Introduction
Genetic counseling of mosaic trisomy at amniocente-sis is difficult because of the phenotypic variability
associated with the condition; some fetuses exhibit the typical phenotype, while others are normal [1–3]. Tri-somy 9, mosaic or non-mosaic, is a relatively uncom-mon chromosomal abnormality that has characteristic phenotypic features including growth and mental retar-dation, dysmorphic faces with low-set malformed ears, microphthalmia, a bulbous nose and a small mouth, a high-arched palate, congenital heart defects (most com-monly ventricular septal defect), genitourinary anomalies (hypoplastic genitalia, cryptorchidism, cystic kidneys, or hydronephrosis), skeletal anomalies (joint dislocations *Correspondence to: Dr Chih-Ping Chen, Department
of Obstetrics and Gynecology, Mackay Memorial Hospital, 92, Section 2, Chung-Shan North Road, Taipei, Taiwan.
E-mail: [email protected] Accepted: July 7, 2010
M
OSAIC
T
RISOMY
9
AT
A
MNIOCENTESIS
: P
RENATAL
D
IAGNOSIS AND
M
OLECULAR
G
ENETIC
A
NALYSES
Chih-Ping Chen1,2,3,4,5,6*, Hsien-Ming Lin7, Yi-Ning Su8, Schu-Rern Chern2, Fuu-Jen Tsai4,9, Pei-Chen Wu1, Chen-Chi Lee1, Yu-Ting Chen2, Meng-Shan Lee1, Chen-Wen Pan1, Wayseen Wang2,10
Departments of 1Obstetrics and Gynecology and 2Medical Research, Mackay Memorial Hospital, 5Institute of
Clinical and Community Health Nursing, 6Department of Obstetrics and Gynecology, School of Medicine, National Yang-Ming University, 7Department of Obstetrics and Gynecology, Far-Eastern Memorial Hospital,
Pan-Chiao, 8Department of Medical Genetics, National Taiwan University Hospital, 10Department of Bioengineering, Tatung University, Taipei, 3Department of Biotechnology, Asia University, 4School of Chinese
Medicine, College of Chinese Medicine, China Medical University, 9Departments of Medical Genetics and Medical Research, China Medical University Hospital, Taichung, Taiwan.
SUMMARY
Objective:To present prenatal diagnosis and molecular genetic analyses of mosaic trisomy 9.
Materials, Methods and Results:A 35-year-old woman, gravida 3, para 1, underwent amniocentesis at 17 weeks of gestation because of her advanced maternal age. Amniocentesis revealed a karyotype of 47,XX,+9[3]/ 46,XX[6]. Repeat amniocentesis at 19 weeks of gestation revealed a karyotype of 47,XX,+9[6]/46,XX[19]. At 22 weeks of gestation, she was referred to a tertiary medical center for genetic counseling, and amniocentesis revealed a karyotype of 47,XX,+9[2]/46,XX[22]. Array comparative genomic hybridization analysis of uncul-tured amniocytes revealed no genomic imbalance in chromosome 9. However, interphase fluorescence in situ hybridization analysis of uncultured amniocytes showed that nine (18%) of 50 cells were trisomic for chromo-some 9. Polymorphic DNA marker analyses also revealed a diallelic pattern with unequal biparental inheritance of chromosome 9 and a dosage ratio of 1:18 (paternal allele:maternal allele) in the uncultured amniocytes and a dosage ratio of 1:36 in the cultured amniocytes, indicating that the euploid cell line had maternal uniparental isodisomy for chromosome 9. Level II ultrasound demonstrated bilateral ventriculomegaly. The pregnancy was subsequently terminated, and a malformed fetus was delivered. Postnatal cytogenetic and polymorphic DNA marker analyses of the fetal and extraembryonic tissues confirmed the prenatal diagnosis.
Conclusion:Mosaic trisomy 9 carries a high risk of fetal abnormalities warranting detailed sonographic investi-gation of congenital malformations. Mosaic trisomy 9 can be associated with maternal uniparental disomy for chromosome 9 in euploid cell lines. Array comparative genomic hybridization is limited for the detection of low-level mosaicism. [Taiwan J Obstet Gynecol 2010;49(3):341–350]
or deformations), and central nervous system anom-alies (hydrocephalus or Dandy-Walker malformation) [4–11]. Cases with mosaic trisomy 9 have been re-ported to be associated with maternal uniparental dis-omy for chromosome 9 (UPD 9) [12–14]. Here, we report the prenatal diagnosis and molecular genetic analyses of mosaic trisomy 9 with maternal isodisomy of chromosome 9 in a second-trimester fetus with ven-triculomegaly and facial dysmorphism.
Materials, Methods and Results
A 35-year-old woman, gravida 3, para 1, underwent amniocentesis at 17 weeks of gestation because of her advanced maternal age. She had experienced one spon-taneous abortion and had a 12-year-old healthy son. Her husband was 38 years old. Both parents were healthy, and there was no family history of congenital malformations. In three out of nine separated colonies of amniocytes, an abnormal karyotype of 47,XX,+9 was found (Figure 1), while the other six colonies had a karyotype of 46,XX. The cytogenetic result of amnio-centesis was 47,XX,+9[3]/46,XX[6]. Repeat amniocen-tesis at 19 weeks of gestation revealed a karyotype of 47,XX,+9[6]/46,XX[19]. She was referred to Mackay Memorial Hospital for genetic counseling at 22 weeks of gestation, and amniocentesis was repeated. Cytoge-netic analysis of cultured amniocytes revealed a karyotype of 47,XX,+9[2]/46,XX[22]. The parental karyotypes were normal. Array comparative genomic hybridization (aCGH) analysis of uncultured amniocytes did not mani-fest any genomic imbalances in chromosome 9 (Figure 2). Fluorescence in situ hybridization (FISH) analysis of uncultured interphase amniocytes using TelVysion 9q SpectrumOrange DNA probe (Abbott, IL, USA) showed three signals in nine out of 50 uncultured amniocytes and two signals in the remaining 41 amniocytes, indi-cating low-level mosaicism for trisomy 9 (Figure 3). Quantitative fluorescent polymerase chain reaction (QF-PCR) analyses of uncultured and cultured amnio-cytes using informative microsatellite markers specific for chromosome 9 revealed a diallelic pattern with un-equal biparental inheritance of chromosome 9 (Figure 4). The uncultured amniocytes had a dosage ratio of 1:18 (paternal allele:maternal allele), and the cultured amniocytes had a dosage ratio of 1:36. The maternal allele dosage was much greater than the paternal allele dosage, indicating that the euploid cell line contained two homologous chromosomes 9 of maternal origin and had maternal uniparental isodisomy 9. Trisomy 9 mosaicism in this case was most likely the result of a postzygotic mitotic error or less likely the result of
partial trisomic zygote rescue of a meiotic II non-disjunction error of maternal origin.
At 24 weeks of gestation, level II ultrasound showed bilateral ventriculomegaly. The parents elected to ter-minate the pregnancy. A 544 g malformed fetus was delivered with clenched hands, hypertelorism, a large
1 6 13 19 20 21 22 Y X 14 15 16 17 18 7 8 9 10 11 12 2 3 4 5 Figure 1.A karyotype of 47,XX,+9. Chromosome 9 p24.3 p24.2 p24.1 p23 p22.3 p22.2 p22.1 p21.3 p21.2 p21.1 p13.3 p13.2 p13.1 p12 p11.2 p11.1 q11 q12 q13 q21.11 q21.12 q21.13 q21.2 q21.31 q21.32 q21.33 q22.1 q22.2 q22.31 q22.32 q22.33 q31.1 q31.2 q31.3 q32 q33.1 q33.2 q33.3 q34.11 q34.12 q34.13 q34.2 q34.3 20 0 40 60 80 100 120 140 .2233.567 1 Ratio 1.52 3 4.5
Figure 2.Array comparative genomic hybridization analysis
of uncultured amniocytes shows no genomic imbalance in chromosome 9.
forehead, bilateral epicanthal folds, a broad nasal bridge, low-set posteriorly rotated ears, a thin upper lip, micro-gnathia, and a short neck (Figure 5).
Cytogenetic analyses of the fetal and extraembry-onic tissues showed a karyotype of 47,XX,+9/46,XX.
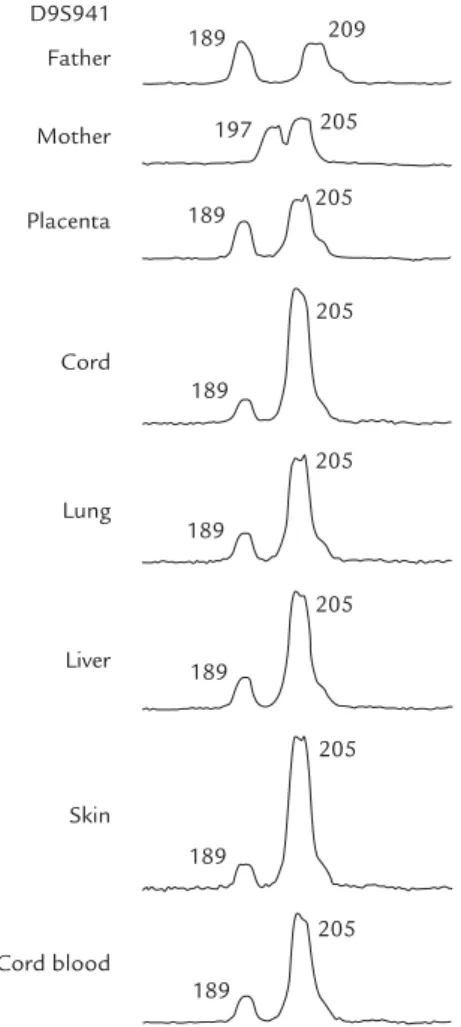
The levels of trisomy 9 in the cells of various tissues were 11% (11/100) in the cord blood, 5% (2/40) in the skin, 2.5% (1/40) in the lung, 22.5% (9/40) in the liver, 10% (4/40) in the cord, 17.5% (7/40) in the amnion, and 100% (40/40) in the placenta. Polymorphic DNA marker analyses of the uncultured fetal and extraembryonic tis-sues showed a diallelic pattern with unequal biparental inheritance of chromosome 9 (Figure 6). The uncultured tissues of cord, lungs, liver, skin, and cord blood had a paternal:maternal dosage ratio of 1:6, and the uncul-tured tissue of placenta had a dosage ratio of 1:2.
Discussion
The present case shows the usefulness of interphase FISH and QF-PCR, and the limitations of aCGH for the identification of low-level mosaicism for trisomy 9 at amniocentesis. The interphase FISH proved to be a very efficient method for confirmation of the status of mosaicism in the amniotic fluid sample prior to cul-ture. The QF-PCR assay requires both parental sam-ples and multiple polymorphic specific loci and shows
B A
Figure 3.Fluorescence in situ hybridization analysis of uncultured interphase amniocytes shows (A) three signals in a cell with
trisomy 9 and (B) two signals in a cell with disomy 9, consistent with the diagnosis of mosaic trisomy 9. 209 189 205 197 205 189 205 189 Father D9S941 Mother Amniotic fluid (uncultured) Amniotic fluid (cultured)
Figure 4. Representative electrophoretograms of
quantita-tive fluorescent polymerase chain reaction assays. The marker D9S941 shows two peaks (189 and 205 bp; paternal and maternal, respectively) of unequal fluorescent activity from two different parental alleles in uncultured amniocytes with a dosage ratio of 1:18 (paternal:maternal) and in cul-tured amniocytes with a dosage ratio of 1:36.
B A
limitations for the detection of a very low level of chro-mosomal mosaicism. Donaghue et al [15] suggested that the QF-PCR assay can detect mosaicism when the abnormal cell line comprises at least 15% of the whole sample. However, in this study, QF-PCR was able to detect the low-level mosaicism in uncultured and cultured amniocytes. aCGH can detect DNA dosage imbalances, including deletions and duplications, but shows limitations for the detection of low-level mo-saicism, balanced translocations, inversions and poly-ploidy. Recent studies have suggested that aCGH can detect mosaicism as low as 20% in peripheral blood cells [16,17]. In this study, aCGH was unable to detect the low-level mosaicism of 18% (9/50) mosaic trisomy 9 in the uncultured amniocytes.
To date, at least 37 cases of prenatally detected mosaic trisomy 9 have been reported (Table). Of these 37 cases, 24 (64.9%) were associated with phenotypic abnormalities, suggesting a high risk of malformation
in fetuses with prenatally detected mosaic trisomy 9. Among normal prenatal fetuses, the sex ratio is 1.07 (males/females). The Table shows that the sex ratio for fetal mosaic trisomy 9 is 0.21 (6/29), indicating a female preponderance in prenatally detected mosaic trisomy 9 and a prenatal selection against mosaic trisomy 9 males.
UPD can be observed together with a chromoso-mal aberration. Liehr [31] suggested that at least one-third of UPD cases are associated with or due to a chromosomal rearrangement. The phenotypic abnor-malities of our case are more likely due to low-level mosaic trisomy 9 rather than the phenotypic effect of maternal UPD 9, because there is no evidence for an imprinting locus on maternal chromosome 9 [31–33]. UPD 9 can be associated with major clinical conse-quences only when a recessive mutation is reduced to homozygosity [34–36]. Sulisalo et al [34] reported UPD 9 with cartilage-hair hypoplasia because of a homozy-gous deletion of the CHH gene. Tiranti et al [35] reported UPD 9 with Leigh syndrome because of a homozygous loss of function mutation of the SURF-1 gene. Castanet et al [36] reported maternal UPD 9 with syndromic congenital hypothyroidism because of homozygosity for a novel FOXE1 mutation.
Cases with maternal UPD 9 have been reported to be associated with confined placental mosaicism for trisomy 9, low-level level II mosaic trisomy 9, low-level mosaic trisomy 9, and mosaic supernumerary ring chromosome 9 [r(9)] [12–14, 37]. Wilkinson et al [13] reported maternal UPD 9 in a fetus with mosaic trisomy 9 at chorionic villus sampling. Slater et al [14] reported maternal UPD 9 in a fetus with trisomy 9 at chorionic villus sampling, level II mosaic trisomy 9 (2.8%, 2 of 71 cells) at amniocentesis, low-level mosaic trisomy 9 (2.9%, 3 of 102 cells) at cordocentesis, and low-level mosaic trisomy 9 (8%, 4 of 50 cells) at neona-tal blood sampling. The case was followed up to 1 year of age and had minor facial dysmorphism, skeletal ab-normalities and growth retardation. Willatt et al [12] reported maternal UPD 9 in a 17-year-old man with growth and mental retardation, facial dysmorphism, skeletal abnormalities, and low-level mosaic trisomy 9 (7%, 7 of 100 cells) in the blood. Anderlid et al [37] reported maternal UPD 9 in a 10-month-old girl described by Blennow et al [38] with psychomotor retardation, moderate mental retardation, speech dif-ficulties, no dysmorphic features, and a supernumer-ary r(9)(p10p12) in 36% of the lymphocytes. Björch et al [32] reported maternal isodisomy of UPD 9 in a 34-year-old woman with isochromosomes for the short and long arms of chromosome 9 without any clinical symptoms. 209 189 205 197 205 189 205 189 Father D9S941 Mother 205 189 205 189 205 189 205 189 Placenta Cord Lung Liver Skin Cord blood
Figure 6.Representative electrophoretograms of
quantita-tive fluorescent polymerase chain reaction assays. The marker D9S941 shows two peaks (189 and 205 bp; paternal and maternal) of unequal fluorescent activity from two dif-ferent parental alleles in the tissues of cord, lungs, liver, skin and cord blood with a dosage ratio of 1:6 (paternal:mater-nal) and in the placenta with a dosage ratio of 1:2.
T able. Repor ted cases of pr enat ally det ect ed mosaic trisomy 9 Author Cases Pr enat al diagnosis Conf irmator y studies
Outcome and phenotype
P olani et al [18] 47,XX, +9/46,XX Amniocent esis: T9 = NA Fet al tissue: mosaic T9 T OP , abnormal abor tus Gr eenber g et al [19] 47,XX, +9/46,XX Amniocent esis: T9 = 24% Blood: 46,XX (75 cells) Normal liveborn (58 cells) Amnion: 46,XX (75 cells) Pur vis-Smith et al [20] 47,XX, +9/46,XX Amniocent esis: T9 = NA NA T OP , abnormal abor tus facial dy smor phism, pulmonar y st enosis, ASD , bicornuat e ut erus, dy smor
phic hands and f
eet Pf eif fer et al [21] 47,XX, +9/46,XX Amniocent esis: T9 = 38% (47 cells) Blood: 46,XX (50 cells) T OP , normal abor tus
Skin: 46,XX (70 cells) Placent
a: 47,XX, +9 (50 cells) Zadeh et al [22] 47,XX, +9/46,XX Amniocent esis: T9 = 84% (21/25 cells) Skin: T9 = 26.3% (5/19 cells) T OP , f acial dy smor phism, ventriculomegaly , a single tr ansver se kidney Her ens et al [23] 47,XX, +mar/ Amniocent esis: T9 = 38.7% (12/31 cells), NA T OP , minor e xt ernal 47,XX, +9/46,XX SMC = 38.7% (12/31 cells) dy smor phism Fet al blood: T9 = 6% (3/50 cells), SMC = 68% (34/50 cells) Schwar tz et al [24] 47,XX, +9/46,XX Amniocent esis: T9 = 25% (13/52 cells) Hear t: T9 = 24% (50 cells) T OP , f acial dy smor phism PUBS: T9 = 1% (1/100 cells) Skin: T9 = 13% (32 cells) Repeat amniocent esis: T9 = 14% (14/100 cells) L ung: T9 = 22% (50 cells) Liver : 46,XX (31 cells) Bur eau et al [25] 47,XY ,+ 9/46,XY Ultr asound: DWM at 34 wk Blood: T9 = 30% Deliver y at 38 wk (2,510 g), Amniocent esis: T9 = 5 0 % facial dy smor phism, DWM, hydr
ocephalus, died at age
2w k Merino et al [26] Case 1 Mosaic T9 Ultr
asound: IUGR, a globular
NA T OP , f acial dy smor phism, stomach, micr or etr ognathia a dist ended stomach Amniocent esis: T9 = 65%
T able. (Continued ) Author Cases Pr enat al diagnosis Conf irmator y studies
Outcome and phenotype
Case 2 47,XY ,+ 9/46,XY Ultr asound: IUGR Skin: T9 = 17% (17/100 cells) T OP , dolichocephaly , f acial Amniocent esis: T9 = 12% (12/100 cells) L ung: T9 = 14% (14/100 cells) dy smor phism, bilat er al
PUBS: 46,XY (100 cells)
hydr onephr osis, glomerulocy stic kidney s Gr oss et al [27] 47,XX, +9/46,XX Amniocent esis: T9 = NA NA T OP , abnormal abor tus, unilat er al chor oid ple xus cy st, two-vessel cord, micr ognathia, renal dy splasia Saur a et al [28] Case 1 47,XX, +9/46,XX CV S: 47,XX, +9 Skin: T9 = 16. 1% (9/56 cells) T OP , no e xt ernal Amniocent esis: T9 = 64% (25 cells) dy smor phic f eatur es PUBS: 46,XX (100 cells) Case 3 47,XX, +9/46,XX CV S: 47,XX, +9 NA T OP , f acial dy smor phism, Amniocent esis: T9 = 50% (25/50 cells) PD A , hor seshoe kidney PUBS: T9 = 3% (3/100 cells) Case 4 47,XY ,+ 9/46,XY Ultr asound: PD A , polyhydr amnios Blood: 46,XY Deliver y at 35 wk (1 ,500 g), PUBS: T9 = 9% (9/100 cells) Skin: 46,XY facial dy smor phism, PD A Case 6 47,XX, +9/46,XX Ultr asound: IUGR Blood: T9 = 6% (6/100 cells) Deliver y at t erm (2,000 g), PUBS: T9 = 2% (2/100 cells) Skin: 46,XX (100 cells) no dy smor phism except hip dislocation, development al delay at age 21 mo Hsu et al [8] Case IX-1 47,XX, +9/46,XX Amniocent esis: T9 = 28% (25 cells) Skin: T9 = 12. 1% (7/58 cells) T OP , normal abor tus Case IX-2 47,XX, +9/46,XX Amniocent esis: T9 = 83.9% (31 colonies) NA
Normal liveborn, normal
PUBS: 46,XX (100 cells) at age 3 yr 8 mo Case IX-3 Mosaic T9 Amniocent esis: NA NA T OP , abnormal abor tus Case IX-4 47,XX, +9/46,XX Amniocent esis: T9 = 50% (48 cells) Placent a: T9 = 80% (8/10 cells) T OP , abnormal abor tus Fet al tissue: T9 = 38.9% (7/18 cells)
Case IX-5 47,XX, +9/46,XX Amniocent esis: T9 = 86.6% (30 cells) Fet al tissue: 47,XX, +9 (5 cells) T OP , abnormal abor tus, facial dy smor phism, IUGR, ambiguous e xt ernal genit alia Case IX-8 47,XY ,+ 9/46,XY Amniocent esis: T9 = 30.4% (23 colonies) Cord blood: T9 = 10% (3/30 cells) Normal f
etus, died at age 4
d Placent a: 47,XXY ,+ 9 (10 cells) af ter pr ematur e bir th Case IX-9 47,XX, +9/46,XX Amniocent esis: T9 = 8.3% (155 cells) Skin: 46,XX (50 cells) T OP , normal abor tus L ung: 46,XX (50 cells) Case IX-10 47,XX, +9/46,XX Amniocent esis: T9 = 42% (40 cells) NA T O P , abnormal abor tus, multiple congenit al anomalies Case IX-11 47,XX, +9/46,XX Amniocent esis: T9 = 10% (39 cells) Fet al tissue: 46,XX T OP , normal abor tus Case IX-13 47,XX, +9/46,XX Amniocent esis: T9 = 25% (32 colonies)
Skin and kidney
: T OP , abnormal abor tus, T9 = 40% (8/20 cells)
abnormal right big toe
Case IX-14 47,XY ,+ 9/46,XY Amniocent esis: T9 = 80% (15 colonies) Kidney : T9 = 16% (4/25 cells) T OP , normal abor tus Villi: T9 = 28% Amnion: T9 = 33% Chorion: T9 = 34% Case IX-15 47,XX, +9/46,XX Amniocent esis: T9 = 15% (70 cells) Blood: T9 = 16.7% (4/24 cells)
Abnormal liveborn, IUGR,
Skin: 46,XX (20 cells) multiple congenit al anomalies, f acial dy smor phism Case IX-16 47,XX, +9/46,XX Amniocent esis: T9 = 12% (68 cells) NA T OP , abnormal abor tus, facial dy smor phism, thick neck , bilat er al tibia tor sion Case IX-21 47,XX, +9/46,XX Amniocent esis: T9 = 58.6% (29 cells) NA T OP , abnormal abor tus, ASD , pulmonar y st enosis Case IX-22 47,XX, +9/46,XX Amniocent esis: T9 = 42% (40 cells) NA T OP , normal abor tus Case IX-23 47,XX, +9/46,XX Amniocent esis: T9 = 7% (59 cells) NA T OP , normal abor tus Case IX-24 47,XY ,+ 9/46,XY Amniocent esis: T9 = 40% (59 cells)
Skin: 46,XY (50 cells)
T OP , normal abor tus Slat er et al [14] 47,XX, +9/46,XX CV S: 47,XX, +9 Neonat al blood: T9 = 8% Deliver y at 38 wk (2,480 g), Amniocent esis: 47,XX, +9 (13 colonies), (4/50 cells) facial dy smor phism, gr owth T9 = 2.8% (2/71 cells) (subcultur e) ret
ardation and skelet
al PUBS: T9 = 2.9% (3/102 cells) abnormalities at age 1 yr
T able. (Continued ) Author Cases Pr enat al diagnosis Conf irmator y studies
Outcome and phenotype
T seng et al [29] 47,XX, +9/46,XX Ultr asound: dolichocephaly , agenesis Cord blood: T9 = 22.5% T OP , facial dy smor phism, of lef t kidney , oligohydr amnios, an (9/40 cells) hydr ocephalus, agenesis intr ahepatic cy
st, varix of the por
tal vein of lef t kidney , single Amniocent esis: T9 = 77 .6% (38/49 cells) umbilical ar ter y, mar ked dilat ed por tal vein Chen et al [10] 47,XX, +9/46,XX Amniocent esis: T9 = 75% (27/36 colonies) Amnion: 46,XX (40 cells) T OP , f acial dy smor phism Placent a: 46,XX (40 cells) Cord: T9 = 20% (8/40 cells) Liver : T9 = 35% (14/40 cells) L ung: T9 = 67 .5% (27/40 cells) Skin: T9 = 5% (2/40 cells) Stipoljev et al [30] 47,XX, +9/46,XX Ultr asound: bilat er al hydr onephr osis, NA T OP , f acial dy smor phism, shor t f emur , oligohydr amnios, hydr onephr osis, thr ee placent al cy sts kidney s, bicornuat e ut erus CV S: T9 = 31% PUBS: T9 = 6% (3/50 cells) Pr esent case 47,XX, +9/46,XX 1 stamniocent esis: T9 (1 st)= 33.3% Cord blood: T9 = 11% (11/100 cells) T OP , ventriculomegaly , (3/9 colonies), 2 nd amniocent esis: Skin: T9 = 5% (2/40 cells) facial dy smor phism T9 = 24% (6/25 colonies), 3 rd L ung: T9 = 2.5% (1/40 cells) amniocent esis: T9 = 8.3% (2/24 colonies), Liver : T9 = 22.5% (9/40 cells) Uncultur ed amniocyt es: T9 = 18% Cord: T9 = 10% (4/40 cells) (9/50 cells), int er phase FISH Amnion: T9 = 17 .5% (7/40 cells) Placent a: 47,XX, +9 (40 cells) T9 = trisom y 9; TOP =
termination of pregnancy; mar
= marker; SMC = supernumer ar y marker chromosome; NA = no t av ailable; D W M = Dandy-W alker malformation; CVS =
chorionic villus sam
pling; PUBS = percutaneous umbilical blood sam pling; IUGR = intr
auterine growth restriction; PD
A = patent ductus ar teriosus; ASD = atrial sep
tal defect; FISH
=
fluorescence in situ h
In summary, there is a female preponderance in pre-natally detected mosaic trisomy 9, and mosaic trisomy 9 can be associated with maternal UPD 9 in euploid cell lines. Mosaic trisomy 9 at amniocentesis carries a high risk of fetal abnormalities and should include detailed sonographic investigation of congenital mal-formations. aCGH shows limitations for the detection low-level mosaicism, whereas interphase FISH and QF-PCR are useful to confirm the status of mosaicism in the uncultured amniocytes.
Acknowledgments
This work was supported by research grants NSC-96-2314-B-195-008-MY3 and NSC-97-2314-B-195-006-MY3 from the National Science Council, and MMH-E-99004 from Mackay Memorial Hospital, Taipei, Taiwan.
References
1. Chen CP, Chern SR, Tsai FJ, Lin HH, Pan CW, Wang W.
Prenatal diagnosis and molecular analysis of trisomy 13 mosaicism. Taiwan J Obstet Gynecol 2009;48:321–2.
2. Chen CP, Chern SR, Tsai FJ, Wu PC, Lee CC, Wang W. Trisomy
13 mosaicism associated with cyclopia and cystic hygroma. Taiwan J Obstet Gynecol 2009;48:434–6.
3. Chen CP. Prenatal diagnosis and genetic counseling for
mosaic trisomy 13. Taiwan J Obstet Gynecol 2010;49:13–22.
4. Schinzel A. Trisomy 8 and trisomy 9 are distinctly different
clinical entities. Am J Med Genet 1993;46:603–4.
5. Arnold GL, Kirby RS, Stern TP, Sawyer JR. Trisomy 9: review
and report of two new cases. Am J Med Genet 1995;56:252–7.
6. Wooldridge J, Zunich J. Trisomy 9 syndrome: report of a
case with Crohn disease and review of the literature. Am J Med Genet 1995;56:258–64.
7. Cantú ES, Eicher DJ, Pai GS, Donahue CJ, Harley RA.
Mosaic vs. nonmosaic trisomy 9: report of a liveborn infant evaluated by fluorescence in situ hybridization and review of the literature. Am J Med Genet 1996;62:330–5.
8. Hsu LYF, Yu MT, Neu RL, et al. Rare trisomy mosaicism
diag-nosed in amniocytes, involving an autosome other than chromosomes 13, 18, 20, and 21: karyotype/phenotype cor-relations. Prenat Diagn 1997;17:201–42.
9. Saneto RP, Applegate KE, Frankel DG. Atypical
manifesta-tions of two cases of trisomy 9 syndrome: rethinking devel-opment delay. Am J Med Genet 1998;80:42–5.
10. Chen CP, Chern SR, Town DD, Wang W, Liao YW. Fetopla-cental and fetoamniotic chromosomal discrepancies in prena-tally detected mosaic trisomy 9. Prenat Diagn 2003;23:1019–21. 11. Chen CP, Chern SR, Cheng SJ, et al. Second-trimester diag-nosis of complete trisomy 9 associated with abnormal maternal serum screen results, open sacral spina bifida and congenital diaphragmatic hernia, and review of the litera-ture. Prenat Diagn 2004;24:455–62.
12. Willatt LR, Davison BC, Goudie D, Alexander J, Dyson HM, Jenks PE, Ferguson-Smith ME. A male with trisomy 9 mo-saicism and maternal uniparental disomy for chromosome 9 in the euploid cell line. J Med Genet 1992;29:742–4. 13. Wilkinson TA, James RS, Crolla JA, Cockwell AE, Campbell PL,
Temple IK. A case of maternal uniparental disomy of chro-mosome 9 in association with confined placental mosaicism for trisomy 9. Prenat Diagn 1996;16:371–4.
14. Slater HR, Ralph A, Daniel A, Worthington S, Roberts C. A case of maternal uniparental disomy of chromosome 9 diagnosed prenatally and the related problem of residual trisomy. Prenat Diagn 2000;20:930–2.
15. Donaghue C, Mann K Docherry Z, Ogilvie CM. Detection of mosaicism for primary trisomies in prenatal samples by QF-PCR and karyotype analysis. Prenat Diagn 2005;25: 65–72.
16. Ballif BC, Rorem EA, Sundin K, et al. Detection of low-level mosaicism by array CGH in routine diagnostic specimens. Am J Med Genet 2006;140A:2757–67.
17. Shaffer LG, Kashork CD, Saleki R, Rorem E, Sundin K, Ballif BC, Bejjani BA. Targeted genomic microarray analysis for identification of chromosome abnormalities in 1500 con-secutive clinical cases. J Pediatr 2006;149:98–102.
18. Polani PE, Alberman E, Alexander BJ, et al. Sixteen years of experience of counseling, diagnosis and prenatal detection in one genetic center: progress, results and problems. J Med Genet 1979;16:166–75.
19. Greenberg F, Elsas NT, Reidy JA, Chen ATL, Stone LB. Autosomal mosaicism in amniotic fluid cells from a twin pregnancy. Am J Med Genet 1982;11:109–12.
20. Purvis-Smith AG, Saville T, Osborn RA. Prenatal diagnosis of trisomy 9 mosaicism. Pathology 1983;15:109.
21. Pfeiffer RA, Ulmer R, Kniewald A, Wagner-Thiessen E. Prena-tal diagnosis of trisomy 9 mosaicism possibly limited to fetal membranes. Prenat Diagn 1984;4:387–9.
22. Zadeh TM, Peters J, Sandlin C. Prenatal diagnosis of mosaic trisomy 9. Prenat Diagn 1987;7:67–70.
23. Herens C, Pierquin G, Verloes A, Schaaps JP, Frederic J. Mosaicism of 46,XX/47,XX,+9/47,XX,+?mar in the same amniotic fluid with apparent loss of one cell line after delivery. Prenat Diagn 1989;9:373–5.
24. Schwartz S, Ashai S, Meijboom EJ, Schwartz MF, Sun CC, Cohen MM. Prenatal detection of trisomy 9 mosaicism. Prenat Diagn 1989;9:549–54.
25. Bureau Y-A, Fraser W, Fouquet B. Prenatal diagnosis of trisomy 9 mosaic presenting as a case of Dandy-Walker malformation. Prenat Diagn 1993;13:79–85.
26. Merino A, De Perdigo A, Nombalais F, Yvinec M, Le Roux MG, Bellec V. Prenatal diagnosis of trisomy 9 mosaicism: two new cases. Prenat Diagn 1993;13:1001–7.
27. Gross SJ, Shulman LP, Tolley EA, Emerson DS, Felker RE, Simpson JL, Elias S. Isolated fetal choroid plexus cysts and trisomy 18: a review and meta-analysis. Am J Obstet Gynecol 1995;172:83–7.
28. Saura R, Traore W, Taine L, et al. Prenatal diagnosis of tri-somy 9. Six cases and a review of the literature. Prenat Diagn 1995;15:609–14.
29. Tseng JJ, Chou MM, Ho ESC. Varix of the portal vein: pre-natal diagnosis in a fetus with mosaic trisomy 9 syndrome. Prenat Diagn 2002;22:495–7.
30. Stipoljev F, Kos M, Kos M, Miskovi B, Matijevic R, Hafner T, Kurjak A. Antenatal detection of mosaic trisomy 9 by ultra-sound: a case report and literature review. J Matern Fetal Neonatal Med 2003;14:65–9.
31. Liehr T. Cytogenetic contribution to uniparental disomy (UPD). Mol Cytogenet 2010;3:8.
32. Björck EJ, Anderlid BM, Blennow E. Maternal isodisomy of chromosome 9 with no impact on the phenotype in a woman with two isochromosomes: i(9p) and i(9q). Am J Med Genet 1999;87:49–52.
33. Kotzot D, Utermann G. Uniparental disomy (UPD) other than 15: Phenotypes and bibliography updated. Am J Med Genet 2005;136A:287–305.
34. Sulisalo T, Mäkitie O, Sistonen P, et al. Uniparental disomy in cartilage-hair hypoplasia. Eur J Hum Genet 1997;5:35–42.
35. Tiranti V, Lamantea E, Uziel G, et al. Leigh syndrome trans-mitted by uniparental disomy of chromosome 9. J Med Genet 1999;36:927–8.
36. Castanet M, Mallya U, Agostini M, et al. Maternal isodis-omy for chromosome 9 causing homozygosity for a novel FOXE1 mutation in syndromic congenital hypothyroidism.
J Clin Endocrinol Metab 2010;98:4031–6.
37. Anderlid B-M, Sahlén S, Schoumans J, et al. Detailed char-acterization of 12 supernumerary ring chromosomes using micro-FISH and search for uniparental disomy. Am J Med Genet 2001;99:223–33.
38. Blennow E, Anneren G, Bui T-H, Berggren E, Asadi E, Nordenskjöld M. Characterization of supernumerary ring marker chromosomes by fluorescence in situ hybridization (FISH). Am J Hum Genet 1993;53:433–42.