Date 2014/ October/30
Type of manuscript: Original article
New title: Increased relative risk of acute pancreatitis in zolpidem users Running head: zolpidem and acute pancreatitis
Authors' full names:
Shih-Wei Lai 1,2, Cheng-Li Lin 3,4, Kuan-Fu Liao 5,6
1School of Medicine, China Medical University and 2Department of Family
Medicine, China Medical University Hospital, Taichung, Taiwan
3Department of Public Health, China Medical University and 4Management
Office for Health Data, China Medical University Hospital, Taichung, Taiwan 5Graduate Institute of Integrated Medicine, China Medical University and
6Department of Internal Medicine, Taichung Tzu Chi General Hospital,
Taichung, Taiwan
Corresponding author: Kuan-Fu Liao, Department of Internal Medicine, Taichung Tzu Chi General Hospital, No.66, Sec. 1, Fongsing Road, Tanzi District, Taichung City, 427, Taiwan
Phone: 886-4-2205-2121 Fax: 886-4-2203-3986
E-mail: [email protected]
ABSTRACT
Objectives. The aim of this study was to investigate the relationship between
zolpidem use and the risk of acute pancreatitis in Taiwan. Methods. In this population-based case-control study using the database from the Taiwan National Health Insurance Program from 2000 to 2011, we selected 4535 subjects aged 20-84 years with the first episode of acute pancreatitis as cases and 18140 subjects without acute pancreatitis matched for sex, age and index year as controls. Immediate use of zolpidem was defined as subjects who received at least 1 prescription for zolpidem within 7 days before the date of diagnosing acute pancreatitis. The absence of zolpidem prescription was defined as never use. The odds ratio (OR) and 95% confidence interval (CI) were used to evaluate the risk of acute pancreatitis associated with zolpidem use and other comorbidities. Results. After adjustment for
confounding factors, the multivariable logistic regression model demonstrated that the adjusted OR of acute pancreatitis was 7.20 for immediate use of zolpidem (95% CI 5.81, 8.92), when compared to those with never use of zolpidem. In further analysis, as a reference of subjects with never use of zolpidem and without any of these comorbidities including alcoholism, biliary stone, diabetes mellitus, hepatitis B, hepatitis C and hypertriglyceridemia, the adjusted OR was 18.04 in those with
immediate use of zolpidem and without any comorbidity (95% CI 12.71, 25.60). The OR increased to 30.32 in subjects with immediate use of zolpidem and with any comorbidity (95% CI 23.71, 38.79). Conclusions. Patients actively using zolpidem are at 7-fold increased odds of acute pancreatitis. Clinicians should be more cautious of acute pancreatitis risk among patients with any comorbidity studied when
prescribing zolpidem.
INTRODUCTION
Acute pancreatitis is a critical public health threat due to its severe morbidity and mortality. Epidemiological studies have published some risk factors associated with the risk of acute pancreatitis. In addition, extensive evidence has illustrated that despite a rare cause, a variety of drugs have pancreatic toxicity to be associated with the risk of acute pancreatitis , but zolpidem has never been mentioned.
Zolpidem is the most frequently used non-benzodiazepine sedative-hypnotic drug in Taiwan. To date, significant morbidities associated with zolpidem use have been reported, including adverse pregnancy outcomes, cancer, stroke and injury, but acute pancreatitis has never been mentioned.
Although no case report was published about zolpidem use and the risk of acute pancreatitis, U.S. Food and Drug Administration (FDA) has reported that since 2001 to 2012, 81 people (0.33%) had acute pancreatitis among 24300 people taking zolpidem with side effects. To date, no causal relationship between zolpidem use and the risk of acute pancreatitis is determined in U.S. FDA report. There is lack of strong evidence based on systematic studies to support the relationship between zolpidem use and the risk of acute pancreatitis. If the relationship really exists, clinicians should be more cautious of acute pancreatitis risk when prescribing zolpidem. Given
extensive use of zolpidem in Taiwan, we designed a case-control study to examine the plausible hypothesis linking zolpidem use and the risk of acute pancreatitis.
METHODS Data Sources
We conducted a population-based case-control study using the nationwide
representative database of the Taiwan National Health Insurance Program. Briefly, the insurance program began in March 1995 and nearly covered 99% of 23 million
people living in Taiwan. The program provided medications, outpatient, inpatient and emergency services. Disease was diagnosed with the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9 codes). The program has been well documented in previous studies. This study was approved by the
Institutional Review Board (IRB) of China Medical University and Hospital (CMU-REC-101-012).
Participants
The index date was defined as the date of diagnosing acute pancreatitis. Subjects aged 20-84 years with the first episode of acute pancreatitis between 2000 and 2011 (ICD-9 codes 577.0) were selected as the case group. To increase the statistical power, for each case identified, four subjects without acute pancreatitis were randomly selected as the control group. Both groups were matched by sex, age (every 5 year) and index year of diagnosing acute pancreatitis. Subjects with chronic pancreatitis or pancreatic cancer before the date of diagnosing acute pancreatitis were excluded from the study (Figure 1).
Definition of zolpidem exposure
Zolpidem is a short-acting agent with a short elimination half-life (approximately 2.1-2.4 hours). Its metabolite is not active and it does not have an accumulating effect. In U.S. FDA report, the timing from using zolpidem to developing acute pancreatitis mainly occurred within 1 month.{eHealthMe study from FDA and social media reports, [cited in 2014 April] #42} In this study, subjects receiving no zolpidem prescription within 1 month but receiving at least 1 zolpidem prescription > 1 month before the date of diagnosing acute pancreatitis were excluded from the study. Therefore, only subjects with zolpidem prescriptions within 1 month before the date of diagnosing acute pancreatitis were included. Immediate use of zolpidem was defined as subjects who received at least 1 prescription for zolpidem within 7 days
before the date of diagnosing acute pancreatitis or the corresponding date for control subjects. Early use of zolpidem was defined as subjects who did not receive a
prescription within 7 days but at least received 1 prescription for zolpidem within 8 to 14 days before the date of diagnosing acute pancreatitis or the corresponding date for control subjects. Late use of zolpidem was defined as subjects who did not receive a prescription within 14 days but at least received 1 prescription for zolpidem within 15 to 30 days before the date of diagnosing acute pancreatitis or the corresponding date for control subjects. The absence of zolpidem prescription was defined as never use.
Comorbidity assessment
Claims data were used to identify comorbidities potentially associated with the risk of acute pancreatitis before index date, including alcoholism, biliary stone, diabetes mellitus, hepatitis B, hepatitis C and hypertriglyceridemia. All comorbidities were diagnosed with ICD-9 codes. In order to avoid subjects who were mistakenly diagnosed or mistakenly coded by accident, only subjects who had at least 3 consensus same diagnoses in the ambulatory care or at least 1 hospitalization diagnosis were included to make sure the diagnosis validity. History of benzodiazepines prescription was also included.
Statistical Analysis
We first compared the differences between cases and controls for distribution of demographic status, zolpidem use, benzodiazepines use and comorbidities by the Chi-square test. In the beginning, all covariables were included in the univariable
unconditional logistic regression model. Only covariables found significantly in the univariable model were further included in the multivariable unconditional logistic regression model to evaluate the odds ratio (OR) and 95% confidence interval (CI) for the risk of acute pancreatitis. We further evaluated the interaction effect between immediate use of zolpidem and comorbidities on risk of acute pancreatitis. The
probability value < 0.05 was considered statistically significant (SAS software version 9.1, SAS Institute Inc., Cary, North Carolina, USA).
RESULTS
Characteristics of the study population
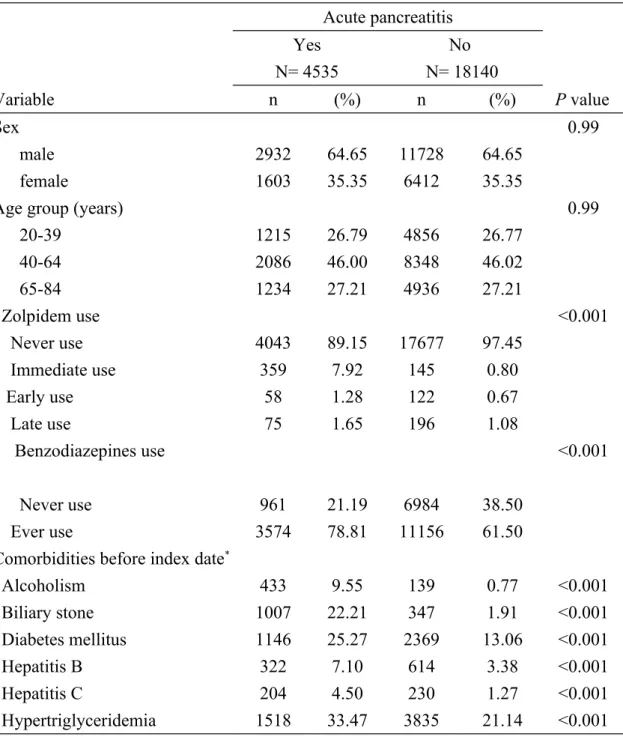
The demographic status, zolpidem use, benzodiazepines use and comorbidities between the case group and the control group are compared in Table 1. There were 4535 cases of acute pancreatitis and 18140 control subjects with equal distributions in sex and age. The mean ages (standard deviation) were 52.64 (16.53) years in the case group and 52.56 (16.57) years in the control group. Cases had higher proportions of ever use of zolpidem, ever use of benzodiazepines, alcoholism, biliary stone, diabetes mellitus, hepatitis B, hepatitis C and hypertriglyceridemia (P value of Chi-square test <0.001 for all).
Risk of acute pancreatitis associated with zolpidem use estimated by odds ratio and 95% confidence interval
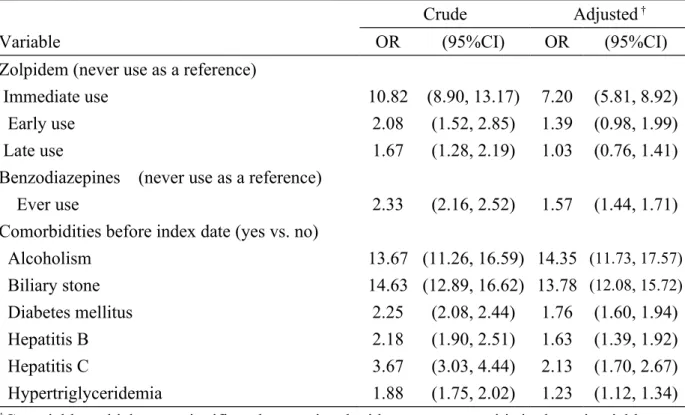
After adjustment for potential confounding factors, the multivariable unconditional logistic regression model demonstrated that the adjusted OR of acute pancreatitis was 7.2 for immediate use of zolpidem (95% CI 5.81, 8.92), with reference to never use of zolpidem (Table 2). The ORs gradually decreased to 1.39 for early use of zolpidem (95% CI 0.98, 1.99) and down to 1.03 for late use of zolpidem (95% CI 0.76, 1.41), but without statistical significance. Ever use of benzodiazepines (OR1.57, 95% CI 1.44, 1.71), alcoholism (OR 14.35, 95% CI 11.73, 17.57), biliary stone (OR 13.78, 95% CI 12.08, 15.72), diabetes mellitus (OR 1.76, 95% CI 1.60, 1.94), hepatitis B (OR 1.63, 95% CI 1.39, 1.92), hepatitis C (OR 2.13, 95% CI 1.70, 2.67) and
hypertriglyceridemia (OR 1.23, 95% CI 1.12, 1.34) were other factors associated with acute pancreatitis.
of zolpidem and comorbidities
In further analysis, as a reference of subjects with never use of zolpidem and without any of these comorbidities including alcoholism, biliary stone, diabetes mellitus, hepatitis B, hepatitis C and hypertriglyceridemia, the OR was 18.04 in those with immediate use of zolpidem and without any comorbidity (95% CI 12.71, 25.60). The OR increased to 30.32 in subjects with immediate use of zolpidem and with any comorbidity (95% CI 23.71, 38.79). The OR was 5.00 in subjects with never use of zolpidem and with any comorbidity (95% CI 4.62, 5.40). This indicates that there is a strong interaction effect between immediate use of zolpidem and comorbidities on risk of acute pancreatitis (P value of interaction test < 0.001, Table 3).
Average daily dose of immediate use of zolpidem and risk of acute pancreatitis
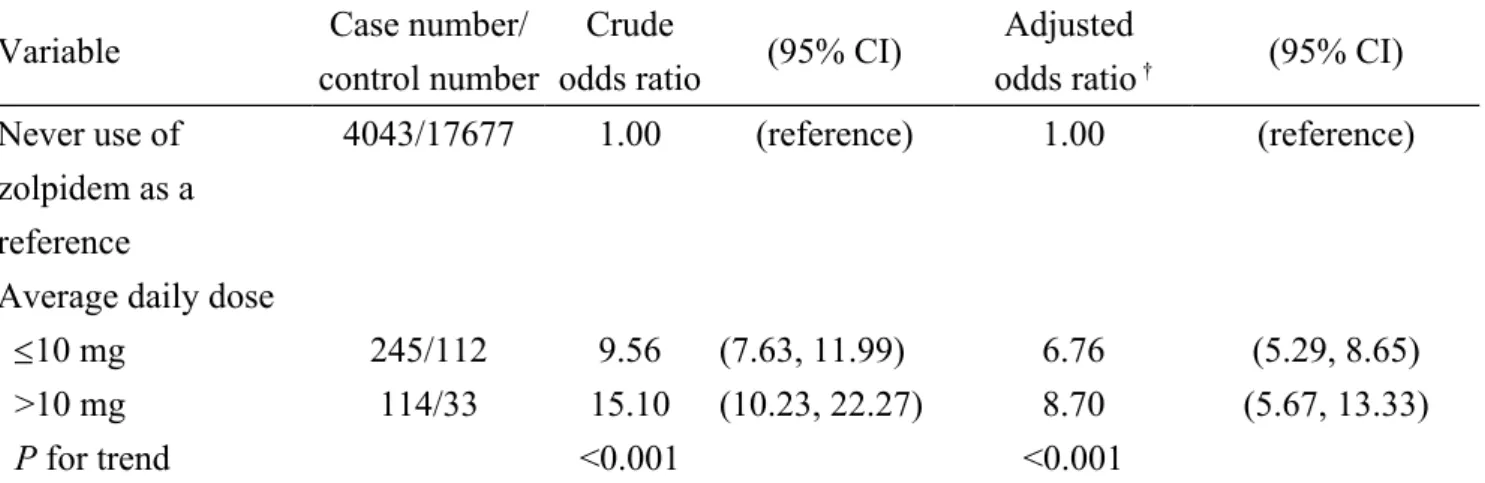
We performed an analysis on the dose-related effect among the group with immediate use of zolpidem (Table 4). The average daily dose of zolpidem was measured by using the total prescribed dose divided by total number of days supplied. Because the commonly used form of zolpidem is 10mg per tablet in Taiwan, we used 10mg as a cut-off point. We categorized study subjects into two groups (high dose and low dose groups). Both high and low doses of zolpidem were associated with increased odds of acute pancreatitis, but subjects using high dose of zolpidem had higher odds ( OR 8.70 vs. 6.76, P value of test for trend <0.001). It indicates that there is a dose-dependent effect of zolpidem on risk of acute pancreatitis.
DISCUSSION
In this population-based case-control study, we found that immediate use of zolpidem was significantly associated with increased odds of acute pancreatitis (OR 7.2), but
there was no significant association between early use or late use of zolpidem and acute pancreatitis. This means that only patients actively using zolpidem would have the risk of acute pancreatitis, but patients who once used zolpidem but are not using it now do not have the risk. To date, a wide variety of drugs have pancreatic toxicity to be associated with the risk of acute pancreatitis. However, it is relatively difficult to prove the causal relationship between pancreatic inflammation and the offending drug. To the best of our knowledge, no case report or other pharmacoepidemiological study has examined the relationship between zolpidem use and the risk of acute pancreatitis. Only U.S. FDA has reported this issue. Whereas the exact mechanism of acute pancreatitis associated with zolpidem use could not be completely illustrated from this observational study and previous studies, we reviewed the literature to explain the potential mechanism. Zolpidem is a short-acting agent with a short elimination half-life (approximately 2.1-2.4 hours). Its metabolite is not active and it does not have an accumulating effect. Therefore, we think zolpidem may have an acute and direct toxic effect on the pancreas, which further precipitates the pancreatic inflammation. That can partially explain why only patients who actively used
zolpidem may have the risk of acute pancreatitis, but those who once used zolpidem but are not using it now do not have the risk. We also observed that among the group with immediate use of zolpidem, patients with average daily dose >10 mg had higher odds of acute pancreatitis than those with average daily dose 10 mg did (OR 8.70 vs. 6.76 in Table 4). This means that there is a dose-dependent effect of zolpidem on risk of acute pancreatitis. In addition, immediate use of zolpidem alone had obviously higher odds of acute pancreatitis than any comorbidity alone did (OR 18.04 vs. 5.00 in Table 3). Therefore, this further suggests that patients actively using zolpidem are associated with increased odds of acute pancreatitis, even lack of any comorbidity
studied, and the higher the dose, the greater the odds.
In further analysis, we found that the odds ratio increased to 30.32 in patients with immediate use of zolpidem and with any comorbidity (Table 3). This means that there is a strong interaction effect between immediate use of zolpidem and comorbidities on risk of acute pancreatitis. Thus, clinicians should be more cautious of acute
pancreatitis risk among patients with any comorbidity studied when prescribing zolpidem.
Some points due to inherent limitation of this database should be noted. First, theoretically, we should analyze patients who took only zolpidem and no other drugs in this database, but the case number needed is too small to be analyzed. Moreover, we cannot correct for all drugs that have ever been associated with acute pancreatitis. We only can present the relative risk of acute pancreatitis in zolpidem users, not absolute risk. Second, the exact cause of acute pancreatitis was not recorded in this database. Similarly, there was not record of severity and mortality of acute
pancreatitis in this database. Whether zolpidem use is an independent risk factor for the severe form of acute pancreatitis or increased mortality could not be determined in this study. Third, because of inherent limitation of an observational study, the role of zolpidem in the pathogenesis of acute pancreatitis could not be determined and the causal-effect relationship could not be addressed in a case-control study. Forth, although zolpidem is a frequently used non-benzodiazepine sedative-hypnotic drug in Taiwan, the exact indication for zolpidem prescription was not recorded in this database. Therefore, we cannot make sure whether zolpidem use or the underlying cause for zolpidem prescription is associated with acute pancreatitis or not. It
indicates a future research direction about the relationship between sleep disorder or mental disease and acute pancreatitis. Fifth, it is unclear how much zolpidem the
patients actually ingested. In sub-analysis, the mean duration of zolpidem therapy was 378.36 days in immediate use group (standard deviation = 669.28), 845.09 days in early use group (standard deviation = 1142.17) and 556.24 days in late use group (standard deviation = 918.21). The early use group seemed to have longer mean duration of zolpidem therapy. However, in Table 2, only immediate use of zolpidem was significantly associated with increased odds of acute pancreatitis, but there was no significant association between early use or late use of zolpidem and acute pancreatitis. This means the zolpidem-related inflammatory side effect on the
pancreas is not associated with total duration of zolpidem therapy, but associated with whether actively using zolpidem or not. Sixth, given the strong association between immediate use of zolpidem and the risk of acute pancreatitis, we still cannot rule out the possibility of unfounded confounders that could not be adjusted by a multivariable model. Moreover, the sample size of this study allows for increased statistical power (22675 subjects in total). There were significant differences in comorbidities between the case group and the control group. This indicates that comorbidities included were really associated with the risk of acute pancreatitis, which was compatible with previous studies.
We conclude that patients actively using zolpidem are at 7-fold increased odds of acute pancreatitis. Whether zolpidem has a direct pancreatic toxicity to be associated with acute pancreatitis needs further investigation.
Funding
This study was supported in part by Taiwan Ministry of Health and Welfare Clinical
Trial and Research Center of Excellence (MOHW103-TDU-B-212-113002). The funding agency did not influence the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Shih-Wei Lai: (1) substantial contributions to the conception of this article; (2) planned and conducted the study; (3) initiated the draft of the article and critically revised the article.
Cheng-Li Lin: (1) conducted data analysis; (2) critically revised the article. Kuan-Fu Liao: (1) planned and conducted the study; (2) participated in data interpretation; (3) critically revised the article.
Conflict of Interest Statement
REFERENCES
Chung SD, Lin CC, Wang LH, Lin HC, Kang JH (2013) Zolpidem Use and the Risk of Injury: A Population-Based Follow-Up Study. PLoS One 8: e67459. Darcourt G, Pringuey D, Salliere D, Lavoisy J (1999) The safety and tolerability of
zolpidem--an update. J Psychopharmacol 13: 81-93.
eHealthMe study from FDA and social media reports ( [cited in 2014 April]) Review: could zolpidem cause acute pancreatitis?
http://www.ehealthme.com/print/ds16535169.
Hsiao F-Y, Hsieh P-H, Gau C-S (2013) Ten-year trend in prescriptions of z-hypnotics among the elderly: A nationwide, cross-sectional study in Taiwan. Journal of Clinical Gerontology and Geriatrics 4: 37-41.
Huang WS, Tsai CH, Lin CC, Muo CH, Sung FC, Chang YJ, Kao CH (2013) Relationship between zolpidem use and stroke risk: a Taiwanese population-based case-control study. J Clin Psychiatry 74: e433-8.
Kao CH, Sun LM, Liang JA, Chang SN, Sung FC, Muo CH (2012) Relationship of zolpidem and cancer risk: a Taiwanese population-based cohort study. Mayo Clin Proc 87: 430-6.
Lai SW, Chen PC, Liao KF, Muo CH, Lin CC, Sung FC (2012a) Risk of
hepatocellular carcinoma in diabetic patients and risk reduction associated with anti-diabetic therapy: a population-based cohort study. Am J
Gastroenterol 107: 46-52.
Lai SW, Liao KF, Chen PC, Tsai PY, Hsieh DP, Chen CC (2012b) Antidiabetes drugs correlate with decreased risk of lung cancer: a population-based observation in Taiwan. Clin Lung Cancer 13: 143-8.
Lai SW, Liao KF, Liao CC, Muo CH, Liu CS, Sung FC (2010) Polypharmacy correlates with increased risk for hip fracture in the elderly: a population-based study. Medicine (Baltimore) 89: 295-9.
Lai SW, Muo CH, Liao KF, Sung FC, Chen PC (2011) Risk of acute pancreatitis in type 2 diabetes and risk reduction on anti-diabetic drugs: a population-based cohort study in Taiwan. Am J Gastroenterol 106: 1697-704.
Liao KF, Lai SW, Li CI, Chen WC (2012) Diabetes mellitus correlates with increased risk of pancreatic cancer: a population-based cohort study in Taiwan. J Gastroenterol Hepatol 27: 709-13.
pancreatitis. JAMA Intern Med 173: 162-4.
Su TP, Chen TJ, Hwang SJ, Chou LF, Fan AP, Chen YC (2002) Utilization of psychotropic drugs in Taiwan: an overview of outpatient sector in 2000. Zhonghua Yi Xue Za Zhi (Taipei) 65: 378-91.
Swainston Harrison T, Keating GM (2005) Zolpidem: a review of its use in the management of insomnia. CNS Drugs 19: 65-89.
Trivedi CD, Pitchumoni CS (2005) Drug-induced pancreatitis: an update. J Clin Gastroenterol 39: 709-16.
Vinklerova I, Prochazka M, Prochazka V, Urbanek K (2010) Incidence, severity, and etiology of drug-induced acute pancreatitis. Dig Dis Sci 55: 2977-81.
Wang LH, Lin HC, Lin CC, Chen YH (2010) Increased risk of adverse pregnancy outcomes in women receiving zolpidem during pregnancy. Clin Pharmacol Ther 88: 369-74.
Table 1. Descriptive characteristics, zolpidem use and comorbidities between acute pancreatitis cases and control subjects
Acute pancreatitis Yes N= 4535 No N= 18140 Variable n (%) n (%) P value Sex 0.99 male 2932 64.65 11728 64.65 female 1603 35.35 6412 35.35
Age group (years) 0.99
20-39 1215 26.79 4856 26.77 40-64 2086 46.00 8348 46.02 65-84 1234 27.21 4936 27.21 Zolpidem use <0.001 Never use 4043 89.15 17677 97.45 Immediate use 359 7.92 145 0.80 Early use 58 1.28 122 0.67 Late use 75 1.65 196 1.08 Benzodiazepines use <0.001 Never use 961 21.19 6984 38.50 Ever use 3574 78.81 11156 61.50
Comorbidities before index date*
Alcoholism 433 9.55 139 0.77 <0.001 Biliary stone 1007 22.21 347 1.91 <0.001 Diabetes mellitus 1146 25.27 2369 13.06 <0.001 Hepatitis B 322 7.10 614 3.38 <0.001 Hepatitis C 204 4.50 230 1.27 <0.001 Hypertriglyceridemia 1518 33.47 3835 21.14 <0.001
Data are presented as the number of subjects in each group, with percentages given in parentheses.
Chi-square test comparing subjects with and without acute pancreatitis
Table 2. Odds ratio and 95% confidence interval of acute pancreatitis associated with zolpidem use and comorbidities
Crude Adjusted †
Variable OR (95%CI) OR (95%CI)
Zolpidem (never use as a reference)
Immediate use 10.82 (8.90, 13.17) 7.20 (5.81, 8.92)
Early use 2.08 (1.52, 2.85) 1.39 (0.98, 1.99)
Late use 1.67 (1.28, 2.19) 1.03 (0.76, 1.41)
Benzodiazepines (never use as a reference)
Ever use 2.33 (2.16, 2.52) 1.57 (1.44, 1.71)
Comorbidities before index date (yes vs. no)
Alcoholism 13.67 (11.26, 16.59) 14.35 (11.73, 17.57) Biliary stone 14.63 (12.89, 16.62) 13.78 (12.08, 15.72) Diabetes mellitus 2.25 (2.08, 2.44) 1.76 (1.60, 1.94) Hepatitis B 2.18 (1.90, 2.51) 1.63 (1.39, 1.92) Hepatitis C 3.67 (3.03, 4.44) 2.13 (1.70, 2.67) Hypertriglyceridemia 1.88 (1.75, 2.02) 1.23 (1.12, 1.34)
†Covariables which were significantly associated with acute pancreatitis in the univariable
unconditional logistic regression model were further analyzed by the multivariable unconditional logistic regression model.
Additionally adjustment for benzodiazepines use, alcoholism, biliary stone, diabetes mellitus, hepatitis B, hepatitis C and hypertriglyceridemia
Table 3. Odds ratio and 95% confidence interval of acute pancreatitis estimated by interaction effect between immediate use of zolpidem and comorbidities
Never use Immediate use
Variable Odds ratio (95% CI)† Odds ratio (95% CI)†
No comorbidity As a reference 18.04 (12.71, 25.60)
Presence of any comorbidity *
5.00 (4.62, 5.40) 30.32 (23.71, 38.79)
†Adjusted for benzodiazepines use
*Comorbidities including alcoholism, biliary stone, diabetes mellitus, hepatitis B, hepatitis C
and hypertriglyceridemia
The interaction between immediate use of zolpidem and presence of any comorbidity was significant (P value for interaction <0.001).
Table 4. Odds ratio and 95% confidence interval of acute pancreatitis in relation to average daily dose of immediate use of zolpidem by logistical regression model
Variable Case number/
control number
Crude
odds ratio (95% CI)
Adjusted
odds ratio † (95% CI)
Never use of zolpidem as a reference
4043/17677 1.00 (reference) 1.00 (reference)
Average daily dose
10 mg 245/112 9.56 (7.63, 11.99) 6.76 (5.29, 8.65)
>10 mg 114/33 15.10 (10.23, 22.27) 8.70 (5.67, 13.33)
P for trend <0.001 <0.001
† Adjusted for benzodiazepines use and comorbidities including alcoholism, biliary stone, diabetes