Original Article
Development and evaluation of an E-health system to care for patients
with bladder pain syndrome/interstitial cystitis
Ming-Huei Lee,1,3 Huei-Ching Wu,2,3 Jen-Yung Lin,4 Tan-Hsu Tan,5 Po-Chou Chan1 and Yung-Fu Chen2,6
Departments of 1Management Information System and 2Healthcare Administration, Central Taiwan University of Science and Technology, 3Department of Urology, Feng Yuan Hospital, Ministry of Health and Welfare, Taichung, 4Department of Computer Science and Information Engineering, Da-Yeh University, Changhua, 5Department of Electrical Engineering, National Taipei University of Technology, Taipei, and 6Department of Health Services Administration, China Medical University, Taichung, Taiwan
Correspondence: Yung-Fu Chen Ph.D., Department of Healthcare Administration, Central Taiwan University of Science and
Technology, Taichung 666 Buzih Road, Beitun District, Taichung 40601, Taiwan. Email: [email protected]
Objectives: Bladder pain syndrome/interstitial cystitis (BPS/IC) is a chronic disease that highly degrades the quality of life
for patients. In the present study, Internet intervention was used to care for bladder pain syndrome/interstitial cystitis patients to alleviate their pain and bothering symptoms.
Methods: Healthcare education was carried out through the Internet by asking the patients, who were randomly divided into
study (40 patients) and control (40 patients) groups, to check possible sensitive foods, habits, and behaviors weekly to remind and consolidate important rules for promoting quality of life. The symptom flares consultation through short message service with the Internet used to elevate healthcare efficiency was undertaken. Questionnaires, including Short Form 36 health survey, O’Leary–Sant symptom and problem indices, as well as visual analog scales pain and urgency scales, were used to evaluate quality of life and disease severity improvements before and after information and communication technology intervention. The outcome was evaluated at week 8.
Results: The quality of life of both the control and study groups was significantly improved. The quality of life and visual
analog scales for the patients in the study group with information and communication technology intervention showed a much greater improvement compared with the patients in the control group (P < 0.05).
Conclusions: The E-health system was shown to be effective in improving quality of life of bladder pain
syndrome/interstitial cystitis patients through intervention of Internet healthcare education and short message service for the consolidation of healthy behavior and lifestyle in the 8-week follow up.
Key words:
Key words: bladder pain syndrome, E-health education, information and communication technology, interstitial cystitis, quality of life.
Abbreviations & Acronyms
Abbreviations & Acronyms
BPS/IC = bladder pain syndrome/interstitial cystitis ICT = information and communication technology LUTS = lower urinary tract symptoms
QOL = quality of life SF-36 = Short Form 36 SMS = short message service VAS = visual analog scales
Introduction
Bladder pain syndrome/interstitial cystitis (BPS/IC) is a poorly defined chronic bladder disease characterized by pelvic pain and urinary storage symptoms (e.g. urinary urgency and frequency) in the absence of proven urinary infection or other definable pathological etiology.1 Several societies, such as the National Institute Digestive, Diabetes, Kidney,
American Urological Association, International Continence Society and Asian IC/BPS group have their definition for the diagnosis and treatment of BPS/IC.2–4 The etiologies of the disease are multifocal, whether it has originated from the
bladder or other pelvic organs, or is a systematic disease is still not elucidated.5
The BPS/IC treatments are very diverse; currently, there is no single therapy that has been found to be effective for the majority of patients.1 Clinically, the patients have been bothered by the disease for a long time, making them feel
frustrated when receiving further therapies, such as medication prescriptions. Recently, it was reported that environmental factors, such as dietary, physical activity, smoking and drinking behaviors, attributed substantially to the occurrence of BPS/IC based on the twin studies.6,7 When the symptoms flare up, most of the patients cannot follow the
regiments of self-management, and they usually seek help by visiting the emergency department without receiving effective treatment, resulting in a waste of medical resources, deficiency of effective healthcare and degradation of quality of life.
It was shown that intervention by sending simple messages through cellular telephones and the Internet can significantly decrease blood pressure, as well as effectively reduce bodyweight and waist circumference. A similar intervention was also shown to be effective in decreasing blood glucose levels of obese type 2 diabetes patients.8
SMS is a simple, low-cost, but effective method of health promotion. It has been used to promote safer sex and sun safety.9
To the best of our knowledge, the E-health system has never been applied to care for patients with BPS/IC before. The motivations of the present study are summarized as follows: it is currently impossible to completely cure BPS/IC disease because of unclear pathogenesis, with the goal of treatment being mainly to alleviate symptoms or to improve the quality of life for the patients; although BPS/IC is not a malignant disease, treatment of BPS/IC patients needs a lot of healthcare resources and might cause a great burden for the country as a result of its chronicity; and intervention using mobile telephone and the Internet is effective in caring for patients with chronic diseases in outpatient settings. Hence, the objectives of the present study were to develop an E-health system by integrating mobile telephone and the Internet to alleviate the pain and symptoms of the BPS/IC patients through weekly health education and symptom flares consultation by a question/answer template service. In addition, behavior can be modified and reinforced through the Internet by asking the patients to check their daily foods, activities and living habits on a weekly basis, which in turn promotes their quality of life.
Methods
Preparation of health educational materials
In the present study, a web service was designed to promote healthy diets and lifestyles for the patients by asking them to check and follow the diets and lifestyles suggested by the physician. It also provided the patients with questionnaires to assess their perceived symptoms and quality of life before and after the experiment. The web service was installed in the web server to respond to or communicate with the mobile telephone by sending/receiving short messages through the Hinet message center. It can be accessed by the patients after they login to the website of Taiwan Interstitial Cystitis Association (TICA; http://taic.hopto.org) through an Internet browser. As shown in Appendix I, the design of the educational materials was based on the following findings:
Items 1, 3–4: The BPS/IC patients are generally sensitive to foods containing vitamin C, potassium, or spices, as well
as beverages containing caffeine or alcohol.10
Item 2: To reduce the recurrence of BPS/IC symptoms, the patients are encouraged to drink 1500 cm3 water daily
(ICA; http://www.ichelp.org/Page.aspx?pid=429).
Item 5: Smoking is associated with a higher risk of BPS/IC.11
Items 6–7: Certain types of exercise, such as pelvic floor muscle exercise, and wearing of tight-fitting clothes might
worsen BPS/IC symptoms in some patients.1 Yoga can be carried out as a complementary and alternative therapy for
patients with anxiety.12
Items 8, 13: The patients are encouraged to have bathed their whole lower abdomen with warm water (40°C) more than
once a day, each time lasting for 15 min. A heat pad can also be placed over the abdomen to relieve uncomfortable symptoms (ICA; http://www.ichelp.org/Page.aspx?pid=429).
Item 9: More than 80% of premenopausal IC women have symptoms flare up before, within, and after the menstrual
cycle, and 35% of IC women choose heating bag to relieve pain. 13
Items 10–12: Treatment and care of the vagina and genital area might affect sexual and reproductive morbidities for
women.14
Item 13: Guided imagery or meditation was shown to be effective in pain and symptom management for BPS/IC
patients. .15
The money to establish the system was approximately $10 000 for 40 patients in our study (including software design fee, mobile telephone fees and fees for SMS).
Management of symptom flares
An SMS application was designed to provide a Q/A service to handle the cases of symptom flares for BPS/IC patients. When an emergent symptom occurred, the patient was encouraged to send a message by typing the event number (Appendix II) to the SMS server through a designated mobile telephone number. The template containing the questions (symptoms) and their corresponding answers was stored in the mobile telephone. The SMS server responded to the question by sending its corresponding answer to guide the patient on how to relieve the symptom immediately.
Participants and protocol
A total of 80 BPS/IC patients were recruited from the urological clinic of Taichung Hospital, Taichung, Taiwan and randomly assigned to either the study group (n = 40) or the control group (n = 40). Among them, seven patients in the
study group and eight in the control group were excluded because of failure to fill the questionnaires in either the pre- or post-test. Hence, only the data of 65 patients, 33 in the study group and 32 in the control group, were used for further analysis. In addition to their regular treatments, patients in the study group were asked to self-manage their diets and lifestyles by responding to health education questions weekly in order to check their compliance in following the suggestions of the provided educational materials. Participants who forgot to fill in the form were notified by email or SMS. This intervention was intended to be used for changing and consolidating their habitual behaviors. In contrast, treatment was only given to the patients in the control group. The study was approved by the institution review board.
Experimental paradigm
In the present study, ICT was used as the intervention method to improve healthcare quality of BPS/IC patients. The demographic information, anesthetic bladder volume, and questionnaires including SF-36 health survey, O’Leary–Sant symptom and problem indices and VAS for the measurement of pain and urgency were given to measure the patient perception of health status before (pre-test) and after (post-test) ICT intervention spanning a period of 8 weeks.
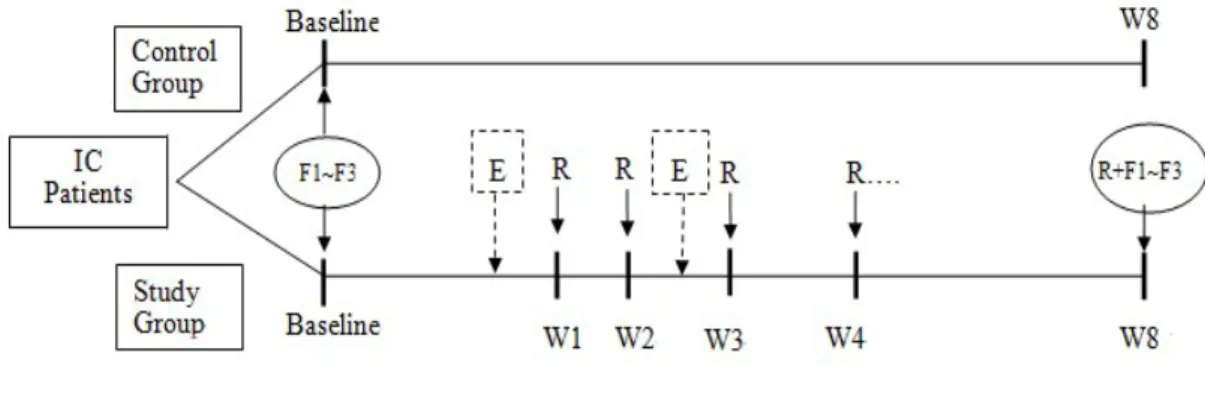
Figure 1 shows the experimental procedure. ICT intervention provided weekly health education for consolidating healthy dieting habit and lifestyle. O’Leary–Sant symptom and problem indices, and VAS of pain and urgency were used to quantify disease severity of the patients. In addition, the SF-36 health survey was used to evaluate patients’ quality of life.
The participating patients were asked to fill in the health education questionnaire once a week to consolidate their behavior of having healthy diets and lifestyles. We hypothesize that the patients will learn to eat healthy diets and live with healthy lifestyles to prevent the recurrence of BPS/IC outbreaks through repetitive health education. If the patients forget to check the health educational materials, the system will automatically send messages to remind them.
Statistical analysis
Descriptive statistics were used to analyze the demographic information, disease severity and questionnaires of the recruited patients, while the inferential statistics (Student’s t-test) were applied to compare the improvement of health status and symptoms between the study and control groups, as well as between pre-test and post-test for both groups.
SAS (SAS Institute Inc., Cary, NC, USA) was used as the tool for statistic analysis.
Results
It can be observed that there was no significant difference (Student’s t-test, P > 0.05) between the two groups with regard to demographic information, including age, marriage and education (Table 1). Neither anesthetic bladder volume nor disease severity showed a significant difference between the two groups. The disease severity assessed with O’Leary–Sant indices and VAS scales before ICT intervention presented no significant difference (Student’s t-test,
P > 0.05) between patients in the two groups (Table 1). Comparison of the SF-36 health survey between the study and
control groups before ICT intervention showed no significant difference (P > 0.05, unpaired Student’s t-test) in seven items, except general health (Table 1).
SF-36 health survey
As shown in Table 2, it can be observed that, except for the social function construct, all the other seven constructs showed significant improvement in the control group. In contrast, all the eight constructs of the SF-36 survey showed significant improvements after ICT intervention for the patients in the study group.
The degree of SF-36 health survey improvement after ICT intervention between the control and study groups was also compared. As shown in Table 2, except for the constructs of role physical and role emotional, the degree of improvements for the study group was significantly higher than the control group (P < 0.05), showing the effectiveness of the ICT intervention in health education.
O’Leary–Sant indices and VAS scales
As shown in Table 3, after ICT intervention, only O’Leary–Sant indices presented a significant difference for the control group (P < 0.01) by comparing the results of pre-test and post-test, whereas both the O’Leary–Sant indices and VAS scales showed significant improvements for the study group.
The degree of improvements of the O’Leary–Sant indices and VAS scales for both the control and study groups shows that VAS scales of the study group achieved significantly greater improvements compared with the control group (P < 0.05), whereas the O’Leary–Sant index showed no significant improvement (P > 0.05).
Discussion
BPS/IC patients are very sensitive to diet, such as foods, drinks, supplements and spices.10,15 Hence, to educate the
patients about consuming healthy food and avoiding sensitive foods is expected to be effective in preventing their recurrence. Clinical experience suggested that behavior or lifestyle modification can improve BPS/IC symptoms in some patients.1,17
By taking poor compliance of self-management regimens into consideration, Celler et al. proposed a Home Telecare System for monitoring physiological signs, scheduling medication and reminding patients to take medication, and healthcare education.17 It was shown to be effective in early the identification of adverse events to avoid hospital
readmission or to reduce length of stay in hospital. Izquierdo et al. reported that the home telemedicine system that is applied to transmit blood glucose and blood pressure data of older patients with type 2 diabetes to a nurse case manager is effective in identifying and remediating urgent situations.18
The education materials presented in Appendix I are intended to remind patients not to not eat food containing a great amount of potassium, as well as not to drink beverages containing caffeine, which is shown to be effective in reducing the recurrence of BPS/IC symptoms.
Smoking is associated with a higher risk of BPS/IC,11 and LUTS in women. As observed by Maserejian et al., female
smokers were more likely to experience LUTS symptoms, especially storage symptoms.19 It is believed that the factors
affecting acquisition of LUTS might also induce occurrence or recurrence of BPS/IC. To persuade patients to quit smoking should be an effective way to improve QOL of BPS/IC patients.
Certain types of exercise, such as pelvic floor muscle exercise, and wearing tight-fitting clothes might worsen BPS/IC symptoms in some patients.1 Hence, regular mild aerobic exercises, such as yoga, hiking, jogging and so on, thus
reaching a high PASE (physical activity scale for the elderly) score, are believed to contribute to reducing BPS/IC recurrences.20
Guided imagery or meditation was reported to be effective in managing the pain and symptoms for patients with BPS/IC,13 and in alleviating symptoms for patients with adjustment disorder, anxiety, and depression.21 Similar to
meditation, yoga has also been used as a therapy to activate the parasympathetic nervous system to lower heart rate and blood pressure, allowing it to effectively alleviate anxiety generally observed in BPS/IC patients. It can be practiced by patients who are unable to carry out moderate aerobic exercise, allowing them to experience the advantages of aerobic exercises.
Dyspareunia is widely observed in female BPS/IC patients, with pain as the most important finding significantly degrading the quality of life.22 It was estimated to occur in 49–90% of the BPS/IC patients; among them, 54% intended
to avoid intercourse most of the time because of the pain incurred.23 Furthermore, the RAND interstitial cystitis
epidemiology study showed that female BPS/IC patients experienced a much higher level of sexual dysfunction, such as lack of interest in sex, arousal difficulties and pain, compared with the general population.24 As pain during intercourse
is a strong indicator of poor quality of life for BPS/IC patients,25 reminding the patients to use lubricant and change
position during intercourse, as well as to clean the vulva and bath the abdomen with warm water after intercourse , through weekly health education is believed to be effective in reducing pain during and after intercourse.
Treatment and care of the vagina and genital area might affect sexual and reproductive morbidities for women.14 It is
reasonable to educate the patient on how to take care of the genital area when symptoms flare up after sexual intercourse.
In the present study, the Internet accompanied with SMS was used for intervention for BPS/IC patients. It was believed that Internet interventions were shown to be effective in the promotion of health behavior change, especially when reinforced by additional methods, such as SMS, to communicate with participants.26 Patients who understand the
information and have the knowledge related to a disease can facilitate behavior change and disease management. SMS was shown to be effective in improving healthcare processes and outcomes.
Furthermore, it was reported that administration of daily educational text messages by SMS improved knowledge and facilitated continuous use of oral contraceptives.27 In contrast, face-to-face behavior counseling accompanied by phone
interviews did not show improved adherence of oral contraceptives among young women.28 Text messaging able to hold
the privacy of participants is deemed as a cost-effectively way in delivering sensitive information, such as sexual health, which might be the reason causing such a discrepancy. Problems during or after intercourse regarding personal privacy frequently occur in patients with BPS/IC. Interventions by SMS showed positive short-term behavior change.29 It
mimics the efficiency and effectiveness of disease management using SMS in alleviating the symptoms of the symptom flares for BPS/IC patients.
As reported by Lailly et al., a good habit or behavior, such as eating, drinking or exercising
behavior, will be formed in a period ranging from 18 to 254 days, with a median of 66 days, for
participants with a good fit.
30Through an intervention of an 8-week (56 days) duration, a period
approximating to 66 days long enough to form good habits for patients, it can be observed that the
BPS/IC patients asked to check and follow the healthy behavior or lifestyle through weekly health
education by ICT intervention is useful to prevent recurrence or deterioration of the disease, which
in turn improve their QOL.
The E-health system supporting health education and providing SMS for patient self-management was shown to be effective in improving QOL and alleviating symptoms for BPS/IC patients in the 8-week follow up. Internet healthcare education is useful to consolidate healthy behavior and lifestyles for patients, as well as to self-manage their disease when the symptoms flare up.
This study was supported in part by Taichung Hospital (Grant no. CTU100-PC-002) and National Science Council of Taiwan (Grant no. NSC100-2410-H-166-007-MY3).
Conflict of interest
None declared.
References
1 Hanno PM, Burks DA, Clemens JQ et al. AUA guideline for the diagnosis and treatment of
interstitial cystitis/bladder pain syndrome. J. Urol. 2011; 185: 2162–70.
2 Hanno PM, Landis JR, Matthews CY et al. The diagnosis of interstitial cystitis revisited: lessons
learned from the National Institutes of Health Interstitial Cystitis Database study. J. Urol. 1999;
161: 553–7.
3 Homma Y, Ueda T, Tomoe H et al. Clinical guidelines for interstitial cystitis and hypersensitive
bladder syndrome. Int. J. Urol. 2009; 16: 597–615.
4 Fall M, Baranowski AP, Elneil S et al. EAU guidelines on chronic pelvic pain. Eur. Urol. 2010;
57: 35–48.
5 Moutzouris DA, Falagas ME. Interstitial cystitis: an unsolved enigma. Clin. J. Am. Soc. Nephrol.
2009; 4: 1844–57.
6 Altman D, Lundholm C, Milsom I et al. The genetic and environmental contribution to the
occurrence of bladder pain syndrome: an empirical approach in a nationwide population sample.
Eur. Urol. 2011; 59: 280–5.
7 Tunitsky E, Barber MD, Jeppson PC et al. Ridgeway bladder pain syndrome/interstitial cystitis in
twin sisters. J. Urol. 2012; 187: 148–52.
8 Kim SI, Kim HS. Effectiveness of mobile and Internet intervention in patients with obese type 2
diabetes. Int. J. Med. Inform. 2008; 77: 399–404.
9 Gold J, Aitken CK, Dixon HG et al. A randomised controlled trial using mobile advertising to
promote safer sex and sun safety to young people. Health Educ. Res. 2011; 26: 782–94.
10 Friedlander JI, Shorter B, Moldwin RM et al. Diet and its role in interstitial cystitis/bladder pain
syndrome (IC/BPS) and comorbid conditions. BJU Int. 2012; 109: 1584–91.
11 Tettamanti G, Nyman-Iliadou A, Pedersen NL et al. Influence of smoking, coffee, and tea
consumption on bladder pain syndrome in female twin. Urology 2011; 77: 1313–17.
12 Sharma M, Haider T. Yoga as an alternative and complementary therapy for patients suffering
from anxiety: a systematic review. J. Evid. Based Complementary Altern. Med. 2013; 18: 15–22.
13 Peters KM, Carrico DJ, Ibrahim IA et al. Characterization of a Clinical Cohort of 87 Women
with Interstitial Cystitis/Painful Bladder Syndrome. Urology 2008;71(4):634-40.
14 Hilber AM, Hull TH, Preston-Whyte E et al. A cross cultural study of vaginal practices and
sexuality: implications for sexual health. Soc. Sci. Med. 2010; 70: 392–400.
15 Carrico DJ, Peters KM, Diokno AC. Guided imagery for women with interstitial cystitis: results
of a prospective, randomized controlled pilot study. J. Altern. Complement. Med. 2008; 14: 53-60.
16 Bassaly R, Downes K, Hart S. Dietary consumption triggers in interstitial cystitis/bladder pain
syndrome patients. Female Pelvic Med. Reconstr. Surg. 2011; 17: 36–9.
17 Rovner E, Propert KJ, Brensinger C et al. Treatments used in women with interstitial cystitis: the
interstitial cystitis database (ICDB) study experience. The Interstitial Cystitis Data Base Study
Group. Urology 2000; 56: 940-5.
18 Celler BG, Lovell NH, Basilakis J Using information technology to improve the management of
chronic disease. Med. J. Aust. 2003; 179: 242–6.
19 Izquierdo R, Meyer S, Starren J et al. Detection and remediation of medically urgent situations
using telemedicine case management for older patients with diabetes mellitus. Ther. Clin. Risk
Manag. 2007; 3: 485–9.
20 Maserejian NN, Kupelian V, Miyasato G, McVary KT, McKinlay JB Are physical activity,
smoking and alcohol consumption associated with lower tract symptoms in men or women? Results
from a population based observation study. J. Urol. 2012; 188: 490–5.
21 Washburn RA, Ficker JL. Physical Activity Scale for the Elderly (PASE): the relationship with
activity measured by a portable accelerometer. J. Sports Med. Phys. Fitness 1999; 39: 336–40.
22 Srivastava M, Talukdar U, Lehan V. Meditation for the management of adjustment disorder
anxiety and depression. Complement. Ther. Clin. Pract. 2011; 17: 241–5.
23 Wehbe SA, Whitmore K, Kellogg-Spadt S. Urogenital complaints and female sexual dysfunction
(Part 1). J. Sex. Med. 2010; 7: 1704–13.
24 Kellogg-Spadt S, Whitmore KE. Role of the female urologist/urogynecologist. In: Goldstein I,
Meston CM, Davis SR, Traish AM (eds). Women’s Sexual Function and Dysfunction: Study,
Diagnosis and Treatment. Taylor and Francis, New York, 2006; 17: 708–14.
25 Bogart LM, Suttorp MJ, Elliott MN et al. Prevalence and correlates of sexual dysfunction among
women with bladder pain syndrome/interstitial cystitis. Urology 2011; 77: 576–80.
26 Nickel JC, Tripp D, Teal V et al. Sexual function is a determinant of poor quality of life for
women with treatment refractory interstitial cystitis. J. Urol. 2007; 177: 1832–6.
27 Webb TL, Joseph J, Yardley L et al. Using the Internet to promote health behavior change: a
systematic review and meta-analysis of the impact of theoretical basis, use of behavior change
techniques, and mode of delivery on efficacy. J. Med. Internet Res. 2010; 12: e4.
28 Castaño PM, Bynum JY, Andrés R et al. Effect of daily text messages on oral contraceptive
continuation: a randomized controlled trial. Obstet. Gynecol. 2012; 119: 14–20.
29 Berenson AB, Rahman MA. A Randomized controlled study of two educational interventions on
adherence with oral contraceptives and condoms. Contraception 2012; 86: 716–24.
30 Fjeldsoe BS, Marshall AL, Miller YD. Behavior change interventions delivered by mobile
telephone short-message service. Am. J. Prev. Med. 2009; 36: 165–73.
31 Lailly P, Van Jaarsveld CHMP et al. How are habits formed: modeling habit formation in the
real world. Eur. J. Soc. Psychol. 2010; 40: 998–1009.
Fig. 1 Experimental procedure.
E: Emergency intervention R: Weekly Health Education
F: Questionnaires
F1: SF-36
F2: O’Leary-Sant Symptom Index and Problem Index Scale
F3: VAS scale of pain &urgency
Table 1 Comparison of demographic information, anesthetic bladder volume, SF-36, and disease severity between study and control groups Demographic information Control (n = 32) Study (n = 33) P-value
Age in years (mean ± SD) 49.5 ± 11.8 46.5 ± 10.2 0.28
Education High school 15 (46.9%) 19 (59.4%) 0.39 University 17 (53.1%) 14 (40.6%) Marriage Yes 30 (93.8%) 27 (81.2%) 0.14 No 2 (6.2%) 6 (18.8%)
Anesthetic bladder volume 649.5 ± 152.7 607.5 ± 210.3 0.36 O’Leary–Sant Index Symptom 11.34 ± 4.78 11.33 ± 4.14 0.99 Problem 10.47 ± 4.71 11.55 ± 5.03 0.38 VAS Pain 5.16 ± 2.58 4.91 ± 2.78 0.71 Urgency 5.06 ± 2.97 5.12 ± 2.60 0.93 SF36–Physical function 81.88 ± 18.17 72.12 ± 23.19 0.06 SF36–Role physical 63.28 ± 38.62 48.48 ± 44.61 0.16 SF36–Bodily pain 63.78 ± 26.31 52.24 ± 24.05 0.07 SF36–General health 54.38 ± 22.69 38.61 ± 23.81 0.01* SF36–Vitality 48.28 ± 13.95 42.73 ± 21.25 0.22 SF36–Social function 66.02 ± 18.58 62.88 ± 25.67 0.58 SF36–Role emotional 59.38 ± 43.78 45.45 ± 47.01 0.22 SF36–Mental health 53.38 ± 18.81 47.15 ± 19.99 0.20
Student’s t-test with *P < 0.05.
Table 2 SF-36 health survey of control and study groups before and after ICT intervention SF-36 health
survey
Groups
Control (n = 32) Study (n = 33) Control vs
study Pre-test (mean ± SD) Post-test (mean ± SD) Improve (mean ± SD) P-value Pre-test (mean ± SD) Post-test (mean ± SD) Improve (mean ± SD) P-value t P-value Physical function 81.88 ± 18.17 83.91 ± 17.21 2.03 ± 3.33 0.003** 72.12 ± 23.19 81.67 ± 19.15 9.55 ± 19.58 0.01* 2.14 0.04* Role physical 63.28 ± 38.62 72.66 ± 30.69 9.38 ± 17.68 0.01* 48.48 ± 44.61 74.24 ± 37.23 25.76 ± 48.20 0.009** 1.81 0.08 Bodily pain 63.78 ± 26.31 68.53 ± 21.87 4.75 ± 7.69 0.002** 52.24 ± 24.05 69.15 ± 17.92 16.91 ± 22.70 <0.001** * 2.87 0.01* General health 54.38 ± 22.69 57.59 ± 18.64 3.22 ± 7.25 0.02* 38.61 ± 23.81 52.48 ± 23.28 13.88 ± 22.28 0.005** 2.58 0.01* Vitality 48.28 ± 13.95 51.41 ± 13.45 3.13 ± 4.88 <0.001** * 42.73 ± 21.25 60.76 ± 20.35 18.03 ± 22.88 <0.001** * 3.61 0.005** Social function 66.02 ± 18.58 68.75 ± 17.39 2.73 ± 10.40 0.15 62.88 ± 25.67 75.00 ± 17.68 12.12 ± 19.64 0.005** 2.40 0.02* Role emotional 59.38 ± 43.78 75.00 ± 38.80 15.63 ± 26.75 0.005** 45.45 ± 47.01 77.78 ± 34.02 32.32 ± 3.69 <0.001** * 1.85 0.07 Mental health 53.38 ± 18.81 55.00 ± 18.32 1.63 ± 4.41 0.05* 47.15 ± 19.99 58.18 ± 17.95 11.03 ± 19.55 0.007** 2.66 0.01* Student’s t-test with *P < 0.05, **P < 0.01, and ***P < 0.001.
Table 3 Disease severity of control and study groups before and after ICT intervention Disease
severity
Groups
Control (n = 32) Study (n = 33) Control vs study
Pre-test (mean ± SD) Post-test (mean ± SD) Improve (mean ± SD) P-value Pre-test (mean ± SD) Post-test (mean ± SD) Improve (mean ± SD) P-value t P-value O’Leary-Sant Index Symptom 11.34 ± 4.78 9.19 ± 4.19 2.16 ± 4.12 0.01* 11.33 ± 4.14 7.76 ± 4.22 3.58 ± 5.61 0.005** 1.16 0.25 Problem 10.47 ± 4.71 5.81 ± 3.80 4.66 ± 4.86 <0.001* ** 11.55 ± 5.03 9.24 ± 5.43 2.30 ± 6.13 0.04* 1.71 0.09 VAS Scale Pain 5.16 ± 2.58 5.13 ± 2.42 0.03 ± 0.86 0.84 4.91 ± 2.78 3.03 ± 1.90 1.88 ± 3.14 0.005** 3.21 0.006** Urgency 5.06 ± 2.97 4.94 ± 2.66 0.13 ± 0.75 0.35 5.12 ± 2.60 3.27 ± 2.17 1.85 ± 3.03 0.005** 3.12 0.006**
Appendix I
Weekly check for consolidating the behavior promoted by health education
Please check “Yes” or “No” based on your experience during the past week.
Y N Item Description
1 Do you follow the suggested diets? 2 Do you drink 1500 c.c. of water or so daily?
3 Do you eat banana, pineapple, citrus fruit, or other food containing a great amount of potassium. 4 Do you drink any beverage that contains alcohol, coffee, vinegar or tea?
5 Do you smoke?
6 Have you done mild aerobic exercise, such as yoga, hiking, jogging, etc,? 7 Do you wear cozy, loose clothes, and put on underwear mainly made of cotton?
If you don’t have pain or sexual intercourse, please check “Unavailable”, otherwise check “Yes” or “No” according to your personal experience.
Y N NA Item Description
8 I have bathed the whole lower abdomen with warm water (40°C) more than once a day, each lasting for 15 min, or placed a heat pad over the abdomen to keep it warm to relieve uncomfortable symptom, especially after sexual intercourse. 9 Before or after menstruation. I used a heat pad to relieve uncomfortable symptom.
10 I have used lubricant (ointment) to relieve uncomfortable feeling during intercourse.
11 When feeling uncomfortable during intercourse, I have changed the position to the top position to maneuver the force exerted and alleviate the pain.
12 I have washed and cleaned the vulva and keep them dry after intercourse.
13 When I experience flare up of symptoms without definite causes, I have tried to relief the symptoms with guided imagery, such as meditation or listening to music.
Appendix II
SMS for management of emergent outbreaks
Event Question Answer
1 Pain or urgency after eating specific food.
Drink a great amount of water to dilute urine concentration. If the symptom is severe and cannot be relieved, visit your physician.
2 Feeling of bladder pain is gradually
deteriorating. Bath the whole lower abdomen with warm water (40°C) more than once every day,each time lasting for 15 min. You can also place a heat pad over the abdomen to keep it warm. If the symptom cannot be relieved, visit your physician.
3 Pain or uncomfortable feeling caused by allergy induced by, for example, weather change or drugs.
Take anti-allergic medication for alleviation of the symptom. If the symptom has lasted for a few days without any improvements, visit your physician.
4 Pain or uncomfortable feeling of abdomen after menstruation.
You can place a heat pad over the abdomen to keep it warm to alleviate uncomfortable symptom.
5 Suspected urethral infection after intercourse.
Drink a lot of water (2000 c.c. a day) during two days after the recurrence. Take a rest by asking someone in your family to do housework for you. If the symptom lasts for a few days, visit your physician.
6 Pain after intercourse. Bath the whole abdomen with warm water (40°C) for 20 min. You can also place a heat pad over the abdomen to keep it warm to alleviate uncomfortable symptom. If the symptom has lasted for a few days, visit your physician.
7 Stress caused by tedious affairs. (1) Sit on the floor and extend your neck muscles by keeping the posture for at least 10 s. Repeat the exercise for several times. (2) Relax all of your body muscles through meditation or concentration on a certain part of your body, e.g. nose tip or fingers.
8 Others (please address your
complaints)