1111 Surg 2010;95:108-116
Classification and Comparison of Niche
Services for Developing Strategy of Medical
Tourism in Asian Countries
Hung-chi Chen\ Hsin-chih Kuo
2,Kuo-Piao Chung
3,Sophia Chang
4,Syi Su
3,Ming-chin Yang
3'Department of Plastic Surgery, E-Da Hospital/I-Shou University, Kaohsiung, Taiwan
(R.O.C)2Department of Health Management, I-Shou University, Kaohsiung, Taiwan
(R.O.C)3Department of Public Health/Institute of Health Care Organization Administration, College of Public
Health, National Taiwan University, Taipei, Taiwan
(R.O.C)4Department of Plastic Surgery, China Medical University Hospital, Taichung, Taiwan
(R.O.C)Medical tourism is a new trend in medical service. It is booming not only in Asian
countries but also in European and South American countries. Worldwide competition of medical service is expected in the future, and niche service will be a ILtrademark'F for the promotion of global medicine. Niche service also functions for market segmentation. Niche services are usually surgical procedures. A study was carried out to compare
different strategies for developing medical tourism in Asian countries. The role of a niche service is evaluated in the initiation and further developluent of medical tourism for individual countries. From this study, a general classification was proposed in terms of treatment procedures. It can be used as a useful guideline for additional studies in medical tourism. Niche service plays the following roles in the development of medical tourism: (1) It attracts attention in the mass media and helps in subsequent promotion of business, (2) it exerts pressure on the hospital, which must improve the quality of health care provided in treating foreign patients, especially the niche services, and (3) it is a tool for setting up the business model. E-Da Hospital is an example for developing medical tourism in Taiwan. A side effect is that niche service brings additional foreign patients, which will contribute to the benefit of the hospital, but this leaves less room for treating domestic patients. A niche service is a means of introduction for entry into the market of
Reprint requests: Ming-chin Yang, MD, PhD, Dcparhncnt of Public Health Carclu1stitute of Health Care Organization Administration, College of Public Health, National Tai\van University, Taipei, Tai\Nan.
Tel.: +886233668067; E-mail: [email protected]
:--aCHE SERVICES FOR GLOBAL MEDICINE CHEN
medical tourism. How to create a successful story is iInportant for the development of a niche service. When a good reputation has been established, the information provided on the Internet can last for a long time and can spread internationally to form a distinguished mark for further development. Niche services can be classified into 3 categories: (1) Low-risk procedures with large price differences and long stay after retirement; (2) high-risk procedures with less of a price difference, and (3) banned procedures that are not allowed legally in home countries of foreign patients, such as stem cell therapy. In establishing a niche service, a high-quality, nonmedical segment should be integrated as well.
Key
words: Niche service - Globallnedicine - Asia - ClassificationS
everal difficulties in the development of medical tourism have been identified: (1) It would be much lllore comfortable to have major surgery near home with family members at the bedside than to travel overseas for surgery and experience culture shock in a developing country, (2) patients and their family are often frustrated \vhen communicating \"lith foreign doctors and nurses because of barriers in language and customs, and (3) patients often worry about their health and are uncertain about the quality of health care in another cOlmtry. They are always fearful about traveling far from home and cannot trust the medical quality of health care organizations in destination countries. In this situ-ation, "trust" should come frOlll "reputation,"which is built on the previous record of health care quality and niche services as presented to the public. However, there are still several reasons for development of international health travel' -5:
1. Saving money-it is an important concern in international medical tourism.
2. Efficiency-the niche service promoted by a certain country should include an efficient standard operating procedure (SOP) for diag-nosis and treahnent of a particular disease.
3. Convenience-it provides convenience and high quality of service.
4. Special disease-treat special diseases, such as Chiari syndrome.
S. Banned therapy-patients seek procedures that have not been approved by the law in their home countries (e.g., steIn cell therapy for advanced heart and neurologic disorders). The effects of these therapies have not been proved in the developed countries, but patients still want to try even when there is little hope of success. 6. Privacy-patients who are the leaders of very
important organizations or chain businesses do not want to leave a record in hOlne
lnt Sms 2010;95
countries, such as health examination or cosmetic surgery.
7. Life of retire1llent-patients seek long stay after retirement.
8. Vacation~a less important factor is the vacation
part of the trip.
In 2007, 3 million people in the world left their hOlne countries and sought health care in other countries.6 Overseas Inedical treahuent included open heart surgery, aesthetic surgery and recon-struction, health examination, treahl1ent for infertil-ity, and other operations. In 2005, 1.25 million foreigners entered TI1ailand for medical travel at a total expense of US $860 million. The Indian govermnent predicted an annual income of US $17 billion from medical travel over the next 6 years. In
Singapore, patients beyond borders increased from 270,000 patients in 2005, to 400,000 patients in 2007, and total income in 2007 was US $1.5 billion. In fact, in some hospitals in Singapore, 40% of the revenue in 2008 was derived from treating foreign patients.
In India and Dubai, many medical cities have been established, including hospitals, affiliated hotels and recreation areas, spas, research units, shopping lnalls, travel agencies, and so forth. Now, 28 counh-ies in 4 continents are devoted to promot-ing international health trave1.7,8
A niche service is established over years of practice to earn a \vorldwide reputation and to "'lin the trust of people. It is necessary to convince people to come over from other cOlliltries for health care. In addition to updated facilities, organizational success depends on trust built by doctors, nurses, and paramedical personnel who provide remarkable service experience.
A niche service meets one or several of the criteria listed below:
1. Safety-it is always a big decision for an individual patient to seek medical treahnent in 109
CHEN
a foreign country. Patients want to Ininimize a certain inherent risk before they go ahead. For example, India is famous for open heart surgery '''lith a 11101tality of 0.9% for nonemergen teases. These data are even better than those of the average American hospital. In the United States, Blue Cross and Blue Shield (South Carolina) was the first American insurance company to provide medical care overseas. This insurance company studied thoroughly the niche services of various countries to provide safe treatment and avoid legal problems afterward. However, most countries do not have the American attitude toward physicians and institutional liability.
2. Pric2 diffa2ilcf~iliche serviceS usually can be
offered more quickly at a lower price by Asian cOlU1tries.
3.
Facility availability-facilities
should be avail-able with enough capacity to provide the service in time (e.g., operations for tumors). 4. Skills needed-skills needed for some nicheservices are available to provide high-level medical treahnent.
5.
Definitive procedures-definitive
procedures can be performed to get a good result within a reasonable period of time.Method
During a literature review, important facts were found regarding the development of various niche services among different Asian countries. On the basis of the analysis, a classification was proposed as a guide to the study of development of medical tourism for Asian countries. The target Asian countries mainly include Malaysia, Korea, TI1ailand, Singapore, and India. Aftenvard, a story of medical tourism for Taiwan will be presented to explore the development of niche services.
In our classification, niche services are divided into 3 categories: (1) Category I includes long stay after retirement (Category Ia) and low-risk proce-dures with large price differences (Category Ib); (2) Category II consists of high-risk procedures with less of a price difference but of high quality and much better in terms of convenience; and (3) Category III is made up of banned procedures that are not allowed legally in home counh·ies.
The history of developing niche services for medical tourisln in each country is different because of variations in geography, social and econOlnic conditions, safety, cultural differences, language,
110
NICHE SERVICES FOR GLOBAL MEDICINE
level of medical care, and so forth. Niche sey\Tices are compared on the basis of efficacy in this study. The niche service provides the basis for subsequent development of a business model and then mainte-nance of a cluster of services.
Results
Every country has different conditions and selects different niche services. TI1e follmving niche services were noted in the literature.6,9-14
Malaysia
Long stay in Malaysia is favored by rich Chinese people and Sing8"poreHIls. Chinp~E' pE'oplf' invest in Malaysia, but Singaporeans like it because of its proximity to Malaysia and its low cost of living. Because of the large potential for profit from cosmetic procedures, Malaysia has established an-other cosmetic city in Penang. Generally speaking, the niche services provided by Malaysia belong to Category I in our classification.
Indonesia and Philippines
Generally speaking, Indonesia and the Philippines are less often considered as the first choice for long stay because of concerns about social stability.
Korea
Korea promotes its cosmetic surgery through actors in famous movies, which are promoted successfully in the theaters of other countries. More than 10,000 women per year go to Korea for aesthetic proce-dures. Generally speaking, the niche services of Korea belong to Category I in our classification.
Thailand
The cost of health care in Thailand is only 30% of that in the United States. Major items of medical service include cosmetic surgery and dentistry. In 2003, Thailand treated 730,000 foreign patients with US $488 million of income. These figures increased by 16% by 2005. In 2006, medical tourism had brought about an annual income of US $700 million for Thailand. About 15% of these patients come from the United States and Canada. Thailand is also fmnous for trans-sexual operations.
Bumrungrad International Hospital has been recognized as one of the top 10 most international-ized hospitals in the world. It is affiliated with
NICHE SEE\'lCES FOE GLOBAL MEmONE
Diethelm Travel Agency and TI1ai Airway to provide services combining medical care and sight-seeing. The Bwnrungrad International Hospital has passed Joint Corrunission International (JCI) accred-itation with an international standard of 11ledical service. JCI is an international standard of health care quality for the insurance company to document and to pay. The other famous hospital is Bangkok International Hospital.
The trust spectrum that we saw from the history of luedical tourisln in Thailand emerged in this order: Spa experiences, denture procedures, cosmet-ic procedures, and finally full surgery. When we want to V\Tin the recognition of a niche service, we should pay attention not only to the articulated needs but also to the unarticulated needs. Nalnely, both medical and supportive services for patients and their attendants are important. Generally speaking, the niche services of Thailand fall into Categories I, II, and III in our classification.
Singapore
In 2003, the Singaporean government focused on medical travel through the combined efforts of various organizations, including those for economic develop-ment, tourism, and the development of international enterprise, which promote medical services with tOuriSlU. Major services provided are high-tech
med-ical service, health examination, and coslnetic surgery. In 2007, Singapore h'eated about 400,000 patients from other counh·ies. This number will be increased to 1 million patients from abroad in 2012. Generally speaking, the niche services of Singapore belong to Categories I and II in our classification.
India
India was famous for its success in conjoined t\,vin surgery. TI1en the government promoted heart surgery and joint replacement. India has several privileges for development of medical travel. Numer-ous Indian phYSicians and surgeons are being trained in the United States and the United Kingdom. Some of them stay in these countries and others go back to India. They form a strong army to provide good service and sh'ong follow-up for international pa-tients. In addition, English is a commonly used language in India. The Indian government is the most important backup for the development of medical traveL Generally speaking, the niche services provid-ed by India belong to Categories I and II in our classification.
lilt 5wg 2010;95
CHEN
Japan
Japan so far has not proll10ted medical tourisln on a large scale because of its already high cost of health care and has offered little or no price difference. However, it has high potential for developing Category II medical tourism with patients from other Asian countries.
Classification of niche services for Asian countries
Niche service is concerned with 3 main factors: (1) The capacity of the medical staff, especially of phYSicians with advanced technology in particular subspecialties, (2) the price difference between the cmmtly providing service and the patient's own country, and (3) the reputation of the service in the desth"1ation country.
Other general factors that support the niche service include the following:
1. Safety, insurance coverage, stability of the country, ensured service quality by some certified institution such as JCl, aud efficiency of various arrangements.
2. Friendliness-attitudes of people toward
for-eigners-friendly or not.
3. Living cost-economic conditions of the people and living standards of the destination country.
4. Convenience in daily life-languages spoken by
most people in that country, cleanliness of the environment, facilities, and resources of sight-seeing.
5. Availability of activities and richness of
culture-relation V\Tith other countries in Hs past historYr religions, culhue, and tradition.
6. Ease of ently or exit-ease of obtaining a visa,
transportation, proximity to the destination country, and availability of follow-up.
According to the number of cases and the severity of disease, niche services are divided jnto 3 categories (Fig. 1).
Category I indicates Im,ver severity of disease and larger numbers of cases such as long stay (Category Ia) and health examinations, dental care, cosmetic surgery, and so forth (Category Ib). This category tends toward service orientation.
Category II indicates higher severity of disease and smaller nU1nbers of cases such as trans-sexual operations, treatment of heart disorders, and so forth. This category tends toward technique orientation.
Category III indicates highest severity of disease and slnallest numbers of cases, such as stem cell therapy for advanced heart and brain therapy (but not recognized internationally). TIus category usu-ally involves some disputed techniques that could be banned at a specific period in some c01ll1tries.
CHEN _ Citegory la - Category Jb Low High Severity of diseases
Fig. 1 Three categories of niche services.
Because each country has different context and resources, each will select a combination of different niche services to obtain its revenue. Each C01Ultry may choose I, 2, or 3 categories as its niche services area (Table 1).
hl terms of changes in the medical tourism market Asian cOlll1tries with the greatest amOlll1t of revenue from global medicine currently are Thailand, India, Singapore, and Malaysia. These COlll1tries adopted their own niche services to get the market and total revenue of medical tourism (Fig. 2). The relationship between total revenue and risk in procedures is sketched according to the present status of the medical tourism market share. For Thailand, niche services are those with low demand on tec]ul0logy, such as health examination.
It deserves to be mentioned that the niche services of Thailand have changed from Category Ia and Ib to Category IT and Category III over time. For Singapore, the niche service consists of high tech-nology, such as neurosurgery.
Table 1 Summary of niche services among Asian collntries
(ounh'y Malaysia Korea TiInilnl1d Singnpore India Category La Long stay Long stay Category I Category Ib Cosmetic surgery Cosmetic surgery Health examinations Dental care Cosmetic surgery Orthopedic surgery Ophthalmology Knee replacement
"Not recognized internationally.
112
N1CHE SERVICES FOR GLOBAL l\:fEDlCINE
-'"
."
-'" ill ~ C ill > ~ro
"
.... ? ;: 0 ~ Low High Risk in proceduresFig. 2 The relationship between total revenue and risk in procedures.
When a counh-y wants to start medical tourism, what niche services will it select? Let's see a successful story of medical tourisnl in Taiwan. A Successful Story of Medical Tourism in Taiwan
E-Da Hospital is the hospital affiliated with I-Shall University, located at Yanchao Township of Kaoh-siung County in Soufh Taiwan. E-Da Hospital has 1200 beds and the most modem equipment. In recent years, a medical city has been established tl1at includes the hospital, a 5-star hotel, which is fhe second largest hotel in Taiwan, a hot spring area, a large shopping mall, a European street, a golf course, and so forfh.
Story beginning from a country in South America
Since the opening of this hospital, many fellows from various countries have corne here to learn reconstructive surgery. One of the fellows visited
Category II Trans-sexual operations Neurosurgery Cancer treahnent Heart surgery ConjOined hvin Category III
Stem cell therapy'" for heart and brain therapy
NICHE SERVICES FOR GLOBAL MEDICL"JE
this country and gave a lechu<e in South America. He "'\vas consulted for a very severe case of lymphedema praecox. He decided to transfer the patient to E-Da Hospital because he knew that E-Da Hospital was able to treat the patient well because it had a large an10unt of previous experience.
The patient had a huge lower limb and had suffered from severe primary lymphedema of the right lower limb for 26 years. This got worse and caused cardiomegaly through the progressive in-crease in lymphatic load. If this problem were left unsolved, it would become intractable within a short time. Therefore E-Da Hospital sent an attending staff from eluergency medicine to escort the patient to Taiwan on November 9, 2007, because he could speak Spanish and was able to perform resuscitatioll during the trip whenever necessary.
Presenting problems
This patient had the following major problems in her daily life:
Severe swelling of right thigh, leg, and foot and inability
to squat down.
111is vvas so heavy that it caused a remarkable disturbance in walking. Every time the patient got up from bed, a lot of blood and lymph would be pooled into her right lower limb, and the sudden decrease in effective intravascular volwue would make her dizzy. On the other hand, when the leg was put back on the bed, the suddenly increased circulatory volume \vould ll1ake her uncomfortable, like a dumping phenomenon of blood and lymph entering the general circulation. Retrospectively, it was found that the right lower limb had 47 kg of extra tissue, which had been reluoved during surgery. 111is "'\vas the cause of the circulatory distill'bance.Osteoarthritic change in right calcaneus.
Osteoar-thritic change in the right calcaneus was due to the heavy load of the right lower limb. It caused the formation of a large bursa beneath the calcaneus, "'\vhich "'\,vas ren10ved during surgery.Appearance of black plaques and induration of the skin
over right lower limb like elephant skill.
The blood supply to the tense skin was severely unpaired. This further rendered the limb susceptible to trauma and infection.Frequent infection (cellulitis) of the right lower limb
ill1d toe infection with very bad smell.
The condition would interfere with social life. Infection of the right lower limb was frequently treated with antibiotics in the hospital.Two major ulcers of skin in the right lower limb with
frequent lymph leakage.
It could be water clear or milky in appearance following a meal, just like an oak h·eelnt Surg 2010;95
CHEN
leaking frOlu a hole cut in its trunk. AccOlupanying the lymph leakage was protein loss, so that the patient had hypoalbuminuria on admission.
Remarkable decrease in sensation in the right lower
limb.
Hm,vever, sensation in the right foot sole was preserved.Problem for the passage of urine.
The mine often spilled to her right thigh, which was so large as to extend across the lnidline. The urine V\7ent into the deep skincreases and presented difficulty in personal hygiene.
Worse condition after
2operations.
The patient had been operated on tvvice in her hOlue country, but th_e condition bec31ue vvorse regardless of these opera-tions.Joblessness and withdrawal from all social activities.
She could not go to work and withdrew from all social activities.Course of treatment: Interdisciplinary team work
The patient was admitted to the ward of plastic surgery before operation. An intravascular supply of albumin was provided. Members from a total of 15 departments in the hospital were consulted and got together to design a detailed treatment plan. These specialties and related departments included plastic surgery, cardiology, pulmonary medicine, vascular surgery, luetabolisn1, infectious disease, psychiatry, rehabilitation, hematology and oncology, radiology, the nutrition deparhuent, a social v1lOrker, intensive care unit (ICU), nursing, especially in the operating room, and administration.11le operation "'\,vas carried out on November 16, 2007. Cardiac output and other hemodynamic conditions were intensively monitored by a cardiol-ogist and an anesthesiolcardiol-ogist during the entire operation, which ""vas finished in 8 hours. The diseased tissue ren10ved measured 47 kg, which was equivalent to the body weight of a nurse taking care of this patient.
After surgery, the patient was put in the lCU for 1 week, with continuous monitoring of PICCO, endocrine fW1CtiOl1, and electrolyte and cardiopul-monary functions; measures to prevent deep vein tlu·ombosis; rehabilitation; and psychological adap-tation to new body images.
Results of operation
The patient felt that her right lower limb became much lighter after surgery. She was so happy and "'\vas moved to tears when she first savv the ne\tv shape of her leg after waking up from anesthesia. It
CHEN
had been a great torture to her for 26 years. After surgery, she began to have a new life. All the nurses treated her very nicely and learned from her hmv to speak some Spanish.
She had only 1 tooth left in the upper gum with obvious difficulty in chewing. She used to take a soft diet and had difficulty digesting hard food. The government also provided free dental implants for her to improve her quality of life.
On behalf of the goverrunent of her home counh-y, a diplomat frequently phoned E-Da Hos-pital to inquire about her condition. This showed great care regarding her h'eatment in Taiwan. He came to see this patient and expressed sincere appreciation to the Taiwanese people.
The patient \t\Tent home as a different person, having good legs and good teeth with dramatic improvement in life quality. The success in treahnent was also a benchmark of intimate collaboration alnong team members in the hospitaL It ,vas all example of patient-centered care. In the treahnent course, the Deparhnent of Health and Ministry of Foreign Affairs provided help to this patient. This successful story ,vas achieved through the combined efforts of all possible resources. It not only offered an experience of hmnanitarian rescue but also formed the basis for development of medical tourism.
Consequence of the successful story
The information spread thmugh the newspaper, television, and the Internet. Since then, E-Da Hospital has treated many international patients, not only those with lymphedema or extremity deformities, but also those with various kinds of diseases needing procedures such as aesthetic surgery. The number of patients beyond borders is increasing. According to Singaporean colleagues, a country that wants to enter the market of medical tourism must take action in accepting international patients through the promotion of niche service. Discussion
Common characteristics of niche services in medical touriSln are as follows:
1.
Good
service or results-good service or result perceived by the patient:114
a. Small incisions (mini-invasive surgery), endo-scopic procedures,- and robotic sm'gely
(e.g.,
prostate surgeq to preserve sex function). b. Better function
(e.g.,
prostate surgery topreserve sex function), obvious deformity ,vell corrected or reconstructed.
NICHE SERVICES FOR GLOBAL MEDICINE
2.
Lower
cost-price one-third that in hOllle coun-tries.3,
Minimal waiting time before scheduling procedures.
4.
Service not available in home countries.
It has been proved that medical outsourcing is effective to decrease expenditures for many countries in Europe, the United States, and Canada. It is more cost-effective than increasing the facility and person-nel of hospitals in these countries. However, COUl1-tries providing international health services must be able to provide evidence to prove their competence, especially regarding safety, convenience, and best quality of h<eahnent, such as JCI accreditation, before they can be considered for medical outsourcing.
People in most countries do not have the same attitude as Americans toward physiCian and insti-tutional liability15-19 If legal recourse is a major concern of a particular patient, the patient is not encouraged to go abroad for medical treahnent. The recent economic crisis seems to have worsened the economic condition of the developed countries and increased the need for medical tourism.
Concerning long stay, safety and cost are regarded as the most important factors for consideration. The requirement of savings in the bank is lowest in Thailand-about US $20,000 for 1 year. The highest is in Aush<alia, which requires US $400,000 of invest-ment, in addition to a US $8000 processing fee. Next for consideration are medical services, traffic condi-tions, the landscape, and the cultural content.
Japanese would list the following criteria for evaluation before deciding the long stay: Medical service, social stability, price of basic living, weather, food, language, a variety of options for sightseeing, living environment, interpersonal relationship (no prejudice for foreigners), ease of stay, and distance from the home country. Thailand provides very good service for long stay, including the following items: Application, rental houses, transportation from the airport, language translation service 24 hours a day, health examinations, arrangements for language learning and other activities, meeting people from other countries, helping to merge into local societies, introducing housekeepers who speak the mother tongue, and so forth.
Niche services strategies adopted by Asian countries
The literature includes 3 strategies: Cost leadership, differentiation, and focused cost leadership and differentiation strategies (Fig. 3).
Thailand offers the general advantage of low-cost labor. Therefore its strategy belongs to cost leadership lnt SUl'g 2010;95
;\!ICHE SERVICES FOR GLOBAL MEDICINE
Competitive advantage Cost leadership Differentiation
Fig. 3 Strategies for niche services.
on a grand scope. Thailand has 3 categories for its niche services in the study, and niche services in 111ailand have been changed over time from Category Ia and Category Ib to Category II and Category ill. Malaysia offers the general advantage of low-cost labor. Korea focuses on cosmetic surgery, 'ivhich is a lower-risk procedure when compared with the difficult proce-dures of open heart surgery performed in India.
India has adopted a differentiation str·ategy with a focus on open heart surgery and joint implants. Singapore shares this str·ategy. It seems better for Taiwan to follow the same policy as well, but it offers a low price difference at this time. Of course the market is dynamic, and a country can Inove from one strategy to another in the future, depend-ing on available resources.
Business model
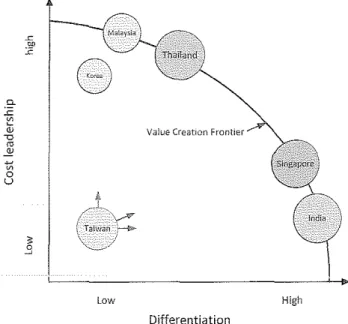
A business model is the combination of strategies used to gain competencies. It can be pursued through both differentiation (unique value to patients) and cost leadership (lower cost struchue). A business model that reaches the value creation frontier could achieve above average profitability. From the value creation frontier view, the niche services proposed by Asian countries will pursue different strategies (Fig. 4)20
Cluster of services
Regarding changes in the global medicine market, in 2008, the Asian countries with the largest revenues from global medicine were Thailand, India, Singa-pore, and Malaysia. If Taiwan is going to launch into this market, thorough study and careful planning should be done. The shortcomings of Taiwan are the lack of marketing and integration of business offered by the govermnent. Just to have high quality of health care is not enough-it must be recognized
lnt Surg 2010;95 CHEN ~ 00
"'
8
g."'
~:v
Value CreatIOn <0 ro .E! t: 0 u k /_.L" / "\..--# ( TaiwJn"'~,
'\.---~// .'l Low High Differentiation Fig. 4 Strategies proposed by Asiart countries.in the world. When language is a barrier, the target market can be defined as the Chinese-speaking population, hence to develop a niche service with attraction to that population.
Since December 15, 2005, large-scale communica-tion between Mainland and Taiwan has been initiated, and numerous tourists have corne to Taiwan for Sightseeing. However, only a fe'i"r have come for health care. Apparently lack of marketing and convenience is a problem, but language barrier is not an issue. Probably people from Hongkong and Macao should be defined as the first target market because of visa issuance and the price gradient. Creation of successful stories based on the niche service paves the way to marketing.
In Taiwan, medical travel is expected to be more important than medical tourisln. Various deformi-ties are far more obvious than disorders of internal organs such as those of the heart and brain. Therefore deformities of the body, such as craniofa-cial deformities and severe cases of lymphedema treated in hospitals in Taivlan, attract more attention and publicity. Successful stories apparently attract-ed a lot of attention after the spread of information through various mass media. They show the high standard of health care and increased cooperation among members of the hospitaL
Conclusion
From the successful stories, a nev·,r business can be established in the following order:
CHEN
Successful Story
For a country to develop Inedical tourism, the target market should be defined first based on the above considerations. Then try to design some-thing different, and propose a niche service (or services). Medical as well as nonmedical services should be emphasized at the same time. When hospitals in Asian countries build their business model, they Inay offer a cluster of services and maintain the business to gain a sustained compet-itive advantage.
References
1. Chambers D, McIntosh 8. Using authenticity to achieve competitive advantage in medical tourism in the English-speaking Caribbean. Third World Quarterly 2008;29(5):919-937
Cluster of Services
NICHE SERVICES FOR GLOBAL MEDICINE
Maintaining the Business
9. Huat JYC Medical tourism and Singapore. It, The International Hospital Fedemtioll Reference Book. Voltaire, France: The Intemational Hospital Federation, 2006/2007
10. Khan ZH, Hamidi S, Miri SM. Craniopagus, Laleh and Ladan twins, sagittal sinus. Turk Neurosurg 2007;17(1):27-32 11. Mahajan JIC, Kumar D, Deb M, Rao KLN. Asymmetric
conjoined hvins: atypical ischiopagus parasite. J Pediatr SlI1g
2002;37(10),e33
12. Ratan S, Rattan K, Magu S, Gupta S, Narang R, Arora B.
Thoracopagus parasites in tvvo sets of twins: evidence for the 'fusion theury.' Fnliult SUIX Illi 2008;24(11):1255-1259
13. Singh M, Singh KP, Shaligram P. Conjoined hvins cephalo-pagus Janiceps mOJlosymmetros: a case report. Birth Defects Res
Clin Mol Teratal 2003;67(4):268-272
14. Wong TG, Ong BC, Ang C Chee H-L. Anesthetic manage-ment for a five-day separation of craniopagus hvins. Allestil
Annlg 2003;97(4),999-1002
2. Connell J. Medical tourism: sea, sun, sand and Tourism Management 2006;27(6):1093-1100
surgery. 15. Burkett L. Medical tourism: concerns, benefits, and the
3. Hume LF, Demicco FJ. Bringing hotels to healthcare-a Rx for success. Journal of Quality Assurance in Hospitality and Tourism
2007;8(lP5-84
4. Pafford B. The third wave-medical tourism in the 21st century. Southem Medical J 2009;102(8):810--813
5. Smyth F. Medical geography: therapeutic places, spaces and networks. Progress ill Humlln Geography
2005;29(4):488-495
6. VVOOdmaI"l. J. Plltients Beyond Borders Taiwan Edition. Chapel Hill, NC: Healthy Travel Media, 2008
7. Page SJ. Current issue in tourism. The evolution of travel medicine research: a new research agenda for tourism? Tourism Management 2009;30(2):149-157
8. York D. Medical tourism: the trend tmvard outsourcing medical procedures to foreign cOlmtries. J Contin Educ Health Prof 2008;28(2),99-1 02
116
AInerican legal perspective. Tile journal of Legal Medicine
2007;28(2),223-245
16. Cossar JB, Reid D, Fallon RL Bell EL Riding MR Follett EA et al. A cumulative revie\v of studies on travellers, their experience of illness and the implications of these findings.
J Infect 1990;21(1)27-42
17. Page SJ, Meyer D. Tourist accidents: an exploratory analysis. Annals of Tourism Research 1996;23(3):666-690
18. Steffen R, Kollaritsch H, Fleischer K. Travelers' diarrhea in the new millennium: consensus among experts from German-speaking countries. J Travel Med 2003;10(1):38-45
19. Svantesson DJ8. From the airport to the surgery to the courtroom-private international lalv and medical tourism. Commonwealth Law Bulletin 2008;34(2):265-276
20. Hill C\-\/L, Jones GR. Strategic Management Theory: Ail
Integrated AppTOnch. 8th ed. Cincinnati, Ohio: South-Western Educational Publishing, 2007