原發性顫抖症:臨床分析及單光子射出性斷層掃描 ( 99m Tc-ECD SPECT)的表現; Essential tremor: clinical analysis and 99m Tc-ECD SPECT findings
61
0
0
全文
(2) 2.
(3) Essential tremor: clinical analysis and 99m Tc-ECD SPECT findings ABSTRACT Background Essential tremor (ET) is the most prevalent movement disorder. The diagnosis is based on clinical findings, and its treatment is mainly symptomatic. The pathogenesis of ET is unknown. Some pieces of evidence suggest that the olivo-cerebello-thalamo-cortical circuitry is pivotal for the development of essential tremor. Previous studies with positron emission tomography (PET) have revealed an alternation of the regional cerebral blood flow (rCBF) in ET patients. However PET is not universally available as compared with single photon emission computed tomography (SPECT). The aim of this study was to evaluate the potential usefulness of technetium-99m ethyl cysteinate dimer (99m Tc ECD) SPECT in detecting the possible alternation of brain perfusion in patients with ET.. 3.
(4) Methods In this study, 25 ET patients with normal findings on brain magnetic resonance imaging (MRI) were examined with a 99m Tc ECD SPECT of the brain to detect the status of the regional cerebral blood flow.. Results Relative hypoperfusion was found in the thalamus, basal ganglia, temporal lobe, and frontal lobe. Among these spots, only the perfusion of the thalamic region contralateral to the more vigorous tremor side was found to be significantly diminished. No statistically significant difference was present in either the basal ganglia or the cerebellum. The decrease in rCBF was irrelevant to the tremor severity and duration of tremor.. Conclusion Our study demonstrates that hypoperfusion of the thalamic region can be detected by 99mTc-ECD brain SPECT in patients with ET, which implies that the thalamus might be crucial for 4.
(5) the generation or modulation of ET. In addition, the finding also strengthens the viewpoint that this SPECT technique is an appropriate and convenient tool for the investigation of ET or other sorts of tremor.. Key Words: Essential tremor, Cerebral blood flow; SPECT; Technetium-99m-ethylcysteinate dimer (99mTc-ECD);. 5.
(6) 原發性顫抖症:臨床分析及單光子射出性斷層掃 描 ( 99m Tc-ECD SPECT)的表現. 摘. 要. 背景 原發性顫抖症(Essential Tremor)是動作障礙疾病中最常見 的。診斷是根據臨床的表現,而它的治療主要是症狀改善。 原發性顫抖症的病因不明。有一些證據認為橄欖核-小腦視丘 腦皮質傳導迴路是產生原發性顫抖症的重要原因。先前以正 子電腦斷層掃描儀(positron emission tomography, PET)的研 究顯示原發性顫抖症患者局部腦血流的改變。不過與單光子 射出性斷層掃描(single photon emission computed tomography, SPECT)比較,正子掃描無法廣泛的被應用。這個研究的目的 是要評估使用 technetium-99m ethyl cysteinate dimer (99m Tc ECD)單光子射出性斷層掃描來偵測原發性顫抖症患者腦部 灌流改變的潛在可行性。. 方法 在這個研究中,針對25位有正常腦部核磁共振影像的原發性 6.
(7) 顫抖症患者實施99m Tc ECD單光子射出性斷層掃描檢查來 偵測局部腦部血流的狀態。. 結果 在視丘、基底核、顳葉及額葉有相對較低灌流的發現。在這 些區域,以較厲害顫抖肢體的對側視丘有著顯著減少的灌 流。在基底核或小腦部位的腦血流差異,則沒有統計學上的 意義。局部腦血流的減少與顫抖的嚴重度及顫抖的存在期間 並無相關。. 結論 我們的研究顯示原發性顫抖症患者視丘部位的血液灌流降 低可以99m Tc ECD單光子射出性斷層掃描檢查來偵測出。這 個結果暗示著視丘可能是產生或調節原發性顫抖症的重要 部位。此外,這個發現給我們一個觀點,就是以單光子射出 性斷層掃描的檢查來探查原發性顫抖症或其他種類的顫抖 症是合適而且便利的工具。. 7.
(8) 關鍵詞:原發性顫抖症,腦部血流,單光子射出性斷層掃描, Technetium-99m-ethylcysteinate dimmer (99mTc-ECD)。. 8.
(9) 本文重要性 由本文的實驗結果,發現在 thalamus 的局部血流降低,具有 統計學上的義意。其他構造是否也有類似情形,需要較多的 病患人數及解像力更佳的 SPECT scan 儀器,或許可得到更 有價值的成果。這可以對原發性顫抖症的病理機轉提供另一 種解釋,並對它的治療方向及臨床評估,提供追蹤療效的工 具。 這個實驗的發現得知 SPECT scan 可以提供客觀的局部血流 數據,所以針對原發性顫抖症病患的研究,它可當作一個工 作平台,例如:台灣人的原發性顫抖症病患的研究、基因定 序、與周邊肌電圖的整合、及治療藥物的開發與療效追蹤等。 此外,由於 SPECT scan 的價格便宜,操作手續較 PET scan 簡單,適合在臨床上推廣使用。. 9.
(10) 誌謝 這篇研究論文的順利完成,需要感謝許多人。台中榮民總醫 院神經內科王寶玉大夫的諮詢指引及校稿,中國醫藥學院附 設醫院核醫科高嘉鴻主任的鼓勵與臨床指導及其核醫團隊 的協助幫忙,及該院神經內科蔡崇豪主任的文章校稿及指 正,這些都是促使這篇碩士論文能得到完美句點的助力。相 信這也是讓這個實驗能朝下一步繼續研究推廣的動力。 兩年的碩士求學生活加上繁重的臨床業務,是緊湊又充實 的。在此,需特別感謝中國醫藥學院醫學系沈戊忠主任的關 心、包容與指導,讓我得以平順完成學業。. 10.
(11) Preface Page. 學位考試委員審定書影本. -----------------------------. 2. Abstract (English) ----------------------------------------. 3. Abstract (中文) -------------------------------------------. 6. 本文重要性 誌謝. ------------------------------------------------. 9. --------------------------------------------------------- 10. Preface ------------------------------------------------------- 11 Introduction ------------------------------------------------- 13 Incidence ---------------------------------------------------- 13 Classification ----------------------------------------------- 14 Symptoms and Signs -------------------------------------- 16 Mortality and Morbidity ---------------------------------- 17 Differential Diagnosis ------------------------------------ 17 Diagnostic Criteria ---------------------------------------- 21 Genetic Research ------------------------------------------ 23 Workup ----------------------------------------------------- 23 Pathophysiology ------------------------------------------ 24 Methods and Materials ----------------------------------- 30 11.
(12) Patients ---------------------------------------------------- 30 99m TC-ECD SPECT ----------------------------------- 32 Data Analysis --------------------------------------------- 34 Visual Assessment --------------------------------------- 34 Semiquantative Assessments --------------------------- 34 Statistical Analysis --------------------------------------- 36 Results ------------------------------------------------------ 36 Discussion ------------------------------------------------- 37 Future Planning ------------------------------------------- 43 References ------------------------------------------------- 45 Appendix- A. Table --------------------------------------- 48 Appendix- B. Figure -------------------------------------- 58 About the Author ----------------------------------------- 61 博碩士頓文電子檔案上網授權書 ---------------------- 62. 12.
(13) n Introduction Essential tremor (ET) is a common neurologic movement disorder, and is characterized by a 4 to 12 Hz postural tremor affecting the distal part of the upper limbs (1). Tremors may affect the head, hands, arms, eyelids, voice, less commonly affects the legs and feet. Both sexes are equally affected. Head tremor is more frequent in women. Postural hand tremor is more severe in men.. n Incidence It affects all age groups, with a bimodal peak of onset occurring in the second and sixth decades (2). The prevalence is from 0.3 to 5.5% in the over-40 age group, as demonstrated in various reports (3). Rare cases of ET have been reported in newborns and infants. (Figure 1) Although ET is progressive, no association has been found between age of onset and severity or disability.. 13.
(14) The prevalence of ET increasing with age.. n Classification Tremor is an involuntary, rhythmic, oscillating movement of reciprocally innervated, antagonistic muscle groups that causes displacement of a body part within a fixed plane. It is often classified according to the conditions that activate it (Table 1). Tremor of a body part that is completely supported against gravity is known as a rest tremor, whereas tremor during voluntary muscle contraction is an action tremor. Action tremor is further classified as postural (tremor in a body part maintained in a position against gravity), isometric (muscle contraction against a rigid stationary object), or kinetic (tremor occurring during voluntary movement). Isolated tremor of a body part 14.
(15) does not constitute essential tremor. However, some experts consider conditions such as primary writing tremor, orthostatic tremor (shaky legs syndrome), isolated voice tremor, isolated head tremor, and task-specific tremors as variants, or formes frustes, of essential tremor.. Table 1. Circumstances that activate various types of tremor Circumstance. Tremor type. Resting. Parkinsonian Rubral*. Posture. Dystonic* Enhanced physiologic Essential Orthostatic Psychogenic Rubral*. Kinesis. Cerebellar Dystonic** Rubral**. 15.
(16) n Symptoms and Signs It may not affect both sides of the body equally. Tremor involves the cranial musculature in about 30% of cases. It usually affects both upper extremities. It begins in one upper extremity and soon affecting the other. It rarely extends from the upper extremity to the ipsilateral leg. Voluntary movement can usually make the tremor more vigorous, while rest will abolish it. It is worsening with emotion stress, exercise and fatigue, and disappears during sleep. Essential tremor typically improves after alcohol (4). Tremor amplitude slowly increases over time. The amplitude is highly variable depending on the state of emotional activation. It was worsened by emotion, hunger, fatigue, and temperature extremes. The baseline amplitude slowly increasing over several years. It could be suppressed by skilled manual tasks. Temporarily reducing tremor amplitude by ethanol intake in an estimated 50-70% of cases. Tremor frequency decreases with increasing age. An 8- to 12-Hz tremor is seen in young adults and a 6- to 8-Hz tremor is seen in the elderly. 16.
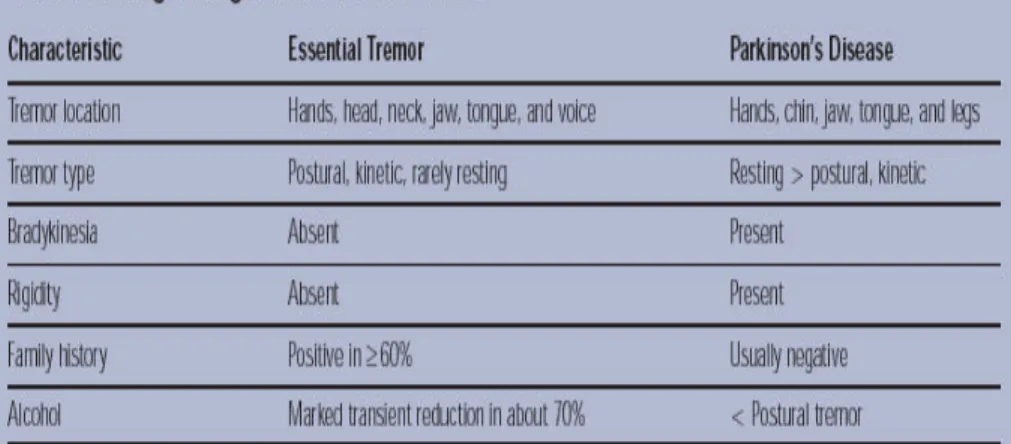
(17) Fig 2 Hand-writing of essential tremor patients.. n Mortality and Morbidity Mortality rates are not increased in patients with ET. However, disability from ET is common. Eighty-five percent of individuals with ET report significant changes in their livelihood and socializing. Fifteen percent report being seriously disabled by ET. Decreased quality of life results from both loss of function and embarrassment. In a study of hereditary ET, 60% of affected individuals did not seek employment; 25% changed jobs or took early retirement; 65% did not dine out; 30% did not attend parties, shop alone, partake of a favorite hobby or sport; and 20% stopped driving.. n Differential Diagnosis Essential tremor is most commonly confused with Parkinson's disease, enhanced physiologic tremor, and dystonic tremor. If 17.
(18) the tremor is asymmetric and occurs at rest from the onset, the diagnosis is most likely Parkinson's disease. Unlike essential tremor, Parkinson's disease manifests other signs, including bradykinesia, shuffling gait, postural instability, masked facies, micrographic handwriting, pill-rolling tremor, and hypokinetic speech. Enhanced physiologic tremor is a postural, fine tremor of high frequency (8 to 12 Hz) that most often accompanies alcohol or drug intoxication, anxiety, and endocrine malfunction (Table 2,3,4). Dystonic tremor, particularly of the head, may be confused with the head tremor of essential tremor. Unlike dystonic head tremor, essential head tremor often presents with a "null point" (ie, a certain head position or tilt that minimizes the tremor). Dystonic head tremor typically increases as the head is turned opposite the direction of pull. Essential voice tremor is also sometimes confused with spasmodic dysphonia, which can sound tremulous. However, the latter has either a strangulated, crackling character (adductor spasmodic dysphonia) or a breathy quality (abductor spasmodic dysphonia). The presence of a strong family history 18.
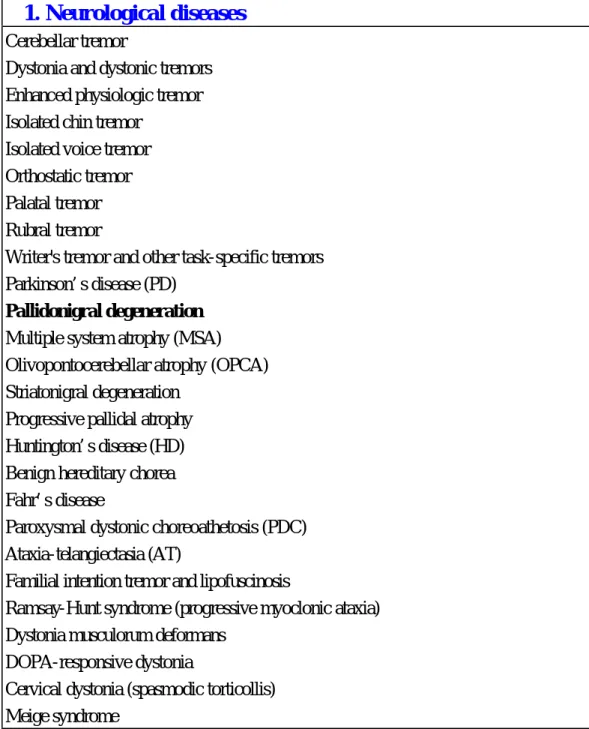
(19) of tremor and marked reduction of tremor with alcohol intake helps distinguish essential tremor from other tremor disorders. It is not associated with any disease and without parkinsonian, cerebellar, or other neurologic signs (5). Table 2. Differential Diagnosis of Tremor. 1. Neurological diseases Cerebellar tremor Dystonia and dystonic tremors Enhanced physiologic tremor Isolated chin tremor Isolated voice tremor Orthostatic tremor Palatal tremor Rubral tremor Writer's tremor and other task-specific tremors Parkinson’s disease (PD) Pallidonigral degeneration Multiple system atrophy (MSA) Olivopontocerebellar atrophy (OPCA) Striatonigral degeneration Progressive pallidal atrophy Huntington’s disease (HD) Benign hereditary chorea Fahr’s disease Paroxysmal dystonic choreoathetosis (PDC) Ataxia-telangiectasia (AT) Familial intention tremor and lipofuscinosis Ramsay-Hunt syndrome (progressive myoclonic ataxia) Dystonia musculorum deformans DOPA-responsive dystonia Cervical dystonia (spasmodic torticollis) Meige syndrome 19.
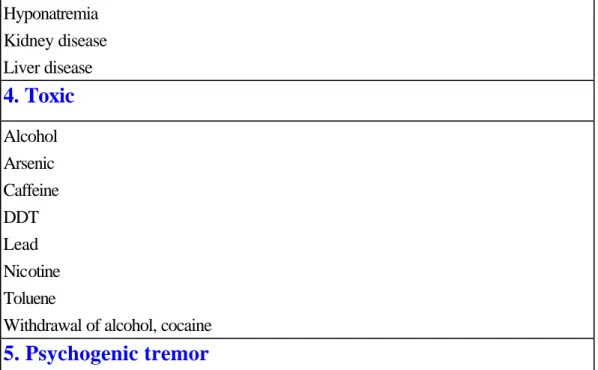
(20) Task-specific tremors (writer’s or voice tremor) Space-occupying lesions of the brain Peripheral neuropathies (e.g., Charcot-Marie-Tooth, Guillain-Barré, etc.). 2. Drug-induced tremors Antidepressants, especially tricyclics Beta-agonists Depakote Dopamine Lithium Metoclopramide Neuroleptics Theophylline Thyroid hormones Withdrawal of drugs. 3. Metabolic B-12 deficiency Hyperthyroidism Hyperparathyroidism Hypocalcemia Hyponatremia Kidney disease Liver disease. 4. Toxic Alcohol Arsenic Caffeine DDT Lead Nicotine Toluene Withdrawal of alcohol, cocaine. 5. Psychogenic tremor. 20.
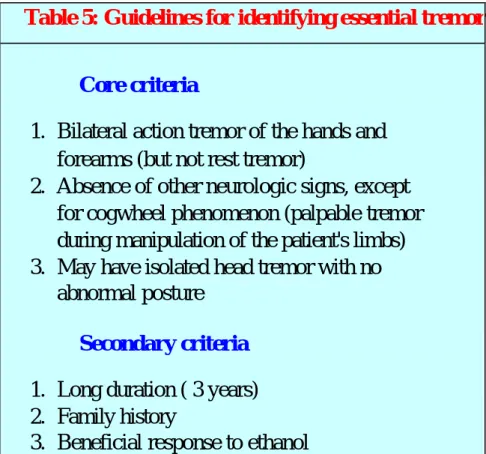
(21) Table 3. Table 4 Classic distinguishing festures of PD and ET.. n Diagnostic Criteria (Table 5) 1.Positive family history of essential tremor. 2.Positive patient history of action tremor beginning in teens or any age for no apparent reason. 3.Evidence of flexion/extension action tremor beginning in the finger/hand, especially the dominant hand. 21.
(22) 4.Positive finger-to-nose test revealing tremor while holding arms outstretched or while moving the finger or hand toward an object. 5.Action tremor worsens as person ages. 6. Possible evidence of head nodding, rest tremor and cogwheel rigidity developing later. 7. No evidence of Parkinson's disease. 8. No evidence of cerebellar disease. 9. No evidence of neurological or other disease. 10. Temporarily relived by alcohol consumption. Table 5: Guidelines for identifying essential tremor Core criteria 1. Bilateral action tremor of the hands and forearms (but not rest tremor) 2. Absence of other neurologic signs, except for cogwheel phenomenon (palpable tremor during manipulation of the patient's limbs) 3. May have isolated head tremor with no abnormal posture Secondary criteria 1. Long duration ( 3 years) 2. Family history 3. Beneficial response to ethanol 22.
(23) Genetic Research There is often a family history of the disorder and approximately 50% of cases have a genetic link with an autosomal dominant disorder. Thus, genetic factors play much more of a role in essential tremor than in Parkinson disease. Several susceptibility loci (autosomal dominant gene) recently have been reported to be genetically linked to dominantly inherited essential tremor. Markers for two genes have been discovered on chromosomes 2 and 3, and additional genes are expected. These include loci in chromosome arm 2p (ETM gene) and band 3q13 (FET1 gene) (11). The cause of essential tremor in people without the genetic mutation is unknown. Having a parent with the disorder increases the risk (12).. n Workup In laboratory studies, there are no biological markers exist for ET. If the family history and examination are indicative of ET, no laboratory or imaging studies are required. If the family. 23.
(24) history and examination are not indicative of ET, laboratory and imaging studies should be considered. Laboratory investigations include standard electrolyte panel, thyroid function tests, BUN, creatinine, liver function tests, and serum ceruloplasmin (for Wilson disease). In imaging studies, the CT scan and MR examination must reveal normal imaging without identified lesions. MRI helps exclude structural and inflammatory lesions (including multiple sclerosis) and Wilson disease. MRI should be performed if the tremor has a history of acute onset or stepwise progression. The electromyography or accelerometry can be used to assess tremor frequency, rhythmicity, and amplitude but are not part of the routine evaluation.. n Pathophysiology There is no specific diagnostic laboratory test for the early diagnosis of ET and diagnosis is mainly based on the clinical features. Its pathophysiologic mechanisms remain unclear.. 24.
(25) There were no consistent lesions have been found at postmortem examinations (13). Much debate exists on the pathophysiologic basis of ET. The underlying mechanism of essential tremor is not known although several theories have been proposed. A group of drugs known as beta-adrenergic blockers such as propranolol are known to improve the symptoms associated with ET. Peripheral mechanisms have also been suggested in ET, mainly because β-blockers that do not easily cross the blood and brain barrier (such as nadolol) can still attenuate tremor. It is possible that these beta-blockers work through peripheral beta2 skeletal muscle adrenoreceptors (receptor mechanisms). However, beta-blockers may also affect central pathways. There is evidence, however, that β-blockers may work centrally as well as peripherally, as nonselective blockade of β2 receptors may improve tremor control. It was reported that alcohol suppression of ET is mediated through a reduction in overactivity (cerebellar synaptic), resulting in an increased afferent input to the inferior olivary 25.
(26) nuclei. The ingestion of ethanol led to bilateral decreases of cerebellar blood flow in both tremor patients and normal subjects, and this was associated with suppression of tremor in the patients. Moreover, alcohol-associated increases of regional cerebral blood flow were observed in the inferior olivary nuclei in the patients but not in the control subjects. In a study of individuals with ET, results of an advanced imaging technique known as positron emission tomography (PET), which examines the biochemistry of the brain, suggested an abnormality in the olivo-cerebellar tracts of the brain. In addition, PET testing in patients with essential tremor reveals increased activity in one brain region known as the cerebellum even while at rest, a finding that is consistent with the cerebellum having an important role in the generation of tremor. Other researchers are investigating the role of stretch loop circuits as well as circuits within the central nervous system that may become unstable and drive muscle contractions (central oscillators), or a combination of both to produce tremor as in ET. A report published in 1997 about the role of clonidine in ET, 26.
(27) lends support the theory of a central oscillating "pacemaker" in ET. In another study with functional magnetic resonance imaging (fMRI) for patients with ET underwent studies of the brain. The results suggested that ET is mainly associated with an additional contralateral cerebellar pathway activation and overactivity in the cerebellum, red nucleus, and globus pallidus without significant intrinsic olivary activation. Focal lesions in the brainstem, cerebellum, and cerebellar projections have also been reported to produce tremor (Figure 2). Secondary tremor similar to ET is most often associated with lesions in the ventrolateral or posterolateral parts of the thalamus and disruption of the cerebellothalamic pathway has been suggested to produce postural and action tremor. Further indirect evidence of cerebellothalamic circuit dysfunction in tremor is derived from the accepted observation that modulation of the VIM thalamic nucleus via thalamotomy or deep brain stimulation (DBS) suppresses tremor by altering the abnormal. 27.
(28) activity of the oversynchronized nuclei. The transmission of oscillatory signals to the limb is believed to occur through the influence of the central oscillator on interconnecting central and peripheral reflex loops. Peripheral loops send alternating impulses to agonistic and antagonistic muscles, resulting in the joint oscillation that characterizes tremor. With current knowledge, it is believed that the primary generator of ET is a central oscillator at the olivo-cerebellothalamo-cortico-spinal circuit, modulated by a peripheral component (14). More controlled studies are required to further investigate the underlying mechanisms of ET. Single-unit electrophysiological recordings in monkeys with harmaline-induced tremor have suggested that the inferior olivary nucleus may play a pivotal role in postural tremor generation, which in turn induces a stream of abnormal neural efferents through the ipsilateral cerebellum, and contralateral red nucleus, thalamus and cerebral motor cortex (15). Ipsilateral cerebellar stroke (16) and contralateral stereotactic lesion of the nucleus ventralis intermedius (Vim) of the thalamus (17) can 28.
(29) abolish ET in humans, further strengthening the notion of a central origin for ET. Cerebral blood flow (CBF) perfusion imaging with radioisotope labeled ligands has been used as a measurement of regional cerebral blood flow (rCBF) in various conditions, including tremors (18). Previous studies with positron emission tomography (PET) have revealed an alternation of the rCBF in ET patients (19). However PET is not feasible for routine clinical use owing to the cost and the lack of availability in most hospitals as compared with SPECT. Recently, technetium 99m ethyl cysteinate dimer (99m Tc ECD) has been developed as a new and reliable marker in quantifying rCBF; without the shortcomings of radiochemical instability and delayed imaging (20, 21). It is intriguing, and mandatory, to investigate whether the alternation of rCBF can be demonstrated by SPECT with this ligand, so as to construct a feasible method for the study of a possible centrally located circuitry of tremor in patients with ET.. 29.
(30) Methods and materials Patients From June 2002 to February 2003, in Changhua county, Taiwan, 25 patients with essential tremor (ET) (mean age, 43 years; range, from 17 to 62 years) were enrolled in this study. All these patients met the published diagnostic criteria for ET (22). None had a history of stroke or signs of dystonia, parkinsonism, or spinocerebellar ataxia on neurological examination. Required criteria for enrolment were (1) postural tremor of moderate amplitude in one or both arms; (2) tremor of moderate amplitude in one or both arms during 4 or more tasks such as: pouring water, using a spoon to eat soup, drinking water, the finger-to-nose maneuver, and drawing a spiral; (3) tremor interferes with one more activities of daily living; (4) medications (lithium, prednisone, levothyroxine, beta-adrenergic bronchodilators, valproate, selective serotonin reuptake inhibitors, and others), caffeine, nicotine, and alcohol are not the cause of the tremor; (5) no other neurologic conditions are the cause of the tremor (23). 30.
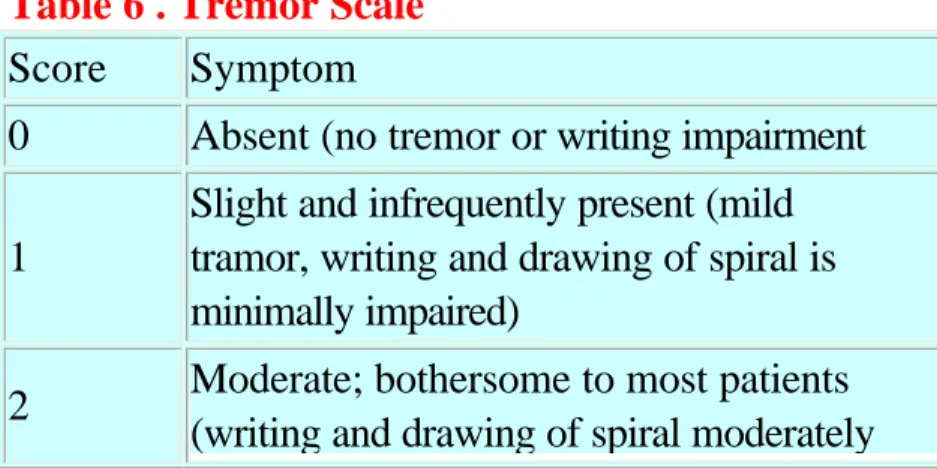
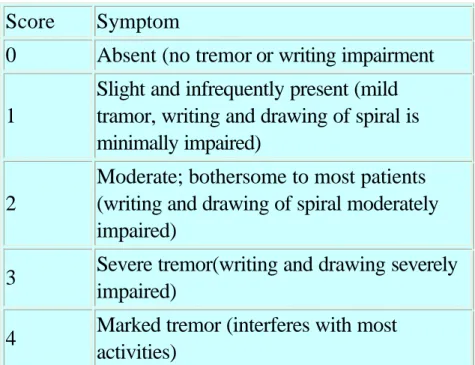
(31) The tremor was rated from 0 to 3 based on the tremor scale (Table 6). For the current analysis, we used the tremor score in the dominant arm (Table 7). All of the 25 patients with ET had normal findings on the brain MRI, and normal thyroid function. Patients with evidence of cerebrovascular disease, other structural brain disease, dementia, head injury, or encephalitis, were excluded. To prevent any potential interaction, the intake of central nervous system stimulants such as amphetamines, anti-anorexia and obesity treatments, sympathomimetics including some nasal decongestants, and antidepressants (amoxapine, buspirone, and benztropine ) were disallowed for 4 weeks prior to entry. Those with standard co-morbid renal, hepatic, and cardiac conditions, and patients with drug or alcohol abuse were excluded. Table 6 . Tremor Scale Score Symptom 0. Absent (no tremor or writing impairment. 1. Slight and infrequently present (mild tramor, writing and drawing of spiral is minimally impaired). 2. Moderate; bothersome to most patients (writing and drawing of spiral moderately 31.
(32) impaired) 3. Severe tremor(writing and drawing severely impaired). 4. Marked tremor (interferes with most activities). 99m Tc ECD SPECT of the brain The 99m Tc ECD was prepared following the instructions on a commercial vial (Neurolite, Dupont Company, USA). The radiochemical purity of the final 99m Tc ECD complex was measured by thin-layer chromatography on Whatman MKC 18 plates developed with acetone and 0.5 M ammonium acetate (60:40). The radiochemical purity was calculated by comparing the peak for the 99m Tc ECD complex with the sum of all other peaks on the plate (24). The radiochemical purities of batches of the 99m Tc ECD were higher than 97%. Brain SPECT with 99m Tc ECD was performed with the patients in a dark and quiet room ( Figure 3). The position of the patient's head was fixed and maintained during SPECT imaging using a hemicylindrical plastic headholder with a radiolucent plastic neck contoured head rest. Fifteen to 45 minutes after intravenous 99m Tc ECD 32.
(33) injection (740 MBq), SPECT data were obtained using a dual headed gamma camera (ADAC, Vertex plus) equipped with fanbeam collimators. Data were collected from 64 projections in the 140 keV photopeak over 360 deg (1800 for each head) in 128x128 matrices, with an acquisition time of 30 s/view. A zoom factor of 1.46 was used. After data acquisition, the data were normalized for the correction of the rotating camera head speed in different directions (upward and downward) and decay of 99m Tc from the first to last frame, so that the number of counts within each frame of the SPECT was the same. Transaxial, coronal, and sagittal slices were reconstructed. Reconstruction of images was performed with attenuation correction using a Butterworth filter at the optimum cut off, and order levels were determined by acquisition counts. For SPECT images, the transaxial sections were reoriented parallel to the base of the brain. This enabled us to obtain coronal and sagittal reconstructions for the determination of the correct anatomical regions of the brain. After image reconstruction, all slices of the SPECT images were normalized to produce the final SPECT 33.
(34) images, the contrast of which was set within the same range of 0-255 gray scales based on the computer screen. Data Analysis Visual Assessment To identify areas of abnormal perfusion, visual interpretation of the SPECT images from each patient was carried out twice in random order with agreement of at least two of three independent experienced observers blind to the clinical information. Normal 99"Tc ECD SPECT findings consisted of homogeneous rCBF in the gray matter of the cortex and basal ganglion without regions of hypoperfusion or visible asymmetry. Abnormal findings included heterogeneous rCBF with regions of hypoperfusion or visible asymmetry on at least two consecutive slices noted twice by at least two of three observers. This meant that at least four of a total of six individual interpretations had to be the same for an agreement.. Semiquantitative Assessments For semiquantitative analysis, the cortical and subcortical 34.
(35) regions of interest (ROIs) in the acquired SPECT data were defined. The relative blood flow ratio in each region was calculated as the average tissue activity in the region divided by the activity in the ipsilateral occipital cortex. Using elliptical templates, ROIs were placed in the frontal, parietal, temporal, occipital, cerebellum, striatum, thalamus, and subcortical white matter regions in each hemisphere (Fig 4). The placement of ROI depended on the visual identification of anatomical regions aided by a stereotaxic atlas. The occipital lobe was used as a reference region (Fig 5, 6). In our preliminary study, data was collected and analyzed in one center, on a standardized form. A correction was made from the occipital cortex readings, because this area receives an equal supply of tracer from the vascular compartment. To determine the activity ratio (brain region/occipital), the counts per ROI of each cortical area were divided by the average counts per ROI found in each occipital hemisphere. This ratio was used as a measure of regional cerebral blood flow (rCBF). All SPECT measurements were performed by a nuclear 35.
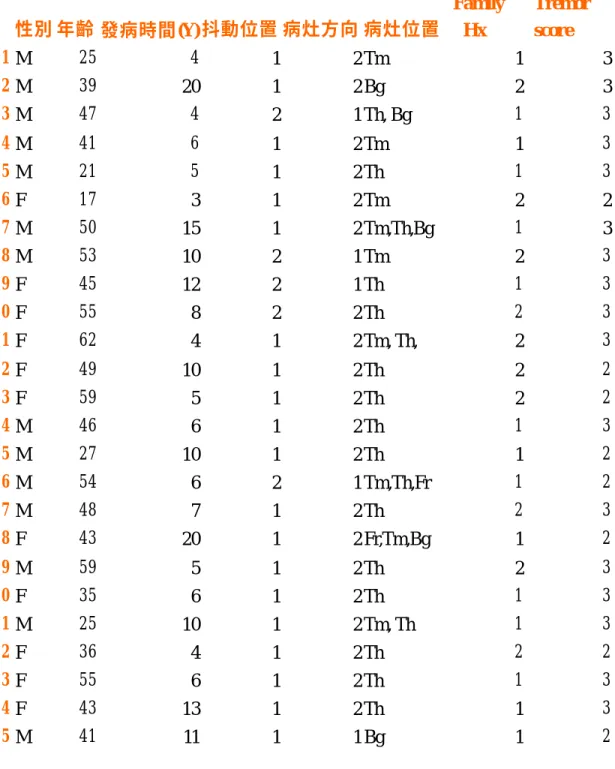
(36) medicine doctor who was blind to the clinical data.. Statistical Analysis The ratios of the rCBF in the ROI in each region of the cortex to that in the occipital cortex are presented as the mean (SD). The Mann-Whitney test was used to compare mean values in each group. The Wilcoxon signed rank sum test was used for comparisons between the right and left rCBF. The Spearman rank correlation coefficient was employed to evaluate correlations between tremor score and age, sex and duration of illness. The significance level was set at P = 0.05. Data were analyzed using SPSS 9.0 J for Windows (SPSS, Chicago, IL, USA).. n Results The duration of the tremor history of the 25 patients with essential tremor was from 3 to 20 years (mean: 8.4 years). Fifteen patients had a positive family history of essential tremor. The tremor score of all the patients ranged from grade 2 to 3. 36.
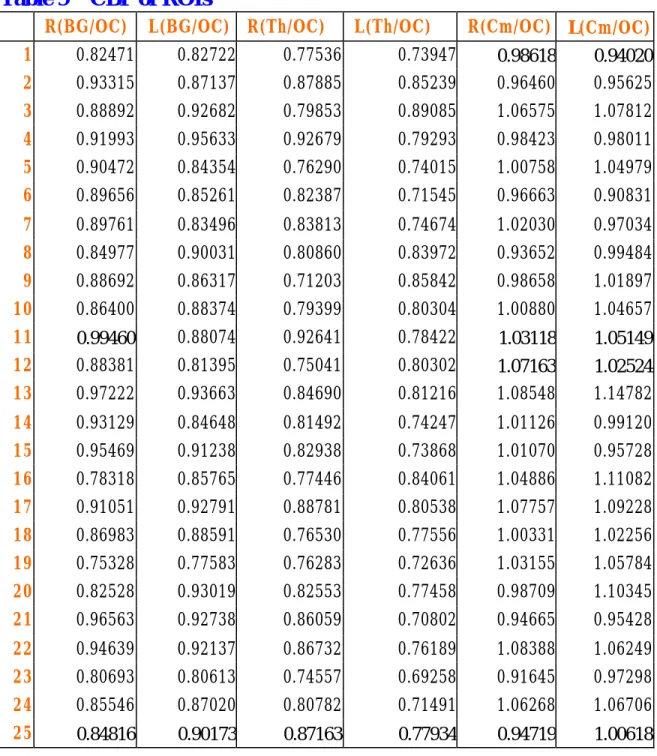
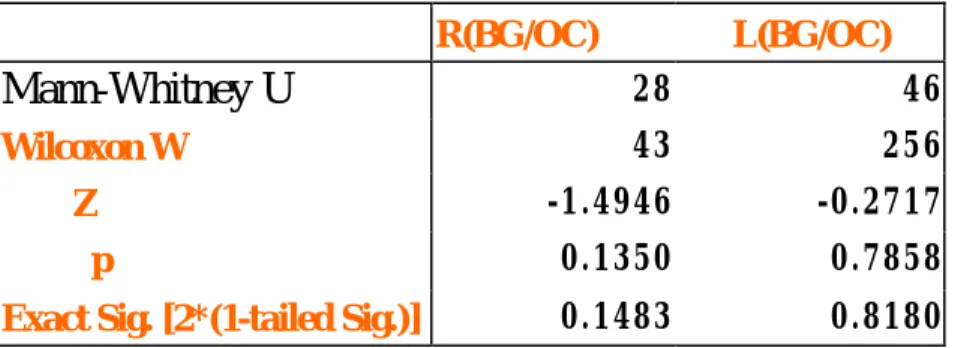
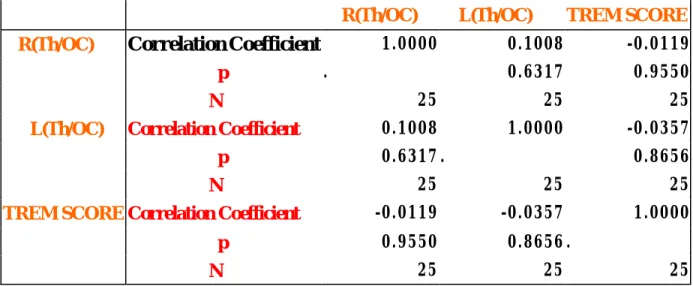
(37) Tables 8 shows the detailed data for the patients. (Table 8) The 99m Tc ECD brain SPECT of these 25 patients showed regions of hypoperfusion in many regions of the brain, including the basal ganglia, thalamus, frontal lobe, and temporal lobe (Figure 4). The calculated rCBF values of the thalamus, basal ganglia, and cerebellum relative to the occipital lobe are shown in Table 9. (Table 9) The thalamus region was the area with the most hypoperfusion in 20 patients, and had a positive statistical significance relative to the contralateral tremor side (P = 0.002797 for the left thalamus; P = 0.0297 for the right thalamus) (Table 10), but no such correlation was found in the basal ganglia and cerebellum(Table 11,12). Significant hypoperfusion of the rCBF was revealed in the thalamus region, corresponding to the contralateral side of the tremor limb. There was no significant relationship between the tremor score and the rCBF of other regions. We found no positive correlation between the rCBF ratios in the thalamus and the tremor score (Table 13). There was no difference in rCBF ratios between patients with or without a family history, patients’age and duration of tremor 37.
(38) (Table 14, 15, 16).. n Discussion Although the pathogenesis of ET remains unclear, several studies have suggested that the olivo-cerebello-thalamo-cortical circuitry plays a pivotal role in its generation (25). This assumption has been strengthened by PET and functional magnetic resonance imaging (fMRI) studies, in which increased blood flow and neural activities have been detected in the cerebellum, as well as basal ganglia (9, 26). In this current 99mTc ECD SPECT study, it was intriguing to find that the rCBF was significantly decreased in the thalamic region contralateral to the more vigorous tremor limb. No significant alternation of the blood perfusion was detected in the hot spots as suggested by the PET or fMRI studies. Before jumping to conclusions, it must be said that, in the current study, the patients were examined in a resting state instead of holding their hand in the air for tremor triggering, as in previous studies. Thus the current study may reflect the static (tremor-free) condition 38.
(39) rather than the dynamic (tremorous) condition of the brain. Since there was no normal control in this study, one can not help but wonder whether this unique SPECT phenomenon could also appear in normal humans. However, this is unlikely, based on our limited experience with 99mTc ECD SPECT findings (unpublished observation) in subjects with diseases other than tremor, in whom no such asymmetric pattern has ever been observed. In addition, the possibility that the hypoperfusion seen with the SPECT was caused by an organic lesion of the brain was also excluded by the normal MRI findings of these ET patients, If the current SPECT result actually reflects the stationary functional alternation of the thalamic region of the ET patients, is there a physiological assumption to explain the finding? Recently, deep brain stimulation (DBS) has been adopted to treat intractable ET by targeting the electrodes in the ventral intermediate (Vim) nucleus of the thalamus. This technique may benefit patients via such mechanisms as “ conduction blocking” (27), preferential activation of inhibitory axon terminals (28) and overriding 39.
(40) rhythmic firing frequencies over irregular firing patterns (29). Also, Perlmutter has demonstrated the increased blood flow at the terminal fields of the thalamocortical projections after DBS of the Vim of thalamus by PET. It has been suggested that the net effect of DBS is to drive the efferent neurons of the thalamus (30). In keeping with the DBS-PET findings, the current finding suggests that the thalamus plays a pivotal role in ET generation or modulation. In addition to the thalamus, the inferior olivary nucleus has also been speculated to play a crucial role in the generation of ET. This working hypothesis was deduced from the observation that in some of the ET patients, the tremor could be suppressed by alcohol consumption. The beneficial effect of alcohol was probably mediated through a reduction in cerebellar overactivity, which culminated in an increased afferent input to the inferior olivary nuclei. This functional alternation has been illustrated in a rCBF study with PET, in which the rCBF was found to be increased in the inferior olivary nuclei after oral alcohol administration in ET patients, but not in the controls (31). Because of the limitation of the SPECT, we were unable to 40.
(41) examine the olivary region in the current study. However, based on the finding gathered in the current study and in the previous reports of PET gathered, the olivo-cerebello-thalamic circuitry might be crucial for the generation of ET. Technetium-99m-ethyl cysteinate dimer (ECD) is a relatively new 99m Tc-labeled lipophilic tracer that became available clinically for SPECT imaging studies of the cerebral area in the most recent decade (32). It has been adopted for the evaluation of several neurological conditions including cerebrovascular disease (33), dementia (34) and epilepsy (35). In all brain regions, 99mTc ECD SPECT showed a higher lesion contrast than that of 99mTc HMPAO SPECT. Thus it is generally agreed that 99mTc ECD is superior to 99mTc HMPAO in detecting brain lesions or functional alternations (36, 37). In addition, 99m Tc ECD does not have the problems of radiochemical instability and delayed imaging (38). With these benefits and the consistent findings gathered in the current study, we recommend ECD SPECT as an appropriate tool for the investigation of ET, apart. 41.
(42) from being applied in the assessment of the aforementioned neurological diseases. There is some variability of regional ECD brain perfusion patterns by 99mECD SPECT scan. It depends on patient’s age, gender, and hemisphere. On average, there was 1.4% higher in the right hemisphere for the whole study group. Global cerebral perfusion decreases with age. The age-related decline in hemispheric blood flow in agreement with the finding of a 3.7% decline per decade in healthy subjects. It was mostly found in the anterior cingulate gyrus, bilateral basal ganglia, left prefrontal, left lateral frontal and left superior temporal and insular cortex (all P=0.001-0.02). There was an overall increase in right/left asymmetry with age, which was most pronounced in the frontal and temporal neocortex. Men had a significantly higher tracer uptake in the cerebellar hemispheres, left anterior temporal cortex and orbitofrontal cortex; otherwise women showed a higher tracer uptake bilaterally in the inferior parietal cortex in women. Average intersubject variability was 4.8% while intrasubject reproducibility was 3.0%. However, 42.
(43) hemispheric asymmetry and intersubject variability of ECD perfusion pattern are relatively small in adults. In addition to the examination of the correlation between the diminution of thalamic rCBF and the tremor severity, the presence of tremor family history and the disease duration were also assessed to determine their impact on the alternation of the rCBF and the results were unremarkable. In conclusion, the current study illustrated the alternation of rCBF in the thalamus region of ET patients and suggests that 99mTc ECD SPECT is a promising tool for the investigation of tremor.. n Future Planning 1. Normal population rCBF: We need to set up the normal data of our laboratory in order to obtain the rCBF ratio data statistically. 2. Collect more ET patients database: To prevent the obtained data not significant statistically, we hope to collect more patients with signs of essential tremor. 43.
(44) 3. More information of rCBF about the subnucleus of thalamus: Inferior olivary nucleus has been thought to be a pivotal role in generating the tremor. Other structures might have the same function as inferior olivary nucleus. We need more upgrade SPECT machines to get the better images of subnucleus. 4. Gene analysis: As mentioned in the introduction of this paper, gene may play a role in ET, and we want to offer the original data of gene sequences of Taiwanese. 5. EMG Study: Electromyogram has been a specific tool to evaluate the nature of ET. We wish to put the SPECT image findings in comparison with the EMG data, for the unresolving problems of ET. 6. Medication: SPECT scan may be a well tool to investigate the mechanisms of drugs that could alleviate the intensity of tremor. It could afford the objective images and data for the effective medications. 44.
(45) References 1. Deuschl G, Bain P, Brin M, Ad Hoc Scientific Committee. Consensus statement of Movement Disorder Society on tremor. Mov Disord 1998;13(suppl 3):2-23. 2.Charles PD, Esper GJ, Davis TL. Classification of tremor and update on treatment. Am Fam Physician 1999;59(6):1565-72. 3. Findley LJ, Koller WC. Essential tremor: a review. Neurology. 1987; 37:1194-1197. 4. Rautakorpi I, Marttila RJ, Rinne UK. Epidemiology of essential tremor. In: Findley LJ, Capildeo R, eds. Movement Disorders: Tremor. New York, NY: Macmillan Publishing Co Inc; 1984:211-218. 5. Findley LJ, Koller WC. Essential tremor: a review. Neurology. 1987; 37:1194-1197. 6. Deutschl G, Elble RJ. The pathophysiology of essential tremor. Neurology 2000;54(Suppl. 4):S14– 20. 7. Tapiador MJ, Perez-Lopez-Fraile I, Lopez-Lopez A. Essential tremor: a review of pathogenic mechanisms. Rev Neurol Dec 1998;27(160):1059– 65. 8. Poirier LJ, Sourkes TL, Bouvier G, et al. Striatal amines, experimental tremor and the effect of harmaline in the monkey. Brain 1996;89:37-52. 9. Dupuis MJ, Delwaide PJ, Boucquey D, Gonsette RE. Homolateral disappearance of essential tremor after cerebellar stroke. Mov Disord 1989;4(2):183-7. 10. Mobin F, De Salles AA, Behnke EJ, Frysinger R. Correlation between MRI-based stereotactic thalamic deep brain stimulation electrode placement, macroelectrode stimulation and clinical response to tremor control. Stereotact Funct Neurosurg 1999;72(2-4):225-32. 11. Christiaan Schiepers;Alfons Verbruggen;Paul Casaer;Michel De Roo. Normal brain perfusion pattern of Technetium-99m-Ethylcysteinate dimer in children. J Nucl Med; New York; Jul 1997. 12. Higgins JJ, Loveless JM, Jankovic J, et al. Evidence that a gene for essential tremor maps to chromosome 2p in four families. Mov 45.
(46) Disord 1998;13(6):972-7. 13. Deuschl G, Bain P, Brin M, and an Ad Hoc Scientific Committee. Consensus statement of the Movement Disorder Society on Tremor. Mov Disord 1998;13(Suppl 3):2-23. 14. Kao CH, Lan JL, ChangLai SP, Chieng PU. Technetium-99m-HMPAO brain SPECT in Sjogren's syndrome. J Nucl Med 1998;39:773-7. 15. Juni JE, Waxman AD, Devous MD. Procedure guideline for brain perfusion SPECT using technetium-99m radiopharmaceuticals. J Nucl Med 1998;39:923-6. 16. Leveille J, Demonceau G, De Roo M. Characterization of Tc-99m-L,L-ECD for brain perfusion. Part 2. Biodistribution and brain imaging in humans. J Nucl Med 1989;30:1902-10. 17. Bain P, Brin M, Deuschl G, Elble R, Jankovic J, Findley L, Koller WC, Pahwa R. Criteria for the diagnosis of essential tremor. Neurology 2000;54(11 Suppl 4):S7. 18. Louis ED, Ford B, Lee H, et al. Diagnostic criteria for essential tremor: a population perspective. Arch Neurol 1998;55(6):823-8 19. Leveille J, Demonceau G, De Roo M, et of. Characterization of Tc-99m-L,L-ECD for brain perfusion. Part 2. Biodistribution and brain imaging in humans. J Nucl Med 1989;30:1902-10. 20. Stein RB, Lee RG, Nichols TR. Modifications of ongoing tremors and locomotion by sensory feedback. Electroencephalogr Clin Neurophysiol Suppl 1978;(34):512-19. 21. Activation mapping in essential tremor with functional magnetic resonance imaging. Bucher SF, Seelos KC, Dodel RC, Reiser M, Oertel WH. Ann Neurol 1997 Jan. 22. Gross C, Rougier A, Guehl D, Boraud T, Julien J, Bioulac B. High-frequency stimulation of the globus pallidus internalis in Parkinson’s disease: a study of seven cases. J Neurosurg 1997; 87: 491–498. 23. Wu YR, Levy R, Ashby P, Tasker RR, Dostrovsky JO. Does stimulation of the GPi control dyskinesia by activating inhibitory axons? Mov Disord 2001; 16: 208–216. 24. Windels F, Bruet N, Poupard A, et al. Effects of high frequency stimulation of subthalamic nucleus on extracellular glutamate and 46.
(47) GABA in substantia nigra and globus pallidus in the normal rat. Eur J Neurosci 2000; 12: 4141–4146. 25. Perlmutter JS, Mink JW, Bastian AJ, Zackowski K, Hershey T, Miyawaki E, Koller W, Videen TO. Blood flow responses to deep brain stimulation of thalamus. Neurology 2002 May 14;58(9):1388-94. 26. Boecker H, Wills AJ, Ceballos-Baumann A. The effect of ethanol on alcohol-responsive essential Tremor: a positron emission tomography study. Ann Neurol 1996 May. 27. Vallabhajosula S, Zimmerman RE, Picard M, et al. Technetium-99m-ECD: a new brain imaging agent: in vivo kinetics and biodistribution studies in normal human subjects. J Nucl Med 1989; 30:599-604. 28. Brass LM, Walovitch RC, Joseph JL, et al. The role of single photon emission computed tomography brain imaging with 99m Tc-bicisate in the localization and definition of mechanism of ischemic stroke. J Cereb Blood Flow Metab 1994;14(suppl 1):S91-S98. 29. Waldemar G, Walovitch RC, Andersen AR, et al. Technetium-99m-bicisate (Neurolite) SPECT brain imaging and cognitive impairment in dementia of the Alzheimer type: a blinded read of image sets from a multicenter SPECT trial. J Cereb Blood Flow Metab 1994; 14(suppl 1):S99-S105. 30. Grunwald F, Menzel C, Pavics L, et al. Ictal and interictal brain SPECTimaging in epilepsy using technetium-99m-ECD. J Nucl Med 1994; 35:1896-1901. 31. Matsuda H, Li YM, Higashi S, Sumiya H, Tsuji S, Kinuya K, et al. Comparative SPECT study of stroke using Tc-99m ECD, I-123 IMP, and Tc-99m HMPAO. Clin Nucl Med 1993;18:754-8. 32. van Dyck CH, Lin CH, Smith EO, et al. Comparison of technetium-99m-HMPAO and technetium-99m-ECD cerebral SPECT images in Alzheimer's disease. J Nucl Med 1996;37:1749-55. 33. C P Chang;Y C Shiau;J J Wang;S T Ho;A Kao. Abnormal regional cerebral blood flow on (99m) Tc-ECD brain SPECTin patients with primary Sjogren's and normal findings on brain magnetic resonance imaging. Annals of the Rheumatic Diseases. 2002;Sep.61(9):774-8. 47.
(48) Appendix A Table 1 Table 1. Circumstances that activate various types of tremor Circumstance. Tremor type. Resting. Parkinsonian Rubral*. Posture. Dystonic* Enhanced physiologic Essential Orthostatic Psychogenic Rubral*. Kinesis. Cerebellar Dystonic** Rubral**. Table 2. Differential Diagnosis of Tremor. 1. Neurological diseases Cerebellar tremor Dystonia and dystonic tremors Enhanced physiologic tremor Isolated chin tremor Isolated voice tremor Orthostatic tremor Palatal tremor Rubral tremor Writer's tremor and other task-specific tremors Parkinson’s disease (PD) 48.
(49) Pallidonigral degeneration Multiple system atrophy (MSA) Olivopontocerebellar atrophy (OPCA) Striatonigral degeneration Progressive pallidal atrophy Huntington’s disease (HD) Benign hereditary chorea Fahr’s disease Paroxysmal dystonic choreoathetosis (PDC) Ataxia-telangiectasia (AT) Familial intention tremor and lipofuscinosis Ramsay-Hunt syndrome (progressive myoclonic ataxia) Dystonia musculorum deformans DOPA-responsive dystonia Cervical dystonia (spasmodic torticollis) Meige syndrome Task-specific tremors (writer’s or voice tremor) Space-occupying lesions of the brain Peripheral neuropathies (e.g., Charcot-Marie-Tooth, Guillain-Barré, etc.). 2. Drug-induced tremors Antidepressants, especially tricyclics Beta-agonists Depakote Dopamine Lithium Metoclopramide Neuroleptics Theophylline Thyroid hormones Withdrawal of drugs. 3. Metabolic B-12 deficiency Hyperthyroidism Hyperparathyroidism Hypocalcemia 49.
(50) Hyponatremia Kidney disease Liver disease. 4. Toxic Alcohol Arsenic Caffeine DDT Lead Nicotine Toluene Withdrawal of alcohol, cocaine. 5. Psychogenic tremor. Table 3 Drugs that may induce tremor.. 50.
(51) Table 4. Classic distinguishing festures of PD and ET.. Table 5. Guidelines for identifying essential tremor Table 5: Guidelines for identifying essential tremor. Core criteria 4. Bilateral action tremor of the hands and forearms (but not rest tremor) 5. Absence of other neurologic signs, except for cogwheel phenomenon (palpable tremor during manipulation of the patient's limbs) 6. May have isolated head tremor with no abnormal posture Secondary criteria 5. Long duration ( 3 years) 6. Family history 7. Beneficial response to ethanol. 51.
(52) Table 6 . Tremor Scale Score. Symptom. 0. Absent (no tremor or writing impairment. 1. Slight and infrequently present (mild tramor, writing and drawing of spiral is minimally impaired). 2. Moderate; bothersome to most patients (writing and drawing of spiral moderately impaired). 3. Severe tremor(writing and drawing severely impaired). 4. Marked tremor (interferes with most activities). Table 7. 52.
(53) Table 8. Basic Data of 25 Patients. Family Tremor 性別 年齡 發病時間(Y) 抖動位置 病灶方向 病灶位置 Hx score 1M 25 4 1 2 Tm 1 3 2M 39 20 1 2 Bg 2 3 3M 47 4 1 3 2 1 Th, Bg 4M. 41. 6. 1. 2 Tm. 5M. 21. 5. 1. 2 Th. 6F. 17. 3. 1. 2 Tm. 7M. 50. 15. 1. 2 Tm,Th,Bg. 8M. 53. 10. 2. 1 Tm. 9F. 45. 12. 2. 1 Th. 2 1. 10 F. 55. 8. 2. 2 Th. 2. 3. 11 F. 62. 4. 1. 2 Tm, Th,. 2. 3. 12 F. 49. 10. 1. 2 Th. 2. 2. 13 F. 59. 5. 1. 2 Th. 2. 14 M. 46. 6. 1. 2 Th. 2 1. 15 M. 27. 10. 1. 2 Th. 2. 16 M. 54. 6. 2. 1 Tm,Th,Fr. 1 1. 17 M. 48. 7. 1. 2 Th. 2. 3. 18 F. 43. 20. 1. 2 Fr,Tm,Bg. 1. 2. 19 M. 59. 5. 1. 2 Th. 3. 20 F. 35. 6. 1. 2 Th. 2 1. 21 M. 25. 10. 1. 2 Tm, Th. 1. 3. 22 F. 36. 4. 1. 2 Th. 2. 2. 23 F. 55. 6. 1. 2 Th. 1. 3. 24 F. 43. 13. 1. 2 Th. 1. 3. 25 M. 41. 11. 1. 1 Bg. 1. 2. 53. 1 1. 3. 2 1. 2. 3 3 3 3. 3 2. 3.
(54) Table 9. CBF of ROIs. R(BG/OC). L(BG/OC) R(Th/OC). L(Th/OC). 1. 0.82471. 0.82722. 0.77536. 0.73947. 2. 0.93315. 0.87137. 0.87885. 3. 0.88892. 0.92682. 4. 0.91993. 5. R(Cm/OC) L(Cm/OC). 0.85239. 0.98618 0.96460. 0.94020 0.95625. 0.79853. 0.89085. 1.06575. 1.07812. 0.95633. 0.92679. 0.79293. 0.98423. 0.98011. 0.90472. 0.84354. 0.76290. 0.74015. 1.00758. 1.04979. 6. 0.89656. 0.85261. 0.82387. 0.71545. 0.96663. 0.90831. 7. 0.89761. 0.83496. 0.83813. 0.74674. 1.02030. 0.97034. 8. 0.84977. 0.90031. 0.80860. 0.83972. 0.93652. 0.99484. 9. 0.88692. 0.86317. 0.71203. 0.85842. 0.98658. 1.01897. 10. 0.86400. 0.88374. 0.79399. 0.80304. 1.00880. 1.04657. 11. 0.88074. 0.92641. 0.78422. 1.03118. 1.05149. 12. 0.99460 0.88381. 0.81395. 0.75041. 0.80302. 13. 0.97222. 0.93663. 0.84690. 0.81216. 1.07163 1.08548. 1.02524 1.14782. 14. 0.93129. 0.84648. 0.81492. 0.74247. 1.01126. 0.99120. 15. 0.95469. 0.91238. 0.82938. 0.73868. 1.01070. 0.95728. 16. 0.78318. 0.85765. 0.77446. 0.84061. 1.04886. 1.11082. 17. 0.91051. 0.92791. 0.88781. 0.80538. 1.07757. 1.09228. 18. 0.86983. 0.88591. 0.76530. 0.77556. 1.00331. 1.02256. 19. 0.75328. 0.77583. 0.76283. 0.72636. 1.03155. 1.05784. 20. 0.82528. 0.93019. 0.82553. 0.77458. 0.98709. 1.10345. 21. 0.96563. 0.92738. 0.86059. 0.70802. 0.94665. 0.95428. 22. 0.94639. 0.92137. 0.86732. 0.76189. 1.08388. 1.06249. 23. 0.80693. 0.80613. 0.74557. 0.69258. 0.91645. 0.97298. 24. 0.85546. 0.87020. 0.80782. 0.71491. 1.06268. 1.06706. 25. 0.84816. 0.90173. 0.87163. 0.77934. 0.94719. 1.00618. 54.
(55) Table 10 CBF -Thalamus and Lesion side R(Th/OC). L(Th/OC). Mann-Whitney U. 18. 6. Wilcoxon W. 33. 216. r. -2.1740. -2.9892. p. 0.0297. 0.0028. R: right; L: left; OC: occipital; Th: thalamus;. Table 11. Basal ganglia CBF and lesion. side R(BG/OC). L(BG/OC). Mann-Whitney U. 28. 46. Wilcoxon W. 43. 256. -1.4946. -0.2717. 0.1350. 0.7858. 0.1483. 0.8180. Z p Exact Sig. [2*(1-tailed Sig.)]. R: right; L: left; BG: basal ganglia; OC: occipital;. Table 12. Cerebellum CBF and lesion side R(Cm/OC). L(Cm/OC). Mann-Whitney U. 49. 33. Wilcoxon W. 64. 243. Z. -0.0679. -1.1549. p. 0.9458. 0.2481. 0.9738. 0.2718. Exact Sig. [2*(1-tailed Sig.)]. R: right; L: left; OC: occipital; Cm: cerebellum. 55.
(56) Table 13. Tremor score and CBF (Th) R(Th/OC). R(Th/OC). 1.0000. Correlation Coefficient N Correlation Coefficient. -0.0119. 0.6317. 0.9550. 25. 25. 25. 0.1008. 1.0000. -0.0357. 0.6317 .. p N TREM SCORE Correlation Coefficient. 25. 25. -0.0119. -0.0357. 1.0000. 0.8656 .. 25. N. 25. R: right; L: left; OC: occipital; Th: thalamus;. Family Hx and CBF. R(Th/OC). L(Th/OC). 41. 43. 231. 64. Z. -1.0181. -0.8908. p. 0.3087. 0.3730. Exact Sig. [2*(1-tailed Sig.)]. 0.3333. 0.4004. Mann-Whitney U Wilcoxon W. R: right; L: left; OC: occipital; Th: thalamus;. 56. 0.8656. 25 0.9550. p. Table 14. TREM SCORE. 0.1008. .. p L(Th/OC). L(Th/OC). 25.
(57) Table 15. Patient’s age and CBF. R(Th/OC). Correlation R(Th/OC) Coefficient. 0.1008. -0.1513. 年齡. 1.0000. 0.6317. 0.4703. 25. 25. 25. Correlation Coefficient. 0.1008. 1.0000. 0.3500. p N. 0.6317 .. .. p N L(Th/OC). 年齡. L(Th/OC). Correlation Coefficient p N. 0.0864. 25. 25. 25. -0.1513. 0.3500. 1.0000. 0.4703. 0.0864 .. 25. 25. 25. R: right; L: left; OC: occipital; Th: thalamus;. Table 16 發病時間 and CBF 發病時間 發病時間. Correlation Coefficient p. 1.0000. R(Th/OC). Correlation Coefficient. 0.2002. 0.9382. 0.3372. 25. 25. 25. 0.0163. 1.0000. 0.1008. 0.9382 .. p. 0.6317. 25. 25. 25. 0.2002. 0.1008. 1.0000. p. 0.3372. 0.6317 .. N. 25. N L(Th/OC). 0.0163. .. N. R(Th/OC) L(Th/OC). Correlation Coefficient. R: right; L: left; OC: occipital; Th: thalamus;. 57. 25. 25.
(58) Appendix B Figure 1. The prevalence of ET increasing with age.. Figure 2. Hand-writing of essential tremor patients. Figure 3. 58.
(59) Figure 4. Figure 5. 59.
(60) Figure 6. 60.
(61) 張振書 52 年 8 月 25 日出生 台灣省台中縣 中國醫藥學院醫學系畢業。 彰化基督教醫院 神經內科主治醫師。 中華民國神經內科專科醫師。 中華民國內科專科醫師。 中華民國重症醫學會專科醫師。 中華民國超音波學會會員。. 61.
(62)
數據
+7
相關文件
The isolated case showed typical features, including fibrocystic breast disease, benign thyroid nodules, and multiple papillomatous lesions in the face and oral cavity, and the
中興國中
中興國中
中興國中
Textbook Chapter 4.3 – The substitution method for solving recurrences Textbook Chapter 4.4 – The recursion-tree method for solving recurrences Textbook Chapter 4.5 – The master
Textbook Chapter 33.4 – Finding the closest pair of points.. Closest Pair of
Textbook Chapter 4.3 – The substitution method for solving recurrences Textbook Chapter 4.4 – The recursion-tree method for solving recurrences Textbook Chapter 4.5 – The master
Calculate the amortized cost of each operation based on the potential function 4. Calculate total amortized cost based on
