DOI: 10.1177/10253823020090010115
2002; 9; 33
Promotion & Education
Lee-Lan Yen
study
Child and adolescent behaviour in long-term evolution (CABLE): a school-based health lifestyle
http://ped.sagepub.com
The online version of this article can be found at:
Published by:
http://www.sagepublications.com
On behalf of:
International Union for Health Promotion and Education
can be found at:
Promotion & Education
Additional services and information for
http://ped.sagepub.com/cgi/alerts Email Alerts: http://ped.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.co.uk/journalsPermissions.nav Permissions: http://ped.sagepub.com/cgi/content/refs/9/1_suppl/33 Citations
Child and adolescent behaviour
in long-term evolution (CABLE):
a school-based health lifestyle study
(Sameroff, et al., 1993). Moreover, thelonger the period of exposure to such behaviours, the greater the damage incurred. Therefore it is important when assessing the relationship between lifestyle and health, to comprehensively assess the various different habits that combine to form an individual’s routine daily life.
Pre-school, primary school and junior high school are times when many behaviours and habits are developed. Therefore it is a period of time that has an important influence on a person’s health. As an individual grows and develops, and the environment around them changes, some of their behaviours may also change, perhaps resulting in even more detrimental behaviours (Eyberg, 1998). A completed survey of Taipei City junior high school students showed that 98.9% consume fast food, 92.6% stay up late, 91.8% suppress urination, 90.4% watch TV or play video games for prolonged periods of time, 73.7% run in stairwells, 62.6% tell offensive jokes, and 58.1% break things when angry (Yen, et al.). Therefore it can be seen that such behaviours are quite common in seventh graders. Moreover, these harmful behaviours have the potential to be prevented or modified at an early stage.
Primary school students aged between 6 and 12, due to their cognitive and behavioural development, gradually become less reliant on their parents and begin to develop into individuals (Piaget, 1929). Therefore, this is also a period where they are more receptive to behavioural guidance. As a result, a longitudinal study that follows a study population from primary school to junior high school should be both economically viable and effective.
Overall objectives
Although some specific study objectives will vary slightly over time and with differing analytical perspectives, the following central objectives for the CABLE project will remain consistent.
1.To understand the distribution, aggregation and changes in health related behaviours of students.
Yearly cross-sectional data will be used to delineate the distribution, factor structure, and cluster characteristics of student health behavior. In addition, data will be compared on the basis of area, school, sex, grade and other factors.
Longitudinal data collected over several years will be used to observe the changes in health behaviours over time.
2.To investigate the influence
of parents on student health behaviour and health status.
There are four kinds of parental-student relationships: father-son,
father-daughter, mother-son, and mother-daughter. The transfer of behaviours, attitudes and habits from generation to generation, was assessed based on the distribution, aggregation, strength and mechanism of health behaviors.
3.To elucidate individual, family and school factors that influence student health behaviours.
After developing an understanding of the students’individual background, interpersonal relationships, family and school characteristics, multivariate statistical methods will be used to
❚Children and adolescents are an important asset for our country and society. Their health is tied to individual factors and the environment that they grow and develop in. After the dramatic decline in the infant mortality rate due to improvements in medical technology and environmental sanitation, the main focus of health promotion has shifted.
Although conducting research on the influence of such things as congenital and environmental factors on the quality of health of infants remains important (Golding, 1989; Farrow and Preece, 1995), investigation of the health status and behavioural development of children and adolescents from individual, family and school perspectives, has become an even more essential area of research
(Glendinning et al., 1997; Griffin, et al., 1999; Jones, et al., 1990; Karronen and Rimpela, 1996; McLellan et al., 1999; Paetsch and Bertrand, 1997; Sweeting and West, 1995). As a lifestyle based study following the development of children and their health related behaviours has never previously been conducted in Taiwan, the CABLE (Children and Adolescent Behaviours in Long-term Evolution: a school-based health lifestyle study) project, a prospective cohort based research model, was designed to collect and explore in-depth a multitude of health behavioural science related information.
According to health statistics for Taiwan, the leading causes of death in the 5-9 years age group, 10-14 years age group, and the 15-19 years age group include: accidental injury, malignant neoplasms, heart disease, and suicide (Dept. of Health, 1999). Many causes of death are intricately linked to a person’s lifestyle (McGinnis and Foege, 1993; CDC, 1996; US DHEW, 1979). For example, it has been well established that smoking, consumption of unhealthy foods, lack of exercise, alcohol abuse, drug abuse and accidental injury lead to both increased morbidity and mortality. The damage caused by a combination of harmful behaviours is much greater than that caused by a single behaviour alone
Yen Lee-Lan
1, Chen Likwang
2,
Lee Szu-Hsien
3, Hsiao Chuhsing
1,
Pan Ling-Yen
21. College of Public Health,
National Taiwan University
2. Division of Health Policy Research,
National Health Research Institutes
3. Department of Humanities
and Social Science,
National Defence Medical Center
Correspondence:
Prof. Lee-Lan Yen, Institute of Health
Policy and Management,
College of Public Health,
National Taiwan University
Email: lan@ha.mc.ntu.edu.tw
establish variables related to student health behavior. In addition, the direct and indirect relationships between these variables will be calculated.
4.To develop an understanding of the health status of students from biological, psychological and sociological perspectives and examine the relationship that this has with health behaviour.
The yearly cross-sectional data will be used to study student health from the three perspectives of biology, psychology and sociology, as well as further verify the relationship between these three areas and health. Data from the longitudinal study can be used to assess the changes in the students’health status over time.
Study design
The CABLE research proposal was passed by the National Health Research Institutes’examining committee in January 2000 and was commenced in March. The acronym “CABLE” was chosen as the project logo in order to
create a common term of reference among those in the research group and also for ease of communication when discussing the project with others. This logo was created from the first letter of each word of the study title. Cable, meaning electrical cable or broadband cable, is an essential item in modern daily life. This project incorporates certain basic qualities akin to those of cables such as length (long-term follow-up), heterogeneity (health is considered
from the different perspectives of biology, psychology, and sociology), and breadth (the scope of the project includes individual, family and school factors). If the world CABLE is read backwards as “ELBAC”, the
pronunciation is similar to the Chinese “ai-r-bai-ke”. This phrase means “an encyclopedia for loving and cherishing children”, emphasising that knowledge about how to care for children is something worth exploring and investigating. The CABLE research team incorporates a love of children with the ideal of health without limits.
The most ideal place for recruiting study subjects for a long-term study of child development is a primary school. As a result it was decided to select first grade primary school students in 2001 as the sample population and follow them consecutively over the next few years. As the reform of the education system has just been completed prior to 2001, this group of students will be the first to experience the first to ninth grade new education system. In order to gain an understanding of the different influences on student lifestyle and health status by
The CABLE study design
Year Grade 1 Grade 2 Grade 3 Grade 4 Grade 5 Grade 6 Grade 7 Grade 8
2001 A1 B1 C1 D1
2002 A2 B2 C2 D2
2003 A3 B3 C3 D3
2004 A4 B4 C4 D4
2005 A5 B5 C5 D5
A1-A5: The 1st cohort of 2001-2005 in Taipei City B1-B5: The 1st cohort of 2001-2005 in Hsinchu County C1-C5: The 2nd cohort of 2001-2005 in Taipei City D1-D5: The 2nd cohort of 2001-2005 in Hsinchu County
Figure 2
The CABLE logo.
Figure 1
Figure 3: The basic study framework of CABLE
Intrapersonal Level
1. Children
Demographics, Health and birth history,
Personal characteristics, Health beliefs,
School performance, Health behaviours,
Health lifestyle, Family structure, Family
SES, etc. etc.
2. Parents
Demographics, Marital status, Health
behaviours, Health lifestyle, etc.
Interpersonal Level
1. Family
Family Interaction, Family support,
Family relationships, etc.
2. School
Social support, Student-teacher
relationships, Peer interactions, etc.
Organisational Level
1. School
Size, Personnel, Facilities, Health
services, Policies, etc.
2. Community
Health and educational resources,
Economic index, etc.
Health lifestyle
1. Health risk behaviors
2. Health protecting
behaviors
3. Health promoting
behaviors.
Health Status
1. Physical health
2. Psychosocial health
the old and new educational systems, an additional study group of fourth graders was chosen. In addition, to compare differences between metropolitan and rural areas, the two locations of Taipei City and Hsinchu County were selected. The basic research design of the project is focused on young students as shown in Figure 2. In both Taipei and Hsinchu, a first grade and a fourth grade sample population was selected, giving a total of four sample groups for the two areas combined. Students and their parents will be surveyed yearly for a planned duration of 5 years.
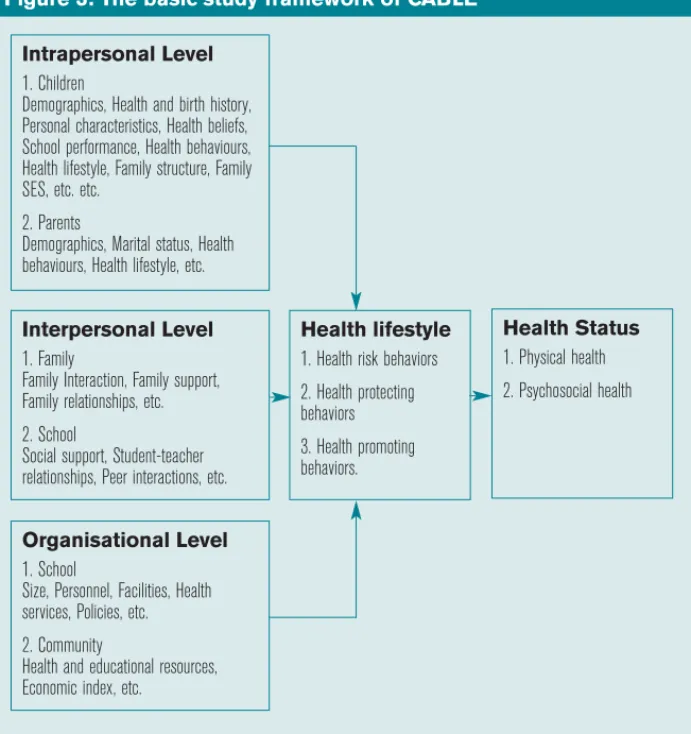
The study’s framework
The design of the CABLE study is based on the principles of the ecological model (Brofenbrenner, 1979) and is shown in Figure 3. The emphasis of the ecological model is that in-depth research should be carried out at a variety of different levels including individual, interpersonal, organisational, community and public policy. This multifaceted approach is a more effective and comprehensive way of looking at problems than by simply focusing on a single level (McLeroy, et al. 1988; Stokols, 1996). The research design
incorporates the two dependent variables of health lifestyle and health behaviour. The variable health lifestyle is made up of health harming behaviours, health protecting behaviours, and health promoting behaviours. The variable health status will be assessed according to biological, psychological and sociological perspectives. The three independent variables of individual factors (student and parental personal characteristics), interpersonal factors (the interpersonal relationships the student has at home and school), and
organisational factors (the structure and function of the family, school and community), will also be considered. During long-term follow up of the study group, additional information will be gathered yearly as illustrated by the long-term research framework in Figure 4. The basic study design will be as mentioned above, with only minor changes over time. Certain factors that are unlikely to change over time such as student and parental population characteristics, family structure, and school size and resources, will be referred to as independent or controlled variables.
Study subjects
There are 152 primary schools in Taipei City and 79 in Hsinchu County. As there are only a few private primary schools in these two areas (10 in Taipei City and 1 in Hsinchu County), and as the origin and family background of the students in these schools is quite dissimilar to the students in public schools, these private schools were excluded from the sample population. Based on the number of first grade students, schools were divided into small (50-199 students), medium-sized (200-399 students) and large (more than 400 students). Schools with less than 50 students were not included in the sample population due to insufficient numbers. After this, schools were randomly selected to participate in the survey. To ensure that the numbers of children chosen from each type of school was about equal it was decided to select 6 small schools, 2 medium-sized schools and 1 large school from each location. An approximate estimate of student numbers was calculated as being 70 x 6 (small schools), 200 x 2 (medium-sized
Study subjects of CABLE 2001 by grade and area
Subjects First grade Fourth grade
Taipei Hsinchu Sub-total Taipei Hsinchu Sub-total
Children: Population (n) 33,652 7,072 40,764 35,242 6,864 42,106 Sample selected (n) 1,950 1,634 3,584 1,842 1,770 3,612 Sample completed (n) 1,297 921 2,218 1,089 986 2,075 Response rate (%) 66.5 56.4 61.9 59.1 55.7 57.4 Children’s fathers (n) 991 736 1,727 867 837 1,704 Children’s mothers (n) 1,167 796 1,963 1,007 881 1,888
Table 1
Figure 4: The basic study framework of CABLE
Independent Variables
1. Children & Parent
3. School Factors
Factors
• Size
• Demographics
• Personnel
• Health history
• Facilities
• Personal characteristics
4. Controlled Factors
2. Family Factors
• Survey time
• Family structure
• Study area
Intermediate variables
Intrapersonal Factors
Time 1
Time i
Interpersonal Factors
Time 1
Time i
Organisational Factors
Time 1
Time i
Dependent variables
Health Lifestyle
Time 1
Time i
Health status
Time 1
Time i
schools), and 400 x 1 (large school) giving a total of 1,220 students. In addition, as two sets of students were chosen (a first grade and a fourth grade group) and there were two different locations, the overall number of students for the study was estimated as being 4880. In the event that some schools would refuse to participate in the study, double the amount of schools required were randomly selected. The grade one and grade four students and their parents were then selected as the study sample from a combined total of 18 schools in the 2 areas. As shown in Table 1, 3,584 first graders and 3,612 fourth graders were selected. However, only 2,218 first graders and 2,075 fourth graders received parental permission and completed their questionnaire forms. The completion rate was 61.9% for first graders and 57.4% for fourth graders. The completion rates for Hsinchu County at 56.4% for first graders and 55.7% for fourth graders, were lower than those of Taipei City at 66.5% for first graders and 59.1% for fourth graders.
Instruments
Initially, numerous discussions were held by the CABLE research team to establish the underlying principles of the project. The team then divided into three groups for literature review after which a draft questionnaire was drawn up. Both the student and parental questionnaires included parts about basic personal and family information, inter-family
relationships, and school life, as well as rating scales for health behaviour, psychological health, and social health. In addition, four different versions of the questionnaires were compiled for the different target groups of first graders, fourth graders, mothers and fathers. These draft questionnaires were reviewed and discussed at the routine weekly meetings and necessary alterations made. In addition,
pronunciation symbols (to help children read complicated Chinese characters) were added to the student
questionnaires. Ten persons with expertise in psychology, sociology, behavioural science, health education, and policy management, were requested to review and comment on the
questionnaires, as were several primary school teachers.
A pilot test was conducted from June to July 2001, using the revised questionnaires. A small-scale pilot study was carried out
on 5 first graders
and 5 fourth graders and their parents. A larger pilot study was also carried out on the students in an after school child care class from two institutes, with a total of 37 first graders and 79 fourth graders participating. In line with certain practical considerations and after analysis of the results from these pilot studies, the questionnaire forms were again modified and the final copy developed. As first graders have a limited attention span, their questionnaires were divided into a “vegetable” section and an “animal” section to be completed on two separate occasions. After the
questionnaires were collected, tests of validity and reliability were performed on the results to confirm the usability of the research instruments.
As the study is being carried out on children, it is necessary to gain the consent of the child’s parent or guardian before including the child in the study. Therefore, an informed consent form was designed that included information about the CABLE project, the methods of participation for students and their parents, data processing methods and strategies for protecting individual privacy. The CABLE proposal,
questionnaires and consent form were all reviewed and passed by the Human Research Medical Ethics Committee of the National Health Research Institutes.
Data collection
So that a long-term co-operative relationship could be formed with the schools involved in the study, the 18 schools were divided into 6 groups, with one CABLE research team member assigned to each group as a supervisor. In each school, a contact person was chosen (either the school administrator, guidance officer or nurse) to create a reliable communication channel between the CABLE team and the school. In addition, there were 60 university students recruited for the project who were given interview training. The main elements of this training included: introduction to the ideals of the CABLE project; explanation of the contents of the questionnaires; explanation of the survey procedure; and any important points to keep in mind when conducting the survey. In addition, as the CABLE research team uses the acting out of a play to present the survey, possible problems that may be
encountered during such a performance were discussed and any questions answered, so that ability and self-confidence could be strengthened. These interviewers were divided into six teams along with a supervisor, each team being responsible for three schools each. In the initial stage, through the assistance of the school’s contact person, first grade and fourth grade student teachers distributed the informed consent forms for parents to complete. Only those students whose parents agreed to their participation in the study were included in the student sample group. From October to December 2001, each survey team conducted surveys of their respective schools according to a schedule. It was decided to conduct the survey of first graders after November, as first graders need a period of time to adjust to school life and learning. The questionnaire forms and other related items used in the survey are all sent to the schools prior to commencing. When the survey team arrives at the school, a team of two people prepares the questionnaire forms, stationery, stickers, and demonstration posters (used when explaining the questionnaires) needed for all the classes. Before commencing, the assistance of the class teacher is sought to ensure that the students are prepared and have gone to the toilet. Then, the students whose parents have given consent are instructed to
congregate on one side of the room. The students whose parents did not give consent are either instructed to group on the other side of the room or are taken out of the classroom by the class teacher. When the survey is being conducted, one interviewer explains the
questionnaire and instructs the students how to complete it. The other interviewer is responsible for keeping order in the classroom. For first graders, an
interviewer reads out the questions and responses slowly, helping the students to answer the questions one by one. Fourth graders are left to fill in the
questionnaires by themselves, and are to raise their hands to ask questions if necessary. The students in the classroom that are not participating in the survey will be given paper by the interviewer for drawing or paper folding. Those students who are sitting quietly at their desk will be rewarded with a sticker. Interviewers are also responsible for calming down students who are being disruptive. The group supervisor will visit all classes
being interviewed and will provide any assistance needed.
The first graders complete the
questionnaire in two class periods. The fourth graders use one class period for questionnaire completion. The interviewers give the parent
questionnaire form to the students to take home as the completed student forms are being collected. The students are requested to give the questionnaire to their parents and hand in the
completed and signed form to their class teacher the following day. Students’ health information will be gathered from the school health records. Schools conduct their health examinations during the second semester, which in 2002 will be from February to May. As it takes some time for the student data files to be completed after the examinations, this information will be gathered from the school health database in September 2002, after the first semester of the new school year has begun.
Data management
After the questionnaires from the first year of the survey have been collected, the data will be coded, keyed in, examined for errors and corrected where necessary. Six computer files will then be created as follows: one for the first grade students, one for the parents of the first grade students, a combined first grade student-parent file, one for fourth grade students, one for the parents of fourth grade students and a combined fourth
grade student-parent file. Statistical analysis will be performed on this cross-sectional data on the basis of the research questions of the study and the characteristics of the variables. Apart from descriptive statistics, inferential statistical methods such as the chi-square test, ANOVA test, multiple regression analysis, logistic regression analysis, hierarchical regression analysis, cluster analysis, and path analysis will also be used.
As the study will be continued over consecutive years, as well as the six cross-sectional database files mentioned above, yearly chronological files will also be produced. After the second year of the study, hypotheses will be developed and verified through repeated
measurements and observing changes in trends. As the data from this study will become more and more complicated over time, the data management systems will be constructed continually.
Preliminary results on the
distribution of health behaviours
The analysis of the data collected from the CABLE project during 2001 will be able to answer many research questions posed by our study objectives. In view of the length limitations of this report, it will only include the results of the statistical analysis of health behaviours and will describe the distribution of health behaviours amongst first and fourth graders. Further reports will be compiled and released in the future. As shown in Table 2, many behaviours beneficial to
health such as eating breakfast, paying attention to safety whilst walking, drinking water, wearing a seatbelt, brushing teeth before sleeping, eating fruit and vegetables, wearing a helmet when on a motorcycle and washing hands before eating, were reported by about 70-80% of both first and fourth graders as being performed either frequently or always. However, the proportion of students participating in exercise (apart from school physical education classes) was lower, at about 50 to 60%.
The proportion of students reporting certain health behaviours was compared according to sex, area and year group (see Table 3). The variation in behaviours amongst first graders was relatively small, however that amongst fourth graders was larger. When comparing behavioural differences between boys and girls, apart from a few behaviours (the proportion of fourth graders who wear seatbelts and do exercise in Hsinchu County) that were more prevalent in boys, the proportion of girls practising positive health
behaviours was higher than that of boys. When the two study locations were compared, where differences were present, the rates of healthy behaviours were higher in Taipei City than in Hsinchu County. Comparison of the two different grades revealed that first graders were more likely than fourth graders to brush their teeth before sleep and eat breakfast. Fourth graders
Distribution of the percentages of children who always or frequently performed
behaviours positive to health by sex, area and grade, 2001
Behaviour First graders Fourth graders
Taipei Hsinchu Taipei Hsinchu
Boy Girl Sub-total Boy Girl Sub-total Total Boy Girl Sub-Total Boy Girl Sub-total Total
Walking carefully 81.5 81.8 81.7 80.6 82.1 81.4 81.6 80.5 88.9 84.6 72.3 80.3 76.0 80.5
Using seat-belts 77.9 80.4 79.1 73.4 77.3 75.3 77.5 83.5 85.4 84.5 75.7 69.7 72.9 79.0
Wearing motorcycle helmet 82.5 81.8 82.2 72.8 71.3 72.1 78.0 87.3 88.9 88.1 63.6 63.3 63.5 76.4
Washing hands before eating 71.2 77.8 74.4 72.6 78.5 75.5 74.9 74.4 79.4 76.8 66.3 77.0 71.4 74.3
Brushing teeth before sleeping 79.9 87.2 83.4 80.1 78.1 79.1 81.6 79.9 85.8 82.8 65.3 76.2 70.4 76.9
Eating breakfast 89.8 90.6 90.2 84.7 86.6 85.7 88.3 86.9 89.8 88.3 80.5 87.8 84.0 86.3
Eating fruit and vegetables 77.3 77.9 77.6 68.0 72.4 70.2 74.5 84.2 88.9 86.5 71.6 78.1 74.7 80.9
Drinking water 84.5 83.7 84.1 77.7 78.1 77.9 81.5 88.9 88.9 88.9 81.7 80.5 81.1 85.2
Doing exercise 61.0 61.4 61.2 59.4 63.9 61.6 61.4 65.9 63.6 64.8 63.3 54.2 59.0 62.0
Results of chi-square tests of the percentages of children who always or frequently
performed behaviours positive to health by sex, area and grade, 2001
Behaviour First graders Fourth graders
Taipei Hsinchu Taipei Hsinchu
By sex By sex By area By sex By sex By area By grade
Walking carefully — — — P<.001 P=.003 P<.001 — (M < F) (M < F) (T > H) Using seat-belts — — — — P=.036 P<.001 — (M >F) (T > H) Wearing motorcycle — — P<.001 — — P<.001 — helmet (T > H) (T > H) Washing hands P=.007 P=.039 — — P<.001 P=.005 — before eating (M<F) (M < F) (M < F) (T > H) Brushing teeth P<.001 — P=.010 P=.010 P<.001 P<.001 P<.001 before sleeping (M < F) (T > H) (M < F) (M < F) (T > H) (1 > 4) Eating breakfast — — P=.001 — P=.002 P=.004 P=.046 (T > H) (M < F) (T > H) (1 > 4) Eating fruit — — P<.001 P=.025 P=.019 P<.001 P<.001 and vegetables (T > H) (M < F) (M < F) (T > H) (1 < 4) Drinking water — — P<.001 — — P<.001 P<.001 (T > H) (T > H) (1 < 4) Doing exercise — — — — P=.004 P=.006 — (M > F) (T > H) —: Non-significant M: Male F: Female T: Taipei City H: Hsinchu county 1: 1stgrade 4: 4thgrade
Table 3
Distribution of the percentages of children who had on one or more occasions performed
behaviours negative to health by sex, area and grade, 2001
Behaviour First graders Fourth graders
Taipei Hsinchu Taipei Hsinchu
Boy Girl Sub-total Boy Girl Sub-total Total Boy Girl Sub-Total Boy Girl Sub-total Total
Staying up late 66.9 65.0 66.0 64.7 66.0 65.3 65.7 86.9 85.8 86.4 79.2 77.9 78.6 82.7
Eating food before sleep 60.8 57.7 59.3 58.9 52.8 55.8 57.8 64.6 65.8 65.2 71.9 74.5 73.1 69.0
Eating fast-food 67.0 59.9 63.5 62.0 53.0 57.6 61.1 69.7 65.1 67.4 63.6 60.6 62.2 64.9
Suppressing urination 49.5 43.2 46.4 50.8 47.7 49.2 47.6 54.4 54.9 54.7 51.5 56.8 54.0 54.4
Playing video games>2hrs 49.8 31.0 40.6 57.6 38.4 48.1 43.8 52.2 28.7 40.8 57.9 31.0 45.2 42.9
Watching TV >2hrs 61.4 51.6 56.6 64.2 63.9 64.0 59.7 63.3 62.7 63.0 74.7 72.5 73.6 68.1
Using vulgar language 36.9 22.9 30.1 31.2 21.5 26.4 28.6 67.0 55.1 61.2 62.6 51.6 57.4 59.4
Destroying things when angry 25.8 13.4 19.8 20.2 14.2 17.2 18.7 31.7 22.5 27.2 33.8 25.1 29.7 28.4
Fighting with others 40.8 25.2 33.2 32.3 23.3 27.9 30.8 56.8 49.3 53.4 57.8 54.1 56.0 54.6
Destroying public property 8.4 5.6 6.19 9.7 6.0 7.8 6.8 8.6 2.1 5.4 13.6 5.1 9.6 7.4
Smoking 7.1 4.9 6.0 15.7 6.4 11.1 8.1 8.0 4.7 6.4 12.5 3.7 8.3 7.3
Drinking alcohol 31.2 20.5 26.0 38.4 23.4 31.0 28.1 40.4 27.9 34.3 38.2 24.2 31.6 33.0
Suicidal ideas 14.6 7.3 11.1 13.7 9.9 11.9 11.4 26.6 26.6 26.6 11.0 13.5 12.2 19.8
were more likely than first graders to eat fruit and vegetables and drink water. Table 4 lists the behaviours harmful to health measured in the study. There were four unhealthy behaviours reported by more than 50% of first grade students, which were in order of incidence: staying up late, eating fast food, watching TV for more than two consecutive hours, and eating late at night. There were seven unhealthy behaviours present in more than 50% of fourth grade students, which were in order of incidence: staying up late, eating food late at night, watching TV for more than two consecutive hours, eating fast food, using vulgar language, getting involved in fights, and
suppressing urination. Although the other unhealthy habits such as playing computer games for more than two consecutive hours, drinking alcohol, breaking things when angry, and suicidal
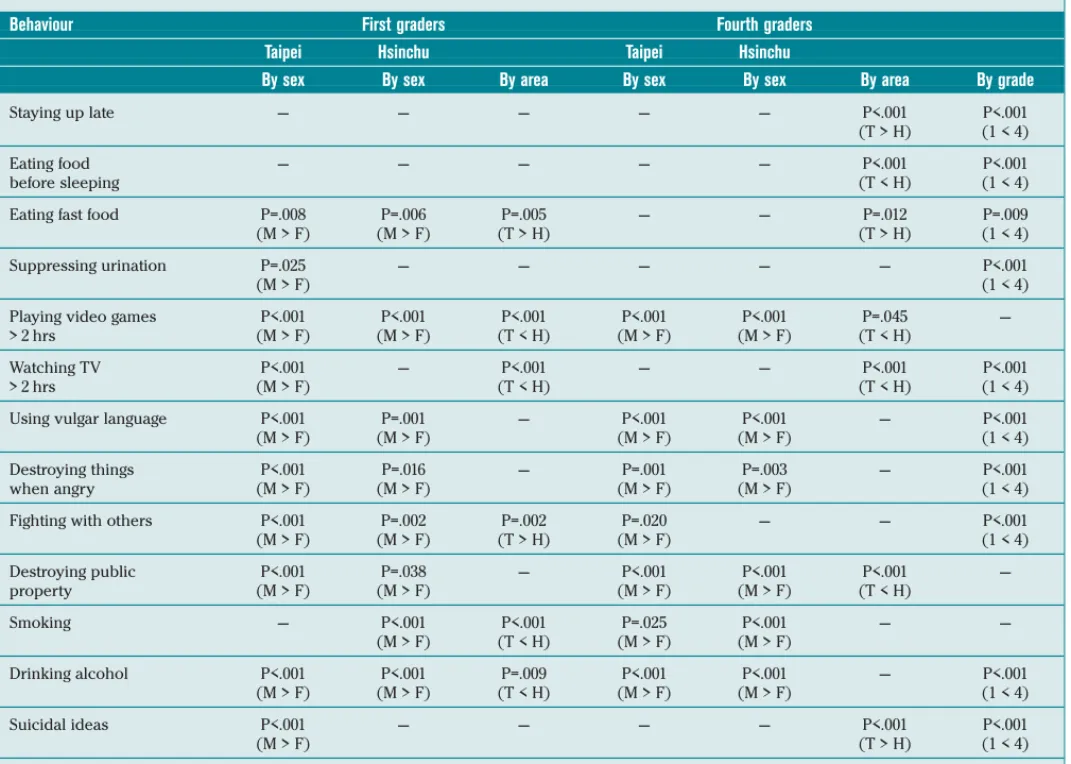
thoughts were reported by less than 50% of students, as 20 to 40% of students have experienced these behaviours, early attention to these areas is required to prevent future problems arising. When the results of negative behaviours were compared according to sex, area, and grade (see Table 5), many
differences were statistically significant. In general, the rates of negative behaviours were higher in boys than in girls. The proportion of first graders eating fast foods and getting into fights was higher in Taipei City than in Hsinchu County. However, the proportion of first grade students engaging in other unhealthy behaviours, including playing computer games for more than 2 consecutive hours, watching TV for more than 2 consecutive hours, smoking and drinking alcohol, was higher in Hsinchu County than in Taipei City. The
proportion of fourth graders staying up late, eating fast food, and experiencing suicidal thoughts was higher in Taipei City. However the proportion of fourth grade students eating late at night, playing computer games for more than 2 consecutive hours, watching TV for more than 2 consecutive hours and causing damage to private property, was higher in Hsinchu County. The proportion of students playing computer games for more than 2 consecutive hours, causing damage to public property, and smoking showed no difference between first and fourth graders. Other negative behaviours were more prevalent in fourth graders than in first graders.
Conclusions
More than 60% of students were already engaging in positive behaviours. However, as such behaviours both
Results of chi-square tests of the percentages of children who had on one or more
occasions performed behaviours negative to health by sex, area and grade, 2001
Behaviour First graders Fourth graders
Taipei Hsinchu Taipei Hsinchu
By sex By sex By area By sex By sex By area By grade
Staying up late — — — — — P<.001 P<.001
(T > H) (1 < 4)
Eating food — — — — — P<.001 P<.001
before sleeping (T < H) (1 < 4)
Eating fast food P=.008 P=.006 P=.005 — — P=.012 P=.009
(M > F) (M > F) (T > H) (T > H) (1 < 4)
Suppressing urination P=.025 — — — — — P<.001
(M > F) (1 < 4)
Playing video games P<.001 P<.001 P<.001 P<.001 P<.001 P=.045 — > 2 hrs (M > F) (M > F) (T < H) (M > F) (M > F) (T < H)
Watching TV P<.001 — P<.001 — — P<.001 P<.001
> 2 hrs (M > F) (T < H) (T < H) (1 < 4)
Using vulgar language P<.001 P=.001 — P<.001 P<.001 — P<.001 (M > F) (M > F) (M > F) (M > F) (1 < 4)
Destroying things P<.001 P=.016 — P=.001 P=.003 — P<.001
when angry (M > F) (M > F) (M > F) (M > F) (1 < 4)
Fighting with others P<.001 P=.002 P=.002 P=.020 — — P<.001
(M > F) (M > F) (T > H) (M > F) (1 < 4) Destroying public P<.001 P=.038 — P<.001 P<.001 P<.001 — property (M > F) (M > F) (M > F) (M > F) (T < H) Smoking — P<.001 P<.001 P=.025 P<.001 — — (M > F) (T < H) (M > F) (M > F) Drinking alcohol P<.001 P<.001 P=.009 P<.001 P<.001 — P<.001 (M > F) (M > F) (T < H) (M > F) (M > F) (1 < 4) Suicidal ideas P<.001 — — — — P<.001 P<.001 (M > F) (T > H) (1 < 4)
—: Non-significant M: Male F: Female T: Taipei City H: Hsinchu county 1: 1stgrade 4: 4thgrade
protect and promote health the higher the number of students engaging in them the better. More concerning was that even for such behaviours as wearing a seatbelt in the car and wearing a helmet when on a motorcycle that already are compulsory by law, there were still 10% to 20% of students in Taipei and 20% to 30% of students in Hsinchu who did not abide by such regulations. In addition, 10% to 40% of students did not carry out such behaviours as washing hands before eating, brushing teeth before sleeping, eating breakfast, eating fruit and vegetables, drinking water, and doing exercise. These activities are some of an individual’s most basic behaviours and are beneficial to health. It would be worthwhile to further investigate the reasons why these students do not perform such behaviours.
As for behaviours harmful to health such as staying up late, eating late at night, eating fast food, suppressing urination, watching TV for more than 2 consecutive hours, using vulgar language, breaking things when angry, getting involved in fights with others, drinking alcohol and suicidal ideation, these were all more common in fourth grade students than in
first graders. Boys were also much more likely to engage in such negative behaviours than girls. There were also some differences noticed in the prevalence of such behaviours between Taipei City and Hsinchu County. It is therefore evident that their exist certain hidden risk factors that have the potential to threaten child health. An individual’s personal habits are not created in an instant, but rather are accumulated slowly over a period of time as the same activity is repeated over and over. Once a behaviour has become a habit and has been incorporated into a person’s daily routine, it is extremely difficult to alter such a behaviour within a short period of time. The effort required and cost involved in encouraging children to develop good habits while they are young or in modifying unhealthy behaviours before they have become well established, is much less than that required to assist adults whose
behaviours are already entrenched. It is an important responsibility of the family, schools and society to provide young people, including pre-school, primary school and junior high school students,
with opportunities to establish healthy lifestyles during their youth, particularly because the earlier such healthy lifestyles are developed the better it is for a person’s health.
Continued analysis of the cross-sectional and longitudinal data from the CABLE study will bring forth even more in-depth empirical data. As the CABLE project is the first such study in Taiwan to conduct lifestyle based research by following the health behaviours and health status of children over a prolonged period, we predict that the study will be of benefit to both those working and conducting research in the fields of public health policy,
behavioural science, health education, psychology and sociology. Many aspects of the study will be of use to the above groups including research design, implementation methods, data filing, statistical analysis, and theory development. The results and recommendations of this research project can be used for the design of child and adolescent health public policy, as well as for preventive educational activities and intervention programmes.