Anti-inflammatory and Structure-protective Effects of Hyaluronans:
Are These Effects molecular weight dependent?
Teng-Le Huang, MD, PhD1,2; Horng-Chaung Hsu, MD1;Chun-Hsu Yao, PhD3; Yueh-Sheng Chen, PhD4; Jeff Wang, PhD5
1 Department of Sports Medicine, College of Health Care, China Medical University,
Taichung 404, Taiwan.
2 Institute of Biomedical Engineering, College of Medicine and College of
Engineering, National Taiwan University, Taipei, Taiwan, ROC.
3 Chair and Professor, Department of Biomedical Imaging and Radiological Science,
China Medical University, Taichung, Taiwan, ROC.
4Lab of Biomaterials, School of Chinese Medicine, China Medical University,
Taichung, Taiwan
5Metal Industry Research & Development Center, Lujhu Township, Kaohsiung,
Taiwan.
Correspondence to: Teng-Le Huang, MD, PhD. Department of Sports Medicine,
College of Health Care, China Medical University, Taichung 404, Taiwan. No.91 Hsueh-Shih Road,Taichung, Taiwan 40402, R.O.C. Phone: 886-4-2205-2121
ext.5052; Fax: 886-4-2233-8592; E-mail: [email protected]. Running title: Role of MW in different effects of HA
Abstract
Although hyaluronans (HA) has been proved to be effective in the treatment of patients with osteoarthritis and rheumatoid arthritis, the correlations between these effects and the molecular weight (MW) of HA have not been systematically followed. Many different HA preparations are now applied worldwide in clinical usage. Their molecular weights are very wide ranged (500-6000 kDa). No systematic review especially addresses on the role of HA’s MW in the effects of anti-inflammation and structure-protection. This study evaluates the literatures of the basic and clinical studies on biological, pathological, and clinical effects of different MW HA. Databases were searched through PubMed (period 1978-2009), using the terms hyaluronan, hyaluronic acid, arthritis, and molecular weight. Reference lists of relevant articles were controlled for additional references. We define the “high” MW as MW greater than 2000 kDa and define the “low” MW as MW less than 2000 kDa in the current study. Most data that support the structure-protective effect of HA are from the studies with low MW HA. On the other hand, the majority of data that recommend the anti-inflammatory effect of HA are from the reports of high MW HA. In conclusion, we suggested that the effects of LMW HA were more
structure-protective and those of HMW HA were more anti-inflammatory. Keyword: Hyaluronans, Inflammatory, Molecular weight, Structure-protective
1. Introduction
Hyaluronic Acid (HA), or Hyaluronan, a linear glycosaminoglycan consisting of alternating disaccharide unit structure of D-glucuronic acid and N-acetyl-glucosamine, is a main component of synovial joint fluids and the extracellular matrix of articular cartilage.1,2 (Figure 1) On the level of molecular biology, HA is manufactured by a group of integral membrane proteins called hyaluronan synthases (HAS). Three human HA synthase (HAS 1, HAS 2 and HAS3) genes have been cloned.3HA with higher molecular weight (2 x 106 Da) is synthesized by HAS 1 and HAS 2, whereas HA with lower molecular weight (2-3 x 105Da) is synthesized by HAS 3.4 Regarding the degradation of HA, a class of enzymes named hyaluronidases (HYAL) are
involved. Up to now, six associated genes, including HYAL1, HYAL2, HYAL 3, HYAL
4, PH-20/SPAM1, and HYALP1 are cloned in human.5
Nonsurgical treatments for osteoarthritis (OA) may be characterized as
symptom-modifying or disease-modifying drugs. As defined by the Osteoarthritis Research Society (OARS), disease-modifying drugs are those that are intended to prevent, retard, stabilize, or reverse development of the morphological changes of OA.6Hyaluronan has been proven to be a safe and effective symptom-modifying treatment for OA of the knee, in terms of significantly reducing pain and improving function.7-10 The original concept for viscosupplementation with HA was based on the
hypothesis that HA could help fluid replacement and restore the visco-elasticity of the synovial fluid.11 However, the fact that all injected HAs are gone within days12 and yet the clinical benefit lasts for months suggests that there may be the other
mechanism through which HAs mediate their clinical benefit. It is now believed that biologic activation of multiple protective mechanisms may explain the long-term clinical benefits13-15. Substantial evidence further recommended that HA in certain patient populations can also have disease-modifying activity.16 To date, there is no systematic review especially addresses on the role of HA’s MW in its effects of symptomatic and structural modifications
Some previous studies reported that, in arthritic joint, the average molecular weight and concentration of HA in the synovial fluid is reduced.17,18 Other scholars 19 further recommended that the high MW HA seems to be depolymerized and degraded into low MW HA in the course of disease process, implying joints with higher MW HA get better function. However, the HAS 3 gene that synthesizes the low MW HA
(200-300 kDa) had later been cloned out. 3,4 Their findings indicated low MW HA can be created by human and is not just the degraded product of high MW HA. If low MW HA is nothing but a depolymerized product, the HAS 3 gene that synthesizes LMW HA should be deleted during the human evolution process. Besides, the surface of articular cartilage is covered with dense horizontal type-two collagen fiber. HA
with high MW and high concentration is very sticky; theoretically, it cannot penetrate this layer and further exert some chondro-protective reactions. (Figure 2A) On the other hand, low MW HA can get better potential in penetrating into the cartilage, especially in the arthritic cartilage. (Figure 2B) Thus, we hypothesize that the phenomenon of the lower HA’s MW and concentration in arthritic joint is the
self-protective and self-remodeling process of human body, not just from the degraded product of high MW HA by disease progression. Furthermore, we also hypothesize that HA with differencing MW may have different contributions in the maintenance of normal joint physiology.
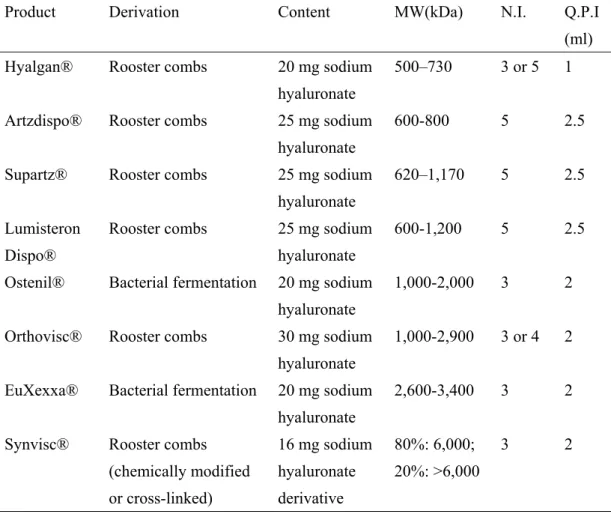
Intra-articular injection of HA is now applied worldwide for the treatment of arthritis. Currently, there are several different preparations of HA with very wide ranged MW (500-6000 kDa), which are marketed in the world. (Table 1) That is, there is still no consensus on the best MW of HA regarding the joints with different arthritic conditions. The differences in efficacy related to the MW of HA remain a subject of debate. In this study, we systemically review the literatures concerning the basic and clinical studies on biological, pathological, and clinical effects of different MW HA. We hopefully clarify the role of HA’s MW in its effects of anti-inflammation and structure-protection.
2. Materials and Methods
2.1 Literatures Search
A review of the literature was carried out based on a PubMed search between 1978 and 2009, using the terms hyaluronan, hyaluronic acid, arthritis, and molecular weight.
2.2 Definition of High and Low Molecular Weight of HA
Before comparison, it is very important to clarify the definition of “high” and “low” MW of HA due to the purpose of this study. By reviewing the literatures, studies regarding the issue of MW of HA all did not identify the definition of High MW or Low MW. Therefore, the same HA product may be regarded as High MW in one report and as Low MW in the other. For example, in the study of Neustadt 20, Orthovisc® (MW up to 2.9 x 106 Da) was regarded as HMW; however, it was considered as LMW in the other report by Karatosun.21
Previous investigators4 have reported that HA with a higher MW (2 x 106 Da) is synthesized by HAS1 and HAS2, whereas HA with a lower MW (2–3 x 105 Da) is synthesized by HAS3. Another report indicated that the MW in normal human
synovial joint fluid could be as high as 6.3-7.6 x 106 Da.18 Because the highest MW of the current commercially available HA is only up to 6.0 x 106 Da, we define the
“high” MW as MW greater than 2 x 106 Da and define the “low” MW as MW less than 2 x 106 Da in the current study.
3. Results
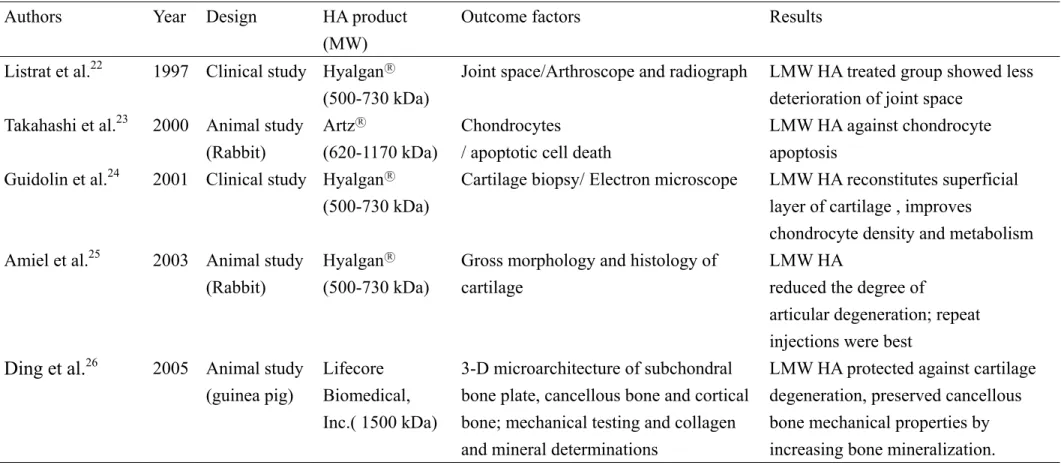
3.1 LOW MOLECULAR WEIGHT HYALURONAN (MW 500-2000 kDa) By reviewing the literatures, most studies providing the evidence of structural modification by HA were conducted with low MW HA. Listrat 22 conducted a prospective, controlled study of one-year duration to evaluate the potential structure-modifying effects of low MW HA (Hyalgan® MW 500-730 kDa). After randomization, either conventional therapy or three cycles (every 3 months) of three intra-articular injections of Hyalgan® (once a week during 2 weeks) were given. The structural outcome was estimated by using the x-rays: joint space narrowing and the arthroscopic findings. Thirty-six patients completed the one-year trial (19 in the Hyalgan® group and 17 in the control group). They found that deterioration in the structural parameters was less in the Hyalgan® group, suggested that repeated intra-articular injections of Hyalgan might delay the structural progression of the disease. Takahashi23 evaluated the effect of intraarticular injections of low MW HA ( Artz○R: MW 620-1170 kDa) on chondrocyte apoptosis and NO production using an experimental OA animal model. Their findings showed that Low MW HA protects against chondrocyte apoptosis during the development of OA, while it may not have
definite effects on NO production in the joints. They recommended that these inhibitory effects of low MW HA on chondrocyte apoptosis may play a role in its mechanism of action in chondroprotection. However, the anti-inflammatory effect of low MW HA is not so dominant, in terms of no significant reduction of NO
production in OA joint. Guidolin24 carried out a histomorphometric study on cartilage samples taken from osteoarthritic human knees before and six months after
intraarticular injections of low MW HA (MW: 500–730 kDa). The results obtained with low MW HA were compared with the results of methylprednisolone acetate treatment. Twenty-four subjects with primary OA of the knee were considered. They found that a significant reconstitution of the superficial layer was observed together with an improvement in chondrocyte density and territorial matrix appearance after six-month low MW HA treatment. In addition, chondrocytes appeared significantly improved in their metabolism, as indicated by the increased extension of the synthetic structures and mitochondria with respect to the organelles having catabolic or storage functions. Their results suggested that low MW HA treatment possessed superior chondro-protective potential to methylprednisolone. Amiel25 analyzed the long-term effect of low MW HA (Hyalgan® MW: 500–730 kDa) on osteoarthritis progression using the rabbit anterior cruciate ligament transection (ACLT) OA model. They compared the gross morphological and histomorphometric changes between groups
treated with one or two courses of five weekly intra-articular injections of low MW HA, or vehicle. The gross morphological and histomorphometric evaluations were performed on harvested knee joints following sacrifice at 26 weeks after ACLT surgery. They discovered that rabbits receiving one or two courses of low MW HA injections showed less disease progression than rabbits treated with ACLT alone or with 10 vehicle injections. They concluded that low MW HA injections reduced the degree of articular degeneration in a rabbit ACLT model of OA. Ding26 carried out an animal study to examine the effects of low MW HA (MW 1500 kDa) on
three-dimensional microarchitecture of subchondral bone tissues in guinea pig primary OA. Their results indicated that low MW HA effectively protects against cartilage degeneration, decreases subchondral bone density and thickness, changes trabecular structure toward rod-like, so that subchondral bone becomes more compliant and thereby reduces cartilage stress during impact loading. Furthermore, low MW HA preserved cancellous bone mechanical properties by increasing bone mineralization. They recommended that early low MW HA administration is effective for intervention of OA initiation and progression, and short-term early low MW HA treatment is sufficient to maintain treatment effects. The detailed summarized data were shown as Table 2.
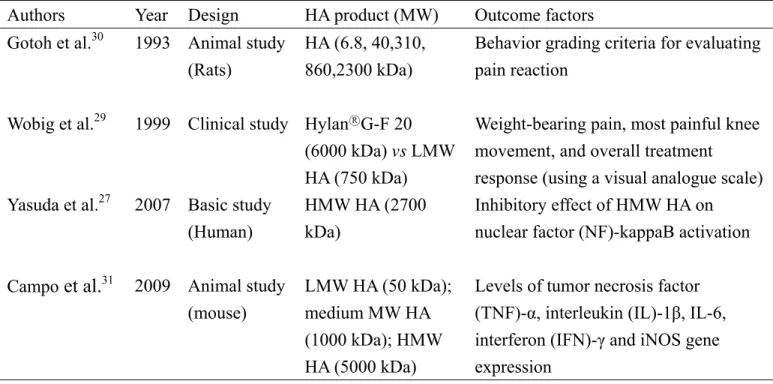
A recent study by Yasuda27 recommended that HMW HA (2700 kDa) could down-regulate the catabolic action of fibronectin fragments in rheumatoid arthritis (RA) joints as a potent inhibitor of nuclear factor (NF)-κB which plays a key role in cytokine-mediated induction of inflammation.28 Recently, Campo 29 also investigate the anti-inflammatory effect of HA with different molecular mass in mouse OA experiment model. They found that HMW HA (5000kDa) can provide significant anti-inflammatory effect, whereas LMW HA (50 kDa and 1000 kDa) cannot. Besides, some investigators 30, 31 suggest that HMW HA has a greater pain-relieving effect when compared with LMW HA. For instance, Wobig 30 conducted a 12-week, double-masked, randomized, multicenter study to compare the effects between HMW HA (6000kDa) and LMW HA (750 kDa) treatment. Their results demonstrated that HMW HA had a significantly greater pain-relieving effect than did the LMW HA. In addition, Gotoh 31 studied the effects of the molecular weight of HA and its action mechanisms on experimental joint pain in rats model. They suggested that HA with MW less than 40 kDa cannot produce an analgesic effect. The detailed summarized data regarding the evidences of anti-inflammatory and pain-relieving effects by high MW HA were shown in Table 3.
4. Discussion
We consider the pain-relieving effect of HA is through the mechanism of
anti-inflammation over synovium, but not directly through the pain related receptors, which is supported by the following rationales and evidences: First, articular cartilage is both avascular and aneural. Consequently, the pain of OA must come from a different source. The pain generation in OA joints could be ascribed to the following causes: Tendonitis over surrounding soft tissue envelope and muscle strain caused by deformity of OA joint will induce pain; Irritation of subchondral nerve endings resulting from cartilage defect or chondromalacia will induce pain; Mechanical irritation rising from loose body or meniscus tear will induce pain.32 However, all of these factors will not be corrected in a short period by nonsurgical method; therefore, the mechanism of rapid symptom relief after HA injection should be associated with the other factor, i.e. the synovitis. (Figure 3) The inflammation of synovium could subside in few days after nonsurgical treatment. In an animal study by Qiu et al, 33 the messenger ribonucleic acid (mRNA) expression of matrix metalloproteinase (MMP)-3 in synovium was significantly suppressed after HA injection. However, in cartilage, the MMP-3 level did not significantly change. Their results also suggest that the rapid therapeutic effect of HA may be through the synovium, but not directly through the cartilage. Second, Gotoh 30 studied the action mechanisms of HA and recommended that HA did not interfere with the analgesic action of the bradykinin antagonist,
indicating that HA does not directly bind with bradykinin receptors. They concluded these effects of HA appear to be caused by the interaction between HA and HA receptors.
4.2 Effect of HA May Be Due To an Intrinsic Carbohydrate-Mediated Mechanism Recently, Castro 34 conducted an animal study to study the analgesic activity of a polysaccharide in experimental osteoarthritis in rats. They compared the analgesic effects of intra-articular injected galactomannan polysaccharide derived from Guar gum (GG) and high molecular weight HA (Hylan G-F20). They found that GG, either as a gel or solution, significantly inhibited joint pain similar to the inhibition achieved with Hylan G-F20. This analgesia is independent of the colloidal state. They
recommend that the analgesic benefit of viscosupplementation, such as HA injection, may be due to an intrinsic carbohydrate-mediated mechanism rather than to the rheologic properties of the material. We completely agree with their recommendation. Actually, a lot of cell surface receptors and signal transduction molecular are
belonging to the glucosaminoglycans (GAGs) family. The HA is also a kind of GAGs. We considered that the effect of HA is also through the intrinsic
carbohydrate-mediated mechanism as well. HA may occupy the sites of cell surface receptors and then block or change the cell behaviors. In other words, after HA occupy most of the receptor engaging sites on cell surface; other molecular cannot
interact with the cell due to limited surface receptor left. Therefore, HA may stabilize the cell through this mechanism.
5. Conclusion
Currently, no pharmacological managements for OA are approved for the indication of modifying the rate of OA progression. However, evaluation of novel agents and agents with established symptom-relieving activity for structure-modifying effects has become a main focus of research in arthritis. By reviewing the literatures, we recommended that the effects of LMW HA were more structure-protective and those of HMW HA were more anti-inflammatory.
ACKNOWLEDGEMENTS
This study was supported by the research grant (DMR 98-068) from China Medical University Hospital.
References
1. Laurent TC, Laurent UBG, Fraser JRE, The structure of hyaluronan: an overview, Immunol Cell Biol 74:A1, 1996.
2. Swann DA, in Sokoloff L (ed) The joints and synovial fluid. Academic Press, New York, 1978.
3. Itano N, Sawai T, Yoshida M, Three isoforms of mammalian hyaluonan synthases have distinct enzymatic properties, J. Biol. Chem 272:25085, 1999.
4. Spicer AP and McDonald JA, Characterization and molecular evolution of a vertebrate hyaluronan synthase gene family, J Biol Chem 273:1923, 1998.
5. Csoka AB, Frost GI, Stern R, The six hyaluronidase-like genes in the human and mouse genomes, Matrix Biol 20:499, 2001.
6. Altman R, Brandt K, Hochberg M, Moskowitz R, Design and conduct of clinical trials in patients with osteoarthritis: recommendations from a task force of the Osteoarthritis Research Society, Osteoarthritis Cartilage 4:217, 1996.
7. Sugimoto H, Yamada H, Terada N, Kanaji A, Kato S, Date H, Ichinose H, Miyazaki K, Intraarticular injection of high molecular weight hyaluronan for osteoarthritis of the knee - prediction of effectiveness with biological markers, J Rheumatol 33:2527, 2006.
8. Neustadt D, Caldwell J, Bell M, Wade J, Gimbel J, Clinical effects of intraarticular injection of high molecular weight hyaluronan (Orthovisc) in osteoarthritis of the knee: a randomized, controlled, multicenter trial, J Rheumatol 32:1928, 2005.
9. Pagnano M, Westrich G, Successful nonoperative management of chronic
osteoarthritis pain of the knee: safety and efficacy of retreatment with intra-articular hyaluronans, Osteoarthritis Cartilage 13:751, 2005.
10. Kotevoglu N, Iyibozkurt PC, Hiz O, Toktas H, Kuran B, A prospective
randomised controlled clinical trial comparing the efficacy of different molecular weight hyaluronan solutions in the treatment of knee osteoarthritis, Rheumatol Int 26:325, 2006.
11. Gossec L, Dougados M, Do intra-articular therapies work and who will benefit most?, Best Pract Res Clin Rheumatol 20:131, 2006.
12. Abatangelo G, O’Regan M, Hyaluronan: biological role and function in articular joints, Eur J Rheumatol Inflamm 151:9, 1995.
13. Namiki O, Toyoshima H, Morisaki N, Therapeutic effect of intra-articular injection of high molecular weight hyaluronic acid on osteoarthritis of the knee, Int J Clin Pharmacol Ther Toxicol 20:501, 1982.
treatment of patients with osteoarthritis of the knee: a randomized clinical trial, J Rheumatol 25:2203, 1998.
15. Scali JJ, Intra-articular hyaluronic acid in the treatment of osteoarthritis of the knee: a long term study, Eur J Rheumatol Inflamm 15:57, 1995.
16. Goldberg VM, Buckwalter JA, Hyaluronans in the treatment of osteoarthritis of the knee: evidence for disease-modifying activity, Osteoarthritis Cartilage 13:216, 2005. 17. Fam H, Bryant JT, Kontopoulou M, Rheological properties of synovial fluids,
Biorheology 44:59, 2007.
18. Dahl LB, Dahl IMS, Engstrom LA, Concentration and molecular weight of sodium hyaluronate in synovial fluid from patients with rheumatoid arthritis and other arthropathies, Ann Rheum Dis 44:817, 1985.
19. Praest BM, Greiling H, Kock R, Assay of synovial fluid parameters: hyaluronan concentration as a potential marker for joint diseases, Clin Chim Acta 266:117, 1997. 20. Neustadt D, Caldwell J, Bell M, Wade J, Gimbel J, Clinical effects of
intraarticular injection of high molecular weight hyaluronan (Orthovisc) in
osteoarthritis of the knee: a randomized, controlled, multicenter trial, J Rheumatol 32:1928, 2005.
21. Karatosun V, Unver B, Gocen Z, Sen A, Comparison of two hyaluronan drugs in patients with advanced osteoarthritis of the knee. A prospective, randomized, double-blind study with long term follow-up, Clin Exp Rheumatol 23:213, 2005. 22. Listrat V, Ayral X, Patarnello F, Bonvarlet J-P, Simonnet J, Amor B, Dougados M,
Arthroscopic evaluation of potential structure modifying activity of
hyaluronan(Hyalgan○R) in osteoarthritis of the knee, Osteoarthritis Cartilage 5:153, 1997.
23. Takahashi K, Hashimoto S, Kubo T, Hirasawa Y, Lotz M, Amiel D, Effect of hyaluronan on chondrocyte apoptosis and nitric oxide production in experimentally induced osteoarthritis, J Rheumatol 27:1713, 2000.
24. Guidolin DD, Ronchetti IP, Lini E, Guerra D, Frizziero L, Morphological analysis of articular cartilage biopsies from a randomized, clinical study comparing the effects of 500-730 kDa sodium hyaluronate (Hyalgan○R) and methylprednisolone acetate on primary osteoarthritis of the knee. Osteoarthritis Cartilage 9:371, 2001. 25. Amiel D, Toyoguchi T, Kobayashi K, Bowden K, Amiel ME, Healey RM,
Long-term effect of sodium hyaluronate (Hyalgan) on osteoarthritis progression in a rabbit model, Osteoarthritis Cartilage 11:636, 2003.
26. Ding M, Christian Danielsen C, Hvid I, Effects of hyaluronan on
primary osteoarthrosis, Bone 36:489, 2005.
27. Yasuda T, Nakamura T, Inhibition of nuclear factor-kappaB by hyaluronan in rheumatoid chondrocytes stimulated with COOH-terminal heparin-binding fibronectin fragment, Mod Rheumatol 17:391, 2007.
28. Marks-Konczalik J, Chu SC, Moss J, Cytokine-mediated transcriptional induction of the human inducible nitric oxide synthase gene requires both activator protein 1 and nuclear factor κB-binding sites, J Biol Chem 273:22201, 1998.
29. Wobig M, Bach G, Beks P, Dickhut A, Runzheimer J, Schwieger G, Vetter G, Balazs E, The role of elastoviscosity in the efficacy of viscosupplementation for
osteoarthritis of the knee: a comparison of hylan G-F 20 and a lower-molecular-weight hyaluronan, Clin Ther 21:1549,1999.
30. Gotoh S, Onaya J, Abe M, Miyazaki K, Hamai A, Horie K, Tokuyasu K, Effects of the molecular weight of hyaluronic acid and its action mechanisms on experimental joint pain in rats, Ann Rheum Dis 52:817, 1993.
31. Campo GM, Avenoso A, Campo S, D'Ascola A, Traina P, Rugolo CA, Calatroni A, Differential effect of molecular weight hyaluronan on lipopolysaccharide-induced damage in chondrocytes, Innate Immun 16:48, 2010.
32. MW Hungerford, MA Mont, DS Hungerford, in JN Insall and WN Scott (eds.) Surgery of the knee(III), Churchill Livingstone Inc, New York, USA, pp.
565-587,2001
33. Qiu B, Liu SQ, Peng H, Wang HB, The effects of sodium hyaluronate on mRNA expressions of matrix metalloproteinase-1, -3 and tissue inhibitor of
metalloproteinase-1 in cartilage and synovium of traumatic osteoarthritis model, Chin J Traumatol 8:8, 2005.
34. Castro RR, Feitosa JP, da Cunha PL, da Rocha FA, Analgesic activity of a polysaccharide in experimental osteoarthritis in rats, Clin Rheumatol 26:1398, 2007.
Table 1. Characteristics of marketed hyaluronans
Product Derivation Content MW(kDa) N.I. Q.P.I
(ml) Hyalgan® Rooster combs 20 mg sodium
hyaluronate
500–730 3 or 5 1 Artzdispo® Rooster combs 25 mg sodium
hyaluronate
600-800 5 2.5 Supartz® Rooster combs 25 mg sodium
hyaluronate
620–1,170 5 2.5
Lumisteron Dispo®
Rooster combs 25 mg sodium hyaluronate
600-1,200 5 2.5 Ostenil® Bacterial fermentation 20 mg sodium
hyaluronate
1,000-2,000 3 2
Orthovisc® Rooster combs 30 mg sodium hyaluronate
1,000-2,900 3 or 4 2 EuXexxa® Bacterial fermentation 20 mg sodium
hyaluronate
2,600-3,400 3 2
Synvisc® Rooster combs (chemically modified or cross-linked) 16 mg sodium hyaluronate derivative 80%: 6,000; 20%: >6,000 3 2 MW: Molecular weight
Table 2 Evidences of chondro-protective effect by LMW HA
Authors Year Design HA product
(MW)
Outcome factors Results
Listrat et al.22 1997 Clinical study Hyalgan○R
(500-730 kDa)
Joint space/Arthroscope and radiograph LMW HA treated group showed less deterioration of joint space
Takahashi et al.23 2000 Animal study
(Rabbit)
Artz○R
(620-1170 kDa)
Chondrocytes
/ apoptotic cell death
LMW HA against chondrocyte apoptosis
Guidolin et al.24 2001 Clinical study Hyalgan○R
(500-730 kDa)
Cartilage biopsy/ Electron microscope LMW HA reconstitutes superficial layer of cartilage , improves
chondrocyte density and metabolism Amiel et al.25 2003 Animal study
(Rabbit)
Hyalgan○R
(500-730 kDa)
Gross morphology and histology of cartilage
LMW HA
reduced the degree of
articular degeneration; repeat injections were best
Ding et al.26 2005 Animal study
(guinea pig)
Lifecore Biomedical, Inc.( 1500 kDa)
3-D microarchitecture of subchondral bone plate, cancellous bone and cortical bone; mechanical testing and collagen and mineral determinations
LMW HA protected against cartilage degeneration, preserved cancellous bone mechanical properties by increasing bone mineralization.
Table 3 Evidences of anti-inflammatory and pain-relieving effects by HMW HA
Authors Year Design HA product (MW) Outcome factors Results
Gotoh et al.30 1993 Animal study
(Rats)
HA (6.8, 40,310, 860,2300 kDa)
Behavior grading criteria for evaluating pain reaction
HMW HA produced high and long-lasting analgesia than LMW HA.
Wobig et al.29 1999 Clinical study Hylan○RG-F 20
(6000 kDa) vs LMW HA (750 kDa)
Weight-bearing pain, most painful knee movement, and overall treatment response (using a visual analogue scale)
HMW HA G-F 20 had significantly greater pain-relieving effects than did the LMW HA
Yasuda et al.27 2007 Basic study
(Human)
HMW HA (2700 kDa)
Inhibitory effect of HMW HA on nuclear factor (NF)-kappaB activation
HMW HA significantly suppressed heparin-binding fibronectin fragment -activated NF-kappaB
Campo et al.31 2009 Animal study
(mouse)
LMW HA (50 kDa); medium MW HA (1000 kDa); HMW HA (5000 kDa)
Levels of tumor necrosis factor (TNF)-α, interleukin (IL)-1β, IL-6, interferon (IFN)-γ and iNOS gene expression
Only HMW HA can reduce all the detrimental effects stimulated by lipopolysaccharide treatment
Legends:
Figure 1: The repeating molecular unit of hyaluranic acid (HA)
Figure 2A: The normal articular cartilage is covered with dense horizontal type-two collagen fiber. Theoretically, HA cannot penetrate this layer and exert some further reactions.
Figure 2B: The surface of arthritic cartilage was damaged and the dense horizontal type-two collagen fiber was torn. There are some fissures through the surface layer and being into the deep layer of the cartilage. HA with low molecular weight can get better potential in penetrating into the cartilage.