U-Health Approach to the National Health
Information Systems in Korea
Young Moon Chae, Ph.D.
Graduate School of Public Health, Yonsei University, Seoul, Korea
Email: [email protected]
Abstract
This study describes the current status of computerization for hospitals and makes various recommendations to improve the level of computerization and information sharing between hospitals in order to strengthen the National Health Information System (NHIS). According to a survey of 314 out of 1,289 hospitals in August 2005, the computerization level was higher for the specialty tertiary hospitals and general hospitals than for smaller hospitals. The computerization rate by applications was 75.6% for outpatient CPOE (Computerized Physician Order Entry System), 70.6% for inpatient CPOE, 47.1% for PACS (Picture Archiving and Communication System), and 20.7% for outpatient EMR (Electronic Medical Record).
In addition, this paper also presents the NHIS plan in Korea and the survey results that examined to identify the user requirements for the electronic health record (EHR), which is a core element of NHIS. According to a survey
conducted in May 2005 of 317 people, ranging from community residents, health workers, and information systems people, most people responded that development of EHR was necessary and that they were willing to use it actively. With regard to key information included in EHR, they made the following recommendations in order: test results, health program, medical examination, immunization, allergy, information about medication and medical treatment, health behavior, genetic information, cause of death, and medical charge information. Most of the respondents wanted to apply EHR to the management of chronic diseases, but they were concerned about the security of private medical information. Based on the results, recommendations for development and implementation strategies were presented.
Keyword: national health information system,
1. Introduction
As information technologies (IT) are rapidly improved, healthcare institutions in Korea are increasingly introducing information systems in order to improve quality of care and reduce administrative costs. There are several factors related to the increasing trends in computerization of health institutions and the increasing demand for the national health information system (NHIS). First, the proportion of the elderly population has been rapidly increasing for the last several years. The elderly population has been increasing at an annual rate of 5% and the elderly population is expected to reach about 23.9% of the total population in 2030 [1]. This rate of increase is higher than that of most OECD countries. Since elderly people place greater demand on healthcare services and resources, there is a need for information systems to support these health services and improve the efficiency in administrative activities at healthcare institutions.
Second, the legal system in Korea has been instrumental in the rapid computerization of the healthcare sector. Three application areas on e-health have been legalized in 2003: telemedicine, electronic medical record (EMR), and e-prescription system for pharmacies, which is a computerized physician order entry (CPOE) system between hospitals and
pharmacies.
Third, a major change in national hospital policy has also affected the information trend. Under the DDA (Doha Development Agenda), the Korean hospital market will be opened to foreign countries in 2007. Many Korean hospitals fear that world-class U.S. hospitals will enter the Korean market by targeting rich patients and using advanced information systems such as telemedicine and EMR. In a response to this, many Korean hospitals are developing more specialized medical services and strengthening their information systems.
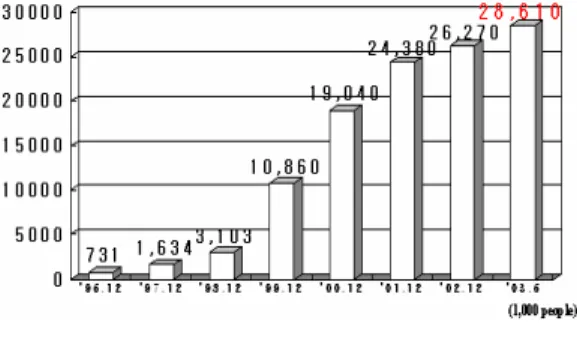
Finally, advanced internet infrastructure and other IT in Korea have been a driving force for the rapid growth in computerization. The broadband uptake rate is in the top level in the world (Figure 1). In addition, Korea is also one of the top countries in the manufacture and export of PCs, computer monitors, hard disks, and other hardware.
Figure 1. Number of subscribers of high-speed internet users in Korea
Many developed countries are actively developing their NHIS according to their health delivery systems. Most countries are developing electronic health record (EHR) as the core element of their national systems [2]. EHR has been defined as a systematic and continuous aggregation of computerized information about medical treatment and individual health. The EHR system includes the information about medical treatment and health collected throughout life from birth to death, as well as family genetic information and personal information on health wellness. In the United States, hospitals at the state level are integrated to form the Local Health Information Infrastructure (LHII), which is further integrated at the national level to form the National Health Information Infrastructure (NHII). Through NHII, an integrated EHR system was developed incorporating public and private insurance. This system was managed by a committee comprised of government officials, health providers, and consumers. The EHR system is being applied to patient care, electronic prescription service, and review of insurance claims [3]. In England, the public health system was divided into 5 regions and the nationwide, unified EHR system was developed and used in all regions to support e-medical treatment reservation service, telephone consultation service, and clinic research, etc.
The Korean government developed its first
10-year national ISP (Information Strategy Plan) for NHIS in 1990, followed by the second version in 2001. The scope of the ISP was broad covering almost all activities of the Ministry of Health and Welfare (MOHW): community health information system for health centers and subcenters, hospital information systems for emergency care and blood management, national health insurance system for processing insurance claims data with a focus on EDI (Electronic Data Interchange) for data transmission, national pension system, quarantine system for imported foods, pharmaceutical information system for processing administrative drug data for KFDA (Korea Food and Drug Administration), infectious disease surveillance system and vaccination system for CDC (Center for Disease Control), national registration system for the handicapped people, and national health statistics system.
The national ISP has been a driving force for upgrading information systems for MOHW. While these information systems have greatly contributed to achieving our national goals of reducing health care costs and improving quality of healthcare, our national systems are still years behind some western countries with respect to standards, e-health related laws, EHR, and telemedicine. This paper presents some key infrastructure (standards, law, and organization), national ISP, and the survey results on EHR.
2. Current Status of
Computerization in Korean
Healthcare Institutions
2.1 Subjects
Chae et al. [4] have conducted a nationwide survey on the computerization of healthcare institutions. 314 out of 1,289 hospitals were surveyed in August 2005.
2.2 Results 2.2.1 Hospitals
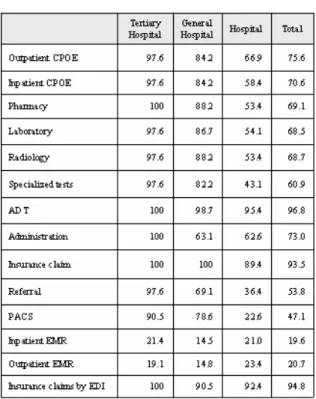
As seen in Table 1, almost all specialty tertiary hospitals implement both outpatient and inpatient CPOE, PACS (Picture Archiving and Communication System), insurance claims processing, including transmitting claims data by EDI, and ADT (Admission, Discharge, and Transfer). However, only about 20% of hospitals were implementing EMR, perhaps because EMR was legalized only in 2003. It is expected that most tertiary hospitals will implement EMR by the end of 2007.
2.2.2 Clinics and Pharmacies
Most private clinics and pharmacies are implementing some form of information system. Over 90% of all clinics and pharmacies are transmitting their insurance claims via EDI network. Even before the government legalized EMR, many clinics had introduced EMR and about 85% of clinics
were implementing EMR in 2005.
Table 1. Status of Computerization in Hospitals ( ): percentages
2.2.3 Public Healthcare Institutions
Similarly, most public healthcare institutions were implementing information systems. All community health centers were implementing CPOE and the reporting systems on infectious diseases and vaccination. The Korean government is in the process of changing client-server based public health information to web-based systems using the ASP (Application Service Provider) approach.
2.2.4 National Health Information System This survey also included items on government policies on NHIS. Most hospitals did not introduce any form of standards on clinical terminology, perhaps due to the absence of both national standards and incentives for using international standards. Despite the government policy on information sharing among health institutions, only 15% of institutions were exchanging information for the purpose of patient referrals. Over 80% of clinics expressed negative opinion on telemedicine due to the high risk of misdiagnosis and loss of patients to large tertiary hospitals. These results have significant implications for developing and disseminating the NHIS.
3. National Health Information
Systems (NHIS ) in Korea
3.1 Information Strategy Plan (ISP)
In 2004, MOHW revised its ISP, which was comprised of three phases. In Phase 1 (2004-2005), ISP for NHIS was developed and standards and e-health related laws were developed. In Phase 2 (2006-2007), EHR and public health information systems are being developed using new standards. In Phase 3 (2008-2009), standards and EHR for health centers will be redeveloped to meet the needs
for the private health institutions.
3.2 Organization
In order to effectively carry out ISP, the MOHW created the organization. Several advisory committees were created for providing policy directions and expert opinions. Two centers were created for carrying out system development and the related researches: Center for NHIS Development and R & D Center for EHR. In addition, several working groups were created for developing the detailed activity plans for each application: telemedicine, consumer health information, and so on.
3.3 Standards
Standard is an important infrastructure for the NHIS because it allows hospitals to exchange and share patient information. In order to develop the national standards, 14 subcommittees were created in 2004: clinical terminology, dental terminology, healthcare terminology, herbal medicine terminology, medical devices, image processing, security, etc.
The committees chose the UMLS (Unified Medical Language System) developed by the NLM (National Library of Medicine) in the United States as a framework for building the Korean standards because it is internationally
accepted standards and there is no charge, which can be a big financial burden for the small hospitals in the future. Matching tables for clinical and other terminologies were created under the UMLS framework in order to develop the Korean national standards.
3.4 e-Health Law
Three revisions in the medical law enacted in 2003 greatly upgraded healthcare information systems in Korea: legalizing telemedicine, legalizing electronic medical record, and legalizing e-prescription system for outside pharmacies. However, there are needs for revising this law again. First, there is a need for providing a legal ground for NHIS. Second, there is a need for strengthening security and confidentiality of patient information. Third, there is a need for modifying some clauses related to telemedicine in order to increase its use in healthcare institutions.
Accordingly, government developed a draft of new e-Health law that includes the following elements: authorizing a creation of the Center for NHIS, including a separate Act for security and confidentiality of patient information, authorizing maintenance of EMR outside of the hospital that holds the ownership in order to allow ASP for public health information systems, and allowing tele-homecare for revisit patients.
3.5 Public Health Information Systems
The public health system in Korea is comprised of a three tier system: 250 community health centers, 1200 health subcenters, and 2000 health posts. They provide primary health services and vaccinations to community residents and collect health statistics at the grass-root level. In an effort to improve their operation and quality of services, health centers started to introduce information systems in the early 90s and now entire health centers are implementing information systems. According to the evaluation survey [5], health center information systems were effective in improving patient satisfaction and increasing the productivity of health workers.
However, updating software and providing timely hardware maintenance have been serious problems for health centers because most health centers are located in remote rural areas and suffer a lack of skilled maintenance people. Since the public health information systems are the backbone of the NHIS, the government decided to strengthen the system by converting current client-server based systems to a web-based system using the ASP approach. In addition, newly developed national standards will be applied to develop community EHR for the new public health information system.
3.6 Telemedicine
First pilot project on telemedicine was carried out from 1995 to 1998 between the Wooljin Health center and the Kyungbook University hospital using a high speed T1 telecommunication network. While this project demonstrated a possibility of providing medical consultation from a distance through network, it was not widely used as much as people anticipated because of inadequate telecommunication network and lack of financial incentives for medical doctors. While several pilot telemedicine projects have been carried out mainly at community health centers since then, most of them had a limited success in community acceptance even after telemedicine was legally allowed in 2003.
3.7 Survey on EHR
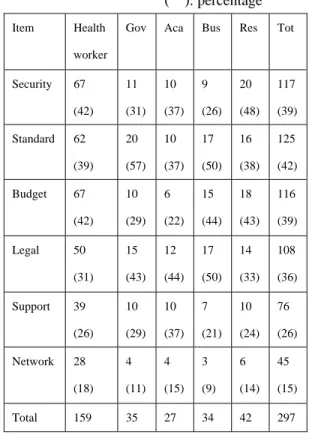
According to a survey conducted in May 2005 of 317 people, ranging from community residents, health workers, and information system people, most people responded that development of EHR was necessary and that they were willing to use it actively [6]. As a prerequisite for the development of EHR, the respondents recommended the development of a security system, standards, budgets, restructuring the legal system, obtaining community support, and telecommunication network (Table 2).
Table 2. Prerequisites for Developing EHR ( ): percentage Item Health
worker
Gov Aca Bus Res Tot
Security 67 (42) 11 (31) 10 (37) 9 (26) 20 (48) 117 (39) Standard 62 (39) 20 (57) 10 (37) 17 (50) 16 (38) 125 (42) Budget 67 (42) 10 (29) 6 (22) 15 (44) 18 (43) 116 (39) Legal 50 (31) 15 (43) 12 (44) 17 (50) 14 (33) 108 (36) Support 39 (26) 10 (29) 10 (37) 7 (21) 10 (24) 76 (26) Network 28 (18) 4 (11) 4 (15) 3 (9) 6 (14) 45 (15) Total 159 35 27 34 42 297 (Gov: Government employee, Aca: Academics,
Bus: Business, Res: Community residents)
The degree of participation was the highest for those in business, followed in order by government employees, academics, health workers, community residents, and health providers. With regard to key information included in EHR, they made the following recommendations in order: test results, health program, medical examination, immunization, allergy, information about medication and medical treatment, health behavior, genetic information, cause of death, and medical charge information. Most of the respondents wanted to apply EHR to the management of
chronic diseases, but they were concerned about the security of private medical information. The majority wanted to access their own personal information through Internet after security validation.
In conclusion, the unified England EHR model was proposed for the EHR system for public health institutions in Korea based on the similarities in the public health delivery system in the two countries and the Korean nationwide registration system. In order to protect the security of private health information, we recommend using an IC security card to access EHR. In addition, we recommend organizing an EHR committee, similar to that of the United States, in order to protect against an infringement of personal information due to the monopoly of information by a single organization.
4. Conclusion
The Korean government is pushing hard with its ambitious plan for the NHIS. The factors which are critical for the success of the plan may include reliable and cost-effective IT, user-friendly application systems, standards, law, budgets, and strong support from various affected groups such as the Korean Medical Association, citizen’s group, etc. Of these, the latter four factors are rather weak areas in
Korea, compared with the technical factors, and therefore they need to be strengthened. Especially, getting support from medical community is very important factor for the success of telemedicine.
5. Reference
[1] Ministry of Health and Welfare. “National Demographic and Health Statistics”, 2003.12 [2] E. Middleton, E. Hammond, P.F. Brennan,
“Accelerating U.S. Adoption”, JAMIA, 2005; 12, pp. 13-19
[3] W.A. Yasnoff, B.L. Humphry, D.E. Detmer, “A Consensus Action Agenda for Achieving the National Health Information Infrastructure”, JAMIA, 2004; 11, pp. 332-338
[4] Y.M. Chae, et al. Status of Computerization in Korean Health Institutions”, Health Insurance Review Agency, 2005.12
[5] Y.M. Chae, S.I. Kim, S.H. Choi, I.S. Kim, “Implementing Health Information System: Measuring Success in Korea’s Health Centers”, International Journal of Health Planning and Management, 1994; 9, pp. 341-348
[6] G.H. Kim, Y.M. Chae, S.I. Kim, Y.E. Kim, “Study on the Korean Model for Community-based EHR”, Journal of Korea Society of Medical Informatics, 2005; 11(2), pp. S18-S23