DISPARITY OF MEDICAL CARE UTILIZATION AMONG
DIFFERENT HEALTH INSURANCE SCHEMES IN TAIWAN
SHOU-HSIA CHENG* and TUNG-LIANG CHIANG
Graduate Institute of Public Health and Center for Health Policy Research, National Taiwan University, College of Public Health, Taipei 10018, Taiwan
AbstractÐPotential excess use of health care services caused by insurance has been a major concern for almost every industrialized county. Moral hazard problems and fee-for-service payment methods are considered to be important factors for higher medical care utilization among those insured. Health care availability is another feature reportedly associated with health care use. Using the data from a National Health Interview Survey in Taiwan in 1990, this study examined dierences in medical care utilization by bene®ciaries under three major social insurance plans (i.e. Labor Insurance-LI, Govern-ment Employees' Insurance-GEI, and Farmers' Insurance-FI) which covered about half the population at that time. Logistic and Poisson regression models were applied to examine the eects of relevant fac-tors on the probability and volume of physician visits. Results from the analyses revealed that (1) per-sons with dierent insurance plans had a similar higher probability of seeing a doctor than the uninsured, with the odds ratios ranged from 1.8 to 2.0. Also (2) the LI/FI participants consumed 60± 73% more physician services than the uninsured, while the GEI enrollees utilized only 30% more phys-ician services. Findings from our study concerning the access and use of physphys-ician services in dierent insurance plans provide some useful information for reforming a health care delivery system. # 1998 Elsevier Science Ltd. All rights reserved
Key wordsÐhealth insurance, physician services, availability of providers
INTRODUCTION
The theoretical base for the excess use of medical care services induced by health insurance is the so-called ``moral hazard'' problem. Basically, it is an extension of the Law of Demand Ð when price goes down, consumption goes up. When a person enrols in an insurance plan, the real price to him/ her for medical care services decreases (while the insurance premium becomes sunk cost to him/her), and the consumption may increase (Feldstein, 1988). The eects of insurance on health care utiliz-ation have been well investigated. The Rand Health Insurance Experiment, a remarkable study on this issue, reported that insurance has removed the ®nancial barrier to health care, and increased the use of care in proportion to the level of free care (Manning et al., 1987). Many researchers made the same conclusion that insurance coverage increased the use of health care, including physician visits and admission to hospitals (Hillman et al., 1989; Davis, 1991; Trevino et al., 1991; Stearns et al., 1992; Hafner-Eaton, 1993; Hanh, 1994). People without health insurance have a higher denial rate in seeking health care (Saver and Peterfreund, 1993; Lieu et al., 1993).
Another theory for the increase in medical care use is the supplier-induced demand (or utilization). This hypothesis reveals that patients are relatively
innocent due to the asymmetry of information. Physicians may induce the consumption of medical care for their own bene®ts instead of the patients' (Folland et al., 1993; Wennberg et al., 1982). Traditional fee-for-service plans provide incentives for physicians to provide more services to insurance enrollees. Capitation-based reimbursement methods had been introduced in response to the potential abuse caused by the fee-for-service based reimburse-ment. A recent review by Miller and Luft (1994) reports that HMO participants use more oce visits and less hospital admissions, compared with those in fee-for-service plans. Hence, the medical care cost is lower for HMO enrollees than their fee-for-service counterparts. Shifting the ®nancial risk from consumers to providers is the key feature. Removing the incentive of providing more (expens-ive) health care, i.e. supplier-induced demand, is the most signi®cant factor for these ®ndings.
Availability of health care providers is another issue in health care utilization. Rural residence and geographical availability of medical care has been reported to be associated with the use of health care services. It is generally concluded that urban area residents consume more services, and distance to a regular source of care is an important factor aecting the use of health care (Gesler and Meade, 1988; Cunningham and Cornelius, 1995; Love and Lindquist, 1995). However, lots of the geographical studies focused on the measurement issues of
dis-# 1998 Elsevier Science Ltd. All rights reserved Printed in Great Britain 0277-9536/98 $19.00 + 0.00
PII: S0277-9536(98)00103-8
*Author for correspondence.
tance-to-care rather than the availability of health care providers (Gesler, 1986). In Taiwan, health care services were provided to insurance bene®ci-aries through insurance-contracted providers, prior to the implementation of National Health Insurance (NHI) in March 1995. Dierent insur-ance plans had various contracted health care pro-viders. The present study explored the insurance eect on the use of ambulatory care, within a unique situation where dierent types of insurance had a dierent level of availability of (contracted) health care providers. It is hypothesized that limited availability of providers may curb the insurance-induced medical care utilization.
HEALTH INSURANCE IN TAIWAN
Taiwan is a small island of 36,000 km2, of which
two-thirds is mountainous with few residences. In 1990, there were 21 million people, with about 19,900 western physicians (in addition to Chinese doctors) in 741 hospitals and 7221 clinics (Department of Health, 1994). All 365 townships, except ®ve in remote mountain areas had at least one practicing physician. Most hospitals were close-system based, i.e. physicians were hired as full-time employees in hospitals and were mainly paid sal-aries plus a performance bonus. Each of the hospi-tals had a substantial outpatient department. Clinic physicians were self-employed and totally indepen-dent from hospitals. Average household annual income was about 580,000 NT Dollars (Dept. of Budget, Account and Statistics, 1990) in Taiwan, with 1 U.S. dollar being equal to 27 NT dollars. The national health care expenditure was about 4% of the GDP. Generally speaking, in 1990 a person conducted 9 physician visits per year in Taiwan (Lin et al., 1991).
Three major types of social health insurance sys-tems existed prior to the implementation of National Health Insurance plan on March 1, 1995. They were labor insurance (LI) which was mainly for private sector working employees, government employees' insurance (GEI), for all governmental employees and retirees, and farmers' insurance (FI) for all farmers. These three insurance types covered about one half of the total Taiwan population in 1990 (Lin et al., 1991; Department of Health, 1994). Children, students at school, housekeepers and the elderly were the main components of the uninsured population. Patient bene®ts of medical care services, including ambulatory care, hospital in-patient care and prescription drugs, were very similar under the three insurance plans. Instead of co-payment requirements, insurance bene®ciaries had to pay a ®xed ``registration fee'' (i.e. 50 NT dollars) for each visit. Patients with no insurance coverage had to pay the full price (usually around NT$ 300±400) out of pocket.
Premiums, payment method to providers, and medical care delivery for the Labor Insurance and Farmers' Insurance bene®ciaries were basically simi-lar. All administrative procedures for the FI were handled by the LI system. About 80% of hospitals and 47% of clinics were contracted with labor/ farmers' insurance. This ®gure accounted for 67% of all western physicians in Taiwan (Department of Health, 1994; Bureau of Labor Insurance, 1994). The LI/FI participants might receive physicians' services in these contracted hospitals' outpatient departments, or in contracted clinics. Contracted health care providers were reimbursed on a fee-for-service basis with the collected ``insurance coupons'' which were handed by the LI/FI patients, after receiving medical services.
On the other hand, government employees' insur-ance had its own health care delivery system. About 38% of all western physicians in Taiwan were con-tracted providers for the GEI enrollees. Sixty-one percent of the hospitals and less than 6% of clinics contracted with the GEI (Central Trust of China, 1994). The GEI also owned six clinical centers (the Government Employees Clinical Centers) in ®ve metropolitan areas in Taiwan. Physicians from large hospitals were selected to provide scheduled primary care services in the six clinical centers. These doctors were paid ®xed wages for each ses-sion in the clinical centers. Other physician services provided in contracted hospitals' OPDs or clinics were paid on a fee-for-service basis, similar to the LI/FI system. Approximately 40% of the primary care services were provided to the GEI enrollees by physicians in the six clinical centers in 1990 (Central Trust of China, 1994). A detailed descrip-tion of Taiwan's health care system is available else-where (Peabody et al., 1995).
Major dierences between the LI/FI plans and the GEI plan were: (1) the LI/FI system paid their contracted providers on a fee-for-service basis; the GEI system used a mixed payment method; (2) the availability of health care providers were dierent, with 67% vs 38% of all physicians contracted for these two systems respectively; (3) the GEI bene®ci-aries received primary ambulatory care only from physicians in the GEI clinical centers, or from con-tracted providers, before any referral could be made; this was not required for the LI/FI members. In consequence, in comparison to the LI/FI partici-pants, seeking health care was less convenient and the freedom of choosing physicians was more lim-ited for the GEI enrollees.
MATERIAL AND METHODS
Data source and variables
Data for this study came from a National Health Interview Survey in Taiwan. A total of 1193 house-holds were selected, via strati®ed random sampling,
as the target sample. Face-to-face interviews were conducted between May and August in 1990. A total of 1031 households with 4196 people of all ages were interviewed successfully, with a response rate of 86.4%. This study sample was nationally representative (Lin et al., 1991). The majority of the failed cases were due to ``moving out'' and ``wrong address''; the ``refused to answer'' cases accounted for 6.6% of the target sample. Of the interviewed subjects, 2664 adults aged 20 or over were included in the analysis, because most persons aged under 20 had no health insurance coverage in 1990.
Andersen's medical care utilization model was employed in the study (Aday and Andersen, 1974). Use of health care is aected by several factors such as individual demographic features, enabling factors, and need characteristics. Health insurance status was classi®ed into four groups: labor insur-ance, government employees' insurinsur-ance, farmers' insurance and the uninsured. Three dummy vari-ables were created for the three insured status groups, while the uninsured was the reference. Dependent variables were the use of physician ser-vices (seeing a doctor or not), and the frequency of physician visits in the past two weeks. Visits to the emergency room in the hospitals was not included in the analysis. Ambulatory care referred to phys-ician visits in clinics or outpatient departments in hospitals. Information on other correlated variables according to the Andersen model was also collected. Basic demographic characteristics included age, sex and education. Enabling factors included family income, family size, regular source of care, and urbanization of residence. Need indicators were rep-resented by self-reported health status, and phys-ician-diagnosed chronic conditions.
Measurement of the study variables is brie¯y described as follows. While using dummy variables in the analyses, we coded the event as 1 and the reference group as 0. Age was divided into three groups, and two dummy variables were used to rep-resent the younger group of ages 20±44 and the middle age group of 45±64, while the older group was the reference. Education was represented by a dummy variable which was assigned 1 if a person attended high school or above, or else 0. A dummy variable was used to indicate a low income family, with less than 20,000 NT dollars (U.S. $740) per month, which represented approximately the lower 20% of all families. Large family size was rep-resented by a dummy variable, with family members equal to 4 or more. The de®nition of a rural area was modi®ed from the Taiwan Standard Classi®cation Report in 1990 (Directorate-General of Budget, Accounting and Statistics, 1993). A chronic condition was coded 1, if an individual reported any of the following nine physician-diag-nosed disorders: hypertension, heart diseases, stroke, diabetes, gastrointestinal ulcer, liver diseases, bronchitis, kidney disorders, and arthritis. Perceived
health status was classi®ed into three groups, i.e. good, fair, and poor health. Two dummy variables were created for the fair and the poor groups while the good health group was the reference.
Statistical models
An alternative statistic model was conducted to examine the eect of health insurance on the use of physician services. Frequently, multiple logistic re-gression is employed to investigate the probability of health care utilization. Although the odds ratio of seeking health care may be estimated, the dis-parity of the quantity of the utilization between groups could not be assessed. A traditional re-gression model is often conducted to estimate the increase of health care utilization caused by health insurance. Sometimes, a two-part model is used to deal with this situation. In this model, logistic re-gression is performed for all subjects ®rst, then ordinary or weighted least square estimates are used for those who have had any physician visits (Kobashigawa and Berki, 1977; Manning et al., 1981; Nolan, 1993). It was noted that ambulatory care usage in a certain period of time should not be treated as continuous numbers; instead it would be more appropriate to be treated as counts. In our study, many subjects had no physician visits in the study period. Therefore, in addition to logistic re-gression, Poisson regression with a log link function was used in the study to estimate the eects of par-ticular factors on the magnitude change of phys-ician services utilization. Although a physphys-ician visit may not be independent from the previous visit by the same person, which does not ®t the Poisson dis-tribution, Cameron and Trivedi (1986) found that ``the major impact of the distribution assumption is on estimated variances rather than point estimates of parameters''.
An overdispersion problem was found in this study's Poisson regression model which indicated that the dispersion estimate was greater than 1 in the model. Using the SAS ``genmod procedure'', we speci®ed the square root of model deviance divided by degree of freedom, as an estimate of the scale parameter (rather than the unity) in order to adjust the overdispersion (SAS Institute, 1993). This adjustment basically would not aect the model parameter estimate values, yet the covariance matrix would be enlarged. Hence the standard errors of the parameter estimates would be increased, which would make the parameter esti-mates less likely to be signi®cant. Furthermore, we preferred to use 1% probability level as a cuto point for de®ning statistical signi®cance because of the large sample size.
While interpreting the results from logistic re-gression, we assumed that using physician services or not was mainly initiated by the patients rather than the physicians. Under this assumption, the problem of supplier-induced demand might be less
severe. On the other hand, the number of visits (if greater than 1) in two weeks could be heavily in¯u-enced by the physician, e.g. repeated visits required by physicians. When the ``number of physician vis-its'' was treated as a dependent variable in the Poisson regression, the eects of independent vari-ables might be contaminated by the in¯uence of physicians Ð the health care providers. This idea should be born in mind.
RESULTS
Description of sample characteristics
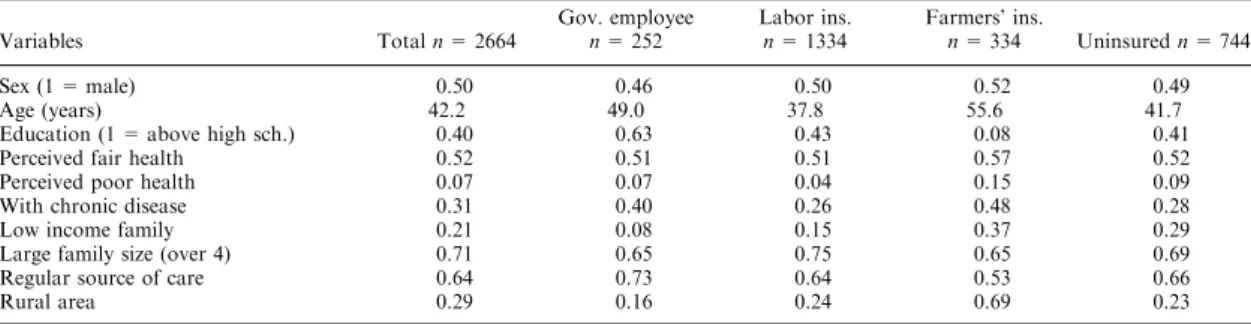
The essential description of the sample is listed in Table 1. The male to female ratio was 1.0 for this sample. The mean age was about 42 years old. Forty percent of the subjects attended high school or above (greater than 9 years schooling). Among these adults, only 7% of them reported poor per-ceived health; 41% and 52% of the individuals reported good and fair health status, respectively. About 31% of the sample had physician-diagnosed chronic disorders. Twenty-one percent of the indi-viduals came from low income families, and 71% of the subjects lived in large families. Sixty-four per-cent of the sample had a regular source of care. About 29% of the individuals lived in rural areas.
While comparing the basic distribution among in-dividuals with the four types of insurance status, we noticed several obvious dierences. First, farmers' insurance enrollees were the oldest group with a mean age of 56, while the labor insurance enrollees were the youngest, with a mean age of 38. Second, the education level was extremely low for the FI enrollees with only 8% of the persons having attended high school or above. Third, the FI enrol-lees had the highest percentage (15%) of perceived poor health and the highest percentage (48%) with chronic conditions. Fourth, only 8% of the govern-ment employees insurance enrollees came from low income families, while 37% of the FI enrollees came from low income families. Finally and natu-rally, most of the FI enrollees (69%) lived in rural areas. According to our knowledge, the uninsured group included house-keeping females, self-employed businessmen, college students, unem-ployed persons, and the retired elderly. Health
insurance status and these relevant factors were considered to be associated with the use of phys-ician services.
Physician services utilization
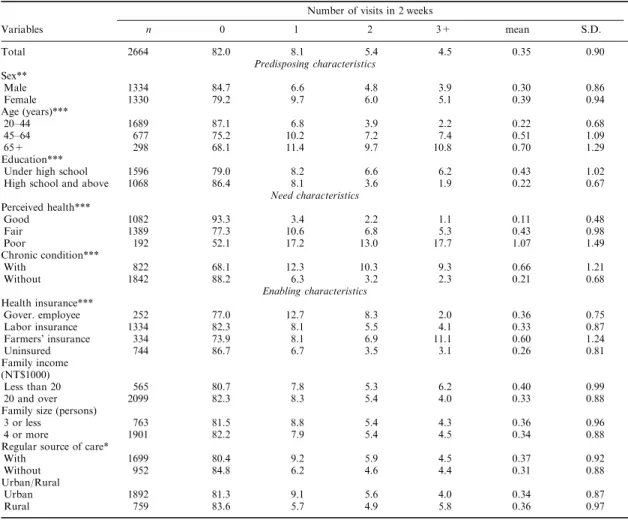
Utilization of ambulatory care in the past two weeks in terms of the number of physician visits is presented in Table 2. The overall mean number of physician visits was 0.35 for the sample, with 82% of them not seeing a doctor at all in the two weeks prior to the interview. As expected, we found that insured people consume more physician services than the uninsured. Government employees had the highest percentage for seeing the doctor once (12.7%), but FI enrollees had the highest percen-tage for seeing a doctor three times or more (11.1%). The mean number of physician visits for the insured ranged from 0.33 to 0.60; it was only 0.26 for the uninsured. The dierences in utilization among these four insurance groups were statistically signi®cant at the p < 0.001 level.
Females were more likely to see a doctor as well as to have more physician visits than males. A typi-cal trend of utilization was observed among three age groups with means of 0.22, 0.51, and 0.70, re-spectively, for the young, middle and old age groups. People with a higher education used less physician services than their counterparts. Need characteristics were found to be signi®cantly associ-ated with use of ambulatory care. Eighteen percent of those with a poor health status had visited their physicians three times or more in the last two weeks. On the contrary, only about 1% of those with good health used as many physician services. People with chronic conditions consumed three times as many physician services as those without chronic conditions (0.66 visits vs 0.21 visits). Those who had a regular source of care used more phys-ician services than their counterparts. Family income and family size were not found to be signi®-cantly associated with ambulatory care utilization. Adjusted eects on physician services utilization
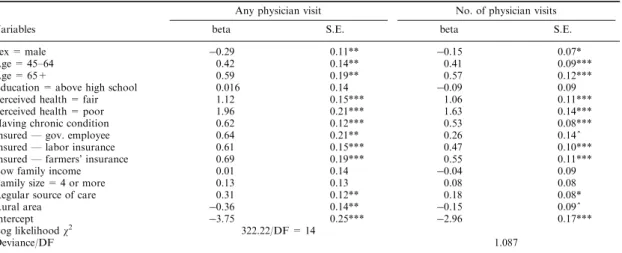
Results from the logistic regression model for examining the insurance eects on the probability of seeing a doctor, and from the Poisson regression model for evaluating the eects on the quantity of
Table 1. Means for independent variables by types of insurance for adults over 20 in Taiwan
Variables Total n = 2664 Gov. employeen = 252 Labor ins.n = 1334 Farmers' ins.n = 334 Uninsured n = 744 Sex (1 = male) 0.50 0.46 0.50 0.52 0.49 Age (years) 42.2 49.0 37.8 55.6 41.7 Education (1 = above high sch.) 0.40 0.63 0.43 0.08 0.41 Perceived fair health 0.52 0.51 0.51 0.57 0.52 Perceived poor health 0.07 0.07 0.04 0.15 0.09 With chronic disease 0.31 0.40 0.26 0.48 0.28 Low income family 0.21 0.08 0.15 0.37 0.29 Large family size (over 4) 0.71 0.65 0.75 0.65 0.69 Regular source of care 0.64 0.73 0.64 0.53 0.66 Rural area 0.29 0.16 0.24 0.69 0.23
physician services, are presented in Table 3. We found that after controlling other factors in the model, the two need factors (perceived health and having chronic disorders), two predisposing factors (age and sex), and three enabling factors (insurance, regular source of care, and urban/rural area) were associated with the likelihood of seeing a doctor. Most of these factors were also observed to be cor-related with the quantity of use of physician ser-vices.
The eect of health insurance on the probability of visiting a physician was obvious, with parameters estimated around 0.61 to 0.69, and p < 0.001. The odds ratios of seeing a doctor for the three types of insured individuals (LI, GEI, or FI) to the unin-sured were close to each other, at around 1.8 to 2.0. However, the eects on the quantity of physician visits used by enrollees, for the three types of insur-ance, were dierent. Farmers' insurance enrollees consumed 73% more physician services than the uninsured (beta = 0.55, the odds = 1.73 since the log link function was used). Labor Insurance par-ticipants used 60% more services (beta = 0.47, the odds = 1.60) than the uninsured. Both FI and LI
eects were statistically signi®cant at the p < 0.001 level. Conversely, the GEI bene®ciaries utilized only 30% more physician services (beta = 0.26, the odds = 1.30), than the uninsured and the eect was not statistically signi®cant.
Both needs indicators, perceived health and chronic conditions, had the most obvious eects on physician services utilization in the models. Results from the logistic regression showed that the odds ratio of seeing a doctor was 3.1 (beta = 1.12) for the fair health group and 7.1 (beta = 1.96) for the poor health group to the good health group, with p < 0.001. Results from the Poisson regression revealed that after controlling demographic and enabling factors in the model, the needs character-istics had very signi®cant in¯uence on the quantity of ambulatory care use. The poor health group uti-lized about 5.1 times the physician services, and the fair health group consumed about 2.9 times more physician services, than the good health individuals. This ®nding highlighted the fact that health need was a critical determinant of the use of physician services, which is common sense and should not be ignored. Results for most of the other controlling
Table 2. Frequency distribution (%) and mean numbers of physician visits by studying variables Number of visits in 2 weeks
Variables n 0 1 2 3+ mean S.D. Total 2664 82.0 8.1 5.4 4.5 0.35 0.90 Predisposing characteristics Sex** Male 1334 84.7 6.6 4.8 3.9 0.30 0.86 Female 1330 79.2 9.7 6.0 5.1 0.39 0.94 Age (years)*** 20±44 1689 87.1 6.8 3.9 2.2 0.22 0.68 45±64 677 75.2 10.2 7.2 7.4 0.51 1.09 65+ 298 68.1 11.4 9.7 10.8 0.70 1.29 Education***
Under high school 1596 79.0 8.2 6.6 6.2 0.43 1.02 High school and above 1068 86.4 8.1 3.6 1.9 0.22 0.67
Need characteristics Perceived health*** Good 1082 93.3 3.4 2.2 1.1 0.11 0.48 Fair 1389 77.3 10.6 6.8 5.3 0.43 0.98 Poor 192 52.1 17.2 13.0 17.7 1.07 1.49 Chronic condition*** With 822 68.1 12.3 10.3 9.3 0.66 1.21 Without 1842 88.2 6.3 3.2 2.3 0.21 0.68 Enabling characteristics Health insurance*** Gover. employee 252 77.0 12.7 8.3 2.0 0.36 0.75 Labor insurance 1334 82.3 8.1 5.5 4.1 0.33 0.87 Farmers' insurance 334 73.9 8.1 6.9 11.1 0.60 1.24 Uninsured 744 86.7 6.7 3.5 3.1 0.26 0.81 Family income (NT$1000) Less than 20 565 80.7 7.8 5.3 6.2 0.40 0.99 20 and over 2099 82.3 8.3 5.4 4.0 0.33 0.88 Family size (persons)
3 or less 763 81.5 8.8 5.4 4.3 0.36 0.96 4 or more 1901 82.2 7.9 5.4 4.5 0.34 0.88 Regular source of care*
With 1699 80.4 9.2 5.9 4.5 0.37 0.92 Without 952 84.8 6.2 4.6 4.4 0.31 0.88 Urban/Rural Urban 1892 81.3 9.1 5.6 4.0 0.34 0.87 Rural 759 83.6 5.7 4.9 5.8 0.36 0.97 *p < 0.05. **p < 0.01. ***p < 0.001 based on w2test.
variables, such as age, sex, regular source of care, and urbanization, were similar to those reported in previous studies (Lin et al., 1991; Trevino et al., 1991; Lieu et al., 1993; Hanh, 1994).
DISCUSSION
Consistent with the ®ndings of previous studies, this study demonstrates that health insurance increases the probability, as well as the quantity, of physician visits. The three health insurance plans (LI, GEI, FI) had a similar eect on the likelihood of seeing a doctor. After controlling other factors in the models, we found that the odds ratio of visiting a doctor was about 1.8 to 2.0 for the insured to the uninsured. As we mentioned earlier, ``seeing a doctor or not'' was mainly decided by the consumer rather than the provider. The ®ndings revealed that no dierence in the likelihood of physician visit was observed among bene®ciaries under the three insur-ance schemes.
On the other hand, the number of physician visits utilized by the LI/FI enrollees was higher than that of the GEI participants. The LI/FI bene®ciaries consumed 60±73% more ambulatory care than the uninsured. Yet, the GEI members utilized only 30% more services. We wondered why the GEI enrollees did not ``use up'' the physician services as did other insured persons. What were the possible explanations? Major factors concerning dierences among the bene®ciaries' characteristics such as age, perceived health, and chronic diseases were included in the model, with signi®cant eects on the amount of physician visits. Three alternative explanations were considered: level of convenience (availability of providers), ®nancial incentives of providers due to payment methods, and quality of care.
Since limited freedom of choice and referral are prevalent in many countries (OECD, 1994), dis-parity of the availability of health care provision was the ®rst reason we thought of. The contracted health care providers for the GEI were very limited. Only 38% of all physicians in the Taiwan area were their contracted providers and many of the phys-icians were working in hospitals. On the contrary, 67% of physicians were contracted with the LI/FI system. In addition, there was a referral require-ment for GEI bene®ciaries to obtain more advanced examination or treatment. Limited availability of health care providers (which implies some spatial inconvenience and less freedom in provider selec-tion) could partially account for fewer physician visits by GEI members than LI/FI enrollees.
Financial incentives for medical care providers could be another in¯uencing factor. We noted ear-lier that the LI/FI contracted health providers col-lected ``insurance coupons'' and were reimbursed on a fee-for-service basis. This payment method pro-vided incentives for physicians to see more patients, or to see a patient many times, in order to collect more coupons. Conversely, the GEI contracted physicians who saw patients in the six GEI clinical centers were paid ®xed wages. This payment method might limit or prevent unnecessarily repeated visits to physicians in the six GEI clinical centers.
The third alternative explanation is that quality of care to the GEI bene®ciaries could be better than that to other programs' participants. Most of the GEI contracted providers were large (teaching) hospitals with good reputations. Although we had no indicators on quality of medical care, we did have a variable from the survey on overall satisfac-tion with medical care services. We found no dier-ences in levels of satisfaction with medical care
Table 3. Results of ambulatory care utilization from logistic and Poisson regression models Any physician visit No. of physician visits
Variables beta S.E. beta S.E.
Sex = male ÿ0.29 0.11** ÿ0.15 0.07* Age = 45±64 0.42 0.14** 0.41 0.09*** Age = 65+ 0.59 0.19** 0.57 0.12*** Education = above high school 0.016 0.14 ÿ0.09 0.09 Perceived health = fair 1.12 0.15*** 1.06 0.11*** Perceived health = poor 1.96 0.21*** 1.63 0.14*** Having chronic condition 0.62 0.12*** 0.53 0.08*** Insured Ð gov. employee 0.64 0.21** 0.26 0.14^ Insured Ð labor insurance 0.61 0.15*** 0.47 0.10*** Insured Ð farmers' insurance 0.69 0.19*** 0.55 0.11*** Low family income 0.01 0.14 ÿ0.04 0.09 Family size = 4 or more 0.13 0.13 0.08 0.08 Regular source of care 0.31 0.12** 0.18 0.08* Rural area ÿ0.36 0.14** ÿ0.15 0.09^ Intercept ÿ3.75 0.25*** ÿ2.96 0.17*** Log likelihood w2 322.22/DF = 14
Deviance/DF 1.087
Omitted group is aged 20±44, with good perceived health, and uninsured. ^p < 0.10.
*p < 0.05. **p < 0.01. ***p < 0.001.
services between GEI and LI/FI bene®ciaries with 43.2% satis®ed, 50.8% fairly satis®ed, and 6.0% dissatis®ed among the former and 41.1% satis®ed, 53.7% fairly satis®ed, and 5.2% dissatis®ed among the later two.
Family income was reported to be an important factor associated with health care utilization (Hafner-Eaton, 1993; Saver and Peterfreund, 1993; Freeman, 1993; Cunningham and Cornelius, 1995). Yet low income was not found to be signi®cant in our physician services regression model, which is worth explanation. In 1990, the average charge for physician services was about 300±400 NT dollars or about 11±15 U.S. dollars per visit, which was rela-tively inexpensive compared to the monthly income of 740 U.S. dollars for lower income families in Taiwan. The aordable cost could be the most im-portant reason for this ®nding concerning the family income eect. Rural residence was not expected to be a signi®cant factor in¯uencing the use of physician services, because Taiwan is a small island with a crowded population. Generally speak-ing, except for the remote mountain areas or o-shore islets, it was not too inconvenient for consu-mers to access their doctors. However, we still found that people living in rural areas were less likely to see a doctor.
The problem of ``moral hazard'' indicated by the excess use of medical care by insured persons is always hard to identify, since it is dicult to know what amount of services is appropriate for a patient under certain situations. Results from this study revealed that even with the inexpensive cost of physician services, dierences of medical care utiliz-ation existed between the insured and uninsured. Limiting the availability of health care provision, accompanied by mixed payment to physicians (i.e. fee-for-service and ®xed wages), may alleviate the higher utilization among the insured population, as the case of GEI illustrates. In a low-income country with relatively insucient medical care resources and little public or private insurance, limiting the availability of physicians may result in declining the utilization of medical care services. Nevertheless, while health care cost-containment is one major task for every industrialized country and many middle-income developing countries which are expanding insurance coverage, results from our study concerning the access and use of physician services in dierent insurance plans, provide useful information for reforming a health care delivery system.
AcknowledgementsÐThis study is supported in part by grants from the Department of Health (DOH84-HR-305) and from the National Science Council (NSC85-2417-H002-018) in Taiwan. The authors owe thanks to Drs F. C. Hu and C. H. Hsiao for their advice on the use of Poisson regression model. The reviewer's helpful com-ments are also appreciated.
REFERENCES
Aday, L. A. and Andersen, R. M. (1974) A framework for the study of access to medical care. Health Serv. Res. 9, 208.
Bureau of Labor Insurance for Taiwan-Fukien Area (1994). Statistical Data for Taiwan-Fukien Area Labor Insurance, p. 372. Taipei, Republic of China.
Cameron, A. C. and Trivedi, P. K. (1986) Econometric models based on count data: Comparisons and appli-cations of some estimators and tests. J. Applied Econometrics 1, 29.
Central Trust of China (1994). Statistical Data for Government Employees' Insurance, p. 474. Taipei, Central Trust of China, Republic of China.
Cunningham, P. J. and Cornelius, L. J. (1995) Access to ambulatory care for American Indians and Alaska natives; the relative importance of personal and commu-nity resources. Soc. Sci. Med. 40, 393.
Davis, K. (1991) Inequality and access to health care. Milbank Q. 69, 253.
Department of Budget, Account and Statistics (1990). Report on the Survey of Family Income and Expenditure Taiwan Province, p. 20. Taichung, Department of Budget, Account and Statistics, Taiwan Provincial Government, Republic of China.
Department of Health (1994). Health and Vital Statistics: General Health Statistics, p. 126. Taipei, Department of Health, Executive Yuan, Republic of China.
Directorate-General of Budget, Accounting and Statistics (1993). Standard Classi®cation for Statistical Areas. Taipei, Directorate-General of Budget, Accounting and Statistics, Executive Yuan, Republic of China.
Feldstein, P. (1988). Health Care Economics, 3rd edn. John Wiley and Sons Inc., New York.
Folland, S., Goodman, A. C. and Stano, M. (1993). The Economics of Health and Health Care, p. 204. Macmillan Publishing Co., New York.
Freeman, H. E. (1993) Insurance status and access to health services among poor persons. Health Serv. Res. 28, 531.
Gesler, W. M. (1986) The use of spatial analysis in medi-cal geography: A review. Soc. Sci. Med. 23, 963. Gesler, W. M. and Meade, M. S. (1988) Locational and
population factors in health care-seeking behavior in Savannah, Georgia. Health Serv. Res. 23, 443.
Hafner-Eaton, C. (1993) Physician utilization disparities between the uninsured and insured. Comparison of the chronically ill, acutely ill, and well nonelderly popu-lations. JAMA 269, 787.
Hanh, B. (1994) Health care utilization: The eect of extending insurance to adults on Medicaid or uninsured. Med. Care 32, 227.
Hillman, A. L., Pauly, M. V. and Kerstein, J. J. (1989) How do ®nancial incentives aect physicians' clinical decisions and the ®nancial performance of health main-tenance organization? N. Engl. J. Med. 321, 86. Kobashigawa, B. and Berki, S. E. (1977) Alternative
re-gression approaches to the analysis of medical care sur-vey data. Med. Care 15, 396.
Lieu, T. A., Newacheck, P. W. and McManus, M. A. (1993) Race, ethnicity, and access to ambulatory care among U.S. adolescents. Am. J. Public Health 83, 960. Lin, R. S., Chiang, T. L., Hong, Y. T. and Chang, M. C.
(1991). The Planning and Experience of the National Health Survey 1990. Final Report to the DOH, Executive Yuen, Taipei.
Love, D. and Lindquist, P. (1995) The geographical acces-sibility of hospitals to the aged: A geographic infor-mation systems analysis within Illinois. Health Serv. Res. 29, 629.
Manning, W. G., Morris, C. N., Newhouse, J. P., et al. (1981) A two-part model of the demand for medical
care: preliminary results from the Health Insurance Study. In Health, Economics, and Health Economics, eds. J. van der Gaag, M. Perlman. North-Holland, Amsterdam.
Manning, W. G., Newhouse, J. P., Duan, N., Keeler, E. B., Leibowitz, A. and Marquis, M. S. (1987) Health insurance and the demand for medical care: Evidence from a random experiment. Am. Econ. Rev. 77, 251. Miller, R. H. and Luft, H. S. (1994) Managed care plan
performance since 1980. A literature analysis. JAMA 271, 1512.
Nolan, B. (1993) Economic incentives, health status and health services utilization. J. Health Econ. 12, 151. OECD (1994). The Reform of Health Care System: A
Review of Seventeen OECD Countries. OECD, Paris. Peabody, J. W., Yu, J. C.-I., Wang, Y.-R. and Bickel, S.
R. (1995) Health system reform in the Republic of China: Formulating policy in a market-based health sys-tem. JAMA 273, 777.
SAS Institute (1993). SAS Technical Report P-243. SAS/ STAT Software: The GENMOD procedure, p. 20, 32. SAS Institute, Inc., Cary, NC.
Saver, B. G. and Peterfreund, N. (1993) Insurance, income, and access to ambulatory care in King County, Washington. Am. J. Public Health 83, 1583.
Stearns, S. C., Wolfe, B. L. and Kindig, D. A. (1992) Physician responses to fee-for-service and capitation payment. Inquiry 29, 416.
Trevino, F. M., Moyer, M. E., Valdez, R. B. and Stroup-Benham, C. A. (1991) Health insurance coverage and utilization of health services by Mexican Americans, Mainland Puerto Ricans, and Cuban Americans. JAMA 265, 233.
Wennberg, J. E., Barnes, B. A. and Zubko, M. (1982) Professional uncertainty and the problem of supplier-induced demand. Soc. Sci. Med. 16, 811.