Kaohsiung J Med Sci October 2009 • Vol 25 • No 10 537 The incidence and mortality rate of hepatocellular
carcinoma (HCC), one of the most common cancers worldwide [1], are rapidly increasing. Associated dis-eases include chronic viral hepatitis types B and C, which comprise approximately 75% of all HCCs [1,2], and liver cirrhosis (70–80% of all cases) [1,2]. Without
treatment, advanced HCC usually causes death within months, and long-term survival is rare [1]. Despite recent advances in diagnostic and therapeutic modal-ities, prognosis is usually poor, particularly in patients with coexisting liver cirrhosis.
In Taiwan, the incidence of HCC per 100,000 people is reportedly as high as 26 and 8 in males and females, respectively [3].
Pyogenic liver abscess usually occurs in patients with diabetes mellitus and malignancy [4]. Possible causes include hematogenous dissemination, ascend-ing cholangitis and superinfection of necrotic tissue [5]. Escherichia coli is the most common bacterium Received: Dec 23, 2008 Accepted: Mar 10, 2009
Address correspondence and reprint requests to: Dr Liang-Yen Wang, Division of Hepatobiliary Medicine, Department of Internal Medicine, Kaohsiung Medical University, 100 Tzyou 1st Road, Kaohsiung 807, Taiwan.
E-mail: [email protected]
H
EPATOCELLULAR
C
ARCINOMA
A
SSOCIATED
W
ITH
L
IVER
A
BSCESS
Ching-I Huang,1Liang-Yen Wang,1,4Ming-Lun Yeh,1Ming-Yen Hsieh,1,3Jee-Fu Huang,2,3 Zu-Yau Lin,1,4and Wan-Long Chuang1,4
1Division of Hepatobiliary Medicine, Department of Internal Medicine, Kaohsiung Medical University Hospital, 2Department of Internal Medicine, Kaohsiung Municipal Hsiao-Kang Hospital,
3Graduate Institute of Medicine, and 4Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
Hepatitis B and hepatitis C are highly prevalent in Taiwan. Chronic hepatitis patients are at high risk of progression to liver cirrhosis and hepatocellular carcinoma (HCC). However, HCC in asso-ciation with liver abscess is very rare. Accordingly, this study analyzed the characteristics of HCC patients with liver abscess to improve the differential diagnosis of this condition. From January 2005 to July 2007, the medical records of nine HCC patients (4 females, 5 males; mean age, 65.8 years) treated for abscess formation at Kaohsiung Medical University Hospital were retro-spectively reviewed. Their clinical characteristics, images, management approaches and outcomes were analyzed. Fever and highly elevated alkaline phosphatase levels were noted in all patients. All aspirate cultures revealed Klebsiella pneumoniae. All of the cases of HCC were confirmed by cytology or pathology. The imaging studies, which included abdominal ultrasonography and com-puted tomography, revealed liver tumors in all patients. In some cases, lead-enhanced hypervas-cular areas were noted. The patients were treated with antibiotic therapy, transhepatic arterial chemoembolization, or surgery. The findings of this study indicate that focal liver inflammatory changes may mimic solid neoplasms. Differential diagnosis of HCC with abscess is extremely difficult and may require aspiration cytology or pathology.
Key Words:abdominal sonography, computed tomography, hepatocellular carcinoma, liver abscess, magnetic resonance imaging
worldwide. Klebsiella pneumoniae was first reported in Taiwan in the 1900s and now surpasses E. coli as the predominant isolate in patients with hepatic abscess [4–6].
An HCC manifesting as a liver abscess, due to either spontaneous liquefied necrosis of the tumor interior or biliary obstruction caused by a tumor fragment [7], is a condition rarely reported in the literature.
This study reviewed all HCC patients treated at this institution during the past 2.5 years and describes the characteristics of those who initially presented with liver abscess.
P
ATIENTS ANDM
ETHODSThis study retrospectively reviewed the medical records of 906 HCC patients treated between January 2005 and July 2007 at Kaohsiung Medical University Hospital (Kaohsiung, Taiwan). Data were collected for all treatment-naïve HCC patients who were initially diagnosed with liver abscess during hospitalization. All patient data, including clinical data, imaging stud-ies and histology, were entered into a database for further analysis.
R
ESULTSThere were a total of nine patients (5 males, 4 females) who were initially diagnosed with liver abscess and in whom the final histology revealed HCC.
Patient characteristics
Nine of 906 (0.99%) patients had HCC with abscess presenting as pyogenic liver abscess. The mean age of the nine patients was 65.8 years (range, 52–80 years). Of the six hepatitis virus carriers, two, one, and three patients had hepatitis B, hepatitis C, and both hepati-tis B and C, respectively. Only three patients were negative for both hepatitis B and hepatitis C. Three patients had diabetes mellitus. None of the patients were diagnosed with combined hepatolithiasis.
Manifestations
Symptoms included fever in all nine patients (with chills in 3), right-upper-quadrant pain in four, poor appetite in four, and fatigue in three. Other promi-nent signs included right-upper-quadrant tenderness in four, and jaundice (with indications including icteric sclera, tea-colored urine, or clay-colored stool) in two. No hepatomegaly or bulging abdominal mass was noted (Table 1).
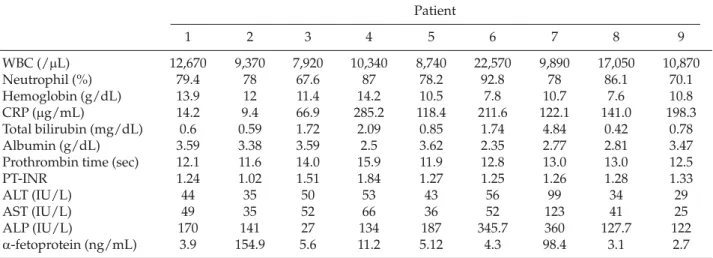
Laboratory data
Of the nine patients, leukocytosis with left shift was noted in six. Anemia (defined as hemoglobin <13g/dL in males and < 12 g/dL in females) was noted in seven patients. The C-reactive protein levels (normal< 5 μg/ mL) were abnormal in all patients. Hyperbilirubinemia (normal 0.2–1.0 mg/dL) was noted in one patient. Six patients had hypoalbuminemia (normal 3.5–4.5 g/dL). In one patient, the prothrombin time was 4 seconds longer than normal (Table 2).
Mild-to-moderate abnormal serum aminotrans-ferase level (< 4-fold increase) and elevated serum
Table 1.Clinical characteristics of hepatocellular carcinoma patients with liver abscess Patient 1 2 3 4 5 6 7 8 9 Sex M M F M F F M F M Age (yr) 52 70 61 55 79 80 61 77 57 HBV + − + + + − + − − HCV + − − − + − + − + DM − + − − + − + − − Fever + + + + + + + + + Chills − − − + + − − − + RUQ pain + + + − − − − − + Poor appetite − − − + + − − + + Fatigue − − − + + − − − + Jaundice − − − + − − + − −
alkaline phosphatase level were noted in eight of the nine patients (Table 2).
Work-up of liver abscesses
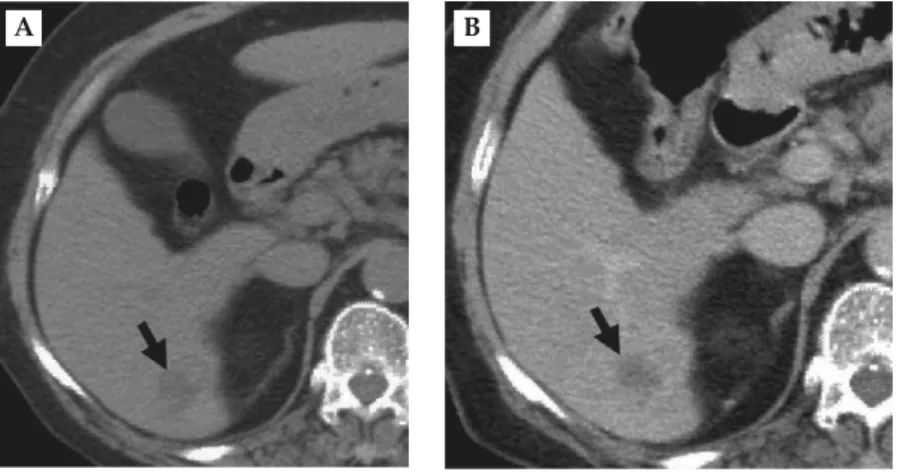
All patients underwent ultrasonography (US; Figure 1) and computed tomography (CT; Figure 2) examina-tions to detect the presence of abscess and character-istics of the liver (Table 3). Abscess aspiration and culture collection were also performed. All abscess cultures were positive for K. pneumoniae. All patients underwent antibiotic therapy, and none required drainage tube insertion.
Characteristics of HCC
Tumor size was 3–13 cm (mean, 5 cm). In eight of the nine patients, liver abscess and HCC were both diag-nosed during the initial hospitalization. One patient ini-tially diagnosed with abscess suffered one recurrence but, after the patient underwent resection of the lesion, the final diagnosis was HCC with liver abscess.
Management of HCC and outcomes
After antibiotic treatment of the liver abscess, one pa-tient received conservative treatment due to hepatic failure. Two patients underwent tumor resection after antibiotic treatment, and neither revealed evidence of recurrence during follow up. Most (6) patients under-went transhepatic arterial chemoembolization after completing antibiotic therapy. One of the nine patients died of sepsis after undergoing three transhepatic arte-rial chemoembolization treatments.
D
ISCUSSIONPatients with liver abscess usually present with fever, chills, anorexia, fatigue, or other symptoms such as nausea, vomiting, right-upper-quadrant pain, diffuse abdominal pain, pleuritic chest pain, and jaundice [8]. Fever, the most common symptom, reportedly occurs in 70–95% of cases [8]. All patients in the current study were febrile. Some also exhibited right-upper-quad-rant pain, fatigue, and jaundice. The most common laboratory finding in these patients is leukocytosis, Table 2.Laboratory data of hepatocellular carcinoma patients with liver abscess
Patient 1 2 3 4 5 6 7 8 9 WBC (/μL) 12,670 9,370 7,920 10,340 8,740 22,570 9,890 17,050 10,870 Neutrophil (%) 79.4 78 67.6 87 78.2 92.8 78 86.1 70.1 Hemoglobin (g/dL) 13.9 12 11.4 14.2 10.5 7.8 10.7 7.6 10.8 CRP (μg/mL) 14.2 9.4 66.9 285.2 118.4 211.6 122.1 141.0 198.3 Total bilirubin (mg/dL) 0.6 0.59 1.72 2.09 0.85 1.74 4.84 0.42 0.78 Albumin (g/dL) 3.59 3.38 3.59 2.5 3.62 2.35 2.77 2.81 3.47
Prothrombin time (sec) 12.1 11.6 14.0 15.9 11.9 12.8 13.0 13.0 12.5
PT-INR 1.24 1.02 1.51 1.84 1.27 1.25 1.26 1.28 1.33
ALT (IU/L) 44 35 50 53 43 56 99 34 29
AST (IU/L) 49 35 52 66 36 52 123 41 25
ALP (IU/L) 170 141 27 134 187 345.7 360 127.7 122
α-fetoprotein (ng/mL) 3.9 154.9 5.6 11.2 5.12 4.3 98.4 3.1 2.7
WBC= white blood cell count; CRP = C-reactive protein; PT-INR = prothrombin time-international normalized ratio; ALT = alanine transaminase; AST= aspartate transaminase; ALP = alkaline phosphatase.
Figure 1.Abdominal sonography shows hepatocellular carcinoma with liver abscess: an irregular 5-cm mosaic echoic mass was found in segment 6 of the liver.
which reportedly occurs in 70–82% of patients [8]. Alkaline phosphatase levels 2–3 times the upper limit of normal are also common [6,8]. Elevated transami-nase levels and hypoalbuminemia are also commonly observed. All of the patients in the current study ex-hibited leukocytosis and high alkaline phosphatase levels [9].
An abscess-like clinical presentation, particularly with the coexistence of tumor necrosis, is one symp-tom of HCC [7,10]. According to Smalley et al, these features occur in approximately 25% of all HCC patients with a non-cirrhotic liver [11]. The literature also describes several cases of abscess-like clinical symptoms [7]. One explanation for these similarities is neoplasm-associated granulocytosis resulting from granulopoietin production by tumor cells as well as pyrogen production by malignant tumor cells or by macrophages followed by tumor necrosis [7,12].
For early diagnosis and differential diagnosis of liver abscess, careful imaging of manifestations and their characteristics is essential. In this study, CT scans revealed low attenuation in all liver abscesses, and 91.7% of the enhanced lesions had a rim-shaped en-hancement in the abscess wall, as described elsewhere [9]. Honeycomb-like, grid-like or strip-like enhance-ments reportedly occur in 75% of cases [9]. The CT findings of hepatic abscess are usually unremarkable, and diagnosing abscess is rarely difficult [9].
An HCC typically presents as an intense enhance-ment in the arterial phase and as a contrast washout in the subsequent venous contrast phase [10]. Well-defined margins are more common in large HCC
lesions than in smaller tumors [10]. The HCC is likely to present as a dominant mass with underlying liver damage characterized by smooth and encapsulated margins, necrosis and hypervascularity [10]. Recog-nizing the enhanced pattern characteristics of HCC is essential for accurate diagnosis. Distinguishing the hypervascular malignant area from the abscess lesion is also important.
A US image of liver abscess usually shows a low-echoic to mixed-low-echoic lesion [13,14]. The margin may be blurred or irregular due to inflammation of surrounding areas [13,14]. During the early stage, mix-echoic parenchyma mass lesions are common, but significant tissue liquefaction is rare [13,14]. Follow-ing the course of inflammation, sonography may re-veal a low-echoic mass lesion. However, HCCs of < 3 cm in diameter usually appear hypoechoic with-out posterior enhancement whereas larger lesions, which are often necrotic and fibrotic, exhibit a more heterogeneous (mosaic) pattern [10]. Accurate differ-ential diagnosis of HCC is essdiffer-ential in endemic areas such as Taiwan. Color Doppler US or even contrast injection are often helpful.
US findings of HCC with abscess may reveal sin-gle or multiple carcinomas, and either lobe may be involved. The size also varies. US can reveal the fea-tures of the liver abscess and, in some cases, those of the tumor itself. In the cases reported here, enhanced abdominal CT revealed that the area affected by the tumor was in the advanced arterial phase, which enabled the differential diagnosis of HCC alone versus liver abscess alone. Color Doppler or
A B
Figure 2.Abdominal computed tomography shows hepatocellular carcinoma with liver abscess. (A) Unenhanced computed tomogra-phy revealed an internal heterogenic attenuated tumor with an irregular and unclear margin (arrow) in segment 6 of the liver. (B) No obvious internal enhancement was noted after contrast infusion (arrow).
T
able 3.
Imaging r
esults for hepatocellular car
cinoma patients with liver abscess
Patient 1 2 3 4 567 8 9 Number Multiple Dif fuse Single Single Single Multiple Single Single Single Location Bilateral Right lobe S6 S5 S6 S8 S6 S3 S3 T umor size Lar gest 6 cm > 10 cm 5 cm 3 cm 3 cm 5 cm 3.2 cm 5 cm 9.5 cm Sonographic Low peripheral Low peripheral Isoechoic Mixed-echoic Low-echoic Mixed-echoic Low-echoic Mixed-echoic Low-echoic featur es ring, mixed ring, mixed-tumor , tumor , low tumor , poorly tumor , low tumor , tumor , tumor , echoic tumor , echoic tumor , poorly peripheral defined peripheral irr egular irr egular irr egular low-echoic and low-echoic defined ring mar gin ring mar gin mar gin, low mar gin central low-septated mar gin periphery echoic tumor , masses homogeneous echogenicity CT featur es Isoechoic to Dif fuse Low-W all-low-density isoechoic to attenuation attenuation
attenuation attenuation attenuation
attenuation thickened tumor in low-density lesion, blurr ed lesion, poorly lesion, poorly lesion, lesion, lesion, and septated pr econtrast tumor over mar gin, defined, defined, irr egular irr egular unenhanced mass with and venous right lobe unenhanced unenhanced unenhanced mar gin, mar gin, on contrast interior phase, high-(> 10 cm) in on contrast on contrast on contrast central unenhanced CT fluid density tumor pr econtrast CT CT CT liquefaction on contrast density in arterial and venous CT phase
phase, high- density tumor in arterial phase with multiple low- density masses inside tumor
Aspiration Pus-like Pus-like Pus-like Pus-like Pus-like sticky Pus-like Pus-like Pus-like Pus-like featur es sticky sticky sticky sticky fluid with sticky sticky sticky sticky fluid fluid fluid fluid mild particles fluid fluid fluid fluid S5 = segment 5; S6 = segment 6; S8 = segment 8; S3 = segment 3; CT = computed tomography .
contrast-enhanced imaging studies are essential to diagnose HCC. Detailed examination of the aspirate is also needed to identify malignant cells.
An abscess-like presentation is one marker for HCC, particularly in patients with tumor necrosis. Distinguishing between HCC and liver abscess with-out aspiration findings and using clinical presenta-tions alone is extremely difficult. In this study, liver tumor aspiration frequently reveals not only pus, but also HCC tissue, which was further confirmed by pathology. The aspiration procedure is essential to diagnose HCC.
Liver abscess and hepatic tumor necrosis are diffi-cult to distinguish by clinical symptoms, serology examination and imaging studies. Verification by punc-tate pathology is essential in HCC-endemic areas of Taiwan.
R
EFERENCES1. But DY, Lai CL, Yuen MF. Natural history of hepatitis-related hepatocellular carcinoma. World J Gastroenterol 2008;14:1652–6.
2. Tan A, Yeh SH, Liu CJ, et al. Viral hepatocarcinogenesis: from infection to cancer. Liver Int 2008;28:175–88. 3. Kao JH, Chen DS. Changing disease burden of
hepato-cellular carcinoma in the Far East and Southeast Asia. Liver Int 2005;25:696–703.
4. Chan KS, Chen CM, Cheng KC, et al. Pyogenic liver abscess: a retrospective analysis of 107 patients during a 3-year period. Jpn J Infect Dis 2005;58:366–8.
5. Branum GD, Tyson GS, Branum MA, et al. Hepatic abscess. Changes in etiology, diagnosis, and manage-ment. Ann Surg 1990;212:655–62.
6. Wong WM, Wong BC, Hui CK, et al. Pyogenic liver abscess: retrospective analysis of 80 cases over a 10-year period. J Gastroenterol Hepatol 2002;17:1001–7.
7. Yeh TS, Jan YY, Jeng LB, et al. Hepatocellular carcinoma presenting as pyogenic liver abscess: characteristics, diagnosis, and management. Clin Infect Dis 1998;26: 1224–6.
8. Lederman ER, Crum NF. Pyogenic liver abscess with a focus on Klebsiella pneumoniae as a primary pathogen: an emerging disease with unique clinical characteristics. Am J Gastroenterol 2005;100:322–31.
9. Wang CL, Guo XJ, Qiu SB, et al. Diagnosis of bacterial hepatic abscess by CT. Hepatobiliary Pancreat Dis Int 2007;6:271–5.
10. Saar B, Kellner-Weldon F. Radiological diagnosis of hepatocellular carcinoma. Liver Int 2008;28:189–99. 11. Smalley SR, Moertel CG, Hilton JF, et al. Hepatoma in
the noncirrhotic liver. Cancer 1988;62:1414–24.
12. Takayama T, Makuuchi M, Kojiro M, et al. Early hepa-tocellular carcinoma: pathology, imaging, and therapy. Ann Surg Oncol 2008;15:972–8.
13. Mortele KJ, Segatto E, Ros PR. The infected liver: radiologic-pathologic correlation. Radiographics 2004; 24:937–55.
14. Ralls PW, Barnes PF, Radin DR, et al. Sonographic fea-tures of amebic and pyogenic liver abscesses: a blinded comparison. AJR Am J Roentgenol 1987;149:499–501.
收文日期:97 年 12 月 23 日 接受刊載:98 年 3 月 10 日 通訊作者:王良彥醫師 高雄醫學大學附設醫院內科部肝膽胰內科 高雄市 807 三民區自由一路 100 號