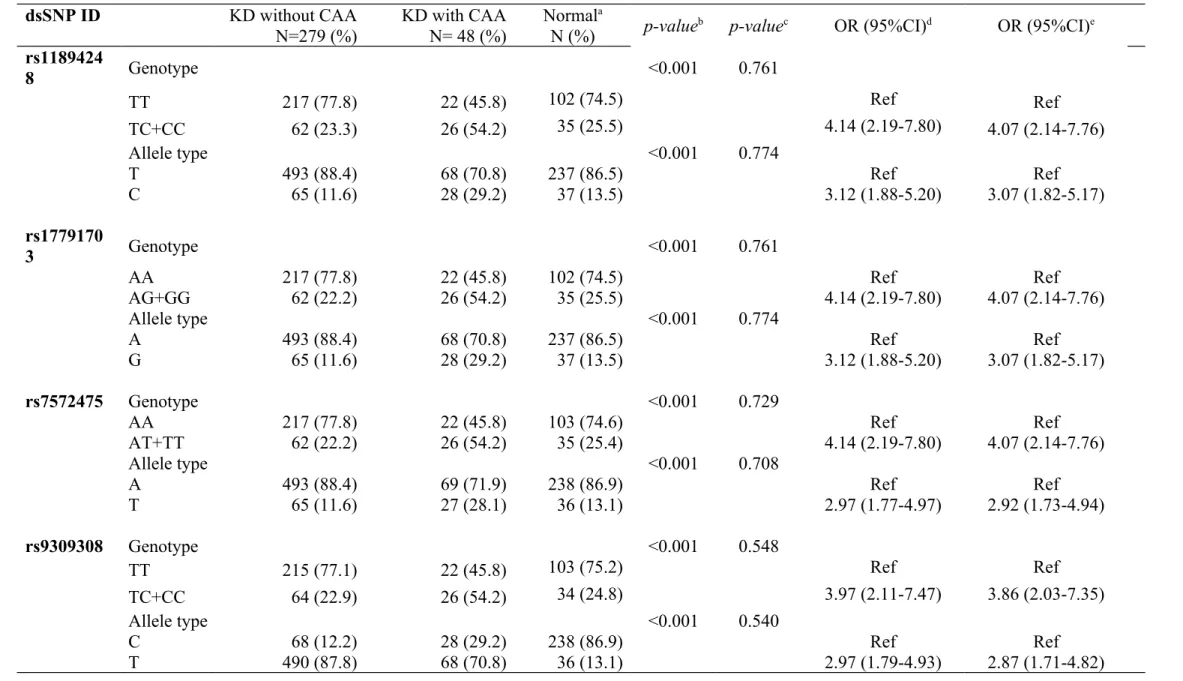
Table 2 plots SRC-1 genotypic and allelic frequencies of rs11894248, rs17791703, rs7572475, and rs9309308, genotype distributions in Hardy-Weinberg equilibrium. We compared the genotype or allele frequencies between KD patients without CAA and with CAA and noted a statistically significant difference in genotype and allele frequencies for rs11894248, rs17791703, rs7572475, and rs9309308 SNPs in KD patients without CAA and with CAA (p < 0.01). In rs11894248, the frequency of the ‘TT’ genotype was lower for KD patients with CAA (45.8%) as compared to the group consisting of KD patients without CAA 96 97 98 99 100 101 102 103 104 105 106 107 108 109 110 111 112 113 114
(77.8%). The frequency of the ‘TC+CC’ genotype was higher in KD patients with CAA (54.2%) than in KD patients without CAA (23.3%). In comparison with the ‘TT’ genotype, the OR of ‘TC+TT’ was 4.14 (95% CI = 2.19-7.80, p <0.001). The allelic frequency of ‘C’ was higher in KD patients with CAA (29.2%) than in KD patients without CAA (11.6%). In comparison to the ‘T’ allele, the OR for the ‘C’ allele was 3.12 (95% CI = 1.88-5.20, p <0.001), the data show statistically significant differences in this comparison. In rs17791703, rs7572475, and rs9309308 SNPs, genotype and allele frequencies also showed statistically significant differences with CAA. Our data indicated that these 4 SRC-1 SNPs may lead to a high risk of development of CAA in KD patients. We also compare KD patients with normal population from HapMap database in SRC-1 SNPs; there were no statistically significant differences in these comparisons. The result of gender comparison also showed no statistically significant differences in this comparison.
Table 3 shows the Smad3 SNP rs12901071 and indicates that the frequency of the ‘TT’ genotype was higher in KD patients with CAA (77.1%) than in KD patients without CAA (66.3%). The frequency of the ‘TC+CC’ genotype was lower in KD patients with CAA (22.9%) than in KD patients without CAA (33.7%). As compared to the ‘TT’ genotype, the OR of ‘TC+CC’ was 0.59 (95% CI = 0.29-1.20, p =0.140). The allelic frequency of ‘C’ was lower in patients with KD patients with CAA (11.5%) than in the KD patients without CAA (18.6%). The OR for the ‘T’ allele was 0.57 (95% CI = 0.29-1.10, p =0.109). The data show 115 116 117 118 119 120 121 122 123 124 125 126 127 128 129 130 131 132 133
non-statistically significant differences in this comparison. We also compare KD patients with normal population from HapMap database in Smad3 SNPs; there was a well-known statistically significant differences in these comparisons. The result of gender comparison also showed no statistically significant differences in this comparison.
Discussion
KD is a systemic vasculitis involving small and medium size blood vessels all over the body, virtually involving the coronaries. Arterial remodeling or revascularization may occur in KD with coronary arteritis. The advancing of stenosis in KD results from active remodeling with proliferation and neoangiogenesis. The growth factors are observably expressed at the aneurysms (19). Although the majority of patients with KD recover without long term consequences, the disorder is associated with vasculitis affecting the coronary arteries and occasionally other muscular arteries, resulting in CAA in over 20% of untreated patients (5, 20). 2%-3% of untreated patients die of coronary artery thrombosis, myocardial infarction, or, rarely, aneurysm rupture. Patients with a large (8 mm or more) CAA are at a long-term risk of developing aneurysm thrombosis or coronary artery stenosis and myocardial infarction, even years after the acute illness (5). In view of the frequency and severity of coronary artery complications, there has been intense interest in treatments to reduce the risk of CAA (21).
TGF- may contribute to aneurysm formation by promoting the generation of 134 135 136 137 138 139 140 141 142 143 144 145 146 147 148 149 150 151 152
myofibroblasts growth factor, which may also be involved in the induction of regulatory T-cells in KD (22). TGFB2, TGFBR2, and Smad3 were found to have a significant association with the susceptibility of KD (7). Genetic polymorphisms in TGF- signaling pathway are associated with KD susceptibility, but not coronary artery lesions formation or intravenous immunoglobulin treatment response in the Taiwanese population (23). We showed SRC-1 gene polymorphism was strongly associated with CAA complication of KD but not Smad3.
SRC-1 interacts with the transcriptional co-activators p300/CBP but not with Smad3 since
SMAD proteins are differentially expressed in target tissues for TGF-, the tissue specific amounts of endogenous SMAD proteins may contribute to the cooperative actions (8, 24). SMAD proteins are differentially expressed in target tissue for TGF-. The tissue-specific amounts of endogenous SMAD proteins may contribute to the cooperative actions (24).
SRC-1 serves as an in vivo co-activator for ER in the blood vessel wall to co-mediate the effect of estrogen on vasoprotection during vascular wall remodeling after an injury. Conversely, SRC-1 down regulation or loss-of-function mutation will reduce or impair the ER function in the vascular wall and thereby enhance the neointima formation in response to a vascular injury (12). Mutant form of SRC-1 lacking the CBP/p300 binding site failed to up-regulate Smad3/4-dependent transcription, while full-length SRC-1 potentiated p300- Smad3 interactions and also triggered the TGF- signaling pathway (8). In early stages of cancer, TGF-β functions as a tumor suppressor because it inhibits proliferation, induces apoptosis, 153 154 155 156 157 158 159 160 161 162 163 164 165 166 167 168 169 170 171
and mediates differentiation. Conversely, in later stages of cancer, TGF-β promotes tumor progression through increasing tumor cell invasion and metastasis. Thus, TGF-β can have opposing roles, likely dependent, in part, on whether the cancer is early or late stage (25).
In conclusion, we have shown that SRC-1 gene polymorphisms susceptible to the development of KD complication of CAA are associated with genetic predisposition in Taiwanese children of Han Chinese ethnic background. Our research also shows that genetic polymorphism in the TGF- signaling pathway, particularly the SRC-1 gene, is associated with susceptibility to CAA as a complication from KD.
Acknowledgments
This work is supported in part by China Medical University (CMU) and China Medical University Hospital (DMR-102-045) in Taiwan. The first author received the fellowship from China Medical University (CMU 101-AWARD-01), Taiwan.
172 173 174 175 176 177 178 179 180 181 182 183 184
References
1. Kawasaki T. Kawasaki disease: a new disease? Acta. Paediatr. Taiwan 2001;42:8-10. 2. Burns JC, Glode MP. Kawasaki syndrome. Lancent 2004;364:533-544.
3. Chang LY, Chang IS, Lu CY, et al. Kawasaki Disease Research, Group. Epidemiologic features of Kawasaki disease in Taiwan, 1996-2002. Pediatrics 2004;114:e678-682.
4. Kato H, Koike S, Yamamoto M, et al. Coronary aneurysms in infants and young children with acute febrile mucocutaneous lymph node syndrome. J Pediatr 1975;86(6):892-898. 5. Kato H, Sugimura T, Akagi T, et al. Long-term consequences of Kawasaki disease. A
10-to 21-year follow-up study of 594 patients. Circulation 1996;94(6):1379-1385.
6. Newburger JW, Takahashi M, Burns JC, et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med 1986;315:341–347.
7. Shimizu C, Jain S, Davila S, et al. Transforming growth factor- signaling pathway in patients with Kawasaki disease. Circ Cardiovasc Genet 2011;4(1):16-25.
8. Dennler S, Pendaries V, Tacheau C, et al. The steroid receptor co-activator-1 (SRC-1) potentiates TGF-/Smad signaling: role of p300/CBP. Oncogene 2005;24:1936-1945. 9. Onate SA, Tsai SY, Tsai MJ, O’Malley BW. Sequence and characterization of a
coactivator for the steroid hormone receptor superfamily. Science 1995;270:1354 –1357 (1995).
10. McKenna NJ, Lanz RB, O’Malley BW. Nuclear receptor coregulators: cellular and molecular biology. Endocr Rev 1999;20:321–344.
185 186 187 188 189 190 191 192 193 194 195 196 197 198 199 200 201 202 203 204
11. Xu J, Li Q. Review of the in vivo functions of the p160 steroid receptor coactivator family. Mol Endocrinol 2003;17:1681–1692.
12. Yuan Y, Xu J. Loss-of-function deletion of the steroid receptor coactivator-1 gene in mice reduces estrogen effect on the vascular injury response. Arterioscler Thromb Vasc Biol 2007;27:1521-1527.
13. Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Pediatrics 2004;114: 1708–1733.
14. Wu SF, Chang JS, Peng CT, Shi YR, Tsai FJ. Polymorphism of angiotensin-1 converting enzyme gene and Kawasaki disease. Pediatr Cardiol 2004;25:529–533.
15. Wu SF, Chang JS, Wan L, Tsai CH, Tsai FJ. Association of IL-1Ra gene polymorphism, but no association of IL-1 and IL-4 gene polymorphisms, with Kawasaki disease. J Clin Lab Anal 2005;19:99-102.
16. Kim S, Dedeoglu F. Update on pediatric vasculitis. Curr Opin Pediatr 2005;17:695–702. 17. Falcini F. Kawasaki disease. Curr Opin Rheumatol 2006;18:33–38.
18. Akagi T, Rose V, Benson LN, Newman A, Freedom RM. Outcome of coronary artery aneurysms after Kawasaki disease. J Pediatr 1992;121:689–694.
19. Suzuki A, Miyagawa-Tomita S, Komatsu K, et al. Active remodeling of the coronary 205 206 207 208 209 210 211 212 213 214 215 216 217 218 219 220 221 222 223
arterial lesions in the late phase of Kawasaki disease: Immunohistochemical study. Circulation 2000;101:2935-2941.
20. Fujiwara H, Hamashima Y. Pathology of the heart in Kawasaki disease. Pediatrics 1978; 61:100–107.
21. Levin M. Steroids for Kawasaki disease: the devil is in the detail. Heart 2013;99(2): 69-70.
22. Shimizu C, Oharaseki T, Takahashi K, Kottek A, Franco A, Burns JC. The role of TGF- and myofibroblasts in the arteritis of Kawasaki disease. Hum Pathol 2013;44(2):189-98. 23. Kuo HC, Onouchi Y, Hsu YW, et al. Polymorphisms of transforming growth factor-
signaling pathway and Kawasaki disease in the Taiwanese population. J Hum Genet 2011; 56(12):840-845.
24. Yanagisawa J, Yanagi Y, Masuhiro Y, et al. Convergence of transforming growth factor- and vitamin D signaling pathways on smad transcriptional coactivators. Science 1999;283: 1317-1321.
25. Smith AL, Robin TP, Ford HL. Molecular pathways: targeting the TGF-β pathway for cancer therapy. Clin Cancer Res 2012;18(17):4514-4521.
225 226 227 228 229 230 231 232 233 234 235 236 237 238 239 240
Table 1. Clinical characteristics of KD patients with CAA and without CAA. KD without CAA with CAA
Number (%) 327 279 (85.32) 48 (14.68) Age at onset (month) 21.00 19.08 20.88 18.60 21.96 21.60 Male/Female ratio 216/111 175/104 41/7 241 242
Table 2. Genotypic and allelic frequencies of SRC-1 genetic polymorphisms in KD patients with and without CAA.
dsSNP ID KD without CAA KD with CAA Normala
p-valueb p-valuec OR (95%CI)d OR (95%CI)e
N=279 (%) N= 48 (%) N (%) rs1189424 8 Genotype <0.001 0.761 TT 217 (77.8) 22 (45.8) 102 (74.5) Ref Ref TC+CC 62 (23.3) 26 (54.2) 35 (25.5) 4.14 (2.19-7.80) 4.07 (2.14-7.76) Allele type <0.001 0.774 T 493 (88.4) 68 (70.8) 237 (86.5) Ref Ref C 65 (11.6) 28 (29.2) 37 (13.5) 3.12 (1.88-5.20) 3.07 (1.82-5.17) rs1779170 3 Genotype <0.001 0.761 AA 217 (77.8) 22 (45.8) 102 (74.5) Ref Ref AG+GG 62 (22.2) 26 (54.2) 35 (25.5) 4.14 (2.19-7.80) 4.07 (2.14-7.76) Allele type <0.001 0.774 A 493 (88.4) 68 (70.8) 237 (86.5) Ref Ref G 65 (11.6) 28 (29.2) 37 (13.5) 3.12 (1.88-5.20) 3.07 (1.82-5.17) rs7572475 Genotype <0.001 0.729 AA 217 (77.8) 22 (45.8) 103 (74.6) Ref Ref AT+TT 62 (22.2) 26 (54.2) 35 (25.4) 4.14 (2.19-7.80) 4.07 (2.14-7.76) Allele type <0.001 0.708 A 493 (88.4) 69 (71.9) 238 (86.9) Ref Ref T 65 (11.6) 27 (28.1) 36 (13.1) 2.97 (1.77-4.97) 2.92 (1.73-4.94) rs9309308 Genotype <0.001 0.548 TT 215 (77.1) 22 (45.8) 103 (75.2) Ref Ref TC+CC 64 (22.9) 26 (54.2) 34 (24.8) 3.97 (2.11-7.47) 3.86 (2.03-7.35) Allele type <0.001 0.540 C 68 (12.2) 28 (29.2) 238 (86.9) Ref Ref T 490 (87.8) 68 (70.8) 36 (13.1) 2.97 (1.79-4.93) 2.87 (1.71-4.82) 243
KD, Kawasaki disease; OR, odds ratio; CI, confidence interval from unconditional logistic regression analysis
a normal population from Han Chinese in Beijing (CHB) (data from HapMap database, http://hapmap.ncbi.nlm.nih.gov/)
b P value from chi-square test; compared KD patients with CAA and without CAA
c P value from chi-square test; compared KD patients with normal population from Han Chinese in Beijing d unadjusted odd ratio
e odd ratio were estimated adjusting for gender
244 245 246 247 248 249 250 251 252 253 254 255 256 257 258 259 260 261 262 263
Table 3. Genotypic and allelic frequencies of Smad3 genetic polymorphism in KD patients with and without CAA.
dsSNP ID KD without
CAA KD with CAA
Normal
p-valuea p-valueb OR (95%CI)d OR (95%CI)e
N=279 (%) N= 48 (%) N (%) rs12901071 Genotype 0.140 0.044 TT 185 (66.3) 37 (77.1) 79 (58.1) Ref Ref TC+CC 94 (33.7) 11 (22.9) 57 (41.9) 0.59 (0.29-1.20) 0.55 (0.26-1.13) Allele type 0.109 0.087 C 104 (18.6) 11 (11.5) 211 (77.6) Ref Ref T 454 (81.4) 85 (88.5) 61 (22.4) 0.57 (0.29-1.10) 0.54 (0.28-1.05)
KD, Kawasaki disease; OR, odds ratio; CI, confidence interval from unconditional logistic regression analysis
a normal population from Han Chinese in Beijing (CHB) (data from HapMap database, http://hapmap.ncbi.nlm.nih.gov/)
b P value from chi-square test; compared KD patients with CAA and without CAA
c P value from chi-square test; compared KD patients with normal population from Han Chinese in Beijing d unadjusted odd ratio
e odd ratio were estimated adjusting for gender
264 265 266 267 268 269 270 271 272 273 274 275