Characteristics of Traditional Chinese Medicine Use for Children with Allergic Rhinitis: A Nationwide Population-based Study
Authors
Hung-Rong Yen1,2,3,4, Kai-Li Liang6,7,8, Tzu-Ping Huang1, Ji-Yu Fan1,2, Tung-Ti Chang2,4,5, Mao-Feng Sun2,3,4
Affiliations
1Research Center for Traditional Chinese Medicine, 2Department of Chinese Medicine, China Medical University Hospital, Taichung, Taiwan
Address: 2 Yude Rd, North District, Taichung 404, Taiwan
3Research Center for Chinese Medicine & Acupuncture, 4School of Chinese Medicine, 5School of Post-baccalaureate Chinese Medicine, China Medical University, Taichung, Taiwan
Address: 91 Hsueh-Shih Road, North District, Taichung 404, Taiwan
6Department of Otolaryngology, Taichung Veterans General Hospital, Taichung, Taiwan
Address: 1650 Taiwan Boulevard Sect. 4, Taichung 407, Taiwan
7Department of Medicine, National Yang-Ming Medical University, Taipei, Taiwan; Address: 155, Sec.2, Linong Street, Taipei 112, Taiwan
8School of Medicine, Chung Shan Medical University, Taichung, Taiwan Address: 110,Sec.1,Jianguo N. Road, Taichung 402,Taiwan
Email:
Hung-Rong Yen: [email protected] Kai-Li Liang: [email protected] Tzu-Ping Huang: [email protected] Ji-Yu Fan: [email protected]
Tung-Ti Chang: [email protected] Mao-Feng Sun: [email protected]
Corresponding Author: Mao-Feng Sun, M.D., Ph.D.
Department of Chinese Medicine, China Medical University Hospital 2 Yude Rd, North District, Taichung 404, Taiwan
Tel.: +886-4-22052121 ext. 1675 Fax: 04-22365141
E-mail: [email protected]
Abstract
Objectives: Allergic rhinitis (AR) is a common allergic disorder in children, some of whom seek complementary treatments, including acupuncture and Chinese herbs. Little, however, is known about the treatment of pediatric AR with traditional Chinese medicine (TCM). To characterize TCM use in pediatric AR, we conducted a nationwide population-based study.
Methods: We screened one million randomly sampled beneficiaries of the National Health Insurance Program in Taiwan from 2002 to 2010 to identify children <18 years of age with newly diagnosed allergic rhinitis (ICD-9 code 477.9). The subjects were categorized according to their use of TCM.
Results: We identified 97,401 children newly diagnosed with AR for inclusion in the study. Among these children, 63.11% (N=61,472) had used TCM. There were significantly more TCM users than non-users among school-age children and adolescents (P<0.001). Most (99.1%) pediatric TCM users received Chinese herbal remedies (99.1%); only 0.9% received acupuncture or manipulative therapies. Xin-yi-qing-fei-tang (Magnolia Flower Lung-Clearing Decoction) was the most frequently prescribed TCM formulation (23.44%), and the most commonly prescribed single herb was Chan-Tui (Periostracum cicadae; 13.78%). Regarding syndrome differentiation (ZHENG) according to TCM theory, prescriptions for the Cold Syndrome exceeded those for the Hot Syndrome throughout the year in Taiwan.
Conclusions: We found that approximately two thirds of pediatric AR patients were prescribed TCM treatments in Taiwan. Further research is warranted to examine the efficacy and safety of TCM for pediatric AR patients.
Keywords: acupuncture; allergic rhinitis; complementary and alternative medicine; pediatrics; traditional Chinese medicine
INTRODUCTION
Allergic rhinitis (AR) is a global problem affecting 400 million people worldwide that usually develops early in childhood [1]. In 2002, the prevalence of pediatric AR in central Taiwan, as established by the International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire, was 27.59% [2]. The cumulative 12-month prevalence in a 2005 ISAAC study of 10- to 12-year-old children in central Taiwan was even higher, at 43% [3]. Comorbidities such as asthma are common in children with AR, supporting the view that the upper and lower airways are united in their functions [4]. The increasing prevalence of allergic rhinitis and its impact on asthma create a significant burden, not only in Taiwan but also worldwide [5].
Many children with allergic disorders seek help from complementary and alternative medicine (CAM) [6]. The current mainstay treatments for pediatric AR include oral antihistamines and nasal corticosteroids [1, 7]. Clinical evidence for efficacy of sublingual immunotherapy in children is also growing [8]. However, some patients experience poor control or are concerned about the side effects of these conventional treatments [9]. Several large-scale studies, including the ISAAC study [10] and the National Health Interview Survey (NHIS) [11], the Allergies, Immunotherapy, and Rhinoconjunctivitis (AIRS) survey [12] in the United States, have addressed pediatric AR issues, but comprehensive information regarding the use of traditional Chinese medicine (TCM) for pediatric AR has been lacking. Our previous questionnaire-based survey found that 34.4% of patients with rhinitis had used TCM [13]. In Taiwan, Japan, Korea and China, TCM is popular and is regarded as both an alternative and a mainstay therapy for some diseases [14]. We previously found in a population-based
epidemiological study that a very high percentage (57.95%) of children with asthma used TCM [15]. Our recent nationwide study also found that AR was one of the four most common diseases for which children in Taiwan visited TCM clinics [16].
Descriptions of allergic rhinitis symptoms have been reported in the ancient Chinese literatures, and there are a number of classic formulae used in the TCM practice. From a TCM standpoint, allergic rhinitis is as a result of pernicious external pathogenic processes invading the lungs and affecting Qi of the lung, spleen and kidney. According to the Western medicine, these allergic rhinitis patients are considered to have the same disease, whereas in the view of TCM, they could be further categorized into two subtypes (TCM Syndromes; “ZHENG” in Chinese), the Cold Syndrome and the Hot Syndrome in the acute stage, based on an overall medical examination of symptoms [17]. Those with the Cold Syndrome present with a watery running nose, cold extremities, and a pale tongue, while those who with Hot Syndrome present with more or less sticky yellowish nasal discharge, thirst, and an erythematous tongue. TCM doctors prescribe different herbal formulas for the Hot and Cold syndromes. AR patients in remission stages received consolidation treatment for the tonification of Qi. Therefore, the prescriptions for allergic rhinitis patients are difficult to standardize as a monotherapy. In light of the large pediatric population using TCM for allergic rhinitis [16], it is necessary to conduct a large-scale, population-based, pharmaco-epidemiologic analysis to investigate the characteristics and potential use of TCM for pediatric allergic rhinitis patients.
since 1996. TCM is frequently used in Taiwan and is regarded as one of the mainstream therapies. In Taiwan, many of the public hospitals and university-affiliated teaching hospitals have TCM clinics. Taiwan installed TCM programs in higher education and has a pioneering TCM education program (8-year M.D. program) integrating Western and Chinese medicine together to nurture skilled TCM professionals since 1958. Graduates are proficient in their knowledge of Western and Chinese medicine, and the majority achieves dual licensures in Western and Chinese medicine after passing their board exams. There are also another post-baccalaureate TCM programs (5-year M.D. program) where graduates are qualified for only TCM board exam. Until 2012, there are approximately 59,017 Western medical doctors and 5,556 board-certified TCM doctors serving 23 million people in Taiwan. 93.7% of the hospitals/clinics are contracted with the National Health Insurance Program. By the end of 2010, approximately 23 million beneficiaries (nearly 99.89% of the Taiwanese population) were enrolled [18]. All claims data are stored in the National Health Insurance Research Database (NHIRD) and are available for academic research. This platform is suitable for evaluating the use of TCM treatments. To explore TCM use in children with AR, we analyzed a cohort of one million randomly sampled beneficiaries from the NHIRD.
METHODS Data Source
This study analyzed datasets from the NHIRD of Taiwan. The National Health Insurance Program was launched in 1995 and has provided Western medical inpatient
and outpatient services since that time; a TCM outpatient service followed in 1996 [18]. We retrieved data from the NHIRD (Longitudinal Health Insurance Database 2000; LHID 2000) from 1,000,000 randomly sampled persons who had enrolled in 2000. All of the data for enrollees from 2000-2010 were de-identified and further scrambled by the National Health Research Institutes in Taiwan before release, to avoid violating the privacy of the patients or healthcare providers. The Institutional Review Board of the China Medical University and Hospital approved this study (CMU-REC-101-012).
Study Subjects
The sampled cohort was screened to identify the 227,056 subjects who were <18 years of age (Fig. 1). The International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) codes were used exclude children without AR (N=95,452), leaving only the subjects with AR (ICD-9-CM code: 477.9). Children diagnosed with AR before the end of 2001 (N=34,653) were also excluded, ensuring that all of the subjects had been newly diagnosed with AR after 2002. Overall, 97,401 children were included in the study cohort. Children who visited the TCM service between 2002 and 2010 were defined as TCM users (N=61,472), while children with no TCM visit records were defined as non-TCM users (N=35,929). Co-morbidities of AR were identified by their ICD-9-CM codes (asthma ICD-9: 493; and atopic dermatitis ICD-9: 691). The prescribed Chinese herbal remedies were categorized according to their therapeutic actions and indications: the Cold Syndrome, the Hot Syndrome and the tonification of Qi. Monthly distributions of the Cold and Hot Syndromes were analyzed by comparing the monthly usage of their respective
prescriptions. Statistical Analysis
The statistical analyses used SAS software, version 9.2 (SAS Institute, Inc., Cary, NC, USA). The data analysis consisted of descriptive statistics, including the frequency of prescriptions for TCM users stratified by the patients’ demographic characteristics, the indications for prescribing TCM, and the most frequently prescribed herbal formulas and single herbs for treating pediatric AR. Primary indications were classified according to their ICD-9-CM codes. The diagnoses were coded according to the ICD-9 and were grouped into distinct broad disease categories. Comparisons of TCM users with non-TCM users employed univariate analysis. The relationships between the categorical variables and the differences between TCM users and non-TCM users were examined by Pearson’s χ2 tests: a P-value <0.05 was considered statistically significant.
RESULTS
Demographic Characteristics of Study Subjects
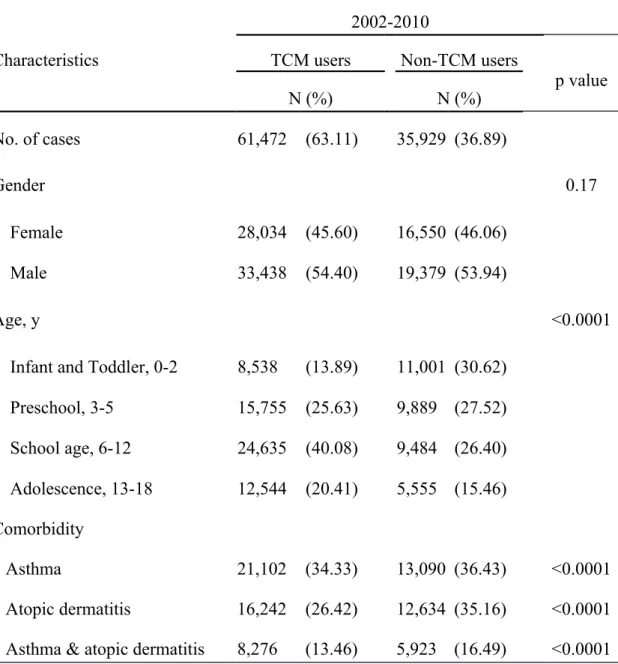
From 2002 to 2010, 97,401 pediatric patients were newly diagnosed with AR. Among these children, 61,472 had used TCM (63.11%) for AR, and 35,929 (36.89%) had not (Table 1). There were no significant differences in TCM use between boys and girls. School-age children and adolescents were more likely to be TCM users. The prevalence of allergic co-morbidities was high in the study subjects. There were significantly more children with asthma, atopic dermatitis or both among the non-TCM users, compared to the TCM users (all P<0.0001). Among the TCM users, 32.3%
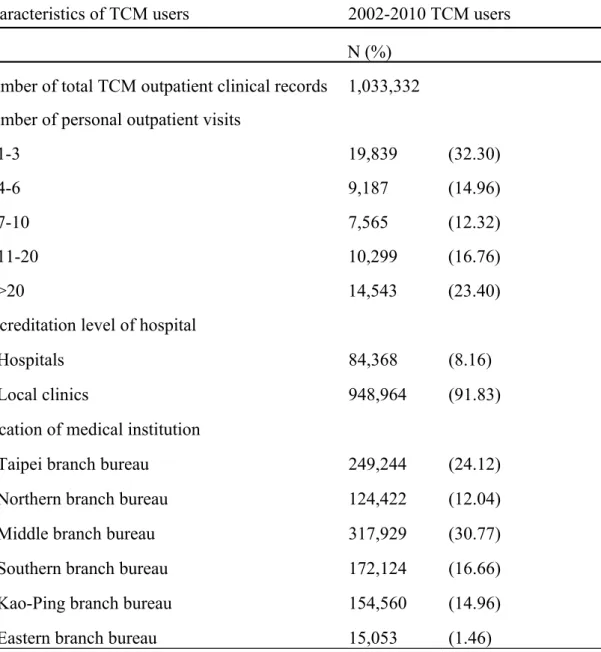
visited TCM outpatient clinics 1-3 times, and 23.40% visited >20 times. Most of the TCM users visited local clinics rather than hospitals (Table 2).
Frequency of TCM Visits by Major Disease Category
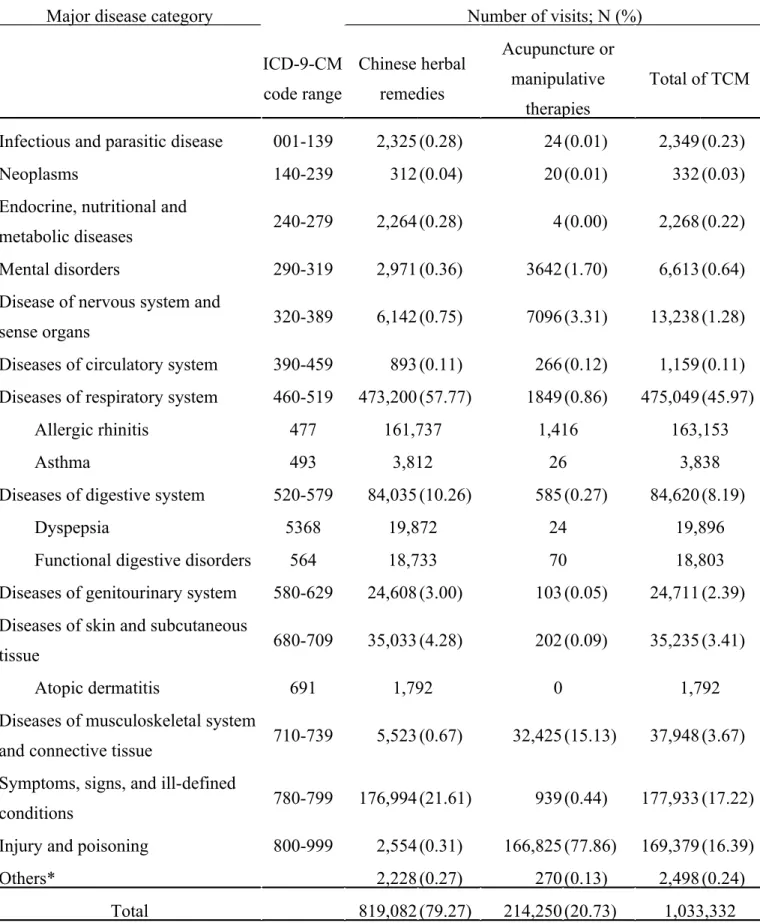
We analyzed the reasons for all TCM visits during the study period by their ICD-9-CM codes (Table 3). The most common reason for TICD-9-CM visits by Taiwanese children was respiratory system disease (45.97%), principally for AR treatment. Herbal remedies accounted for 79.27% of all TCM use; 20.73% consisted of acupuncture or manipulative therapies. Nevertheless, TCM treatments for children with AR mostly used herbs (161,737 of 163,153 visits, 99.1%) rather than acupuncture (1,415 of 163,153 visits, 0.9%).
TCM Prescription Patterns for Pediatric AR
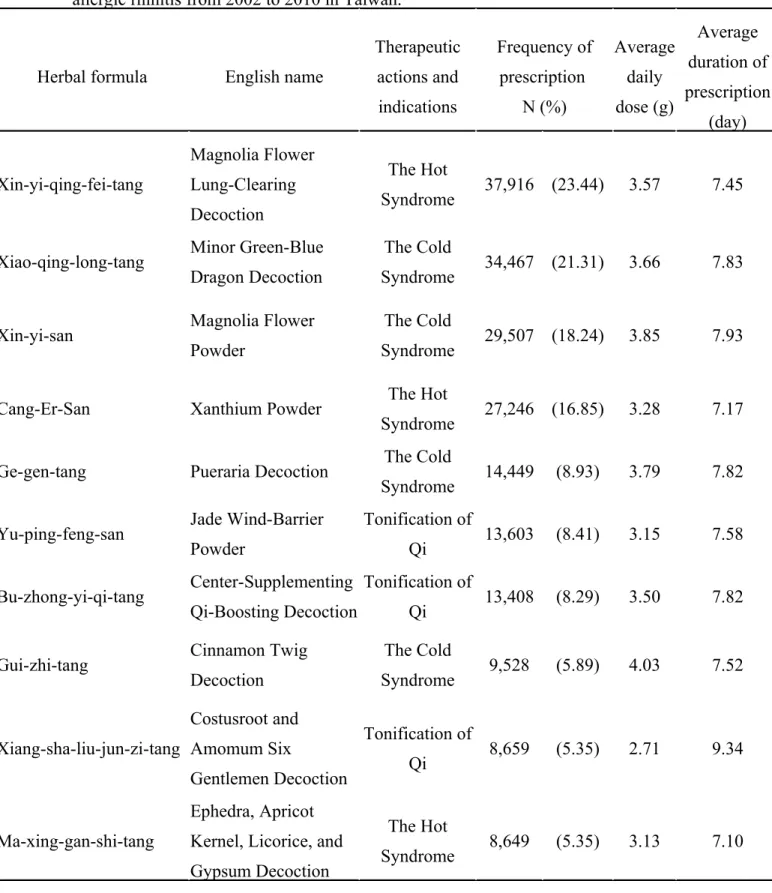
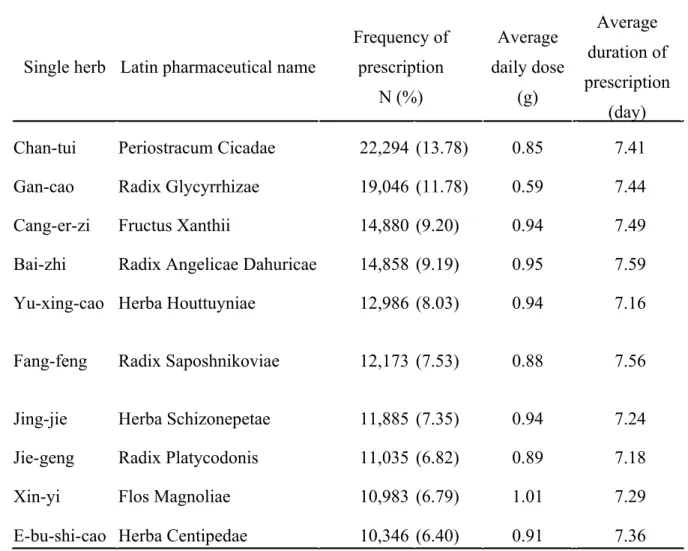
The ten most commonly prescribed TCM herbal formulas and single herbs are listed in Tables 4 and 5, respectively. They were “Xin-Yi-Qing-Fei-Tang” (Magnolia Flower Lung-Clearing Decoction; 23.44%), followed by “Xiao-Qing-Long-Tang” (Minor Blue-green Dragon Decoction; 21.31%), “Xin-Yi-San” (Magnolia Flower Powder; 18.24%), “Cang-Er-San” (Xanthium Powder; 16.85%) and “Ge-Gen-Tang” (Pueraria Decoction; 8.93%). The single herbs most frequently prescribed for pediatric AR were: Chan-tui (Periostracum cicadae; 13.78%), Gan-cao (Radix glycyrrhizae; 11.78%), Cang-er-zi (Xanthii fructus; 9.20%), Bai-zhi (Radix angelicae dahurica; 9.19%) and Yu-xing-cao (Herba houttuyniae; 8.03%).
Monthly Distribution of the Cold and Hot Syndromes
Diagnoses in Western medicine are usually based on patients’ clinical symptoms and laboratory data. The TCM diagnostic system differs in that the diagnosis, ZHENG
(TCM syndrome), is a thorough analysis according to TCM symptoms and signs. Therefore, patients with the same disease by Western medical criteria could have different TCM ZHENG diagnoses and might be prescribed different TCM treatments [17].
The subjects’ prescription patterns were further divided into two groups, according to the indications for the TCM formula Patients who received Xiao-qing-long-tang, Xin-yi-san, Ge-gen-tang and Gui-zhi-tang were treated for the Cold Syndrome; patients who received Xin-yi-quing-fei-tang, Gang-er-san, and Ma-xing-gan-shi-tang were treated for the Hot Syndrome (Table 4). The monthly distributions of prescriptions for the Hot and Cold Syndromes are shown in Figure 2. We found that the numbers of TCM prescriptions were higher during the winter (November, December, January) (Fig. 2A). In addition, TCM formulas for the Cold Syndrome were more frequently prescribed throughout the four seasons (Fig. 2B).
DISCUSSION
Allergic rhinitis is a chronic airway disease that usually requires long-term medical treatment. The possible side effects of anti-allergic treatments in Western medicine have been an important issue in pediatrics [19]. TCM has been used in Asian countries for centuries and has been perceived as safe. These reasons account for the popularity that TCM has gained in Taiwan. Our previous study found that approximately 20% of children visited TCM clinics in Taiwan [16]. In the present study, 63.11% of the subjects had used TCM. However, the 2010 revision of the Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines did not recommend using either acupuncture or herbs for allergic rhinitis because the available evidence for efficacy was of low quality [7]. The latest meta-analysis of randomized, controlled efficacy studies from 1999 to 2011 concluded that TCM appeared to benefit patients with persistent allergic rhinitis but that these studies were too small to draw firm conclusions [20]. The wide use of TCM in pediatric AR and the limited evidence of efficacy indicate that further investigations of the efficacy and mechanisms of TCM treatments are needed.
Some Chinese herbal products have been reported to have anti-allergic and anti-inflammatory effects. A combination of Xin-yi-san, Xiao-qing-long-tang and Xiang-sha-liu-jun-zi-tang reduced nasal symptoms and decreased the serum specific IgE, IFN-gamma and IL-5 of AR patients [21]. Xiao-qing-long-tang and Ma-xing-gan-shi-tang have shown anti-inflammatory and immunomodulatory effects in animal models [22, 23]. TCM theories regard allergic rhinitis as a condition that develops when the body does not produce sufficient-quality Qi relative to deficiencies in the internal organs. Therefore, approaches to tonify Qi are used to supplement these
deficiencies. Bu-zhong-yi-qi-tang, Xiang-sha-liu-jun-zi-tang and Yu-ping-feng-san are frequently used in pediatric AR patients in remission, to restore the deficiencies of the internal organs. In a randomized, controlled study, Bu-zhong-yi-qi-tang significantly improved nasal symptom scores [24]. The total serum IgE and the IL-4 stimulated production of prostaglandin E2 and leukotriene C4 by polymorphonuclear neutrophils were also significantly suppressed in the Bu-zhong-yi-qi-tang group. Animal experiments have also shown that Yu-ping-feng-san could significantly decrease the serum concentration of antigen-specific antibodies in allergic mice [25]. Two of the ingredients of Yu-ping-feng-san, Radix Saposhnikoviae and Radix Astragali, were also the major ingredients of an effective herbal products, Biminne, for perennial AR [26]. Moreover, respiratory infections, seen as exterior evils in TCM, are important triggers of AR exacerbation. Therefore, exterior-releasing formulations, such as Ge-gen-tang [27], are also commonly used.
Most of the commonly prescribed single herbs have allergic or anti-inflammatory effects in vitro or in vivo. Periostracum Cicadae had been show to have antioxidant and anti-inflammatory activities [28]. Radix Glycyrrhizae could inhibit memory Th2 responses and reduce eosinophilic pulmonary inflammation, serum IgE levels, IL-4 and IL-13 levels [29]. Radix Angelicae Dahuricae decreased the IgE and histamine levels and improved the skin lesions in a dust mite-induced dermatitis murine model [30]. Fructus Xanthii exerted anti-allergic rhinitis effect by ameliorating the nasal symptoms and down-regulating IgE levels in AR rats [31]. Flos Magnoliae inhibited mast cell-derived histamine release in vitro [32].
Several randomized, controlled studies have reported that acupuncture improves symptoms or enhances the quality of life of patients with AR [33-35]. In a double-blind, randomized, placebo-controlled trial of acupuncture for the treatment of pediatric AR, 8-week acupuncture treatment was more effective than sham acupuncture in decreasing the symptom scores and increasing the symptom-free days [34]. In the Acupuncture in Seasonal Allergic Rhinitis (ACUSAR) trial conducted in Germany, acupuncture significantly improved disease-specific quality of life and antihistamine use [33, 36]. However, very few of our study subjects used acupuncture, perhaps because most pediatric patients and their families would not tolerate the use of needles for AR treatment.
Seasonal change or temperature fluctuation has impact on allergic disorders, such as pediatric asthma [37]. We found that the numbers of TCM prescriptions were highest in the winter, and most of the patients suffered from the Cold Syndrome. The prevalence of the Cold/Hot Syndromes is constant throughout the year. An explanation for this lack of seasonality could be that most Taiwanese AR patients are perennial AR allergic to mites, instead of seasonal rhinitis [38] Patients with mite allergies are usually symptomatic throughout the year, but they can experience exacerbation in the winter. Unlike pollen allergies, our subjects rarely had seasonal flare-ups in the spring [39]. The Cold Syndrome and the Hot Syndrome are two key conditions of the TCM syndrome, and they are widely used in the diagnosis of diseases, including inflammation, infection, stress, and autoimmune disorders. The TCM diagnosis of the Hot Syndrome in AR patients more or less equates with a secondary microbial infection. Our results showed that a significant proportion of AR patients had the Hot
Syndrome, but any correlation between the Hot Syndrome and microbial infection requires further investigation.
Our study had several limitations. First, the rates of TCM utilization might have been underestimated because we did not include TCM treatments that were not covered by the National Health Insurance (NHI), such as folk medicine, which can be directly purchased from pharmacies. However, prescriptions covered by the NHI were from board-certified TCM doctors and thus were more accurate and reliable treatment choices. Second, the NHRID does not allow for evaluation of patients’ disease severity or TCM treatments’ efficacy. Therefore, a relationship between disease severity and TCM utilization or prescription patterns could not be established.
In conclusion, we found that approximately two thirds of pediatric AR patients
sought help from TCM in Taiwan. Our results should provide valuable information for pediatricians, parents of children with AR and the government concerning the health care of children with AR. Further research is warranted to examine the efficacy and safety of TCM for pediatric AR patients.
List of Abbreviations
CAM: complementary and alternative medicine; AR: allergic rhinitis; NHIRD: National Health Insurance Research Database; TCM: traditional Chinese medicine; ICD-9-CM: the International Classification of Diseases, 9th Revision, Clinical Modification
The authors declare that they have no conflict of interest.
Acknowledgments
This study was supported by China Medical University under the Aim for Top University Plan of the Ministry of Education, Taiwan. This study was also supported in part by the Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW103-TDU-B-212-113002). Yen H-R. was supported by a physician scientist grant (DMR-103-123) from China Medical University Hospital and a career-developing grant (NHRI-EX101-10124SC, NHRI-EX102-10124SC and NHRI-EX103-10124SC) from the National Health Research Institutes, Taiwan. This study was based in part on data from the National Health Insurance Research Database, provided by the National Health Insurance Administration, Ministry of Health and Welfare, and managed by National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of National Health Insurance Administration, Ministry of Health and Welfare, or National Health Research Institutes.
Authors’ Contribution:HRY and MFS conceptualized the study. TPH performed the statistical analysis. HRY, HYF, TTC and MFS contributed to the interpretation of TCM data and KLL the Western medicine data. HRY, KLL and MFS drafted the manuscript and finalized the manuscript.
REFERENCES
1. Greiner AN, Hellings PW, Rotiroti G, Scadding GK: Allergic rhinitis. Lancet
2011, 378(9809):2112-2122.
2. Liao PF, Sun HL, Lu KH, Lue KH: Prevalence of childhood allergic diseases in
central Taiwan over the past 15 years. Pediatrics and neonatology 2009,
50(1):18-25.
3. Chiang LC, Chen YH, Hsueh KC, Huang JL: Prevalence and severity of
symptoms of asthma, allergic rhinitis, and eczema in 10- to 15-year-old
schoolchildren in central Taiwan. Asian Pacific journal of allergy and immunology /
launched by the Allergy and Immunology Society of Thailand 2007, 25(1):1-5.
4. Feng CH, Miller MD, Simon RA: The united allergic airway: connections
between allergic rhinitis, asthma, and chronic sinusitis. American journal of
rhinology & allergy 2012, 26(3):187-190.
5. Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, Zuberbier
T, Baena-Cagnani CE, Canonica GW, van Weel C et al: Allergic Rhinitis and its
Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health
Organization, GA(2)LEN and AllerGen). Allergy 2008, 63 Suppl 86:8-160.
and alternative medicine use among patients presenting to a pediatric
otolaryngology clinic. International journal of pediatric otorhinolaryngology 2013,
77(5):721-725.
7. Brozek JL, Bousquet J, Baena-Cagnani CE, Bonini S, Canonica GW, Casale TB,
van Wijk RG, Ohta K, Zuberbier T, Schunemann HJ et al: Allergic Rhinitis and its
Impact on Asthma (ARIA) guidelines: 2010 revision. The Journal of allergy and
clinical immunology 2010, 126(3):466-476.
8. Larenas-Linnemann D, Blaiss M, Van Bever HP, Compalati E, Baena-Cagnani
CE: Pediatric sublingual immunotherapy efficacy: evidence analysis, 2009-2012.
Annals of allergy, asthma & immunology : official publication of the American College of Allergy, Asthma, & Immunology 2013, 110(6):402-415 e409.
9. Canonica GW, Bousquet J, Mullol J, Scadding GK, Virchow JC: A survey of the
burden of allergic rhinitis in Europe. Allergy 2007, 62 Suppl 85:17-25.
10. Worldwide variation in prevalence of symptoms of asthma, allergic
rhinoconjunctivitis, and atopic eczema: ISAAC. The International Study of
Asthma and Allergies in Childhood (ISAAC) Steering Committee. Lancet 1998,
351(9111):1225-1232.
Adults: national health interview survey, 2012. Vital and health statistics Series 10,
Data from the National Health Survey 2014(260):1-171.
12. Blaiss MS, Dykewicz MS, Skoner DP, Smith N, Leatherman B, Craig TJ, Bielory
L, Walstein N, Allen-Ramey F: Diagnosis and treatment of nasal and ocular
allergies: the Allergies, Immunotherapy, and RhinoconjunctivitiS (AIRS) surveys.
Annals of allergy, asthma & immunology : official publication of the American College of Allergy, Asthma, & Immunology 2014, 112(4):322-328 e321.
13. Koo M, Liang KL, Tsao H, Yen TT, Jiang RS, Yeh YC: Factors Associated with
the Use of Different Treatment Modalities among Patients with Upper Airway
Diseases in Taiwan: A Cross-Sectional Survey Study. Journal of allergy 2013,
2013:720879.
14. Park HL, Lee HS, Shin BC, Liu JP, Shang Q, Yamashita H, Lim B: Traditional
medicine in china, Korea, and Japan: a brief introduction and comparison.
Evidence-based complementary and alternative medicine : eCAM 2012, 2012:429103.
15. Huang TP, Liu PH, Lien AS, Yang SL, Chang HH, Yen HR: Characteristics of
traditional Chinese medicine use in children with asthma: a nationwide
population-based study. Allergy 2013, 68(12):1610-1613.
population-based study of traditional Chinese medicine usage in children in
Taiwan. Complementary therapies in medicine 2014, 22(3):500-510.
17. Liang KL, Jiang RS, Lee CL, Chiang PJ, Lin JS, Su YC: Traditional Chinese
Medicine ZHENG Identification Provides a Novel Stratification Approach in
Patients with Allergic Rhinitis. Evidence-based complementary and alternative
medicine : eCAM 2012, 2012:480715.
18. Yen HR, Huang TP, Sun MF: Chinese medicine usage in Taiwan: a nationwide
population-based study. RCHM Journal 2013, 10(2):21-27.
19. Juniper EF, Stahl E, Doty RL, Simons FE, Allen DB, Howarth PH: Clinical
outcomes and adverse effect monitoring in allergic rhinitis. The Journal of allergy
and clinical immunology 2005, 115(3 Suppl 1):S390-413.
20. Wang S, Tang Q, Qian W, Fan Y: Meta-analysis of clinical trials on traditional
Chinese herbal medicine for treatment of persistent allergic rhinitis. Allergy 2012,
67(5):583-592.
21. Yang SH, Hong CY, Yu CL: Decreased serum IgE level, decreased
IFN-gamma and IL-5 but increased IL-10 production, and suppressed cyclooxygenase
2 mRNA expression in patients with perennial allergic rhinitis after treatment
2001, 1(6):1173-1182.
22. Kao ST, Lin CS, Hsieh CC, Hsieh WT, Lin JG: Effects of xiao-qing-long-tang
(XQLT) on bronchoconstriction and airway eosinophil infiltration in
ovalbumin-sensitized guinea pigs: in vivo and in vitro studies. Allergy 2001, 56(12):1164-1171. 23. Kao ST, Yeh TJ, Hsieh CC, Shiau HB, Yeh FT, Lin JG: The effects of
Ma-Xing-Gan-Shi-Tang on respiratory resistance and airway leukocyte infiltration in
asthmatic guinea pigs. Immunopharmacol Immunotoxicol 2001, 23(3):445-458. 24. Yang SH, Yu CL: Antiinflammatory effects of Bu-zhong-yi-qi-tang in patients
with perennial allergic rhinitis. Journal of ethnopharmacology 2008,
115(1):104-109.
25. Makino T: [Pharmacological properties of Gyokuheifusan, a traditional
Kampo medicinal formula]. Yakugaku zasshi : Journal of the Pharmaceutical
Society of Japan 2005, 125(4):349-354.
26. Hu G, Walls RS, Bass D, Ramon B, Grayson D, Jones M, Gebski V: The
Chinese herbal formulation biminne in management of perennial allergic rhinitis:
a randomized, double-blind, placebo-controlled, 12-week clinical trial. Annals of
allergy, asthma & immunology : official publication of the American College of Allergy, Asthma, & Immunology 2002, 88(5):478-487.
27. Wu MS, Yen HR, Chang CW, Peng TY, Hsieh CF, Chen CJ, Lin TY, Horng JT:
Mechanism of action of the suppression of influenza virus replication by Ko-Ken
Tang through inhibition of the phosphatidylinositol 3-kinase/Akt signaling
pathway and viral RNP nuclear export. Journal of ethnopharmacology 2011,
134(3):614-623.
28. Xu MZ, Lee WS, Han JM, Oh HW, Park DS, Tian GR, Jeong TS, Park HY:
Antioxidant and anti-inflammatory activities of N-acetyldopamine dimers from
Periostracum Cicadae. Bioorganic & medicinal chemistry 2006, 14(23):7826-7834. 29. Yang N, Patil S, Zhuge J, Wen MC, Bolleddula J, Doddaga S, Goldfarb J,
Sampson HA, Li XM: Glycyrrhiza uralensis flavonoids present in anti-asthma
formula, ASHMI, inhibit memory Th2 responses in vitro and in vivo.
Phytotherapy research : PTR 2013, 27(9):1381-1391.
30. Lee H, Lee JK, Ha H, Lee MY, Seo CS, Shin HK: Angelicae Dahuricae Radix
Inhibits Dust Mite Extract-Induced Atopic Dermatitis-Like Skin Lesions in
NC/Nga Mice. Evidence-based complementary and alternative medicine : eCAM
2012, 2012:743075.
31. Peng W, Ming QL, Han P, Zhang QY, Jiang YP, Zheng CJ, Han T, Qin LP:
strumarium L. in rodent animals. Phytomedicine : international journal of
phytotherapy and phytopharmacology 2014, 21(6):824-829.
32. Shen Y, Pang EC, Xue CC, Zhao ZZ, Lin JG, Li CG: Inhibitions of mast
cell-derived histamine release by different Flos Magnoliae species in rat peritoneal
mast cells. Phytomedicine : international journal of phytotherapy and
phytopharmacology 2008, 15(10):808-814.
33. Brinkhaus B, Ortiz M, Witt CM, Roll S, Linde K, Pfab F, Niggemann B,
Hummelsberger J, Treszl A, Ring J et al: Acupuncture in patients with seasonal
allergic rhinitis: a randomized trial. Annals of internal medicine 2013,
158(4):225-234.
34. Ng DK, Chow PY, Ming SP, Hong SH, Lau S, Tse D, Kwong WK, Wong MF,
Wong WH, Fu YM et al: A double-blind, randomized, placebo-controlled trial of
acupuncture for the treatment of childhood persistent allergic rhinitis. Pediatrics
2004, 114(5):1242-1247.
35. Lee MS, Pittler MH, Shin BC, Kim JI, Ernst E: Acupuncture for allergic
rhinitis: a systematic review. Annals of allergy, asthma & immunology : official
publication of the American College of Allergy, Asthma, & Immunology 2009,
36. Reinhold T, Roll S, Willich SN, Ortiz M, Witt CM, Brinkhaus B:
Cost-effectiveness for acupuncture in seasonal allergic rhinitis: economic results of the
ACUSAR trial. Annals of allergy, asthma & immunology : official publication of the
American College of Allergy, Asthma, & Immunology 2013, 111(1):56-63.
37. Li S, Baker PJ, Jalaludin BB, Guo Y, Marks GB, Denison LS, Williams GM: An
Australian national panel study of diurnal temperature range and children's
respiratory health. Annals of allergy, asthma & immunology : official publication of
the American College of Allergy, Asthma, & Immunology 2014, 112(4):348-353
e341-348.
38. Lee YL, Shaw CK, Su HJ, Lai JS, Ko YC, Huang SL, Sung FC, Guo YL:
Climate, traffic-related air pollutants and allergic rhinitis prevalence in
middle-school children in Taiwan. The European respiratory journal 2003, 21(6):964-970. 39. Liang KL, Su MC, Shiao JY, Wu SH, Li YH, Jiang RS: Role of pollen allergy in
Taiwanese patients with allergic rhinitis. Journal of the Formosan Medical
Figure legends
Figure 1. Flow recruitment chart of subjects from the one million random samples obtained from the National Health Insurance Research Database (NHIRD) of Taiwan.
Figure 2. Monthly distribution of the prescriptions for the Cold and Hot Syndromes. The number (A) and percentage (B) of TCM herbal formulas for treating the Cold Syndrome (dotted line) and the Hot Syndrome (solid line).
Table 1: Demographic characteristics of TCM and non-TCM users among children with allergic rhinitis from 2002 to 2010 in Taiwan.
Characteristics
2002-2010
TCM users Non-TCM users
p value N (%) N (%) No. of cases 61,472 (63.11) 35,929 (36.89) Gender 0.17 Female 28,034 (45.60) 16,550 (46.06) Male 33,438 (54.40) 19,379 (53.94) Age, y <0.0001
Infant and Toddler, 0-2 8,538 (13.89) 11,001 (30.62) Preschool, 3-5 15,755 (25.63) 9,889 (27.52) School age, 6-12 24,635 (40.08) 9,484 (26.40) Adolescence, 13-18 12,544 (20.41) 5,555 (15.46) Comorbidity Asthma 21,102 (34.33) 13,090 (36.43) <0.0001 Atopic dermatitis 16,242 (26.42) 12,634 (35.16) <0.0001 Asthma & atopic dermatitis 8,276 (13.46) 5,923 (16.49) <0.0001 TCM: traditional Chinese medicine
Table 2: Demographic characteristics of TCM users among children with allergic rhinitis in Taiwan during 2002-2010.
Characteristics of TCM users 2002-2010 TCM users N (%)
Number of total TCM outpatient clinical records 1,033,332 Number of personal outpatient visits
1-3 19,839 (32.30)
4-6 9,187 (14.96)
7-10 7,565 (12.32)
11-20 10,299 (16.76)
>20 14,543 (23.40)
Accreditation level of hospital
Hospitals 84,368 (8.16)
Local clinics 948,964 (91.83)
Location of medical institution
Taipei branch bureau 249,244 (24.12)
Northern branch bureau 124,422 (12.04)
Middle branch bureau 317,929 (30.77)
Southern branch bureau 172,124 (16.66)
Kao-Ping branch bureau 154,560 (14.96)
Eastern branch bureau 15,053 (1.46)
Table 3: Frequency of TCM visits by major disease category (according to the 9th ICD codes) in children with allergic rhinitis from 2002 to 2010 in Taiwan.
Major disease category Number of visits; N (%)
ICD-9-CM code range Chinese herbal remedies Acupuncture or manipulative therapies Total of TCM
Infectious and parasitic disease 001-139 2,325 (0.28) 24 (0.01) 2,349 (0.23)
Neoplasms 140-239 312 (0.04) 20 (0.01) 332 (0.03)
Endocrine, nutritional and
metabolic diseases 240-279 2,264 (0.28) 4 (0.00) 2,268 (0.22)
Mental disorders 290-319 2,971 (0.36) 3642 (1.70) 6,613 (0.64)
Disease of nervous system and
sense organs 320-389 6,142 (0.75) 7096 (3.31) 13,238 (1.28)
Diseases of circulatory system 390-459 893 (0.11) 266 (0.12) 1,159 (0.11) Diseases of respiratory system 460-519 473,200 (57.77) 1849 (0.86) 475,049 (45.97)
Allergic rhinitis 477 161,737 1,416 163,153
Asthma 493 3,812 26 3,838
Diseases of digestive system 520-579 84,035 (10.26) 585 (0.27) 84,620 (8.19)
Dyspepsia 5368 19,872 24 19,896
Functional digestive disorders 564 18,733 70 18,803
Diseases of genitourinary system 580-629 24,608 (3.00) 103 (0.05) 24,711 (2.39) Diseases of skin and subcutaneous
tissue 680-709 35,033 (4.28) 202 (0.09) 35,235 (3.41)
Atopic dermatitis 691 1,792 0 1,792
Diseases of musculoskeletal system
and connective tissue 710-739 5,523 (0.67) 32,425 (15.13) 37,948 (3.67) Symptoms, signs, and ill-defined
conditions 780-799 176,994 (21.61) 939 (0.44) 177,933 (17.22)
Injury and poisoning 800-999 2,554 (0.31) 166,825 (77.86) 169,379 (16.39)
Others* 2,228 (0.27) 270 (0.13) 2,498 (0.24)
Table 4: Ten most common herbal formulas prescribed for the treatment of pediatric allergic rhinitis from 2002 to 2010 in Taiwan.
Herbal formula English name
Therapeutic actions and indications Frequency of prescription N (%) Average daily dose (g) Average duration of prescription (day) Xin-yi-qing-fei-tang Magnolia Flower Lung-Clearing Decoction The Hot Syndrome 37,916 (23.44) 3.57 7.45
Xiao-qing-long-tang Minor Green-Blue Dragon Decoction
The Cold
Syndrome 34,467 (21.31) 3.66 7.83
Xin-yi-san Magnolia Flower
Powder
The Cold
Syndrome 29,507 (18.24) 3.85 7.93
Cang-Er-San Xanthium Powder The Hot
Syndrome 27,246 (16.85) 3.28 7.17 Ge-gen-tang Pueraria Decoction The Cold
Syndrome 14,449 (8.93) 3.79 7.82 Yu-ping-feng-san Jade Wind-Barrier
Powder Tonification of Qi 13,603 (8.41) 3.15 7.58 Bu-zhong-yi-qi-tang Center-Supplementing Qi-Boosting Decoction Tonification of Qi 13,408 (8.29) 3.50 7.82
Gui-zhi-tang Cinnamon Twig Decoction The Cold Syndrome 9,528 (5.89) 4.03 7.52 Xiang-sha-liu-jun-zi-tang Costusroot and Amomum Six Gentlemen Decoction Tonification of Qi 8,659 (5.35) 2.71 9.34 Ma-xing-gan-shi-tang Ephedra, Apricot Kernel, Licorice, and Gypsum Decoction
The Hot
Table 5: Ten most common single herbs prescribed for the treatment of children with allergic rhinitis from 2002 to 2010 in Taiwan.
Single herb Latin pharmaceutical name
Frequency of prescription N (%) Average daily dose (g) Average duration of prescription (day) Chan-tui Periostracum Cicadae 22,294 (13.78) 0.85 7.41
Gan-cao Radix Glycyrrhizae 19,046 (11.78) 0.59 7.44
Cang-er-zi Fructus Xanthii 14,880 (9.20) 0.94 7.49
Bai-zhi Radix Angelicae Dahuricae 14,858 (9.19) 0.95 7.59 Yu-xing-cao Herba Houttuyniae 12,986 (8.03) 0.94 7.16
Fang-feng Radix Saposhnikoviae 12,173 (7.53) 0.88 7.56
Jing-jie Herba Schizonepetae 11,885 (7.35) 0.94 7.24
Jie-geng Radix Platycodonis 11,035 (6.82) 0.89 7.18
Xin-yi Flos Magnoliae 10,983 (6.79) 1.01 7.29