Community-based Epidemiological Study of Impaired Activities of Daily Living in Older People
6
0
0
全文
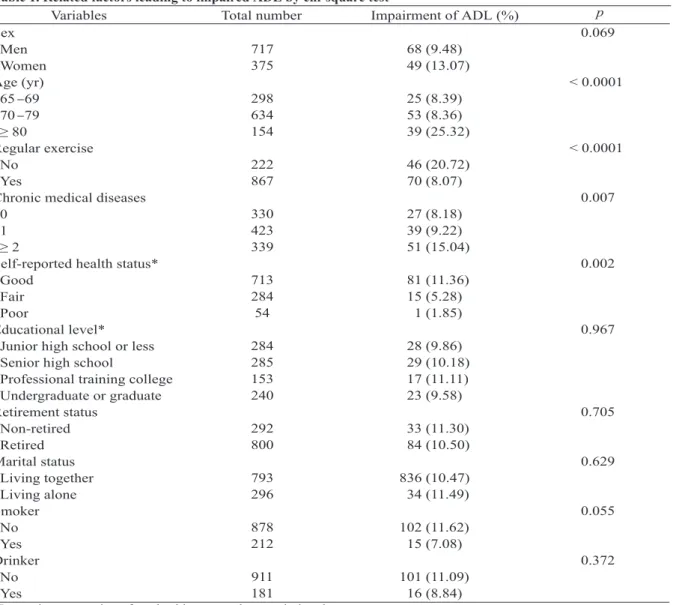
(2) 166. Activities of Daily Living in Older People. Table 1. Related factors leading to impaired ADL by chi-square test Variables Total number Impairment of ADL (%) Sex 717 68 (9.48) Men 375 49 (13.07) Women Age (yr) 298 25 (8.39) 65 69 634 53 (8.36) 70 79 154 39 (25.32) ≥ 80 Regular exercise 222 46 (20.72) No 867 70 (8.07) Yes Chronic medical diseases 330 27 (8.18) 0 423 39 (9.22) 1 339 51 (15.04) ≥2 Self-reported health status* 713 81 (11.36) Good 284 15 (5.28) Fair 54 1 (1.85) Poor Educational level* 284 28 (9.86) Junior high school or less 285 29 (10.18) Senior high school 153 17 (11.11) Professional training college 240 23 (9.58) Undergraduate or graduate Retirement status 292 33 (11.30) Non-retired 800 84 (10.50) Retired Marital status 793 836 (10.47) Living together 296 34 (11.49) Living alone Smoker 878 102 (11.62) No 212 15 (7.08) Yes Drinker 911 101 (11.09) No 181 16 (8.84) Yes *Imprecise summation of total subjects was due to missing data.. to the preservation of ADL [8,11-15]. In addition, older people with impaired ADL always indicate that long term care is needed. This issue has become a challenging problem for public health policy makers [5-7,16]. In order to explore the prevalence of impaired ADL and to identify the potential determinants that might be helpful for our country to develop effective public health strategies to intervene in this issue, we conducted a comprehensive health survey in older people living at Chung-Hsing Village in Taiwan. MATERIALS AND METHODS. In May 1998, a community-based, cross-. p 0.069. < 0.0001. < 0.0001. 0.007. 0.002. 0.967. 0.705. 0.629. 0.055. 0.372. sectional study was conducted at Chung-Hsing Village located in central Taiwan. All individuals aged 65 and over (n = 1774) were eligible for this study. A total of 1092 subjects participated in this study. The response rate was 61.6%. Information about each subject's medical condition, sociodemographic characteristics, lifestyle patterns and health-related behaviors was collected by welltrained interviewers via face-to-face interviews. Self reported health status was classified as good, fair and poor. If subjects exercised regularly, their status was classified as exercise. If not, their status was defined as no exercise. Subjects who never smoked or quit smoking were defined as nonsmokers. Subjects who currently smoke were.
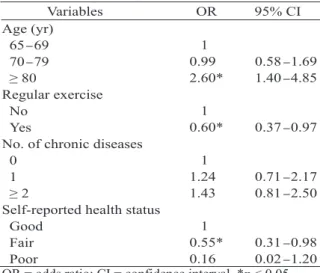
(3) Tsai-Chung Li, et al.. Table 2. Related factors leading to impaired ADL by multivariate logistic regression Variables OR 95% CI Age (yr) 1 65 69 0.99 0.58 1.69 70 79 1.40 4.85 2.60* ≥ 80 Regular exercise 1 No 0.37 0.97 0.60* Yes No. of chronic diseases 1 0 0.71 2.17 1.24 1 0.81 2.50 1.43 ≥2 Self-reported health status 1 Good 0.31 0.98 0.55* Fair 0.02 1.20 0.16 Poor OR = odds ratio; CI = confidence interval. *p < 0.05.. defined as smokers. Subjects who never drink alcohol or drink alcohol occasionally were classified as nondrinkers. Subjects who reported drinking alcohol often were classified as habitual drinkers. The educational levels were classified as junior high school or less, senior high school, professional training college, and undergraduate or graduate. If the subject was retired, the status was classified as retired. If the subject lived with a spouse or other family members, the marital status was defined as living together. If not, the marital status was defined as living alone. ADL included the following items: bathing, dressing, taking care of personal appearance, ability to walk, ability to get in and out of bed, toileting and eating [9,10]. Impaired ADL was defined as needing help with at least one of these seven items. Chronic diseases, including cataracts, cancer, cardiovascular disease, stroke, Parkinson's disease, osteoporosis, hypertension, and diabetes mellitus, were recorded by history taking. The statistical analyses were performed by the aid of an SAS package (Version 6.12, SAS Institute Inc., Cary, North Carolina). The chisquare test identified the factors that might be associated with impaired ADL in this study population. Multivariate logistic regression of the factors identified by the chi-square test as having a significant association was conducted. A p. 167. value less than 0.05 was considered statistically significant. RESULTS. Among the1092 subjects, 65.66% were men and 34.34% were women. The mean age was 73.4 years (standard deviation = 5.6). The factors related to impaired ADL according to chi-square test are displayed in Table 1. The prevalence of impaired ADL was 10.71%. Only age, regular exercise, chronic medical diseases, and self-reported health status were statistically associated with impaired ADL. The factors related to impaired ADL by multivariate logistic regression are listed in Table 2. After controlling for the covariates, with the age group 65 to 69 as a reference, odds ratio (OR) for the risk of impaired ADL was considerably higher in people ≥ 80 years (OR = 2.60, 95% confidence interval (CI) = 1.40 to 4.85, p < 0.05). With no regular exercise as a reference, odds ratio for the risk of impaired ADL was considerably lower in people who regularly exercised (OR = 0.60, 95% CI = 0.37 to 0.97, p < 0.05). With good self-reported health status as a reference, the odds ratio for the risk of developing impaired ADL was considerably lower in people with fair selfreported health status (OR = 0.55, 95% CI = 0.31 to 0.98, p < 0.05). The number of chronic medical diseases was not related to the risk of developing impaired ADL. DISCUSSION. With the progressive aging of the population, functional impairment has become a critically serious challenge to health care delivery systems. Our study identified that the prevalence of impaired ADL was 10.71%. In Hebert and colleagues' study, the incidence of functional decline was 11.9% [17]. In Wu and colleagues' study [7], 11.0% of participants developed impaired ADL during a three year observation period. Because of the different items of ADL surveyed, the different environmental factors and the different races, it is relatively difficult to gauge the reason for the variation between studies. Our study elicited that increasing age was a.
(4) 168. statistically significant factor of developing impaired ADL, which was similar to previous studies [7,18,19]. That is, the older people become, the lower their functional status level becomes. Strawbridge et al [18] suggested that age-related declines in functional status in older people are deeply complex and heterogeneous. This study also exhibited that lack of regular exercise was a significantly related factor of developing impaired ADL, a finding consistent with previous studies [7,20-22]. Stessman and colleagues suggested that older people should be encouraged to engage in regular physical activity to increase survival [22]. We also observed that co-existing chronic medical diseases was not a related factor of developing impaired ADL. However, our result was not consistent with previous studies [19,2326]. We found that people with good selfreported health status were more likely to develop impaired ADL than people with fair self-reported health status. In Beck and colleagues' study [27], no difference was observed between groups in self-reported health and functional status. However, other studies have disclosed that people with good self-reported health status performed well in ADL [28,29]. To date, there is no evidence to support our result. Limitation. Although information was collected by well-trained interviewers via face-to-face interviews, if subjects refused, we could not interview them. Therefore, the subjects in this study were volunteers. That was why the response rate was only 61.6%. Furthermore, most people living in Chung-Hsing Village moved to Taiwan from Mainland China after the civil war during their military service. Because most of them were men, the proportion of men in this sample was higher than that of women. In conclusion, increasing age and lack of regular exercise are significantly related factors of developing impaired ADL in older people.. Activities of Daily Living in Older People. REFERENCES. 1. National Health Administration, Taiwan: Health statistics: I. Vital statistics. 1971-1996. 2. D e pa rtme nt of H e a lth, Ta iw a n: http://w ww. doh.gov.tw/english/901123/Health/II/II-2.doc (Accessed April 2005). 3. Main Causes of Death of the Elderly in Taiwan in 2002, Department of Health, Taiwan: http://www.doh. gov.tw/ufile/Doc/S02/9109-eng.xls (Accessed April 2005). 4. Posner BM, Fanelli MT, Krackenfels MM. Position of the American Dietetic Association:nutrition, aging, and the continuum of health care. J Am Diet Assoc 1987; 87:344-7. 5. Lau SC, Lee LL, Lin BJ, et al. The health status of rural and urban ambulatory elderly in Taipei County. Chang Gung Med J 2001;24:492-501. 6. Wu SC, Hsu HC, Chuang YC, et al. Application of functional assessment in estimating long-term care need among non-institutionalized elderly adults in Taiwan. Chinese Public Health (Taipei) 1996;15:53345. 7. Wu SC, Leu SY, Li CY. Incidence of and predictors for chronic disability in activities of daily living among older people in Taiwan. J Am Geriatr Soc 1999;47: 1082-6. 8. Ensrud KE, Nevitt MC, Yunis C, et al. Correlates of impaired function in older women. J Am Geriatr Soc 1994;42:481-9. 9. Katz S, Ford AB, Moskowitz RW, et al. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA 1963;185:914-9. 10. Hsiao SH, Chiu HC, Liu HW. A replication of multidimensionality of activities of daily living (ADL): on the elderly in southern Taiwan. Kaohsiung J Med Sci 1994;10:449-57. (In Chinese; English abstract) 11. Frederiks CM, te Wierik MJ, Visser AP, et al. The functional status and utilization of care of elderly people living at home. J Community Health 1990;15: 307-17. 12. Wachtel TJ, Derby C, Fulton JP. Predicting the outcome of hospitalization for elderly persons: home versus nursing home. South Med J 1984;77:12835,1290. 13. Narain P, Rubenstein LZ, Wieland GD, et al. Predictors of immediate and 6-month outcomes in.
(5) Tsai-Chung Li, et al.. hospitalized elderly patients. The importance of functional status. J Am Geriatr Soc 1988;36:775-83. 14. Fillenbaum GG. Screening the elderly. A brief instrumental activities of daily living measure. J Am Geriatr Soc 1985;33:698-706. 15. Desai MM, Lentzner HR, Weeks JD. Unmet need for personal assistance with activities of daily living among older adults. Gerontologist 2001;41:82-8. 16. Li TC, Lai MC, Yang WH, et al. Cost analysis of nursing homes. Mid Taiwan J Med 2001;6:223-32. 17. Hebert R, Brayne C, Spiegelhalter D. Incidence of functional decline and improvement in a communitydwelling, very elderly population. Am J Epidemiol 1997;145:935-44. 18. Strawbridge WJ, Kaplan GA, Camacho T, et al. The dynamics of disability and functional change in an elderly cohort: results from the Alameda County Study. J Am Geriatr Soc 1992;40:799-806. 19.Guralnik JM, LaCroix AZ, Abbott RD, et al. Maintaining mobility in late life. I. Demographic characteristics and chronic conditions. Am J Epidemiol 1993;137:845-57. 20.LaCroix AZ, Guralnik JM, Berkman LF, et al. Maintaining mobility in late life. II. Smoking, alcohol consumption, physical activity, and body mass index. Am J Epidemiol 1993;137:858-69. 21. Kaplan GA, Strawbridge WJ, Cohen RD, et al. Natural history of leisure-time physical activity and its correlates: associations with mortality from all causes. 169. and cardiovascular disease over 28 years. Am J Epidemiol 1996;144:793-7. 22. Stessman J, Maaravi Y, Hammerman-Rozenberg R, et al. The effects of physical activity on mortality in the Jerusalem 70-year-olds longitudinal study. J Am Geriatr Soc 2000;48:499-504. 23. Fu LL, Yang JF. Health status and physical function of long term care facility elderly. J Phys Ther Assoc (Taiwan) 1998;23:194-201. 24. Tseng IL, Lee SH, Lee MC. Comparative studies on the health status between the elderly in rural and urban areas. Chung Shan Med J 1995;6:65-87. 25. Patrick L, Knoefel F, Gaskowski P, et al. Medical comorbidity and rehabilitation efficiency in geriatric inpatients. J Am Geriatr Soc 2001;49:1471-7. 26. Kaplan GA. Maintenance of functioning in the elderly. Ann Epidemiol 1992;2:823-34. 27. Beck A, Scott J, Williams P, et al. A randomized trial of group outpatient visits for chronically ill older HMO members: the Cooperative Health Care Clinic. J Am Geriatr Soc 1997;45:543-9. 28. Szczerbinska K, Hubalewska A. The health status of the long lived elderly in Cracow. Przegl Lek 2004;61: 1360-8. (In Polish; English abstract) 29. Reddy KK, Reddy BK, Rao AP. Interaction among body composition, self-rated health and functional status of the elderly in an Indian population. Asia Pac J Clin Nutr 2004;13:78-85..
(6) 170. 1. 1. 2. 1. 1998. 5. 1774. 2. 65. 1092. 61.6%. 65.66%. 34.34%. 73.4. 5.6. 10.71% 80. 65-69. (95%. 1.40-4.85) 0.60. (95%. 0.37-0.97). 2005;10:165-70. 404. 2. 2005. 4. 27. 2005. 8. 22. 2005. 8. 1. 2.60.
(7)
數據
相關文件
“People should know what kinds of foods are good for health.” To live a healthier life, we should read what our foods are made of by reading the ingredient lists on food cans
Predicting Successful Employment in the Community for People with a History of Chronic Mental Illness.Occupational Therapy Mental Health,6,31-49. Predictors of employment outcome
Employment of Foreign Workers, overseas Chinese students shall meet the student status regulated in the Regulations on Study and Counseling Assistance in Taiwan for
6 《中論·觀因緣品》,《佛藏要籍選刊》第 9 冊,上海古籍出版社 1994 年版,第 1
Reading Task 6: Genre Structure and Language Features. • Now let’s look at how language features (e.g. sentence patterns) are connected to the structure
Research findings from the 1980s and 90s reported that people who drank coffee had a higher risk of heart disease.. Coffee also has been associated with an increased risk of
The elderly health centres provide people aged 65 or above with comprehensive primary healthcare services which include health assessments, physical check-ups, counselling,
Topic 4 - Promotion and Maintenance of Health and Social Care in the Community 4CAspects of risk assessment and
