Urinary arsenic profile affects the risk of urothelial carcinoma
even at low arsenic exposure
☆
Yeong-Shiau Pu
a, Shu-Mei Yang
b, Yung-Kai Huang
c, Chi-Jung Chung
b, Steven K. Huang
c,d,
Allen Wen-Hsiang Chiu
d,e, Mo-Hsiung Yang
f, Chien-Jen Chen
g, Yu-Mei Hsueh
h,⁎
aDepartment of Urology, National Taiwan University College of Medicine, Taipei, Taiwan bGraduate Institute of Public Health, Taipei Medical University, Taipei, Taiwan cGraduate Institute of Medical Sciences, Taipei Medical University, Taipei, Taiwan
dDepartment of Urology, Chi-Mei Medical Center, Tainan, Taiwan e
Department of Urology, Taipei City Hospital, Taipei, Taiwan
f
Department of Nuclear Science, National Tsing-Hua University, Hsinchu, Taiwan
g
Graduate Institute of Epidemiology, College of Public Health, National Taiwan University, Taipei, Taiwan
h
Department of Public Health, School of Medicine, Taipei Medical University, Taipei, No. 250 Wu-Hsing Street, Taipei 110, Taiwan Received 13 July 2006; revised 22 September 2006; accepted 23 September 2006
Available online 10 November 2006
Abstract
Arsenic exposure is associated with an increased risk of urothelial carcinoma (UC). To explore the association between individual risk and
urinary arsenic profile in subjects without evident exposure, 177 UC cases and 313 age-matched controls were recruited between September 2002
and May 2004 for a case–control study. Urinary arsenic species including the following three categories, inorganic arsenic (As
III+ As
V),
monomethylarsonic acid (MMA
V) and dimethylarsinic acid (DMA
V), were determined with high-performance liquid chromatography-linked
hydride generator and atomic absorption spectrometry. Arsenic methylation profile was assessed by percentages of various arsenic species in the
sum of the three categories measured. The primary methylation index (PMI) was defined as the ratio between MMA
Vand inorganic arsenic.
Secondary methylation index (SMI) was determined as the ratio between DMA
Vand MMA
V. Smoking is associated with a significant risk of UC
in a dose-dependent manner. After multivariate adjustment, UC cases had a significantly higher sum of all the urinary species measured, higher
percent MMA
V, lower percent DMA
V, higher PMI and lower SMI values compared with controls. Smoking interacts with the urinary arsenic
profile in modifying the UC risk. Differential carcinogenic effects of the urinary arsenic profile, however, were seen more prominently in
non-smokers than in non-smokers, suggesting that smoking is not the only major environmental source of arsenic contamination since the UC risk differs in
non-smokers. Subjects who have an unfavorable urinary arsenic profile have an increased UC risk even at low exposure levels.
© 2006 Published by Elsevier Inc.
Keywords: Bladder neoplasms; Contamination; Carcinogenesis; Synergy; Tobacco
Introduction
Urothelial carcinoma (UC) arises exclusively from the
urothelium including the renal pelvis, ureter, bladder and
urethra, with bladder cancer being the most common form. In
most developed countries, it is among the top 10 leading
cancers. The most well known risk factor for UC is cigarette
smoking (
Brennan et al., 2000; Zeegers et al., 2000
). Current
cigarette smokers have approximately a two- to three-fold risk
compared to non-smokers. The mechanism by which cigarette
smoking causes bladder cancer has yet to be determined. It
seems likely that the risk is related to a large number of
carcinogenic chemicals in cigarette smoke.
We have previously shown that chronic arsenic intoxication
due to contamination of artesian well water with inorganic
arsenic compounds is responsible for elevated mortality rates
☆ Grant support: NSC91-3112-B-038-0019, NSC92-3112-B-038-001,NSC93-3112-B-038-001, NSC94-2314-B-038-023 and NSC95-2314-B-038-007 from the National Science Council, Executive Yuan, ROC.
⁎ Corresponding author. Fax: +886 2 27384831. E-mail address:[email protected](Y.-M. Hsueh). 0041-008X/$ - see front matter © 2006 Published by Elsevier Inc. doi:10.1016/j.taap.2006.09.021
from cancers of the bladder, renal pelvis and/or ureter, lung and
other organs in Taiwan (
Chen et al., 1985
). More specifically,
we have demonstrated that bladder cancer mortality rates for
patients who consumed well water with arsenic levels of
600
μg/L or higher had a mortality rate of over 30 to 60 times
greater than the unexposed population (
Chen et al., 1988
).
Evidence from elsewhere in the world also suggests that
ingested inorganic arsenic very likely causes internal cancers
(
Morales et al., 2000; Bates et al., 2004; Smith et al., 2006
). It
has also been shown that combined cancer mortality rates are as
high as 1 out of 100 people from drinking water containing
50
μg/L of arsenic (
Smith et al., 1992
). Two reports from the
National Research Council (USA) have also affirmed that
cancer risks might be of the order of 1 in 100 at an arsenic level
of 50
μg/L (
National Research Council, 1999, 2001
). This
estimated cancer risk is more than 100 times greater than that for
any other contaminant in drinking water at the maximal
contaminant level (
US EPA, 1998
). Thus, within the U.S., the
maximum contaminant level for arsenic in public water supplies
will be lowered from 50
μg/L, a level that was established in
1942, to 10
μg/L in 2006 (
Smith et al., 2002
). The arsenic
concentration allowance in public water supplies in Taiwan was
50
μg/L; in 2000, a new standard of 10 μg/L was then
announced. According to the Taipei Water Department of Taipei
City Government, the average arsenic concentration of tap
water in Taipei is 0.7
μg/L ranging from non-detectable to
4.0
μg/L. Whether cancer risks are higher at 50 μg/L than at
10
μg/L is still debatable. Even without confounding factors,
reduction of cancer risks with the new standard of 10
μg/L will
not be seen for decades. However, should it be shown that
arsenic metabolic capability affects cancer risks in subjects
exposed 50
μg/L of arsenic, it might still be carcinogenic for
some genetically predisposed subjects.
Arsenic is usually found in drinking water in the form of
arsenate (As
V) or arsenite (As
III) (
Andreae, 1977
). Inorganic
arsenic is bio-transformed in humans to monomethylarsonic
acid (MMA
V) and dimethylarsinic acid (DMA
V). Previously,
methylation of inorganic arsenic has always been considered a
detoxification mechanism because pentavalent MMA (MMA
V)
and pentavalent DMA (DMA
V) have relatively low toxicity
(
Yamauchi and Fowler, 1994
) and are rapidly excreted in the
urine (
Vahter, 2002
). However, recent studies have confirmed
the existence of trivalent intermediates and products of
monomethylarsonous acid (MMA
III) and dimethylarsinous
acid (DMA
III) that are more toxic than inorganic arsenite
(
Thomas et al., 2001; Mass et al., 2001; Styblo et al., 2002
). For a
more accurate assessment of arsenic metabolism, it is therefore
necessary to determine specific arsenic species in urine.
The capability of metabolizing inorganic arsenic differs
among individuals. We have previously shown that the
capability of arsenic methylation is related to the risks of skin
cancer (
Hsueh et al., 1997; Chen et al., 2003a
) and bladder
cancer in high arsenic-exposed subjects (
Chen et al., 2003b
).
Whether or not urinary arsenic profile affects UC risks among
subjects who had no evident arsenic exposure history is an
important issue. We hypothesized that, if an arsenic level of
50
μg/L in the water supply is still “unsafe”, the UC risk may
significantly differ between people with favorable and
unfavor-able arsenic methylation profile. We therefore conducted a
hospital-based case–control study to investigate the association
of urinary arsenic profile with the risk of UC. The possible
interactions between urinary arsenic profile and cigarette
smoking were also explored.
Material and methods
Study subjects and questionnaire interview. One hundred and seventy-seven patients with pathologically proven UC (age range 24 to 93 years) were recruited from the Department of Urology, National Taiwan University Hospital, between September 2002 and May 2004. Pathological verification of UC was done by routine urological practice including endoscopic biopsy or surgical resection of urinary tract tumors followed by histopathological examination by board-certified pathologists. Cytological evidence alone was not accepted as an adequate diagnosis of UC. A total of 313 age-matched control subjects with no evidence of UC or any other malignancy were accrued from a hospital-based pool, including those receiving senior citizen health examinations at Taipei Medical University Hospital and those receiving adult health examinations at Taipei Municipal Wan Fang Hospital. All three hospitals are located in Taipei approximately 200 to 300 km away from the contaminated areas in Taiwan. No case subjects or controls came from arsenic-contaminated areas in southwestern (Chen et al., 2003b) or northeastern (Chiou et al., 2001) Taiwan.
Well-trained personnel carried out standardized personal interviews based on a structured questionnaire. Information collected included demographic and socioeconomic characteristics, general potential risk factors for malignancies such as lifestyle, alcohol consumption, cigarette smoking in quantified details, exposure to potential occupational and environmental carcinogens such as hair dyes and pesticides, chronic medication history, consumption of conventional and alternative medicines and personal and family history of urological diseases. Frequent alcohol drinkers referred to those who consumed alcohol three or more days per week, continuing for at least 6 months. Those who consumed less than this level were classified as occasional drinkers. Pesticide users were farmers who used pesticides for agricultural purposes. The Research Ethics Committee of National Taiwan University Hospital, Taipei, Taiwan, approved the study. All patients provided informed consent forms before sample and data collection. The study was consistent with the World Medical Association Declaration of Helsinki. Urine samples were stored at−20°C until further use for urinary arsenic speciation. Bladder cancer was staged into three groups: superficial (Ta, T1 and Tis), locally advanced (T2–4N0M0) and metastatic (N+ or M+). Tumor grading was based on the WHO (1999)
classification system (WHO, 1999).
Determination of urinary arsenic species. It has been shown that urinary arsenic species is stable for at least 6 months when preserved at−20°C (Chen et al., 2002); thus, the urine assay was performed within 6 months post-collection. Frozen urine samples were thawed at room temperature, dispersed by ultrasonic wave, filtered through a Sep-Pak C18column (Mallinckrodt Baker In., NJ) and
levels for AsIII, AsV, MMAVand DMAVwere determined. A urine aliquot of 200μL was used for the determination of arsenic species by high-performance liquid chromatography (HPLC) (Waters 501, Waters Associates, MA) with columns obtained from Phenomenex (Nucleosil, Torrance, CA). The contents of inorganic arsenic and their metabolites were quantified by hydride generator-atomic absorption spectrometry (HG-AAS) (Hsueh et al., 1998). The concentration of four arsenic species in standard solution, sample and sample spiked standard solution was determined by using on-line HPLC-HG-AAS respectively. Recovery rates of the four arsenic species were calculated by [(sample spiked standard solution concentration)−sample concentration]/ standard solution concentration × 100 respectively. Recovery rates for AsIII,
DMAV, MMAVand AsVranged between 93.8% and 102.2% with detection
limits of 0.02, 0.06, 0.07 and 0.10μg/L, respectively. Urinary concentration of the sum of inorganic arsenic, MMA and DMA was normalized against urinary creatinine levels (μg/g creatinine). The standard reference material, SRM 2670, contains 480 ± 100μg/L inorganic arsenic and was obtained from the National
Institute of Standards and Technology (NIST, Gaithersburg, MD). SRM 2670 was used as a quality standard and analyzed along with urine samples. The mean value of SRM 2670 determined by our system was 507 ± 17 (SD)μg/L (n=4). Arsenic methylation index was assessed by percentages of various urinary arsenic species in the sum of inorganic arsenic, MMA and DMA. The primary methylation index (PMI) was defined as the ratio between MMAVand inorganic arsenic (AsIII+ AsV) levels and the secondary methylation index (SMI) was defined as the ratio between DMAVand MMAV(Tseng et al., 2005).
Statistical analysis. Continuous variables are expressed as mean ± standard error. Student's t-test was used to compare differences in the urinary arsenic profile between case subjects and controls. ANOVA and Student–Newman– Keuls multiple comparison correction was applied to compare urinary arsenic profiles between varied exposure strata. Multiple logistic regression models were used to estimate the multivariate adjusted odds ratio (OR) and the 95% confidence interval (CI). Cutoff points for continuous variables were the respective tertiles of the controls. Significance tests for linear trend among ORs across exposure strata were calculated by categorizing exposure variables and treating scored variables as continuous. For the joint effect analysis, the cutoff points for the percentages of arsenic species, PMI and SMI were the respective medians of the controls. The joint effects of urinary arsenic species and cigarette
smoking on the UC risk were evaluated on both multiplicative and additive scales. The binary interaction terms were calculated by multiplying the indicators for two explored risk factors and were added to the main effect models. Their significance was then tested by the likelihood ratio statistic based on a multiplicative model. The synergy index proposed by Rothman was computed to assess the empirical deviation from the additive interaction relationship (Rothman, 1986). The synergy index is equal to the calculation of [OR(AB)− 1] / [(OR(Ab) −1) +(OR(aB) −1)], where A and B denote the presence of the two risk factors and a and b are designated as the absence of the risk factors, respectively. An observed synergy index value that departs substantially from the expected additive null, i.e., synergy index not equal to 1, suggests an additive interaction effect. The OR values and their variance covariance matrix were then used to calculate values for synergy index and 95% CIs (Hosmer and Lemeshow, 1992). SAS version 8.2 was used for all statistical analyses.
Results
The sociodemographic characteristics of cases and controls
are shown in
Table 1
. Subjects who had higher educational
levels had a lower risk than those with lower educational levels.
Mainland Chinese had a significantly lower UC risk than the
Fukien Taiwanese. Age, ABO blood type, marital status or use
of hair dye did not affect the UC risk. Occasional alcohol
drinkers had a significantly lower UC risk than non-drinkers
and frequent drinkers. Pesticide users had a significantly higher
UC risk than non-users.
Comparing cases and controls in terms of smoking duration,
daily smoking amount and cumulative smoking in pack-years,
Table 1
Sociodemographic characteristics of 177 urothelial carcinoma cases and 313 age-matched non-cancer controls
Variables Groups Controls n (%)
UC cases n (%)
Age and gender adjusted OR (95% CI) Gender Male 201 (64.2) 124 (70.1) 1.0 Female 112 (35.8) 53 (29.9) 0.8 (0.5–1.1)a Total 313 (100) 177 (100) Age (years) 64.4 ± 0.7 63.9 ± 0.9 0.9 (0.9–1.0)b Blood type A 80 (28.0) 47 (29.0) 1.0 B 57 (19.9) 37 (22.8) 1.1 (0.6–1.9) O 133 (46.5) 64 (39.5) 0.8 (0.5–1.3) AB 16 (6.6) 14 (8.7) 1.6 (0.7–3.7) Not available 27 15
Marital status Single 16 (6.3) 13 (7.3) 1.0 Married 237 (75.6) 139 (78.5) 0.8 (0.4–1.7) Divorced 14 (4.4) 6 (3.4) 0.6 (0.2–2.0) Widowed 46 (13.7) 19 (10.7) 0.6 (0.2–1.7) Ptrend= 0.35 Educational level Elementary school or below 83 (26.7) 73 (41.3) 1.0 High school 105 (33.8) 65 (36.7) 0.6 (0.4–0.9) College or above 123 (39.5) 39 (22.0) 0.3 (0.2–0.4) Ptrend< 0.0001 Paternal ethnicity Fukien Taiwanese 177 (56.5) 147 (73.1) 1.0 Hakka Taiwanese 28 (9.0) 19 (9.5) 8 (0.4–1.5) Mainland Chinese 108 (34.5) 35 (17.4) 0.4 (0.2–0.6) Ptrend< 0.0001 Maternal ethnicity Fukien Taiwanese 180 (57.5) 31 (17.6) 1.0 Hakka Taiwanese 28 (9.0) 15 (8.5) 0.8 (0.4–1.5) Mainland Chinese 103 (32.9) 35 (17.5) 0.4 (0.3–0.7) Not available 2 (0.6) 0 (0.0) Ptrend= 0.0001 Alcohol drinking Never 164 (52.4) 107 (60.5) 1.0 Frequent 52 (16.6) 41 (23.1) 1.0 (0.6–1.7) Occasional 97 (31.0) 29 (16.4) 0.4 (0.2–0.7) Ptrend= 0.0006 Hair dye usage No 188 (60.7) 122 (68.9) 1.0 Yes 122 (39.3) 55 (31.1) 0.7 (0.5–1.1) Pesticide usage No 299 (95.8) 150 (85.2) 1.0 Yes 13 (4.2) 26 (14.8) 4.0 (2.0–8.0) a
Age-adjusted odds ratio by logistic regression.
b
Gender-adjusted odds ratio by logistic regression.
Table 2
Comparison of detailed smoking behavior between cases and controlsa Variables Controls n (%) UC cases
n (%) Age and gender adjusted OR (95% CI) Multivariate adjusted ORb (95% CI) Non-smoker 196 (62.6) 85 (48.0) 1.0 1.0 Former smoker 66 (21.1) 65 (36.7) 2.6 (1.5–4.3) 2.6 (1.5–4.7) Current smoker 51 (16.3) 27 (15.3) 1.3 (0.7–2.3) 1.3 (0.6–2.5) Duration of cigarette smoking (years)
0 196 (65.1) 86 (51.5) 1.0 1.0 0.1–33 50 (16.6) 34 (20.4) 1.4 (0.8–2.6) 1.4 (0.7–2.7) > 33 55 (18.3) 47 (28.1) 2.2 (1.3–3.9) 2.4 (1.2–4.6) Ptrend= 0.005 Ptrend= 0.01
Amount of cigarette smoking (pack/day)
0 196 (65.1) 86 (51.5) 1.0 1.0 0.1–0.75 49 (16.3) 23 (13.8) 1.0 (0.6–2.0) 1.5 (0.8–3.0) > 0.75 56 (18.6) 58 (34.7) 2.5 (1.5–4.3) 2.2 (1.2–4.2) Ptrend= 0.0007 Ptrend= 0.01
Cumulative cigarette smoking (pack-years)c
0 196 (65.1) 85 (50.9) 1.0 1.0 0.1–22 49 (16.3) 28 (16.8) 1.4 (0.7–2.5) 1.1 (0.6–2.3) > 22 56 (18.6) 54 (34.7) 2.4 (1.4–4.0) 2.5 (1.3–4.7) Ptrend= 0.002 Ptrend= 0.004 a Detailed quantified smoking history was unavailable in twelve (3.8%)
controls and ten (5.6%) case subjects.
b Multivariate adjusted ORs: adjusted for age, gender, education, paternal and
maternal ethnicity, alcohol drinking and pesticide usage.
c
cigarette smokers had a significantly higher UC risk than
non-smokers in a dose-dependent manner (
Table 2
). Heavy smokers
who smoked for more than 33 years, 0.75 packs per day and 22
pack-years had a 2.4-, 2.2- and 2.5-fold risk, respectively,
compared to non-smokers by multivariate adjusted logistic
regression. Modest dose smokers, however, did not have a
significantly increased risk compared to non-smokers.
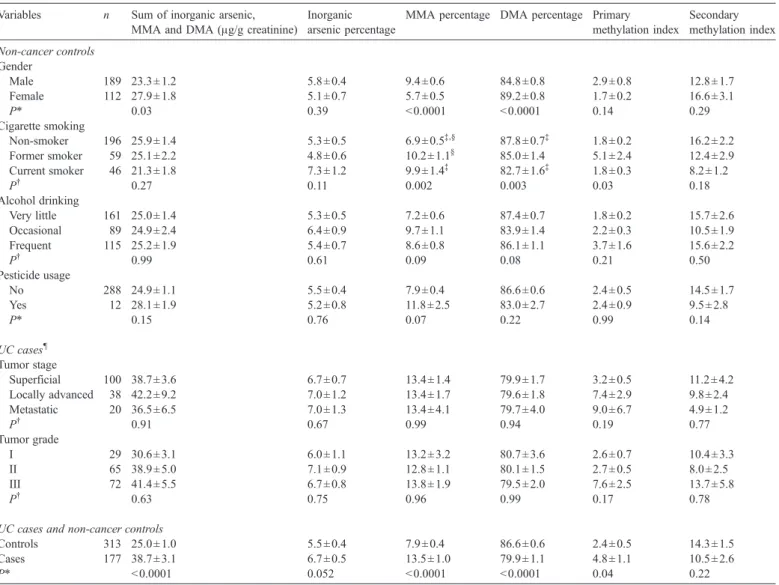
Table 3
compares the urinary arsenic profile between
varied exposure strata. Among non-cancer controls, male
subjects had a lower sum of inorganic arsenic, MMA and
DMA level, higher MMA percentage and lower DMA
percentage than females. Current smokers had a higher
MMA percentage and lower DMA percentage than
non-smokers. No significant differences were found in urinary
arsenic profiles between subjects consuming varied amount of
alcohol. Pesticide users had an insignificantly higher MMA
percentage than non-users.
UC cases had a significantly higher sum of inorganic arsenic,
MMA and DMA levels, higher MMA percentages, lower DMA
percentages and higher PMI levels than controls (
Table 3
).
Inorganic arsenic percentage was marginally higher in cases
than in controls (P = 0.052). To examine if various cancer stages
affect urinary arsenic profile, we performed an analysis showed
that urinary arsenic profile did not differ between patients of
various tumor stages or grades in case subjects (
Table 3
). With
trend analysis on exposure strata in tertiles, all urinary arsenic
parameters, with the exception of inorganic arsenic percentage,
were found to be significantly associated with the UC risk after
the multivariate analysis (
Table 4
).
Since both smoking and urinary arsenic indices affect the UC
risk, further analyses were carried out to assess joint effects of
the two risk factors (
Table 5
). Trend analysis revealed
progressively increased risks through exposure to no risk factor,
either one of the factors, or both of the two risk factors.
Table 3
Comparison of urinary arsenic species between varied exposure strata Variables n Sum of inorganic arsenic,
MMA and DMA (μg/g creatinine)
Inorganic arsenic percentage
MMA percentage DMA percentage Primary methylation index Secondary methylation index Non-cancer controls Gender Male 189 23.3 ± 1.2 5.8 ± 0.4 9.4 ± 0.6 84.8 ± 0.8 2.9 ± 0.8 12.8 ± 1.7 Female 112 27.9 ± 1.8 5.1 ± 0.7 5.7 ± 0.5 89.2 ± 0.8 1.7 ± 0.2 16.6 ± 3.1 P* 0.03 0.39 < 0.0001 < 0.0001 0.14 0.29 Cigarette smoking Non-smoker 196 25.9 ± 1.4 5.3 ± 0.5 6.9 ± 0.5‡,§ 87.8 ± 0.7‡ 1.8 ± 0.2 16.2 ± 2.2 Former smoker 59 25.1 ± 2.2 4.8 ± 0.6 10.2 ± 1.1§ 85.0 ± 1.4 5.1 ± 2.4 12.4 ± 2.9 Current smoker 46 21.3 ± 1.8 7.3 ± 1.2 9.9 ± 1.4‡ 82.7 ± 1.6‡ 1.8 ± 0.3 8.2 ± 1.2 P† 0.27 0.11 0.002 0.003 0.03 0.18 Alcohol drinking Very little 161 25.0 ± 1.4 5.3 ± 0.5 7.2 ± 0.6 87.4 ± 0.7 1.8 ± 0.2 15.7 ± 2.6 Occasional 89 24.9 ± 2.4 6.4 ± 0.9 9.7 ± 1.1 83.9 ± 1.4 2.2 ± 0.3 10.5 ± 1.9 Frequent 115 25.2 ± 1.9 5.4 ± 0.7 8.6 ± 0.8 86.1 ± 1.1 3.7 ± 1.6 15.6 ± 2.2 P† 0.99 0.61 0.09 0.08 0.21 0.50 Pesticide usage No 288 24.9 ± 1.1 5.5 ± 0.4 7.9 ± 0.4 86.6 ± 0.6 2.4 ± 0.5 14.5 ± 1.7 Yes 12 28.1 ± 1.9 5.2 ± 0.8 11.8 ± 2.5 83.0 ± 2.7 2.4 ± 0.9 9.5 ± 2.8 P* 0.15 0.76 0.07 0.22 0.99 0.14 UC cases¶ Tumor stage Superficial 100 38.7 ± 3.6 6.7 ± 0.7 13.4 ± 1.4 79.9 ± 1.7 3.2 ± 0.5 11.2 ± 4.2 Locally advanced 38 42.2 ± 9.2 7.0 ± 1.2 13.4 ± 1.7 79.6 ± 1.8 7.4 ± 2.9 9.8 ± 2.4 Metastatic 20 36.5 ± 6.5 7.0 ± 1.3 13.4 ± 4.1 79.7 ± 4.0 9.0 ± 6.7 4.9 ± 1.2 P† 0.91 0.67 0.99 0.94 0.19 0.77 Tumor grade I 29 30.6 ± 3.1 6.0 ± 1.1 13.2 ± 3.2 80.7 ± 3.6 2.6 ± 0.7 10.4 ± 3.3 II 65 38.9 ± 5.0 7.1 ± 0.9 12.8 ± 1.1 80.1 ± 1.5 2.7 ± 0.5 8.0 ± 2.5 III 72 41.4 ± 5.5 6.7 ± 0.8 13.8 ± 1.9 79.5 ± 2.0 7.6 ± 2.5 13.7 ± 5.8 P† 0.63 0.75 0.96 0.99 0.17 0.78
UC cases and non-cancer controls
Controls 313 25.0 ± 1.0 5.5 ± 0.4 7.9 ± 0.4 86.6 ± 0.6 2.4 ± 0.5 14.3 ± 1.5 Cases 177 38.7 ± 3.1 6.7 ± 0.5 13.5 ± 1.0 79.9 ± 1.1 4.8 ± 1.1 10.5 ± 2.6 P* < 0.0001 0.052 < 0.0001 < 0.0001 0.04 0.22 *Student's t-test. †ANOVA. ‡,§
P < 0.05 by Student–Newman–Keuls multiple comparisons.
¶
Although cigarette smoking tended to interact additively with
urinary arsenic species in modifying the UC risk, the
interactions were all statistically insignificant as shown by the
absence of a substantial deviation from 1 in the synergy index.
Likelihood ratio tests, however, revealed that smoking effects
interact synergistically with PMI (P = 0.003).
Since both PMI and SMI levels were associated with an
altered UC risk, they were jointly analyzed. Subjects with a
PMI
≤1.1 and an SMI >8.2 served as the referent group. A
significant trend of progressively increased risks was observed
in subjects who had none, either one, or both of the two
unfavorable indices (
Table 6
). More specifically, subjects with
both high PMI and low SMI were associated with a
significantly increased risk compared to the referent group
by logistic regression analysis. Interestingly, the association
was statistically significant in both non-smokers and smokers.
The UC risk in non-smokers who had a high PMI and a low
SMI was 6.6-fold higher (95% CI 2.5–17.4) than that of the
referent group.
Discussion
Our data are consistent with other published reports that
smoking is associated with an increased risk of UC in a
dose-dependent manner (
Zeegers et al., 2004
). Of particular note,
our data showed that those who were medium-dose smokers
had an insignificantly elevated risk compared to non-smokers.
Only those who were heavy smokers had a significantly
increased risk compared to non-smokers. It has been reported
that exposure to certain carcinogens in cigarette smoke may
contribute to DNA damage, including DNA adducts from
arylamines (
Vineis et al., 1996
). The mechanism of arsenic
intoxication also involves the formation of DNA adducts
(
Tezuka et al., 1993
) and DNA damage (
Schwerdtle et al.,
2003b
). The additive and even synergistic interaction between
the two risk factors may be a consequence of shared
mechanisms of intoxication. Indeed, the following factors
have been reported and may explain the synergistic
carcino-genic effects observed between benzo(a)pyrene, major
compo-nent of cigarette smoking and arseniasis: (1) both benzo(a)
pyrene and arsenic co-treatment increase benzo(a)pyrene DNA
adducts (
Evans et al., 2004
); (2) arsenite and MMA
IIIincrease
benzoapyrene-7,8-diol,9,10-expoxide (BPDE)-DNA adduct
formation and diminish repair (
Schwerdtle et al., 2003a
); (3)
arsenite inhibits DNA adduct excision induced by different
DNA-damaging agents (
Chien et al., 2004
); and (4) arsenic
inhibits the repair of DNA damage induced by benzo(a)pyrene
(
Tran et al., 2002
).
A recent study showed that mortality from bladder cancer
declined gradually after improving the supply system of
drinking water in southwest Taiwan to eliminate arsenic
exposure from artesian well water (
Yang et al., 2005
). This
finding substantiates the association between arsenic exposure
and bladder cancer risk. A former study evaluating the
association between inorganic arsenic and UC risk focused on
the estimated total arsenic ingested from drinking water
(
Chiou et al., 2001
). It would be more relevant if the
proportion of urinary arsenic species was used as an indicator
of arsenic metabolism. In the study, we demonstrated that
urinary arsenic profile indices are significantly associated with
the risk of UC. A higher PMI and lower SMI indicate
accumulation of MMA by an increased upstream input and
reduced downstream output of the arsenic methylation
pathway. Recently, MMA
IIIand DMA
IIIhave been identified
in human urine (
Le et al., 2000; Mandal et al., 2001
). Many
studies have demonstrated that these trivalent methylated
arsenic species are more toxic than the inorganic compounds
(
Petrick et al., 2000; Mass et al., 2001
). In addition, MMA
IIIis a potent and irreversible inhibitor of thioredoxin reductase
(
Lin et al., 2001
) that regulates cellular response to oxidative
stress in rat hepatocytes. However, the trivalent methylated
arsenic metabolites are not stable. Whether they can be
detected or not depends on the conditions and temperature of
sample storage and concentrations in the urine. The reason
why we did not observe any trivalent methylated metabolites
in the study is that the analytical method used lacks the
requisite specificity. In general, arsenic methylation is
Table 4
Urinary arsenic profiles of 177 UC patients and 313 non-cancer controls Variables Controls
n (%)
UC cases n (%)
Age and gender adjusted OR (95% CI)
Multivariate adjusted ORa
(95% CI) Sum of inorganic arsenic, MMA and DMA (μg/g creatinine)
≤15.4 104 (33.2) 24 (13.6) 1.0 1.0 15.5–26.4 104 (33.2) 44 (24.8) 1.9 (1.1–3.4) 1.6 (0.8–3.0) > 26.4 105 (33.6) 109 (61.6) 5.3 (3.1–9.0) 3.2 (1.8–5.9) Ptrend< 0.0001 Ptrend< 0.0001
Inorganic arsenic percentage
≤2.4 93 (29.7) 40 (22.6) 1.0 1.0 2.5–5.2 113 (36.1) 56 (31.6) 1.2 (0.7–1.9) 1.6 (0.9–2.7) > 5.2 107 (34.2) 81 (45.8) 1.7 (1.1–2.7) 1.2 (0.7–2.0) Ptrend= 0.024 Ptrend= 0.70 MMA percentage ≤3.0 89 (28.4) 37 (20.9) 1.0 1.0 3.1–9.2 111 (35.5) 36 (20.3) 0.8 (0.4–1.3) 0.9 (0.5–1.9) > 9.2 113 (36.1) 104 (58.8) 2.2 (1.3–3.5) 2.8 (1.6–4.8) Ptrend= 0.0002 Ptrend< 0.0001 DMA percentage ≤85.0 114 (36.4) 105 (59.3) 1.0 1.0 85.1–92.5 102 (32.6) 44 (24.9) 0.5 (0.3–0.7) 0.6 (0.4–0.9) > 92.5 97 (31.0) 28 (15.8) 0.3 (0.2–0.5) 0.4 (0.2–0.7) Ptrend< 0.0001 Ptrend= 0.0004
Primary methylation index
≤0.3 91 (29.1) 42 (23.7) 1.0 1.0 0.4–2.0 113 (36.1) 53 (29.9) 1.0 (0.6–1.6) 1.3 (0.7–2.2) > 2.0 109 (34.8) 82 (46.4) 1.6 (1.0–2.6) 3.1 (1.7–5.6) Ptrend= 0.029 Ptrend< 0.0001
Secondary methylation index
≤4.8 98 (31.3) 84 (47.5) 1.0 1.0 4.9–12.7 111 (35.5) 70 (39.5) 0.7 (0.5–1.1) 0.9 (0.5–1.4) > 12.7 104 (33.2) 23 (13.0) 0.3 (0.2–0.4) 0.3 (0.2–0.6) Ptrend< 0.0001 Ptrend= 0.001 a
Multivariate adjusted OR: adjusted for age, gender, education, father and mother ethnicity, alcohol drinking, and pesticide usage.
considered a detoxification process where MMA
Vand DMA
Vare generally considered non-toxic. In fact, inhibition of the
secondary methylation process, resulting in higher MMA
Vand
lower DMA
Vpercentages in the urine, has been reported to
be associated with an increased risk of skin cancers in Mexico
(
Hopenhayn-Rich et al., 1996
). In summary, DMA is the end
methylation and detoxification product. UC cases have lower
DMA percentages and lower SMI, suggesting weaker
detoxification capabilities that lead to a higher cancer risk.
Seaweed contains appreciable amounts of arsenosugars.
Consuming arsenosugars present in seaweed (
Ma and Le, 1998
)
or synthetic forms of arsenosugars (
Francesconi et al., 2002
)
may increase urinary DMA concentration. Our previous study,
however, has shown that the frequencies of fish, shellfish and
seaweed intake do not significantly correlate with urinary
arsenic species in Taipei residents (
Hsueh et al., 2002
). In
addition, a study based on people living in southwestern Taiwan
revealed that there were no increases in urinary inorganic
arsenic, MMA
Vor DMA
Vlevels in subjects who ate seafood
(
Lin, 1986
). This evidence suggests that seafood or seaweed
intake does not influence urinary arsenic profiles in our
population.
All our cases and controls were intentionally recruited
from geographical regions away from the two
arsenic-contaminated areas in Taiwan. Thus, the exposure levels
should be fairly low in both cases and controls. The sum of
Table 5
Interaction between urinary arsenic indices and cigarette smokinga
Variables n of controls/UC
cases
Age and gender adjusted OR (95% CI)
Synergy index (95% CI) Likelihood ratio test Cigarette smoking Sum of inorganic arsenic,
MMA and DMA (μg/g creatinine)
No ≤20.3 95/17 1.0 1.35 (0.70–2.66) Estimated OR 0.83 χ2 0.021; P = 0.88 No > 20.3 101/68 4.4 (2.3–8.5) Yes ≤20.3 56/21 2.9 (1.3–6.5) Yes > 20.3 49/61 8.2 (3.8–17.8) Ptrend< 0.0001
Cigarette smoking Inorganic arsenic percentage
No ≤3.7 99/39 1.0 1.21 (0.36–4.05) Estimated OR 1.01 χ2 0.038; P = 0.84 No > 3.7 97/46 1.1 (0.7–1.9) Yes ≤3.7 44/27 2.0 (1.0–4.3) Yes > 3.7 61/55 2.4 (1.3–4.7) Ptrend= 0.007
Cigarette smoking MMA percentage
No ≤6.1 105/25 1.0 0.86 (0.42–1.77) Estimated OR 0.96 χ23.34; P = 0.07 No > 6.1 34/20 3.3 (1.4–7.6) Yes ≤6.1 34/20 3.3 (1.4–7.6) Yes > 6.1 71/62 4.7 (2.3–9.5) Ptrend< 0.0001
Cigarette smoking DMA percentage
No > 89.1 101/24 1.00 1.09 (0.53–2.24) Estimated OR 1.03 χ2 2.08; P = 0.15 No ≤89.1 95/61 2.9 (1.7–5.2) Yes > 89.1 37/16 2.9 (1.2–6.9) Yes ≤89.1 68/66 5.1 (2.5–10.5) Ptrend< 0.0001
Cigarette smoking Primary methylation index
No ≤1.1 103/29 1.0 0.93 (0.43–2.03) Estimated OR 0.88 χ2 11.78; P = 0.003 No > 1.1 93/56 2.2 (1.3–3.8) Yes ≤1.1 39/27 2.8 (1.3–6.0) Yes > 1.1 66/55 3.8 (1.9–7.5) Ptrend= 0.0002
Cigarette smoking Secondary methylation index
No > 8.2 106/30 1.0 1.31 (0.60–2.85) Estimated OR 0.97 χ22.14; P = 0.16 No ≤8.2 90/55 2.6 (1.5–4.5) Yes > 8.2 43/18 2.1 (0.9–4.9) Yes ≤8.2 62/64 4.5 (2.3–8.9) Ptrend< 0.0001 a
inorganic arsenic, MMA and DMA levels of UC cases and
non-cancer controls in this study were 26.6 ± 1.4 and 22.1 ±
1.8
μg/L (data not shown), respectively. These values were
significantly lower than those in our previous study, where
the levels for skin cancer patients and healthy controls from
the arsenic-contaminated area in Taiwan were 104.1 ± 15.2
and 89.5 ± 7.2
μg/L, respectively (
Hsueh et al., 1997
). Taken
together, these values indicate that our cases and controls
were subjects of low exposure. Nonetheless, we still observed
an elevated UC risk in subjects with unfavorable urinary
arsenic profile. More strikingly, unfavorable PMI and SMI
levels confer an increased risk in non-smokers, suggesting
that undetectable or negligible environmental arsenic still
plays an important role.
Although the allowed arsenic levels in drinking water were
not greater than 50
μg/L prior to year 2000, there may be minor
differences in arsenic levels between various regions in Taiwan.
According to the Taipei Water Department of the Taipei City
Government, the average arsenic concentration in Taipei tap
water is 0.7
μg/L and ranges from non-detectable to 4.0 μg/L.
We do not know whether differential exposure within a low
allowable range affects UC risk. However, we have
demon-strated that differential urinary arsenic profile in subjects with
no arsenic exposure history who had consumed low allowable
levels of arsenic in water significantly affected UC risk. This
finding suggests that low arsenic levels in drinking water may
still be unsafe for susceptible subjects.
Smoking was found to interact with urinary arsenic profile in
affecting the UC risk. The synergy indices of the two factors
ranged from 0.86 to 1.35, although they were all statistically
insignificant. The likelihood ratio test, however, revealed
sig-nificant synergistic interactions between smoking and inorganic
arsenic and PMI. This finding is similar to a recent study that
demonstrated a significant interaction between smoking and
SMI on the risk of bladder cancer (
Chen et al., 2005
). These data
indicate that subjects who have unfavorable urinary arsenic
profile are at a greater risk if they smoke.
Our previous study has shown that as concentrations of
urinary selenium and serum alpha-tocopherol increased, percent
inorganic arsenic significantly decreased and percent DMA
increased (
Hsueh et al., 2003
). Bangladesh study found that the
plasma folate was positively and negatively associated with the
DMA and MMA percentage, respectively (
Gamble et al., 2005
).
Several antioxidants, including N-acetylcysteine, zinc,
methio-nine and cysteine, when used in conjunction with standard
chelating agents, can improve the mobilization and excretion of
arsenic compounds (
Patrick, 2003
). Heavy medications
espe-cially those which induce or inhibit cellular glutathione
contents, glutathione S-transferase, multi-drug resistance-1,
multi-drug resistance associated protein-1, etc. may all
significantly affect arsenic metabolism. For the vast majority
(> 95%) of our patients, however, the chance of getting
interfered by medications in case subjects was no different
from that of controls. Understanding the arsenic methylation
pathway has important clinical implications. Chemoprevention
for high-risk populations is thus feasible by facilitating the
arsenic methylation process and increasing the excretion of
toxic metabolites.
References
Andreae, M.O., 1977. Determination of arsenic species in natural waters. Anal. Chem. 49, 820–823.
Bates, M.N., Rey, O.A., Biggs, M.L., Hopenhayn, C., Moore, L.E., Kalman, D., Steinmaus, C., Smith, A.H., 2004. Case–control study of bladder cancer and exposure to arsenic in Argentina. Am. J. Epidemiol. 159, 381–389. Brennan, P., Bogillot, O., Cordier, S., Greiser, E., Schill, W., Vineis, P.,
Lopez-Abente, G., Tzonou, A., Chang-Claude, J., Bolm-Audorff, U., Jockel, K.H., Donato, F., Serra, C., Wahrendorf, J., Hours, M., T'Mannetje, A., Kogevinas, M., Boffetta, P., 2000. Cigarette smoking and bladder cancer in men: a pooled analysis of 11 case–control studies. Int. J. Cancer 86, 289–294.
Chen, C.J., Chuang, Y.C., Lin, T.M., Wu, H.Y., 1985. Malignant neoplasms among residents of a blackfoot disease-endemic area in Taiwan: high-arsenic artesian well water and cancers. Cancer Res. 45, 5895–5899.
Chen, C.J., Kuo, T.L., Wu, M.M., 1988. Arsenic and cancers. Lancet 1, 414–415.
Chen, Y.C., Amarasiriwardena, C.J., Hsueh, Y.M., Christiani, D.C., 2002. Stability of arsenic species and insoluble arsenic in human urine. Cancer Epidemiol., Biomarkers Prev. 11, 1427–1433.
Chen, Y.C., Guo, Y.L., Su, H.J., Hsueh, Y.M., Smith, T.J., Ryan, L.M., Lee, M.S., Chao, S.C., Lee, J.Y., Christiani, D.C., 2003a. Arsenic methylation and skin cancer risk in southwestern Taiwan. J. Occup. Environ. Med. 45, 241–248.
Chen, Y.C., Su, H.J., Guo, Y.L., Hsueh, Y.M., Smith, T.J., Ryan, L.M., Lee, M.S., Christiani, D.C., 2003b. Arsenic methylation and bladder cancer risk in Taiwan. Cancer Causes Control 14, 303–310.
Chen, Y.C., Su, H.J., Guo, Y.L., Houseman, E.A., Christiani, D.C., 2005. Interaction between environmental tobacco smoke and arsenic methylation ability on the risk of bladder cancer. Cancer Causes Control 16, 75–81. Chien, Y.H., Bau, D.T., Jan, K.Y., 2004. Nitric oxide inhibits DNA-adduct
excision in nucleotide excision repair. Free Radical Biol. Med. 36, 1011–1017. Chiou, H.Y., Chiou, S.T., Hsu, Y.H., Chou, Y.L., Tseng, C.H., Wei, M.L., Chen, Table 6
Interaction of primary and secondary methylation indices stratified by cigarette smoking status Primary methylation index Secondary methylation index n of controls/ UC cases
Age and gender adjusted OR (95% CI)
Multivariate adjusted ORa
(95% CI) All subjects (case n = 177, control n = 313)
≤1.1 > 8.2 70/21 1.0 1.0 > 1.1 > 8.2 88/31 1.2 (0.6–2.3) 2.0 (1.0–4.3) ≤1.1 ≤8.2 77/41 1.9 (1.0–3.3) 1.5 (0.7–3.0) > 1.1 ≤8.2 78/84 3.6 (2.0–6.5) 5.0 (2.5–9.9) Ptrend< 0.0001 Ptrend< 0.0001
Non-smokers (case n = 85, control n = 196)
≤1.1 > 8.2 53/11 1.0 1.0 > 1.1 > 8.2 53/19 1.8 (0.8–4.2) 2.5 (0.9–7.2) ≤1.1 ≤8.2 50/18 1.7 (0.7–4.4) 1.4 (0.5–3.7) > 1.1 ≤8.2 40/37 4.7 (2.1–10.6) 6.6 (2.5–17.4)
Ptrend< 0.0001 Ptrend= 0.0004
Current and former smokers (case n = 92, control n = 117) ≤1.1 > 8.2 17/10 1.0 1.0 > 1.1 > 8.2 35/12 0.5 (0.2–1.5) 1.1 (0.4–3.7) ≤1.1 ≤8.2 27/23 1.3 (0.5–3.4) 1.0 (0.3–2.9) > 1.1 ≤8.2 38/47 2.1 (0.9–5.1) 3.1 (1.1–8.6) Ptrend= 0.004 Ptrend= 0.01 a
Multivariate adjusted OR: adjusted for age, gender, education, paternal and maternal ethnicity, alcohol drinking, and pesticide usage.
C.J., 2001. Incidence of transitional cell carcinoma and arsenic in drinking water: a follow-up study of 8,102 residents in an arseniasis-endemic area in northeastern Taiwan. Am. J. Epidemiol. 153, 411–418.
Evans, C.D., LaDow, K., Schumann, B.L., Savage Jr., R.E., Caruso, J., Vonderheide, A., Succop, P., Talaska, G., 2004. Effect of arsenic on benzo[a] pyrene DNA adduct levels in mouse skin and lung. Carcinogenesis 25, 493–497.
Francesconi, K.A., Tanggaar, R., McKenzie, C.J., Goessler, W., 2002. Arsenic metabolites in human urine after ingestion of an arsenosugar. Clin. Chem. 48, 92–101.
Gamble, M.V., Liu, X., Ahsan, H., Pilsner, R., Ilievski, V., Slavkovich, V., Parvez, F., Levy, D., Factor-Litvak, P., Graziano, J.H., 2005. Folate, homocysteine, and arsenic metabolism in arsenic-exposed individuals in Bangladesh. Environ. Health Perspect. 113, 1683–1688.
Hopenhayn-Rich, C., Biggs, M.L., Smith, A.H., Kalman, D.A., Moore, L.E., 1996. Methylation study of a population environmentally exposed to arsenic in drinking water. Environ. Health Perspect. 104, 620–628.
Hosmer, D.W., Lemeshow, S., 1992. Confidence interval estimation of interaction. Epidemiology 3, 452–456.
Hsueh, Y.M., Chiou, H.Y., Huang, Y.L., Wu, W.L., Huang, C.C., Yang, M.H., Lue, L.C., Chen, G.S., Chen, C.J., 1997. Serum beta-carotene level, arsenic methylation capability, and incidence of skin cancer. Cancer Epidemiol., Biomarkers Prev. 6, 589–596.
Hsueh, Y.M., Huang, Y.L., Huang, C.C., Wu, W.L., Chen, H.M., Yang, M.H., Lue, L.C., Chen, C.J., 1998. Urinary levels of inorganic and organic arsenic metabolites among residents in an arseniasis-hyperendemic area in Taiwan. J. Toxicol. Environ. Health, Part A 54, 431–444.
Hsueh, Y.M., Hsu, M.K., Chiou, H.Y., Yang, M.H., Huang, C.C., Chen, C.J., 2002. Urinary arsenic speciation in subjects with or without restriction from seafood dietary intake. Toxicol. Lett. 133, 83–91.
Hsueh, Y.M., Ko, Y.F., Huang, Y.K., Chen, H.W., Chiou, H.Y., Huang, Y.L., Yang, M.H., Chen, C.J., 2003. Determinants of inorganic arsenic methylation capability among residents of the Lanyang Basin, Taiwan: arsenic and selenium exposure and alcohol consumption. Toxicol. Lett. 137, 49–63.
Le, X.C., Ma, M., Cullen, W.R., Aposhian, H.V., Lu, X., Zheng, B., 2000. Determination of monomethylarsonous acid, a key arsenic methylation intermediate, in human urine. Environ. Health Perspect. 108, 1015–1018. Lin, S.M., 1986. Diagnostic usefulness of trace arsenic in human urine, whole
blood, hair and fingernails. Gaoxiong Yixue Kexue Zazhi 2, 100–113. Lin, S., Del Razo, L.M., Styblo, M., Wang, C., Cullen, W.R., Thomas, D.J.,
2001. Arsenicals inhibit thioredoxin reductase in cultured rat hepatocytes. Chem. Res. Toxicol. 14, 305–311.
Ma, M., Le, X.C., 1998. Effect of arsenosugar ingestion on urinary arsenic speciation. Clin. Chem. 44, 539–550.
Mandal, B.K., Ogra, Y., Suzuki, K.T., 2001. Identification of dimethylarsinous and monomethylarsonous acids in human urine of the arsenic-affected areas in West Bengal, India. Chem. Res. Toxicol. 14, 371–378.
Mass, M.J., Tennant, A., Roop, B.C., Cullen, W.R., Styblo, M., Thomas, D.J., Kligerman, A.D., 2001. Methylated trivalent arsenic species are genotoxic. Chem. Res. Toxicol. 14, 355–361.
Morales, K.H., Ryan, L., Kuo, T.L., Wu, M.M., Chen, C.J., 2000. Risk of internal cancers from arsenic in drinking water. Environ. Health Perspect. 108, 655–661.
National Research Council, 1999. Arsenic in Drinking Water. National Academy Press, Washington, DC.
National Research Council, 2001. Arsenic in Drinking Water Update. National Academy Press, Washington, DC.
Patrick, L., 2003. Toxic metals and antioxidants: Part II. The role of antioxidants in arsenic and cadmium toxicity. Altern. Med. Rev. 8, 106–128.
Petrick, J.S., Ayala-Fierro, F., Cullen, W.R., Carter, D.E., Vasken, A.H., 2000.
Monomethylarsonous acid (MMA(III)) is more toxic than arsenite in Chang human hepatocytes. Toxicol. Appl. Pharmacol. 163, 203–207.
Rothman, K.J., 1986. Modern Epidemiology. Litter Brown and Company, Boston, MA.
Schwerdtle, T., Walter, I., Hartwig, A., 2003a. Arsenite and its biomethylated metabolites interfere with the formation and repair of stable BPDE-induced DNA adducts in human cells and impair XPAzf and Fpg. DNA Repair (Amst.) 2, 1449–1463.
Schwerdtle, T., Walter, I., Mackiw, I., Hartwig, A., 2003b. Induction of oxidative DNA damage by arsenite and its trivalent and pentavalent methylated metabolites in cultured human cells and isolated DNA. Carcinogenesis 24, 967–974.
Smith, A.H., Hopenhayn-Rich, C., Bates, M.N., Goeden, H.M., Hertz-Picciotto, I., Duggan, H.M., Wood, R., Kosnett, M.J., Smith, M.T., 1992. Cancer risks from arsenic in drinking water. Environ. Health Perspect. 97, 259–267. Smith, A.H., Lopipero, P.A., Bates, M.N., Steinmaus, C.M., 2002. Public
health—Arsenic epidemiology and drinking water standards. Science 296, 2145–2146.
Smith, A.H., Marshall, G., Yuan, Y., Ferreccio, C., Liaw, J., von Ehrenstein, O., Steinmaus, C., Bates, M.N., Selvin, S., 2006. Increased mortality from lung cancer and bronchiectasis in young adults after exposure to arsenic in utero and in early childhood. Environ. Health Perspect. 114, 1293–1296. Styblo, M., Drobna, Z., Jaspers, I., Lin, S., Thomas, D.J., 2002. The role of
biomethylation in toxicity and carcinogenicity of arsenic: a research update. Environ. Health Perspect. 110 (Suppl. 5), 767–771.
Tezuka, M., Hanioka, K., Yamanaka, K., Okada, S., 1993. Gene damage induced in human alveolar type II (L-132) cells by exposure to dimethylarsinic acid. Biochem. Biophys. Res. Commun. 191, 1178–1183. Thomas, D.J., Styblo, M., Lin, S., 2001. The cellular metabolism and systemic
toxicity of arsenic. Toxicol. Appl. Pharmacol. 176, 127–144.
Tran, H.P., Prakash, A.S., Barnard, R., Chiswell, B., Ng, J.C., 2002. Arsenic inhibits the repair of DNA damage induced by benzo(a)pyrene. Toxicol. Lett. 133, 59–67.
Tseng, C.H., Huang, Y.K., Huang, Y.L., Chung, C.J., Yang, M.H., Chen, C.J., Hsueh, Y.M., 2005. Arsenic exposure, urinary arsenic speciation, and peripheral vascular disease in blackfoot disease-hyperendemic villages in Taiwan. Toxicol. Appl. Pharmacol. 206, 299–308.
US EPA, 1998. Arsenic, inorganic (CASRN 7440-38-2). Ref Type: Internet Communication.
Vahter, M., 2002. Mechanisms of arsenic biotransformation. Toxicology 181–182, 211–217.
Vineis, P., Talaska, G., Malaveille, C., Bartsch, H., Martone, T., Sithisarankul, P., Strickland, P., 1996. DNA adducts in urothelial cells: relationship with biomarkers of exposure to arylamines and polycyclic aromatic hydrocarbons from tobacco smoke. Int. J. Cancer 65, 314–316.
WHO, 1999. Histological Typing of Urinary Bladder Tumours. International Classification of Tumours. World Health Organization, Geneva.
Yamauchi, H., Fowler, B.A., 1994. Toxicity and metabolism of inorganic and methylated arsenicals. In: Nriagu, J.O. (Ed.), Arsenic in the Environment, Part 2: Human Health and Ecosystem Effects. John Wiley and Sons, New York, pp. 33–43. Ref Type: Serial (Book,Monograph).
Yang, C.Y., Chiu, H.F., Chang, C.C., Ho, S.C., Wu, T.N., 2005. Bladder cancer mortality reduction after installation of a tap-water supply system in an arsenious-endemic area in southwestern Taiwan. Environ. Res. 98, 127–132.
Zeegers, M.P., Tan, F.E., Dorant, E., van Den Brandt, P.A., 2000. The impact of characteristics of cigarette smoking on urinary tract cancer risk: a meta-analysis of epidemiologic studies. Cancer 89, 630–639.
Zeegers, M.P., Kellen, E., Buntinx, F., van den Brandt, P.A., 2004. The association between smoking, beverage consumption, diet and bladder cancer: a systematic literature review. World J. Urol. 21, 392–401.