Maxillofacial Growth in Children with Unilateral
Cleft Lip and Palate following Secondary
Alveolar Bone Grafting: An Interim Evaluation
Hong-Po Chang, D.M.D., Ph.D., Min-Chi Chuang, D.D.S., M.D.S., Yi-Hsin Yang, M.S., Ph.D., Pao-Hsin Liu, M.S., Chih-Han Chang, M.S., Ph.D., Chen-Feng Cheng, D.D.S., M.D.S., and Jui-Pin Lai, M.D.
Kaohsiung and Tainan, Taiwan
This study evaluates the effect of alveolar bone grafting on the maxillofacial growth in children of mixed dentition with unilateral complete cleft lip– cleft palate. Twenty pa-tients received an iliac crest alveolar bone graft between the ages of 6 years 10 months and 10 years 10 months, whereas 20 matched controls between the ages of 6 years 11 months and 10 years 6 months did not. Geo-metric morphoGeo-metric assessments were used to localize alterations between the initial and final cephalographs in the two groups of cleft children, using Procrustes analysis and thin-plate spline analysis, in addition to con-ventional cephalometric techniques. It is concluded that no statistically significant dif-ference in maxillofacial growth was found between the cleft children having received secondary alveolar bone grafting and the nongraft controls in general during the first to third postoperative years. Further investi-gation will be undertaken to determine the long-term effects after the age of skeletal
maturity. (Plast. Reconstr. Surg. 115: 687,
2005.)
Boyne and Sands1,2introduced secondary
al-veolar bone grafting as a procedure for repair of alveolar defects in patients with cleft lip–
cleft palate. This procedure has gained in-creased popularity since then and is currently the standard of care in most cleft palate and craniofacial centers. The goals and benefits of bone grafting are well recognized and include the creation of bony support for subsequent tooth eruption, elimination of oronasal fistu-las, improved status of oral hygiene by separat-ing the nasal cavity from the oral cavity, recon-struction of the hypoplastic piriform aperture and soft-tissue nasal base support, and stabili-zation of the maxillary arch.1– 8
However, the belief that surgical interven-tion has a traumatic effect is well established, and the adverse effect on maxillofacial growth of the various surgical techniques of lip and palate repair has been demonstrated in the literature.9 –11Nevertheless, there is no
consen-sus in the literature pertaining to secondary alveolar cleft bone grafting of unilateral com-plete cleft lip– cleft palate as to whether this procedure causes disruption of maxillofacial
growth. Ross,12in a comparative study of three
centers, noted that bone grafting during the period of late mixed dentition adversely affects the vertical dimensions of the anterior maxilla and, indirectly, the lower face. However, Semb13 found no statistically significant
differ-ence in either anteroposterior or vertical max-illary growth when comparing children with unilateral complete cleft lip– cleft palate who had alveolar bone grafts during the period of
From the Department of Orthodontics, Faculty of Dentistry, and the Graduate Institute of Oral Health Sciences, Kaohsiung Medical University; the Institute of Biomechanical Engineering, National Cheng-Kung University; and the Division of Orthodontics, Department of Dentistry, and the Department of Plastic Surgery, Kaohsiung Chang-Gung Memorial Hospital. Received for publication October 7, 2003; revised March 9, 2004.
DOI: 10.1097/01.PRS.0000152432.24053.52
mixed dentition to a control group of children with unilateral complete cleft lip– cleft palate who had no alveolar bone grafts. The results of
the studies by Daskalogiannakis and Ross14and
Levitt et al.15 are in agreement with the
find-ings by Semb.13
Conventional cephalometrics, based on angular and linear measurements, has shown
an increasing number of limitations,16 and
the actual sites of putative craniofacial skele-tal change are insufficiently evidenced in
tra-ditional cephalometric analysis.17 Recently,
newer disciplines of geometric morphomet-rics have evolved, enabling a more thorough analysis of form change. These disciplines
include Procrustes analysis,18,19 thin-plate
spline analysis,20,21 and other methods using
landmark data. All these methods are coor-dinate-free and insusceptible to translation or rotation, which offers a great advantage over conventional cephalometrics.
This study evaluates the maxillofacial growth of children with unilateral complete cleft lip– cleft palate who had secondary alveolar bone grafting to determine whether the maxillofa-cial growth was disturbed by this procedure. This was conducted to carry out geometric morphometric assessments to localize alter-ations between the initial and final cephalo-graphs in children with cleft lip– cleft palate, both with and without secondary alveolar bone grafting, using Procrustes analysis and thin-plate spline analysis, in addition to conven-tional cephalometric techniques.
PATIENTS AND METHODS Sample
All patients were born with unilateral com-plete cleft lip– cleft palate. At 1 to 2 weeks after birth, the infants underwent nasoalveolar
molding therapy,22 using an acrylic intraoral
molding plate with a nasal stent rising from the labial vestibular flange. The effectiveness of therapy using an intraoral molding plate with a nasal stent is enhanced by adequately support-ing the presurgical orthopedic appliance against the palatal tissues and by strapping the lip segments together across the cleft with 3M (St. Paul, Minn.) tape. This treatment modality includes as its objectives the active molding and repositioning of the deformed nasal carti-lages and alveolar processes, in addition to the
correction of the nasal tip and the alar base on the affected side and the position of the
phil-trum and columella.22
At 3 to 4 months of age, the infants had a
Millard rotation-advancement cheiloplasty,23,24
followed by a one-stage two-flap palatoplas-ty25,26at the age of 9 to 18 months. At 5 years of
age, the patients underwent open tip rhino-plasty27with or without lip revision. If
velopha-ryngeal insufficiency had occurred, sphincter
pharyngoplasty28was also performed at 5 years
of age. All patients underwent passive preoper-ative orthodontic treatment. They were treated at approximately the same time with the same technique in the sequence by the same sur-geons and orthodontists on the cleft palate team.29
Details of the sample are presented in Table I. The grafted group consisted of 20 children (13 boys and seven girls) who underwent an iliac crest alveolar bone graft. The alveolar bone grafting procedure used was that
de-scribed by Hall and Posnick,8with minor
mod-ifications.29The control nongrafted group
con-sisted of 20 children (13 boys and seven girls) who did not receive an alveolar bone graft. The control group was chosen randomly from non-grafted cleft subjects with similar chronologic age, skeletal age (cervical vertebral bone age),30,31sex, and observation period (Table I).
Because the two groups were not individually matched, the statistical analysis was based on two independent groups.
TABLE I Summary of Sample Data
Grafted Group Nongrafted Group Sex distribution Female 7 7 Male 13 13
Age at graft (ABG), year, month
Mean 8, 2 —
Range 6, 10–10, 10 —
Stage of examination, year, month Younger (pre-ABG) Mean 7, 11 7, 11 Range 6, 9–10, 8 6, 11–10, 6 Older (follow-up) Mean 11, 4 11, 2 Range 8, 7–14, 3 8, 8–14, 2
Observation period, year, month
Mean 3, 2 3, 3
Range 1, 11–4, 4 1, 10–4, 2
Time period treated 1996–2000 1986–1987
Methods
Lateral cephalometric radiographs were ob-tained at two different times: at the younger or pre–iliac crest alveolar bone graft stage and at the older or follow-up stage. The magnification of each cephalograph used in this study was 10 per-cent. Each cephalograph was traced by one in-vestigator and checked by another inin-vestigator.
An appropriate software package32 was used to
digitize 14 homologous landmarks on the cranio-facial complex (Fig. 1). The landmarks were used to compare 10 angles and three distances.
To assess errors involved in cephalometric tracing and digitizing, 30 randomly selected lateral cephalographs were traced and digi-tized. The same cephalographs were retraced and redigitized under the same conditions af-ter an inaf-terval of 1 week. Correlations between the double measurements were then analyzed for both angular and linear measurements. The correlation coefficients between the
dou-ble measurements were over 0.9.33
Conventional cephalometric analysis. The paired
t test was used to evaluate any statistically
signifi-cant differences between the younger or pre–iliac crest alveolar bone graft stage and the older or follow-up stage in the two groups. After this uni-variate analysis, measurements were compared by a multivariate Hotelling’s T2test34so that the
re-sults derived from the Procrustes analysis could be corroborated. The Hotelling’s T2test was used on
these 10 angular and three linear variables to de-termine whether the overall mean differences in outcome were beyond chance.
The analysis of covariance was performed to investigate the statistical significance of differ-ences attributable to sex and presence or ab-sence of a bone graft, using the younger values as a covariate. In this way, any differences that ex-isted between the two groups at the younger or pre–iliac crest alveolar bone graft stage would be taken into account in the comparison of the later differences at the older or follow-up stage.
Procrustes analysis. A generalized least-squares
Procrustes analysis18,19 procedure was used to
compute the average configuration of the younger or pre–iliac crest alveolar bone graft stage and the older or follow-up stage of two groups. Each subject’s coordinates were trans-lated, rotated, and scaled iteratively until the least-squares fit of all configurations was no longer improved. Craniofacial configurations were reg-istered with respect to one another and scaled to equivalent areas, which eliminated any difference
related to size. The procedure was repeated for each stage to produce a mean geometric config-uration. To determine whether craniofacial con-figurations differed between stages, mean geom-etries were statistically compared using analysis of variance.18,19,35
Thin-plate spline analysis. After the mean geo-metric configurations for each group were com-puted using Procrustes analysis,18,19they were
sub-jected to thin-plate spline analysis.20,21,36
Thin-plate spline analysis facilitates the construction and display of transformation grids that capture the shape change between forms. The biological shape change is modeled as a deformation, and the spatial changes between the compared mor-phologies can be seen as deformation grids.37This
conceptually simple maneuver quickly shows the
FIG. 1. Cephalometric landmarks: S, sella; Se, spheno-eth-moidale; N, nasion; PtmS, pterygomaxillare superius; PtmI, pterygomaxillare inferius; Pns, posterior nasal spine; Ans, an-terior nasal spine; A, subspinale; B, supramentale; Pog, pogo-nion; Gn, gnathion; Me, menton; Go, gonion interceptive; Ar, articulare. Cephalometric planes or lines: SN, sella-nasion plane; PP, palatal plane; MP, mandibular plane; RP, ramal plane.
TABLE II
Procrustes Analysis of Mean Craniofacial Configurations in the Grafted and Nongrafted Groups between Younger or
Pre-ABG and Older or Follow-Up Stages
Group
Procrustes Analysis
Residual F Test p*
Grafted 0.000109 0.2264 ⬎0.05 Nongrafted 0.000588 0.1351 ⬎0.05
ABG, iliac crest alveolar bone graft. * p⬎ 0.05, nonsignificant.
location and extent of the deformation. Separate transformation grids were obtained for the younger or pre–iliac crest alveolar bone graft stage and the older or follow-up stage compari-sons in the grafted and nongrafted groups.
RESULTS Procrustes Analysis
Residuals computed from the Procrustes analysis were compared using an F distribution.
FIG. 2. Thin-plate splines (above) generated from mean craniofacial configuration in the nongrafted group at a younger stage in untransformed space and (below) generated from mean differences in shape coordinates between younger and older stages in the nongrafted group. S, sella; N, nasion; PtmS, pterygomaxillare superius; PtmI, pterygomax-illare inferius; Pns, posterior nasal spine; Ans, anterior nasal spine; A, subspinale; B, supramentale; Pog, pogonion; Gn, gnathion; Me, menton; Go, gonion interceptive; Ar, articulare.
FIG. 3. Thin-plate splines (above) generated from mean craniofacial configuration in the grafted group at the pre–iliac crest alveolar bone graft alveolar bone graft stage in untrans-formed space and (below) generated from mean differences in shape coordinates between pre–iliac crest alveolar bone graft stage and follow-up stage in the grafted group. S, sella; N, nasion;
PtmS, pterygomaxillare superius; PtmI, pterygomaxillare
infe-rius; Pns, posterior nasal spine; Ans, anterior nasal spine; A, subspinale; B, supramentale; Pog, pogonion; Gn, gnathion; Me, menton; Go, gonion interceptive; Ar, articulare.
Differences in the craniofacial configurations between the younger or pre–iliac crest alveolar bone graft stage and the older or follow-up
stage were considered not significant at the p⬎
0.05 level for both the grafted and nongrafted groups (Table II).
Thin-Plate Spline Analysis
The total spline showed little change of the grafted and nongrafted groups at the end of the observation periods (Figs. 2 and 3). Point A (subspinale) was relatively backward in both groups.
Conventional Cephalometric Analysis
The grafted group revealed a significant change only in the mean palatal length (pos-terior nasal spine–an(pos-terior nasal spine dis-tance) between the younger and the older stages (Table III). The mean palatal length increased 2.1 mm in this group. However, the nongrafted group showed no significant change in all linear and angular measurements studied between the two stages, even though the mean palatal length increased 2.0 mm (Ta-ble IV).
At the younger stage compared with the non-grafted group, the non-grafted group exhibited a statistically significantly longer palatomaxillary complex (as evidenced by posterior nasal spine–anterior nasal spine, subspinale–poste-rior nasal spine, and subspinale–pterygomaxil-lare inferius/palatal plane distances), more retruded mandible with more vertical ramus (as shown by nasion-supramentale, sella-nasion-pogonion,
subspinale-nasion-supra-mentale, gonial, and sella-nasion/ramal plane angles), and more proclined lower incisors (as evidenced by the L1/mandibular plane angle)
(Table V). The multivariate Hotelling’s T2tests
confirmed that statistically significant differ-ences existed between the two groups at the younger stage, although only for angular mea-surements (Table VI).
However, at the end of the observation peri-ods, the differences in 15 of the 18 cephalo-metric measurements were not statistically sig-nificant between the two groups. The only three measurements that did reach statistical significance were sella-nasion-supramentale, sella-nasion-pogonion, and sella-nasion/pala-tal plane angles, which appeared to have
dif-ferences of an average of ⫺1.37, ⫺1.36, and
1.24 degrees, respectively, in the grafted group compared with the nongrafted group (Table VII). However, they were of little clinical significance.
DISCUSSION
Secondary bone grafting of the alveolar cleft during the period of mixed dentition, in con-junction with orthodontic treatment, has be-come a well-accepted treatment modality for patients with unilateral complete cleft lip– cleft palate. Most cleft palate and craniofacial cen-ters support the use of secondary bone grafting because of the detrimental effects of primary
alveolar grafting on maxillary growth.3– 6
Pri-mary bone grafting also has a more severe impact on vertical than on sagittal growth of
the maxilla.38 Nevertheless, a few advocates of
primary bone grafting remain.39 – 42
TABLE III
Comparison of Means for the Grafted Group between Pre–Iliac Crest Alveolar Bone Graft and Follow-Up Stages
Variable
Pre–Iliac Crest Alveolar Bone Graft Stage
(mean⫾ SD) Follow-Up Stage (mean⫾ SD) Paired t Test (p) SNA, degrees 78.53⫾ 4.20 77.80⫾ 4.67 0.6074 SNB, degrees 75.85⫾ 3.81 77.08⫾ 4.40 0.3517 SNPog, degrees 76.07⫾ 4.01 77.58⫾ 4.66 0.2810 ANB, degrees 2.67⫾ 3.81 0.72⫾ 4.03 0.1235 SN/MP, degrees 36.50⫾ 6.00 35.82⫾ 6.47 0.7326 SN/PP, degrees 10.19⫾ 3.38 10.15⫾ 4.11 0.9780 PP/MP, degrees 26.31⫾ 5.38 25.67⫾ 5.58 0.7118 LI/MP, degrees 93.89⫾ 9.03 90.20⫾ 9.45 0.2146 SN/RP, degrees 92.18⫾ 4.60 92.03⫾ 4.36 0.9182 Gonial, degrees 124.32⫾ 5.21 123.78⫾ 5.39 0.7532 ANS-PNS, mm 46.56⫾ 2.81 48.66⫾ 3.03 0.0285* A-PtmI/PP, mm 44.75⫾ 2.91 46.18⫾ 3.08 0.1395 A-PNS, mm 43.73⫾ 2.94 44.56⫾ 2.85 0.3677
S, sella; N, nasion; PtmI, pterygomaxillare inferius; PNS, posterior nasal spine; ANS, anterior nasal spine; A, subspinale; B, supramentale; Pog, pogonion; SN, sella-nasion plane; PP, palatal plane; MP, mandibular plane; RP, ramal plane; LI, lower incisor.
Ideally, secondary bone grafting should be performed at the early transitional dentition stage, after the eruption of the permanent in-cisors but before the eruption of the
perma-nent maxillary canines.1,4,43– 45 The optimal
time for performing secondary alveolar bone grafting is probably between 7 and 12 years of
age,46 and the dental age needs to be
consid-ered. Bone grafting should be performed be-fore eruption of the canine in the cleft region when the root is one-fourth to two-thirds
formed.47At this period, the procedure would
be able to create an osseous environment that permits the spontaneous eruption or orth-odontic adjustment of the canine tooth. Be-cause sagittal and transverse growth is largely finished by 8 to 9 years of age,44,45 the chances
of interfering with maxillary growth are mini-mal after this age; however, vertical growth of the alveolar process is still going on. The ben-eficial effect of bone grafting before eruption of the canine is that, as the canine erupts, it induces deposition of bone on the alveolar crest and adds to the vertical height of the
maxilla.47 However, extensive mobility of the
palatal mucosa during surgery may result in reduced vertical development of the maxil-la.48,49Pearl and Kaplan50and Semb and Shaw51
failed to substantiate a significant effect of pha-ryngeal flaps on midfacial growth, whereas
Long and McNamara52 and Ren et al.53 found
increased vertical growth direction following surgery. The latter found the changes to be temporary and stated that the influence of a
pharyngeal flap on facial growth had no long-term clinical importance.
Based on principles suggested by Boyne and
Sands,1,2 the technique of secondary alveolar
bone grafting was introduced in Taiwan in 1982 and in southern Taiwan in 1987. Since then, most of the unilateral complete cleft lip– cleft palate cases with an average to favorable growth pattern have been recommended for bone grafting. Cases that exhibit a severe skel-etal discrepancy that would warrant orthog-nathic surgery at skeletal maturity are generally not considered for secondary alveolar bone grafting, because these patients could have maxillary advancement surgery with bone grafting at a later age. To prevent the introduc-tion of bias, the nongrafted group for this study was selected from patient records before 1987.
Thin-plate spline analysis shows the shape difference or deformation, which appears as
TABLE IV
Comparison of Means for the Nongrafted Group between Younger and Older Stages
Variable Younger Stage (mean⫾ SD) Older Stage (mean⫾ SD) Paired t Test (p) SNA, degrees 77.84⫾ 4.09 77.21⫾ 3.89 0.6176 SNB, degrees 79.25⫾ 2.86 79.34⫾ 3.21 0.9312 SNPog, degrees 79.11⫾ 3.08 79.55⫾ 3.57 0.6758 ANB, degrees –1.41⫾ 4.10 –2.13⫾ 4.31 0.5926 SN/MP, degrees 37.23⫾ 6.07 37.03⫾ 6.12 0.9175 SN/PP, degrees 10.25⫾ 3.28 11.46⫾ 3.82 0.2882 PP/MP, degrees 26.98⫾ 6.10 25.57⫾ 6.51 0.4837 LI/MP, degrees 88.11⫾ 8.46 86.19⫾ 8.10 0.4687 SN/RP, degrees 88.39⫾ 3.13 89.21⫾ 3.78 0.4614 Gonial, degrees 128.84⫾ 6.02 127.82⫾ 5.72 0.5865 ANS-PNS, mm 44.07⫾ 3.44 46.10⫾ 4.03 0.0963 A-PtmI/PP, mm 42.35⫾ 3.56 44.11⫾ 4.29 0.1670 A-PNS, mm 40.97⫾ 3.53 42.26⫾ 4.06 0.2903
S, sella; N, nasion; PtmI, pterygomaxillare inferius; PNS, posterior nasal spine; ANS, anterior nasal spine; A, subspinale; B, supramentale; Pog, pogo-nion; SN, sella-nasion plane; PP, palatal plane; MP, mandibular plane; RP, ramal plane; LI, lower incisor.
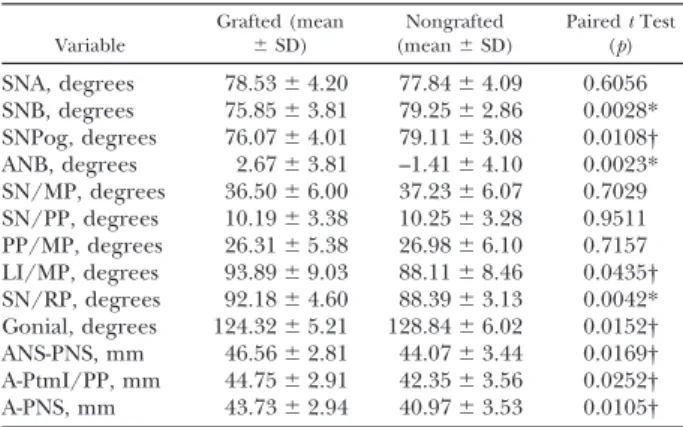
TABLE V
Comparison of Means for the Grafted and Nongrafted Groups at Younger or Pre–Iliac Crest Alveolar Bone
Graft Stage Variable Grafted (mean ⫾ SD) (meanNongrafted⫾ SD) Paired t Test (p) SNA, degrees 78.53⫾ 4.20 77.84⫾ 4.09 0.6056 SNB, degrees 75.85⫾ 3.81 79.25⫾ 2.86 0.0028* SNPog, degrees 76.07⫾ 4.01 79.11⫾ 3.08 0.0108† ANB, degrees 2.67⫾ 3.81 –1.41⫾ 4.10 0.0023* SN/MP, degrees 36.50⫾ 6.00 37.23⫾ 6.07 0.7029 SN/PP, degrees 10.19⫾ 3.38 10.25⫾ 3.28 0.9511 PP/MP, degrees 26.31⫾ 5.38 26.98⫾ 6.10 0.7157 LI/MP, degrees 93.89⫾ 9.03 88.11⫾ 8.46 0.0435† SN/RP, degrees 92.18⫾ 4.60 88.39⫾ 3.13 0.0042* Gonial, degrees 124.32⫾ 5.21 128.84⫾ 6.02 0.0152† ANS-PNS, mm 46.56⫾ 2.81 44.07⫾ 3.44 0.0169† A-PtmI/PP, mm 44.75⫾ 2.91 42.35⫾ 3.56 0.0252† A-PNS, mm 43.73⫾ 2.94 40.97⫾ 3.53 0.0105†
S, sella; N, nasion; PtmI, pterygomaxillare inferius; PNS, posterior nasal spine; ANS, anterior nasal spine; A, subspinale; B, supramentale; Pog, pogo-nion; SN, sella-nasion plane; PP, palatal plane; MP, mandibular plane; RP, ramal plane; LI, lower incisor.
* p⬍ 0.01. † p⬍ 0.05.
TABLE VI
Hotelling’s T2of Mean Craniofacial Configurations in the
Grafted and Nongrafted Groups at Younger or Pre–Iliac Crest Alveolar Bone Graft Stage*
Variable Hotelling’s T2 p
Linear 15.8308 0.0578
Angular 41.2763 0.0073†
* Mean values of 10 angular and three linear measurements for the non-grafted and non-grafted groups at younger or pre–iliac crest alveolar bone graft stage listed in Table V.
vertical compression/extension and/or hori-zontal compression/extension of the grids on the graphical displays when the younger and the older stage lateral cephalographs are su-perimposed and the landmark configurations
compared.32 Although the thin-plate spline
analysis is unable to determine whether there is a statistical difference between mean config-urations, it allows the visualization of the dif-ferences as a transformation grid, whether these are statistically significant or not. There-fore, to determine whether the craniofacial
TABLE VII
Analysis of Covariance Tests for Growth of Craniofacial Variables in the Grafted and Nongrafted Groups at Older or Follow-Up Stages
Variable
Parameter
Estimate SE t Ratio p
SNA, degrees
Grafted versus nongrafted 0.04 0.65 0.06 0.9547
Male versus female –0.08 0.70 –0.11 0.9115
SNA at T1 0.08 0.08 0.98 0.3335
SNB, degrees
Grafted versus nongrafted –1.37 0.52 –2.62 0.0128*
Male versus female –0.24 0.49 –0.48 0.6310
SNB at T1 –0.07 0.07 –0.94 0.3522
SNPog, degrees
Grafted versus nongrafted –1.36 0.47 –2.92 0.0061†
Male versus female –0.07 0.45 0.16 0.8752
SNPog at T1 –0.10 0.06 –1.60 0.1174
ANB, degrees
Grafted versus nongrafted 1.11 0.60 1.86 0.0713
Male versus female –0.04 0.55 –0.08 0.9406
ANB at T1 0.03 0.07 0.44 0.6602
SN/MP, degrees
Grafted versus nongrafted 0.49 0.58 0.84 0.4075
Male versus female –0.70 0.62 –1.14 0.2606
SN/MP at T1 0.01 0.05 0.21 0.8372
SN/PP, degrees
Grafted versus nongrafted 1.24 0.60 2.07 0.0460*
Male versus female 0.79 0.63 1.25 0.2181
SN/PP at T1 –0.05 0.09 –0.54 0.5919
PP/MP, degrees
Grafted versus nongrafted –0.71 0.86 –0.82 0.4152
Male versus female –1.62 0.91 –1.78 0.0840
PP/MP at T1 0.08 0.08 1.08 0.2892
LI/MP, degrees
Grafted versus nongrafted 0.73 1.77 0.41 0.6829
Male versus female –0.16 1.82 –0.09 0.9306
L1/MP at T1 0.18 0.10 1.77 0.0853
SN/RP, degrees
Grafted versus nongrafted 0.70 0.66 1.07 0.2937
Male versus female –0.35 0.62 –0.56 0.5781
SN/RP at T1 0.07 0.08 0.88 0.3861
Gonial angle, degrees
Grafted versus nongrafted 0.00 0.78 0.00 0.9985
Male versus female –0.59 0.78 –0.76 0.4493
Gonial angle at T1 0.11 0.07 1.60 0.1182
ANS-PNS, mm
Grafted versus nongrafted –0.20 0.68 –0.30 0.7695
Male versus female –0.01 0.66 –0.01 0.9886
ANS-PNS at T1 0.05 0.10 0.47 0.6399
A-PNS, mm
Grafted versus nongrafted 0.20 0.68 0.29 0.7722
Male versus female 0.35 0.65 0.54 0.5926
A-PNS at T1 0.09 0.10 0.96 0.3446
A-PtmI/PP, mm
Grafted versus nongrafted 0.22 0.71 0.31 0.7565
Male versus female –0.31 0.70 –0.44 0.6640
A-PtmI/PP at T1 0.04 0.11 0.41 0.6877
S, sella; N, nasion; PtmI, pterygomaxillare inferius; PNS, posterior nasal spine; ANS, anterior nasal spine; A, subspinale; B, supramentale; Pog, pogonion; SN, sella-nasion plane; PP, palatal plane; MP, mandibular plane; RP, ramal plane; LI, lower incisor. T1, younger or pre-ABG stage.
* p⬍ 0.05. † p⬍ 0.01.
configurations between the younger or pre– iliac crest alveolar bone graft and the older or follow-up stages are morphologically different, we relied on the residuals of homologous land-marks from Procrustes analysis.18,19,37
As can be seen, the measured variables of palatomaxillary complex length demonstrated significant differences between the two groups at the younger stage. There were also signifi-cant differences found in the variables of man-dibular position. These findings represent a preexisting difference between the group to receive bone grafts and their matched controls. On the contrary, there was lack of significant difference between the two groups in the mea-sured variables of palatomaxillary complex length at the older stage. However, inspection of thin-plate spline transformation grids in Fig-ures 2 and 3 would suggest a trend for the grafted group to become more relatively max-illary retrusive after grafting.
Even in a successfully treated complete uni-lateral cleft lip– cleft palate patient, the charac-teristics of the cleft face are always there. The patients with clefts clearly exhibit the underly-ing potential for class III growth or midfacial deficiency as the result of the original defor-mity and subsequent multiple operations nec-essary for its repair. It has been suggested that growth deficiencies of children with unilateral cleft lip– cleft palate do not become manifest until adolescence. In this study, the final ceph-alometric film was obtained 1 to 3 years after the repair procedure, which was before the cessation of the patient’s growth. The long-term effects of both the intrinsic growth and the external therapies applied to remedy the craniofacial deficiencies in the unilateral com-plete cleft lip– cleft palate patient are especially
evident during the pubertal growth period.49
Therefore, the possibility of a significant differ-ence becoming evident if the patients had been examined once they had grown through adolescence and had reached skeletal maturity cannot be ruled out.
CONCLUSIONS
Secondary alveolar cleft bone grafting at the mixed dentition stage seems to cause no delete-rious effects on the growth of the midface and maxillary growth in general after a 1- to 3-year observation period. Thin-plate spline analysis may show the degree of transformation within the craniofacial geometric configuration attribut-able to maxillofacial growth changes, primarily
caused by intrinsic growth and surgically induced scar tissues, as seen on lateral cephalometric ra-diographs. Longitudinal studies of patients are required to fully appreciate the long-term impli-cations, using Procrustes analysis and thin-plate spline graphical analysis corroborated by conven-tional cephalometric analysis.
Hong-Po Chang, D.M.D., Ph.D. Department of Orthodontics Faculty of Dentistry
Kaohsiung Medical University 100 Shih-Chuan 1st Road Kaohsiung 80708, Taiwan [email protected].
ACKNOWLEDGMENT
This study was supported in part by the National Science Council, Taiwan (NSC 90-2314-B-037-087).
REFERENCES
1. Boyne, P. J., and Sands, N. R. Secondary bone grafting of residual alveolar and palatal clefts. J. Oral Surg. 30: 87, 1972.
2. Boyne, P. J., and Sands, N. R. Combined orthodontic surgical management of residual alveolar cleft defects.
Am. J. Orthod. 70: 20, 1976.
3. El Deeb, M., Messer, L. B., Lehnert, M. W., Hebda, T. W., and Waite, D. E. Canine eruption into grafted bone in maxillary alveolar cleft defects. Cleft Palate J. 19: 9, 1982. 4. Åbyholm, F., Bergland, O., and Semb, G. Secondary bone grafting of alveolar clefts. Scand. J. Plast. Reconstr.
Surg. 15: 127, 1981.
5. Turvey, T., Vig, K., Moriarty, J., and Hoke, J. Delayed bone grafting in the cleft maxilla and palate: A ret-rospective multidisciplinary analysis. Am. J. Orthod. 6: 244, 1986.
6. El Deeb, M., Hinrichs, J. E., Waite, D. E., Bandt, C. L., and Bevis, R. Repair of alveolar cleft defects with autog-enous bone grafting: Periodontal evaluation. Cleft
Pal-ate J. 23: 126, 1986.
7. Bertz, J. E. Bone grafting of alveolar clefts. J. Oral Surg. 39: 874, 1981.
8. Hall, H. D., and Posnick, J. C. Early results of secondary bone grafts in 106 alveolar clefts. J. Oral Maxillofac.
Surg. 41: 289, 1983.
9. Graber, T. M. Craniofacial morphology in cleft palate and cleft lip deformity. Surg. Gynecol. Obstet. 88: 359, 1949. 10. Graber, T. M. The congenital cleft palate deformity.
J. Am. Dent. Assoc. 48: 375, 1954.
11. Slaughter, W. S., and Brodie, A. G. Facial clefts and their surgical management in view of recent research.
Plast. Reconstr. Surg. 4: 311, 1949.
12. Ross, R. B. Treatment variables affecting facial growth in complete unilateral cleft lip and palate: Part 3. Alveolar repair and bone grafting. Cleft Palate J. 24: 33, 1987. 13. Semb, G. Effect of alveolar bone grafting on maxillary
growth in unilateral cleft lip and palate patients. Cleft
Palate J. 25: 288, 1988.
14. Daskalogiannakis, J., and Ross, R. B. Effect of alveolar bone grafting in the mixed dentition on maxillary
growth in complete unilateral cleft lip and palate pa-tients. Cleft Palate Craniofac. J. 34: 455, 1997. 15. Levitt, T., Long, R. E., Jr., and Trotman, C. A. Maxillary
growth in patients with clefts following secondary alve-olar bone grafting. Cleft Palate Craniofac. J. 36: 398, 1999. 16. Moyers, R. E., and Bookstein, F. L. The inappropriate-ness of conventional cephalometrics. Am. J. Orthod. 75: 599, 1979.
17. Bookstein, F. L. On the cephalometrics of skeletal change. Am. J. Orthod. 82: 177, 1982.
18. Rohlf, F. J., and Slice, D. Extensions of the Procrustes method for the optimal superimposition of land-marks. Syst. Zool. 39: 40, 1990.
19. Goodall, C. R. Procrustes methods in the statistical anal-ysis of shape (with discussion and rejoinder). J. R. Stat.
Soc. (B) 53: 285, 1991.
20. Bookstein, F. L. Principal warps: Thin-plate splines and the decomposition of deformations. I.E.E.E. Trans.
Pattern Anal. Mach. Intell. 11: 567, 1989.
21. Bookstein, F. L. Morphometric Tools for Landmark Data.
Cambridge: Cambridge University Press, 1991. 22. Grayson, B. H., Santiago, P. E., Brecht, L. E., and Cutting,
C. B. Presurgical nasoalveolar molding in infants with cleft lip and palate. Cleft Palate Craniofac. J. 36: 486, 1999.
23. Millard, D. R. Refinements in rotation-advancement cleft lip technique. Plast. Reconstr. Surg. 33: 26, 1964. 24. Millard, D. R. Extensions of the rotation-advancement principle for wide unilateral cleft lips. Plast. Reconstr.
Surg. 37: 535, 1968.
25. Bardach, J., Hogan, M., and Salyer, K. E. Two flap pal-atoplasty technique. In J. Bardach (Ed.), Surgical
Tech-niques in Cleft Lip and Palate: Fifth Annual Workshop.
New York: Institute of Reconstructive Plastic Surgery, 1982. Pp. 1-19.
26. Bardach, J. Cleft palate repair: Two flap palatoplasty. Research, philosophy, technique and results. In J. Bar-dach and H. L. Morris (Eds.), Multidisciplinary
Man-agement of Cleft Lip and Palate. Philadelphia: Saunders,
1990. Pp. 352-365.
27. Chen, K. T., and Noordhoff, M. S. Open tip rhinoplasty.
Ann. Plast. Surg. 28: 119, 1992.
28. Sloan, G. M. Posterior pharyngeal flap and sphincter pharyngoplasty: The state of the art. Cleft Palate
Cranio-fac. J. 37: 112, 2000.
29. Huang, F., Tsao, S. B., Wong, R., et al. Retrospective analysis of 1175 cleft lip and palate patients in Kao-hsiung Chang Gung Memorial Hospital. J. Plast.
Re-constr. Surg. Assoc. R.O.C. 5: 78, 1996.
30. Chang, H. P., Liao, C. H., Yang, Y. H., Chang, H. F., and Chen, K. C. Correlation of cervical vertebra matu-ration with hand-wrist matumatu-ration in children.
Kaohsi-ung J. Med. Sci. 17: 29, 2001.
31. Baccetti, T., Franchi, L., and McNamara, J. A., Jr. The cer-vical vertebral maturation method: Some need for clari-fication. Am. J. Orthod. Dentofac. Orthop. 123: 19A, 2003. 32. Chang, H. P., Liu, P. H., Chang, H. F., and Chang, C. H. Thin-plate spline (TPS) graphical analysis of the man-dible on cephalometric radiograph. Dentomaxillofac.
Radiol. 31: 137, 2002.
33. Houston, W. J. B. The analysis of errors in orthodontic measurements. Am. J. Orthod. 83: 382, 1983. 34. Hotelling, H. Relations between two sets of variates.
Biometrika 28: 321, 1936.
35. Rohlf, F. J. Statistical power comparisons among alter-native morphometric methods. Am. J. Phys. Anthropol. 111: 463, 2000.
36. Dryden, I. L., and Mardia, K. V. Statistical Shape Analysis.
New York: Wiley, 1998.
37. Rohlf, F. J., and Marcus, L. F. A revolution in morpho-metrics. Trends Ecol. Evol. 8: 129, 1993.
38. Sameshima, G. T., Banh, D. S., Smahel, Z., and Melnick, M. Facial growth after primary periosteoplasty versus primary bone grafting in unilateral cleft lip and palate.
Cleft Palate Craniofac. J. 33: 300, 1996.
39. Rosenstein, S. W., Jacobson, B. N., Monroe, C., Griffith, B. H., and McKinney, P. A series of cleft lip and palate children five years after undergoing orthopedic and bone grafting procedures. Angle Orthod. 42: 1, 1972. 40. Rosenstein, S. W., Monroe, C. W., Kernahan, D. A.,
Ja-cobson, B. N., Griffith, B. H., and Bauer, B. S. The case of early bone grafting in cleft lip and cleft palate.
Plast. Reconstr. Surg. 70: 297, 1982.
41. Rosenstein, S. W., Dado, D. V., Kernahan, D. A., Griffith, B. H., and Grasseschi, M. The case of early bone grafting in cleft lip and cleft palate: A second report.
Plast. Reconstr. Surg. 87: 644, 1991.
42. Rosenstein, S. W., Grasseschi, M., and Dado, D. V. A long-term retrospective outcome assessment of facial growth, secondary surgical need, and maxillary lateral incisor status in a surgical-orthodontic protocol for complete clefts. Plast. Reconstr. Surg. 111: 1, 2003. 43. Sindet-Pederson, S., and Enemark, H. Comparative study
of secondary and late bone-grafting in patients with re-sidual cleft defects. Int. J. Oral Surg. 14: 389, 1985. 44. Bergland, O., Semb, G., and Åbyholm, F. Elimination of
residual alveolar clefts by secondary bone grafting and sub-sequent orthodontic treatment. Cleft Palate J. 23: 175, 1986. 45. Bergland, O., Semb, G., Borchgrevinck, H., and Esland, G. Secondary bone grafting and orthodontic treat-ment in patients with bilateral complete clefts of lip and palate. Ann. Plast. Surg. 17: 460, 1986.
46. Witsenburg, B. The reconstruction of anterior residual bone defects in patients with cleft lip alveolus and palate: A review. J. Maxillofac. Surg. 13: 197, 1985. 47. Kortebein, M. J., Nelson, C., and Sadove, A. M.
Retro-spective analysis of 135 secondary alveolar cleft grafts using iliac or calvarial bone. J. Oral Maxillofac. Surg. 49: 493, 1991.
48. Enemark, H., Simonsen, E. K., and Schramm, J. E. Sec-ondary bone grafting in unilateral cleft lip and palate patients: Indications and treatment procedures. Int.
J. Oral Surg. 14: 2, 1985.
49. Enemark, H., Sindet-Pederson, S., and Bundgaard, M. Long-term results after secondary bone grafting of alveolar clefts. J. Oral Maxillofac. Surg. 45: 913, 1987. 50. Pearl, R. M., and Kaplan, E. N. Cephalometric study of facial growth in children after combined pushback and pharyngeal flap operations. Plast. Reconstr. Surg. 57: 480, 1976.
51. Semb, G., and Shaw, W. C. Pharyngeal flap and facial growth. Cleft Palate J. 27: 217, 1990.
52. Long, R. E., Jr., and McNamara, J. A., Jr. Facial growth following pharyngeal flap surgery: Skeletal assessment on serial lateral cephalometric radiographs. Am. J.
Orthod. 87: 187, 1985.
53. Ren, Y. F., Isberg, A., and Henningsson, G. The influ-ence of pharyngeal flap on facial growth: Long-term results in the patients with isolated cleft palate. Scand.