Clonidine as adjuvant for oxybuprocaine, bupivacaine or
dextrorphan has a significant peripheral action in intensifying
and prolonging analgesia in response to local dorsal cutaneous
noxious pinprick in rats
Yu-Wen Chen, Ph.D.,1,2 Chin-Chen Chu, M.D., Ph.D.,3 Yu-Chung Chen, M.S.,4 Ching-Hsia Hung, Ph.D.,5,* Meng-I Hsueh, B.S.,1 Jhi-Joung Wang, M.D., Ph.D.3
1
Department of Physical Therapy, China Medical University, Taichung, Taiwan
2
Graduate Institute of Neural and Cognitive Sciences, China Medical University, Taichung, Taiwan
3
Department of Medical Research, Chi-Mei Medical Center, Tainan, Taiwan
4
Division of Physical Therapy, Department of Physical Medicine and Rehabilitation, Cheng Hsin General Hospital, Taipei, Taiwan
5
Institute & Department of Physical Therapy, National Cheng Kung University, Tainan, Taiwan
*Address correspondence and reprint requests to: Ching-Hsia Hung, PhD, Department of Physical Therapy, National Cheng Kung University, No.1 Ta-Hsueh Road, Tainan, Taiwan
Tel: 886-6-2353535 ext 5939 Fax: 886-6-2370411
Abstract
The aim of the study was to evaluate co-administration of clonidine with
oxybuprocaine (ester type), bupivacaine (amide type) or dextrorphan (non-ester or
non-amide type) and to see whether it could have a peripheral action in enhancing
local anesthesia on infiltrative cutaneous analgesia in rats. Cutaneous analgesia was
evaluated by a block of the cutaneous trunci muscle reflex (CTMR) in response to
local dorsal cutaneous noxious pinprick in rats. The analgesic effect of the addition of
clonidine with oxybuprocaine, bupivacaine or dextrorphan by subcutaneous injection
was evaluated. On an ED50 basis, the rank of drug potency was oxybuprocaine >
bupivacaine > dextrorphan (P<0.01). Mixtures of clonidine (0.12 μmol) with
oxybuprocaine, bupivacaine or dextrorphan (ED50 or ED95) extended the duration of
action and increased the potency on infiltrative cutaneous analgesia. Among these
drugs, the addition of clonidine to bupivacaine (amide type) elicits the most effective
cutaneous analgesia. Clonidine at the dose of 0.12 and 0.24 µmol did not produce
cutaneous analgesia. Oxybuprocaine showed more potent cutaneous analgesia than
bupivacaine or dextrorphan in rats. Co-administration of oxybuprocaine, bupivacaine
or dextrorphan with clonidine increased the potency and duration on infiltrative
cutaneous analgesia. The addition of clonidine to bupivacaine (amide type) elicits
(non-ester or non-amide type).
Key Words: Clonidine; Oxybuprocaine; Bupivacaine; Dextrorphan; Infiltrative
Oxybuprocaine (benoxinate), an ester type local anesthetic, produces the dose-related
cutaneous analgesia [16] and spinal anesthesia [17]. In a previous study we have
shown that systemic toxicity following intravenous oxybuprocaine and
proxymetacaine occurred later compared to equipotent doses of bupivacaine, an
amide-linkage local anesthetic [16]. Dextrorphan, a non-ester or non-amide type local
anesthetic, has a local anesthetic effect on infiltrative cutaneous analgesia, [7] spinal
or sciatic nerve blockades [4, 15]. In addition, intravenous equipotent analgesic dose
of dextrorphan is better tolerated to elicit cardiovascular and central nervous system
toxicity than bupivacaine [8]. Furthermore, oxybuprocaine or dextrorphan showed a
long-acting local anesthetic effect similar to that provided by bupivacaine [4, 17].
Clonidine is a frequently used adjuvant to local anesthetics. The analgesic effects
of clonidine when administered epidurally or intrathecally have been showed and are due to its α2-adrenoreceptor properties [10, 11]. The benefit of clonidine when added to local anesthetics for peripheral nerve blockades is less clear, although it is widely
believed that clonidine decreases postoperative analgesic requirement or improves the
quality and duration of local anesthetic blockade [22]. Several experiments are
focused on the benefit of clonidine added to amino-amide local anesthetic for nerve
blocks [22]. The aim of the study was to evaluate co-administration of clonidine with
see whether it could have a peripheral action in enhancing the quality and duration of
local anesthesia after a single subcutaneous injection.
Two hundred and sixteen male Sprague-Dawley rats weighting 200-250 g were
obtained from the National Laboratory Animal Centre (Taipei, Taiwan), and housed
in a climate controlled room, with food and water available ad libitum up to time of
testing. The climate- controlled room was maintained at 22˚C with approximately
50% relative humidity on a 12-h light/dark cycle (6:00 AM–6:00 PM). The
experimental protocols were approved by the Institutional Animal Care and Use
Committee (IACUC) of China Medical University, Taichung, Taiwan and conformed
to the recommendations and policies of the International Association for the Study of
Pain (IASP).
Benoxinate (oxybuprocaine) HCl, bupivacaine HCl, dextrorphan tartrate, and
clonidine HCl were purchased from Sigma-Aldrich Chemical Co. (St. Louis, MO,
USA). All drugs were dissolved in 0.9% NaCl.
Three experiments were performed. In experiment 1, the time course of
oxybuprocaine (1.20, 0.60, 0.15, 0.03 µmol), bupivacaine (1.80, 0.45, 0.30, 0.23
µmol), dextrorphan (9.00, 6.00, 3.00, 0.60 µmol), and clonidine (0.24, 0.12 µmol) on
infiltrative cutaneous analgesia was evaluated (n = 8 rats for each dose of each drug).
under curves (AUCs) of drug (ED50 or ED95) or co-administration of drug (ED50 or
ED95) and clonidine (0.12 µmol) were tested on infiltrative cutaneous analgesia (n = 8
rats for each dose of each drug). In experiment 3, after the above experiments, one
control group was performed to rule out the possibility of systemic effect of drugs on
infiltrative cutaneous analgesia. Animals (n = 8 rats for each dose of each drug)
received subcutaneous injection (the region of rats' thigh) of testing drug (oxybuprocaine, bupivacaine or dextrorphan) at a dose of 2ED95 or clonidine at a
dose of 0.24 µmol.
On the day before the subcutaneous injection, the hair on the rats' dorsal surface
of the thoracolumbar region (10×6 cm2) was mechanically shaved. The subcutaneous injection of drug was performed as reported previously [6, 16]. In brief, drug
dissolved in 0.6 mL was injected subcutaneously using a 30-gauge needle in
unanesthetized rats at the dorsal surface of the thoracolumbar region. After
subcutaneous injection, a circular elevation of the skin, a wheal, approximately 2 cm
in diameter occurred. The wheal was marked with ink within one minute after
subcutaneous injection. For consistency, one experienced investigator (Dr. Chen Y.W.)
who was blinded to the drugs injected was responsible for assessing the cutaneous
analgesic effect.
during the experiment and generally improve their experimental performance before
the experiment. Cutaneous analgesia was evaluated by the cutaneous trunci muscle
reflex (CTMR), characterized by the reflex movement of the skin over the back
produced by twitches of the lateral thoracospinal muscle in response to local dorsal
cutaneous stimulation after drug injections [6, 16]. A Von Frey filament (No.15;
Somedic Sales AB, Stockholm, Sweden), to which the cut end of an 18-gauge needle
was affixed, was used to produce the standardized nociceptive stimulus (19±1 g).
After observing an animal normal reaction to pinpricks applied outside the wheal and
on the contralateral side, we applied six pinpricks with a frequency of 1 Hz inside the
wheal and scored the number to which the rat failed to react. Cutaneous analgesic
effect of each drug was assessed quantitatively as the number of times the pinprick
failed to elicit a response, with, for example, the complete absence of six responses
was defined as complete nociceptive block (100% of possible effect; 100% PE).
The test of six pinpricks was applied at 0, 2 and 5 min after injection, every 5
min after injection for the first 30 min afterwards, then again every 10 min after
injection for 30-60 min, and every 15-30 min thereafter until the CTMR fully
recovered from the block. During the test, the maximum blockade in a time course of
cutaneous analgesia of the drug was described as the %MPE. The duration of action
(no analgesic effect or 0% MPE) [6, 16].
After subcutaneously injecting the rats with four doses of each drug (n = 8 for
each dose of each drug), dose-response curves were obtained by the % MPE for each
dose of each drug. The value of 50% or 95% effective dose (ED50 or ED95), defined as
the dose that caused 50% or 95% cutaneous analgesic effect, respectively, was
obtained by a SAS NLIN analysis (SAS Institute Inc., Carey, NC) [5, 19].
Data are presented as mean SD (range) or ED50 and ED95 values with 95%
confidence interval (95% CI). Data were analyzed by the Student’s t-test or 1-way analysis of variance (ANOVA) followed by pairwise Tukey’s honest significance difference (HSD) test. A statistical software, SPSS for Windows (version 17.0, SPSS,
Inc, Chicago, IL, USA), was used, and a P value less than 0.05 was considered statistically significant.
Subcutaneous injections of oxybuprocaine, bupivacaine, and dextrorphan
produced dose-dependent cutaneous analgesia in rats (Fig. 1; [8, 16]). Clonidine alone
at the doses of 0.12 and 0.24 µmol (data not shown) showed no cutaneous analgesia.
The ED50s and ED95s of drugs constructed from Figure 1 were demonstrated in Table
1. On an ED50 basis, the rank of drug potency was oxybuprocaine > bupivacaine >
dextrorphan (Table 1).
complete sensory blockade (100% MPE) in the oxybuprocaine (8 of 8 rats) or
bupivacaine (8 of 8 rats) group occurred, but not in the dextrorphan (5 of 8 rats) group
(Fig. 2 and Table 2). Subcutaneous injection of clonidine alone at the dose of 0.12
µmol showed no cutaneous analgesia (Fig. 2). Compared with drugs at the dose of
ED50 alone, drugs (ED50) co-injected with 0.12 µmol clonidine, the AUCs were
increased in the oxybuprocaine, bupivacaine, and dextrorphan groups (P<0.05). The
%MPE, duration and AUCs of drugs at the dose of ED50 with clonidine were greater
(P<0.05) than drugs (ED50) without clonidine in Table 2. The rank in intensifying
complete block time, full recovery time, and AUCs of the co-administration of drug
(ED50) and clonidine was bupivacaine = ocybuprocaine > dextrorphan (Table 2;
P<0.05) when compared with drug (ED50) alone.
At the dose of ED95, oxybuprocaine, bupivacaine, and dextrorphan elicited 92%,
90%, and 88% sensory blockade, respectively,in Figure 2 and Table 3. Subcutaneous
injection of clonidine alone at the dose of 0.12 µmol demonstrated no cutaneous
analgesia (Fig. 2). After drugs at the dose of ED95 were co-injected with clonidine
(0.12 µmol), oxybuprocaine, bupivacaine, and dextrorphan caused 100%, 100%, and
100% sensory blockade (100% MPE), respectively(Fig. 2 and Table 3). The %MPE,
duration and AUCs of drugs at the dose of ED95 with clonidine were greater (P<0.05)
time, full recovery time, and AUCs of the co-administration of drug (ED95) and
clonidine was bupivacaine > ocybuprocaine > dextrorphan (Table 3; P<0.05).
Neither the thigh subcutaneous injection of clonidine (0.24 µmol) nor thigh
subcutaneous injections of oxybuprocaine, bupivacaine, and dextrorphan (2ED95)
demonstrated cutaneous analgesia, loss of motor activity or sedation (data not shown).
All rats recovered completely after each subcutaneous injection of drug.
In this report we showed for the first time that oxybuprocaine was a more potent
local anesthetic on infiltrative cutaneous analgesia than dextrorphan. Clonidine
dramatically improves the sensory blocking effect and duration of oxybuprocaine,
bupivacaine, and dextrorphan. The benefit rank of adding clonidine to local
anesthetics is bupivacaine > oxybuprocaine > dextrorphan.
The clinical relevance of this prolonged sensory blockade, though useful in
certain situations, may be limited overall, when considering the higher incidence of
motor blockade caused by clonidine [9]. Hypotension may be an important problem
when using clonidine as adjuvant in neuraxial anesthesia or in pain regimens [2, 9].
Motor blockade following central neuraxial block and sedative effects of clonidine
should be limited. Given these dose-limiting central side effects, clonidine may be
beneficial to apply peripherally. In addition, both scientific and clinical studies have
additive, as well as suggesting local anesthetic-like properties of clonidine itself [3,
13]. Therefore, this study evaluated the adding clonidine to local anesthetics on
infiltrative cutaneous analgesia in rats. We found that co-administration of clonidine
(0.12 μmol) with oxybuprocaine, bupivacaine or dextrorphan prolonged duration of
action and enhanced cutaneous analgesia. Our data agree with those results, which
showed that clonidine has a significant peripheral action in enhancing local anesthetic
duration on subcutaneous co-infiltration with lidocaine [23].
In this study, cutaneous analgesia (AUC) of co-administration of drug
(oxybuprocaine, bupivacaine and dextrorphan) at the dose of ED95 and clonidine (0.12
μmol) was approximately 3.7-, 4.2-, and 2.9-folds greater than drug alone, respectively. Our results also demonstrated that clonidine as an adjuvant for
oxybuprocaine, bupivacaine, and dextrorphan increased the potency of drug on
infiltrative cutaneous analgesia. Furthermore, cutaneous analgesia (AUC) of
co-administration of drug (oxybuprocaine, bupivacaine and dextrorphan) at the dose
of ED50 and clonidine (0.12 μmol) was approximately 7.7-, 8.2-, and 5.3-folds greater
than drug alone, respectively. Coadministration of bupivacaine with clonidine
extended longer duration on infiltrative cutaneous analgesia than oxybuprocaine or
dextrorphan. It has been mentioned that clonidine, clinically added to preparations of
clonidine may cause local vasoconstriction, [10, 27] thus decreasing local anaesthetic
spread and removal around nerves [10, 21]. Secondly, clonidine blocked C and Aδ
fibres [3, 12] as a consequence of an increase in K+ conductance in isolated neurons, [1, 20] thus intensifying local anesthetic conduction block [12]. Thirdly, spinal
clonidine combined with local anesthetics [21, 25] or used in peripheral nerve
blockades [12, 23] intensifies and prolongs anesthesia.
A single subcutaneous injection of clonidine (1.2 mg/kg) resulted in delayed
tactile hypersensitivity 24–34 h after clonidine administration in rats [24]. Our study
displayed that subcutaneous injection of clonidine (0.12–0.24 µmol; 0.14–0.28
mg/kg), an α2-adrenoreceptor agonist, did not produce any cutaneous analgesia to
local dorsal cutaneous noxious pinprick. Our previous experiment showed that
dextrorphan with epinephrine produced an additive effect on infiltrative cutaneous
analgesia, [7] but adding clonidine to dextrorphan elicited a supra-additive effect as a
cutaneous analgesic (Fig. 2). It may be explained that α1-adrenoceptor agonists (e.g.
epinephrine and phenylephrine) at these doses between 0.003 – 1.47 µmol can mainly act by mixed subtypes of α1-adrenoceptor to induce the local anesthetic activity [26]. In this study, we used the pinprick with a frequency of 1 Hz [14, 18] which is
impossible that repeated pinpricks may change, in fact decrease the response to
In summary, oxybuprocaine produced more potent cutaneous analgesia than
dextrorphan on an ED50 basis, and the effect of clonidine on infiltrative local
anesthesia with oxybuprocaine, bupivacaine or dextrorphan has a significant
peripheral action in intensifying and prolonging local anesthetic effects. On an
equipotent basis (ED50 or ED95), bupivacaine (amide type) showed more effective
cutaneous analgesia than oxybuprocaine (ester type) or dextrorphan (other type) when adding clonidine.
Acknowledgements
This work was supported by the National Science Council of Taiwan (NSC
Table 1. The 50% effective doses (ED50s) and ED95s of drugs on infiltrative cutaneous analgesia Drug ED50s ( 95% CI ) ED95s ( 95% CI ) Oxybuprocaine 0.23 (0.19 – 0.28) 1.29 (1.23 – 1.39) Bupivacaine 0.66 (0.55 – 0.78) 1.97 (1.88 – 2.09) Dextrorphan 2.47 (2.03 – 3.00) 8.45 (8.33 – 8.68)
ED50s and ED95s of drugs (μmol) were obtained from Figure 1. CI = confidence
interval. Potencies of drugs (ED50s) were oxybuprocaine > bupivacaine > dextrorphan
(P<0.01, for each comparison) using 1-way ANOVA followed by pairwise Tukey’s HSD test.
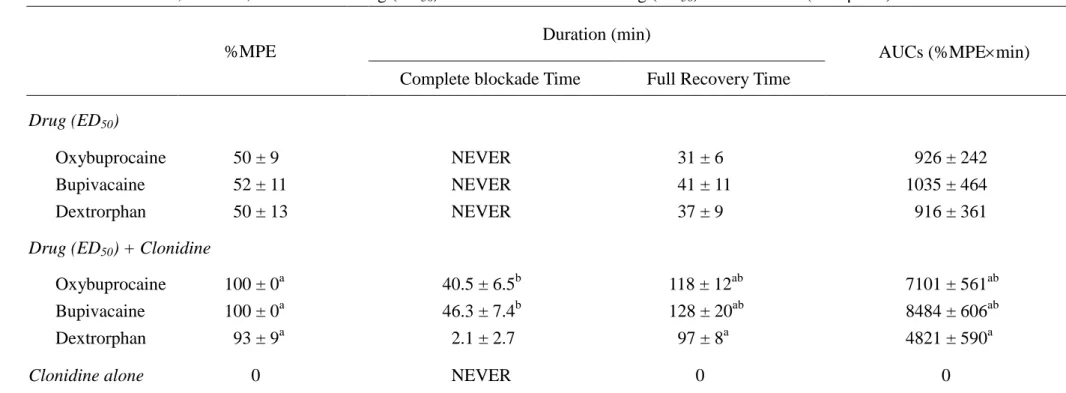
Table 2. The %MPE, duration, and AUCs of drug (ED50) or co-administration of drug (ED50) and clonidine (0.12 µmol)
%MPE
Duration (min)
AUCs (%MPEmin) Complete blockade Time Full Recovery Time
Drug (ED50)
Oxybuprocaine 50 ± 9 NEVER 31 ± 6 926 ± 242
Bupivacaine 52 ± 11 NEVER 41 ± 11 1035 ± 464
Dextrorphan 50 ± 13 NEVER 37 ± 9 916 ± 361
Drug (ED50) + Clonidine
Oxybuprocaine 100 ± 0a 40.5 ± 6.5b 118 ± 12ab 7101 ± 561ab
Bupivacaine 100 ± 0a 46.3 ± 7.4b 128 ± 20ab 8484 ± 606ab
Dextrorphan 93 ± 9a 2.1 ± 2.7 97 ± 8a 4821 ± 590a
Clonidine alone 0 NEVER 0 0
Percent of maximum possible effect (%MPE), duration of action, area under curves (AUCs) for drug (ED50) or co-administration of drug (ED50)
and clonidine at 0.12 µmol (n = 8 in all groups) on infiltrative cutaneous analgesia (mean SD). NEVER: the complete blockade was never obtained. The symbol (a) indicates P < 0.05 when drug alone compared with the co-administraion of drug and clonidine using a student's t test. The symbol (b) indicates P < 0.05 when dextrorphan compared with oxybuprocaine or bupivacaine using 1-way ANOVA followed by pairwise Tukey’s HSD test. Clonidine was at the dose of 0.12 µmol.
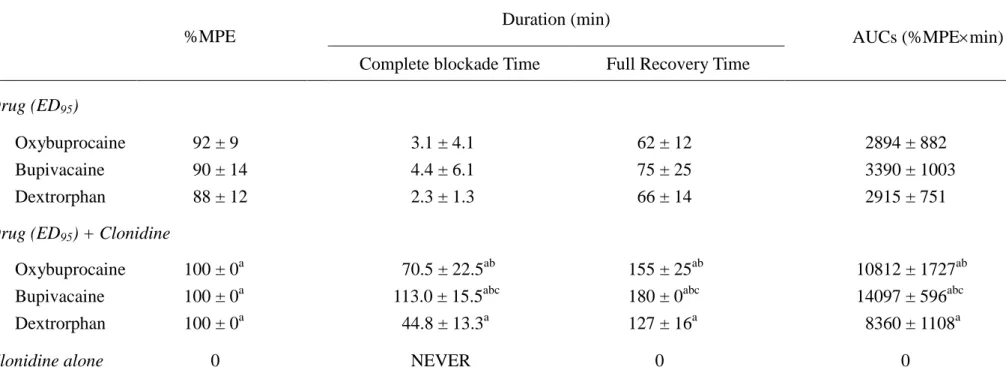
Table 3. The %MPE, duration, and AUCs of drug (ED95) or co-administration of drug (ED95) and clonidine (0.12 µmol)
%MPE
Duration (min)
AUCs (%MPEmin) Complete blockade Time Full Recovery Time
Drug (ED95)
Oxybuprocaine 92 ± 9 3.1 ± 4.1 62 ± 12 2894 ± 882
Bupivacaine 90 ± 14 4.4 ± 6.1 75 ± 25 3390 ± 1003
Dextrorphan 88 ± 12 2.3 ± 1.3 66 ± 14 2915 ± 751
Drug (ED95) + Clonidine
Oxybuprocaine 100 ± 0a 70.5 ± 22.5ab 155 ± 25ab 10812 ± 1727ab
Bupivacaine 100 ± 0a 113.0 ± 15.5abc 180 ± 0abc 14097 ± 596abc
Dextrorphan 100 ± 0a 44.8 ± 13.3a 127 ± 16a 8360 ± 1108a
Clonidine alone 0 NEVER 0 0
Percent of maximum possible effect (%MPE), duration of action, area under curves (AUCs) for drug (ED95) or co-administration of drug (ED95)
and clonidine at 0.12 µmol (n = 8 in all groups) on infiltrative cutaneous analgesia (mean SD). NEVER: the complete blockade was never obtained. The symbol (a) indicates P < 0.05 when drug alone compared with the co-administraion of drug and clonidine using a student's t test. The symbol (b) indicates P < 0.05 when dextrorphan compared with oxybuprocaine or bupivacaine using 1-way ANOVA followed by pairwise Tukey’s HSD test. The symbol (c) indicates P < 0.05 when oxybuprocaine compared with bupivacaine using 1-way ANOVA followed by pairwise Tukey’s HSD test.
Legends to figures
Figure 1. Time courses of cutaneous analgesia of oxybuprocaine, bupivacaine, and
dextrorphan on infiltrative cutaneous analgesia (four doses in each group) in rats. Values are expressed as mean SD; n = 8 rats for each dose of each drug.
Figure 2. The addition of clonidine (CL) with oxybuprocaine, bupivacaine or
dextrorphan (ED50 or ED95) on infiltrative cutaneous analgesia in rats. Clonidine was
at the dose of 0.12 µmol and produced no cutaneous analgesia. Values are expressed as mean SD; n = 8 rats for each dose of each drug. The ED50 or ED95 means 50% or
References
[1] R. Andrade, G.K. Aghajanian, Opiate- and alpha 2-adrenoceptor-induced
hyperpolarizations of locus ceruleus neurons in brain slices: reversal by cyclic
adenosine 3':5'-monophosphate analogues, J. Neurosci. 5 (1985) 2359-2364.
[2] S. Bhatnagar, S. Mishra, S. Madhurima, M. Gurjar, A.S. Mondal, Clonidine as
an analgesic adjuvant to continuous paravertebral bupivacaine for
post-thoracotomy pain, Anaesth. Intensive Care 34 (2006) 586-591.
[3] J.F.t. Butterworth, G.R. Strichartz, The alpha 2-adrenergic agonists clonidine
and guanfacine produce tonic and phasic block of conduction in rat sciatic
nerve fibers, Anesth. Analg. 76 (1993) 295-301.
[4] Y.W. Chen, Y.C. Chen, C.N. Lin, C.C. Chu, M.T. Lin, J.J. Wang, C.H. Kao,
The spinal anaesthetic effect of dextromethorphan, dextrorphan, and
3-methoxymorphinan, Eur. J. Pharmacol. 569 (2007) 188-193.
[5] Y.W. Chen, C.C. Chu, Y.C. Chen, J.J. Wang, C.H. Hung, The dose-dependent
study of verapamil and diltiazem on spinal anesthesia in the rat, Neurosci. Lett.
482 (2010) 76-80.
[6] Y.W. Chen, K.S. Chu, C.N. Lin, J.I. Tzeng, C.C. Chu, M.T. Lin, J.J. Wang,
Dextromethorphan or dextrorphan have a local anesthetic effect on infiltrative
[7] Y.W. Chen, K.S. Liu, J.J. Wang, W. Chou, C.H. Hung, Isobolographic analysis
of epinephrine with bupivacaine, dextromethorphan, 3-methoxymorphinan, or
dextrorphan on infiltrative anesthesia in rats: dose-response studies, Reg.
Anesth. Pain Med. 33 (2008) 115-121.
[8] Y.W. Chen, J.J. Wang, T.Y. Liu, Y.C. Chen, C.H. Hung, Systemic
dextromethorphan and dextrorphan are less toxic in rats than bupivacaine at
equianesthetic doses, Can. J. Anaesth. 58 (2011) 55-61.
[9] X. Culebras, E. Van Gessel, P. Hoffmeyer, Z. Gamulin, Clonidine combined
with a long acting local anesthetic does not prolong postoperative analgesia
after brachial plexus block but does induce hemodynamic changes, Anesth.
Analg. 92 (2001) 199-204.
[10] J.C. Eisenach, M. De Kock, W. Klimscha, alpha(2)-adrenergic agonists for
regional anesthesia. A clinical review of clonidine (1984-1995),
Anesthesiology 85 (1996) 655-674.
[11] N. Elia, X. Culebras, C. Mazza, E. Schiffer, M.R. Tramer, Clonidine as an
adjuvant to intrathecal local anesthetics for surgery: systematic review of
randomized trials, Reg. Anesth. Pain. Med. 33 (2008) 159-167.
[12] D.M. Gaumann, P.C. Brunet, P. Jirounek, Clonidine enhances the effects of
[13] D.M. Gaumann, P.C. Brunet, P. Jirounek, Hyperpolarizing afterpotentials in C
fibers and local anesthetic effects of clonidine and lidocaine, Pharmacology 48
(1994) 21-29.
[14] A. Haderer, P. Gerner, G. Kao, V. Srinivasa, G.K. Wang, Cutaneous analgesia
after transdermal application of amitriptyline versus lidocaine in rats, Anesth.
Analg. 96 (2003) 1707-1710.
[15] C.H. Hou, J.I. Tzeng, Y.W. Chen, C.N. Lin, M.T. Lin, C.H. Tu, J.J. Wang,
Dextromethorphan, 3-methoxymorphinan, and dextrorphan have local
anaesthetic effect on sciatic nerve blockade in rats, Eur. J. Pharmacol. 544
(2006) 10-16.
[16] C.H. Hung, K.S. Liu, D.Z. Shao, K.I. Cheng, Y.C. Chen, Y.W. Chen, The
systemic toxicity of equipotent proxymetacaine, oxybuprocaine, and
bupivacaine during continuous intravenous infusion in rats, Anesth. Analg. 110
(2010) 238-242.
[17] C.H. Hung, J.J. Wang, Y.C. Chen, C.C. Chu, Y.W. Chen, Intrathecal
oxybuprocaine and proxymetacaine produced potent and long-lasting spinal
anesthesia in rats, Neurosci. Lett. 454 (2009) 249-253.
[18] M.A. Khan, P. Gerner, G. Kuo Wang, Amitriptyline for prolonged cutaneous
[19] S. Minkin, K. Kundhal, Likelihood-based experimental design for estimation
of ED50, Biometrics 55 (1999) 1030-1037.
[20] R. Murphy, J.E. Freedman, Morphine and clonidine activate different K+
channels on rat amygdala neurons, Eur. J. Pharmacol. 415 (2001) R1-3.
[21] T. Nishikawa, S. Dohi, Clinical evaluation of clonidine added to lidocaine
solution for epidural anesthesia, Anesthesiology 73 (1990) 853-859.
[22] D.M. Popping, N. Elia, E. Marret, M. Wenk, M.R. Tramer, Clonidine as an
adjuvant to local anesthetics for peripheral nerve and plexus blocks: a
meta-analysis of randomized trials, Anesthesiology 111 (2009) 406-415.
[23] J.N. Pratap, R.K. Shankar, T. Goroszeniuk, Co-injection of clonidine prolongs
the anesthetic effect of lidocaine skin infiltration by a peripheral action,
Anesth. Analg. 104 (2007) 982-983.
[24] A. Quartilho, H.P. Mata, M.M. Ibrahim, T.W. Vanderah, M.H. Ossipov, J. Lai,
F. Porreca, T.P. Malan, Jr., Production of paradoxical sensory hypersensitivity
by alpha 2-adrenoreceptor agonists, Anesthesiology 100 (2004) 1538-1544.
[25] A. Rochette, O. Raux, R. Troncin, C. Dadure, R. Verdier, X. Capdevila,
Clonidine prolongs spinal anesthesia in newborns: a prospective dose-ranging
study, Anesth. Analg. 98 (2004) 56-59.
methoxamine induce infiltrative anesthesia via alpha1-adrenoceptors in rats,
Acta. Pharmacol. Sin. 30 (2009) 1227-1236.
[27] T. Sjoberg, L. Norgren, K.E. Andersson, S. Steen, Comparative effects of the
alpha-adrenoceptor agonists noradrenaline, phenylephrine and clonidine in the
human saphenous vein in vivo and in vitro, Acta Physiol. Scand. 136 (1989)