行政院國家科學委員會專題研究計畫 成果報告
Caveolin-1 造成癌細胞多重抗藥性機制的探討
計畫類別: 個別型計畫 計畫編號: NSC93-2314-B-002-217- 執行期間: 93 年 08 月 01 日至 94 年 07 月 31 日 執行單位: 國立臺灣大學醫學院內科 計畫主持人: 何肇基 共同主持人: 楊泮池 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 94 年 10 月 30 日
Introduction:
Although chemotherapy has improved the prognosis of lung cancer patients, there
are still many patients who have initial resistance to chemotherapy or develop the
drug resistance after several courses of chemotherapy (1). Understanding and control
of drug resistance has become an important improvement in cancer therapy.
Caveolin-1, a 21- to 24-kD protein, is the principal component of caveolae, which
are special invaginated microdomains of the plasma membrane present in most
mammalian cells.(2) The role of caveolin-1 in cancer cells is quite diverse. Caveolin-1
functions as a tumor suppressor by contact inhibition of signaling molecules by its
scaffolding domain.(3) Up-regulation of caveolin-1 prevents anchorage-independent
growth (4) and sensitizes apoptotic machinery through phosphatidylinositol 3 kinase
(PI-3K) in different cells.(5) However, there is also substantial evidence that
caveolin-1 expression increases metastatic ability and increases the survival rate in
prostate cancer and other malignancies. (6, 7)
Recent studies have shown that acquisition of the MDR phenotype is associated
with the up-regulation of lipids including glucocylceramide (GlcCer) and cholesterol,
which constitute lipid rafts and caveolae. (8) Some multidrug resistant cancer cell
lines express very high caveolin-1 levels.(8-10) The up-regulation of caveolin-1 is
cancer cells.(9, 10) In addition, P-glycoprotein, a plasma membrane drug efflux
ATPase confering multidrug resistance, is enriched in caveolae within some MDR
cancer cells. However, caveolin-1 expression is not necessarily correlated with
P-glycoproein, because caveolin-1 is up-regulated in MDR cells with little
P-glycoprotein expression.
Cisplatin based combination chemotherapy displays significant anti-tumor activity
against lung cancer and remains one of the regimens in lung cancer patients. Although
caveolin-1 is over-expressed in cisplatin treated cancer cells compared with parent
cells, there is no direct correlation between caveolin-1 expression and cisplatin
resistance. In this study, we observe the cavoelin-1 and P-glycoprotein expression in
the paraffin-embedded specimens from pathologically proven lung cancer patients
who received cisplatin plus gencitabine after biopsy. Correlation between caveolin-1
expression and the chemotherapy resistance is established.
Materials and Methods:
Cell Culture
Cells were grown in Dulbecco’s modified Eagle’s medium supplemented with
10% heat-inactivated fetal bovine serum and 2 mM L-glutamine at 37oC, 5% CO2 in a
humidified incubator. Different concentrations of cytotoxic drugs such as cisplatin
added in the culture medium.
An SV-40-transformed, nontumorigenic bronchial epithelial cell line, BEAS-2B
(CRL9609; American Type Culture Collection, Rockville, MD), was grown in
modified F12 medium admixed with Hepes stock solution (1.5 mol/L, pH 7.2 to 7.4)
and supplemented with growth factors as previously described.
SDS-PAGE and Western Blotting
The cells (1x106) were harvested and prepared by application of 500 µl of boiling
2X concentrated electrophoresis sample buffer (125 mM Tris-HCl, pH 6.8, 2% SDS,
5% glycerol, 0.003% bromophenol blue, and 1% β-mercaptoethanol) to each 10-cm
diameter dish. Protein samples were separated by SDS-PAGE and transferred to a
PVDF membrane, which was subjected to immunoblotting by anti-human caveolin-1
antibody (1:1000 dilution, BD Transduction Laboratories, Lexington, KY), followed
by blotting with HRP-conjugated rabbit anti-human antibody (1: 3500 dilution,
Amersham, Buckinghamshire, United Kingdom). An enhanced chemiluminescence
(ECL) reaction (Amersham) was applied for signal detection. Immunoblotting with
anti-human α-tubulin antibody (1:1000 dilution, Oncogene, Darmstadt, Germany)
was used as an internal marker both for quantity and quality control.
Immunohistochemistry
diagnosed as non-small cell lung cancer were obtained from the Department of
Pathology, National Taiwan University Hospital, during the period of 1998 to 2000.
Tumor staging was performed using the TNM classification system of international
union against cancer. The follow-up data was obtained from medical records. All
patients had advanced diseases, at least stage IIIb, in the initial presentation and did
not receive total excision for the tumor. They all had good performance and received
chemotherapy with the regimen of gencitabine plus cisplatin after diagnosis.
Immunohistochemistry
Paraffin-embedded 5 µm-thick sections were deparaffinized, heated in citrate
buffer (0.01M), treated with 0.3% H2O2, and re-hydrated. After blocking, serial
sections from the same patients were incubated respectively with anti-caveolin-1 IgG
(clone 2297, 1:500 dilution, BD Transduction Laboratories, Lexington, KY) and
anti-P-glycoprotein IgG (clone C494, 1:250 dilution, Signet Laboratories, Dedham,
MA) for 1 hour at room temperature, washed, and then blotted with biotin-labeled
bridge antiserum (1:200, Vector Laboratories, Burlingame, CA). After several washes
with PBS, sections were incubated with a solution of avidin and biotin-conjugated
peroxidase complex (Vector Laboratories) for 30 minutes at room temperature. DAB
colorization was applied, and slides were further counter-stained with hematoxylin.
For each specimen, the entire population of cancer cells in the lung tissue was
scanned. All specimens were evaluated without knowledge of the patients’ clinical
data. Caveolin-1 immunoreactivity was normally localized to fibroblasts, type I
pneumocytes, and endothelial cells of blood vessels in all tissue specimens examined,
which served as an internal quality control in immunohistochemistry. We artificially
chose 30% caveolin-1 immunoreactivity as a cutoff value for the assignment of
positivity (or negativity) of caveolin-1 staining. Although antibody against
P-glycoprotein had shown to cross-react with Pyruvate Carboxylase, unequivocal plasma
membrane patterns of immunostaining represent true P-glycoprotein expression. Positive staining of P-glycoprotein was defined if 30% or more of the neoplastic cells showed membrane staining.
Statistical Analysis
The correlation of caveolin-1 immunoreactivity with patients’ clinical variables was
analyzed by χ2-test or Fisher’s exact test (2-sided). Survival curve was plotted by
the Kaplan-Meier product-limit method and the statistical significance was assessed
by the log-rank test. Univariate and multivariate analyses were performed using the
Cox proportional-hazards regression model. P < 0.05 was considered to indicate
statistical significance in all of the analyses. All analyses were done with statistical
Result:
Up-regulation of caveolin-1 expression by cytotoxic drugs in drug-sensitive
cancer cells
We treated the lung cancer cell lines A549 with cisplatin and gemcitabine cytotoxic
drugs. As shown in Figure 1, drug-sensitive A549 cells had less or absent caveolin-1
expression. After exposure of the cancer cells to these cytotoxic drugs, up-regulation
of caveolin-1 expression was found. Higher concentration of cytotoxic drug and
longer exposure time also increased the expression of caveolin1.
Clinical Finding
We examined the status of caveolin-1 expression in specimens obtained from
patients who received chemotherapy. In this retrospective study, 73 specimens
diagnosed as lung cancer were obtained from the Department of Pathology, National
Taiwan University Hospital, during the period of 1998 to 2000. All patients had
advanced diseases, good performance and received chemotherapy with the regimen of
gencitabine plus cisplatin. The patients consisted of 41 man and 32 women. The mean
age was 57 years old (range 25-83). Forty-four patients had an age lower than 65
years old with 29 patients older than 65 years old. The pathological findings disclosed
adenocarcinoma in 49 patients, squamous cell carcinoma in 18 patients, and large cell
classification of the International Union against cancer. Eleven patients were in stage
IIIb, and 59 patients were in stage IV. Twenty-three patients had response to
chemotherapy, 32 patients remained stable during chemotherapy and 19 patients had
disease progression during chemotherapy.
Expression of cavoelin-1 in advanced lung cancer
Caveolin-1 immunoreactivity was normally localized to fibroblasts, type I
pneumocytes, and endothelial cells of blood vessels in all tissue specimens examined,
which could serve as an internal quality control in immunohistochemistry. We
artificially chose 30% caveolin-1 immunoreactivity as a cutoff value for the
assignment of positivity (or negativity) of caveolin-1 staining. Twelve of 73 patients
had caveolin-1 expression (Fig. 2). To determine the significance of caveolin-1
expression, all patients were divided into two groups according their cavoelin-1
expression: caveolin-1 negative group (n=61 patients) and cavoelin-1 positive group
(n=12 patients). The clinicopathologic variables of the caveolin-1 negative and
caveolin-1 positive group are listed in table 1.
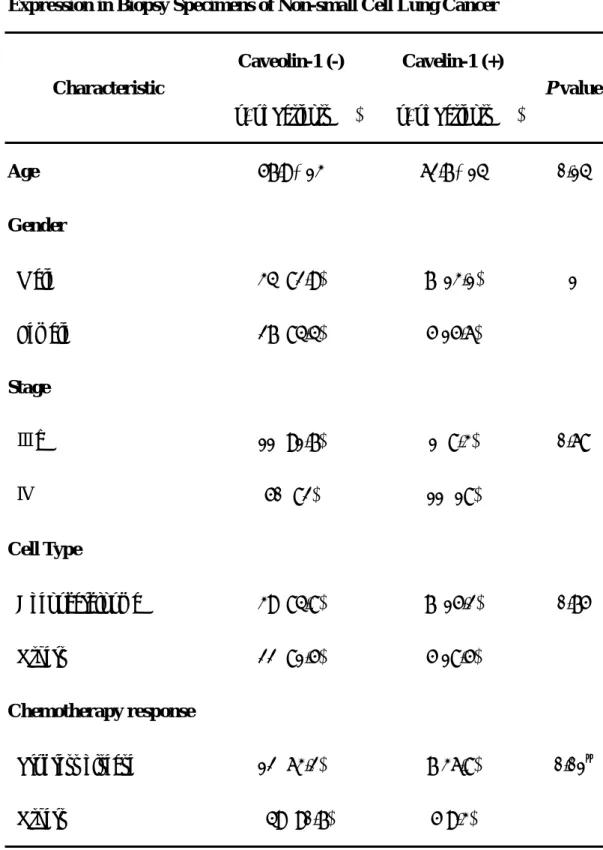
Correlation of caveolin-1 expression and poor response to chemotherapy
Among the 12 patients with caveolin-1 expression, only four patients remained
stable disease during chemotherapy. The other eight patients had progressive disease
caveolin-1 expression found in their specimens. Correlation between caveolin-1
expression and progress disease during chemotherapy was established (P=0.01, table
1).
We also examined the status of P-glycoprotein expression in these specimens and
4 patients had unequivocal plasma membrane patterns of immunostaining represent true
P-glycoprotein expression. In these 4 patients, one patient had progress disease during chemotherapy, two patients had partial response during chemotherapy and one patient remained stable during chemotherapy. Only one patient had caveolin-1 and P-glycoprotein co-expression and this patient remained stable during chemotherapy.
Prognostic significance of caveolin-1 expression
Analysis of the association of caveolin-1 expression with patients’ survival rate
was performed on the 73 patients of non-small cell lung cancer. The survival time
after chemotherapy for these 12 patients with caveolin-1 expression and 61 patients
without caveolin-1 expression was calculated by the Kaplan-Meier method (Fig. 3).
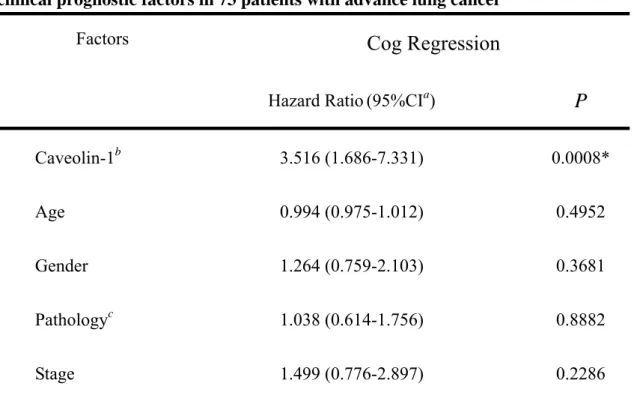
Multivariate analysis was also performed for caveolin-1 immunoreactivity and other
factors as stage, age, sex, and chemotherapy response. Performance status was
excluded for analysis because all of the patients were good enough to received
chemotherapy at the beginning. The univariate log-rank test for each variable was
multiple cog regression model suggested that the expression of caveolin-1 was an
independent factor for prediction of poor survival in patients with non-small cell lung
cancer (hazard ratio 3.516; P=0.0008) (Table 2)
Discussion:
In this study, immunohistochemical staining was performed in 73 specimens
from lung cancer patients with advanced disease receiving chemotherapy. Only 12
patients had caveolin-1 immunostaining. Among them, four patients had stable
disease during chemotherapy and eight had disease progression during chemotherapy.
Caveolin-1 expression is correlated with a poor response to chemotherapy. Although
up-regulation of caveolin-1 was found in many MDR cancer cell lines (8-11), this is
the first study with clinical data to demonstrate the relationship between caveolin-1
expression and possible drug resistance.
Caveolin-1 is thought to be a tumor suppressor gene, and its expression is
down-regulated in oncogenically transformed fibroblast, as well as breast and lung
cancer (12-14). However, after cytotoxic drug stress, up-regulation of caveolin-1
could be seen both in cancer lines and in vivo (15, 16). It has been reported that little
or no caveolin-1 immunostaining is in non-small cell lung cancer patients before
chemotherapy. But re-expression of caveolin-1 has been observed in half of the
Up-regulation of caveolin-1 after cytotoxic drugs is thought to be an early cellular
response before drug resistance is manifested. However, in this study, 12 of 73
patients who had advanced non-small cell lung cancer (at least stage IIIb) without
chemotherapy before biopsy showed positive caveolin-1 immunostaining. Many of
them had disease progression during chemotherapy. Expression of caveolin-1 before
administration of cytotoxic drugs is a good predictor for drug resistance.
Several mechanisms have been proposed for caveolin-1 up-regulation in MDR
cells. P-glycoprotein (P-gp), an ATPase that pumps out drugs used in chemotherapy,
has been found to be enriched in caveolin-1 rich membrane domain in some MDR
cells (9). But up-regulation of caveolin-1 is correlated with little P-gp expression in
other MDR cells and over-expression of P-gp is not localized in caveolae (17).
Reintroduction of caveolin-1 expression into drug sensitive cancer cells does not
increase the expression of P-gp (9, 18). In the specimens of ovarian cancer patients,
caveolin-1 expression is not correlated with P-gp expression (19). In our study,
P-glycoprotein was present in 4 patients without correlation of caveolin-1 expression.
It is interesting that caveolin-1 and cholesterol could regulate each other
reciprocally (20-23). Induction of caveolin-1 expression enhances the cholesterol
efflux and reduction of their expression with caveolin-1 antisense DNA, oxysterols or
Caveolin-1 is also transcriptionally regulated by
sterol-regulatory-element-binding-protein (SREBP) (20). A high cholesterol efflux
pathway may serve as a platform for lipophilic drugs transport from intracellular
compartment to plasma membrane against a steep concentration gradient, although
there is still no direct evidence to elucidate this. However, some cytotoxic drugs used
to establish MDR cancer cell lines with caveolin-1 up-regulation have low
lipophilicity including doxorubicin and cisplatin.
Another possibility is that caveolin-1 expression exerts negative regulation in
apoptotic machanisms, although such results are in recent conflict. Down-regulation
of caveolin-1 by anti-sense vector prevents staurosporine-induced apoptosis in
NIH-3T3 and T24 cells (25). Caveolin-1 sensitizes Rat-1 fibroblast to
ceramide-induced apoptosis and also increases 293 cells and HeLa cells to arsenite
cytotoxicity through PI-3K pathway (5, 26). However, Caveolin-1 could inhibit
anoikis in MCF-7 breast cancer cells (27), and suppresses c-myc-induced apoptosis
(28). In acid sphingomyelinase-deficient (asmase-/-) mice, loss of caveolae and
glycolipid-enriched membrane microdomains (GEM) increases susceptibility to
apoptosis after T cell receptor stimulation probably through decrease of MAPK
activation (29). A recent paper reported caveolin-1 has anti-apoptotic effect in prostate
and MDM2 (30). These conflicting reports may indicate caveolin-1 effect are cell
type- and expression level-dependent (5, 28, 31).
In summary, our study reveals that up-regulation of caveolin-1 in cancer cells has
more cytotoxic drug resistance no matter hydrophilic or lipophilic drugs. Caveolin-1
is down-regulated in newly-transformed cells and almost absent in the early stages of
lung cancer (14). However, its re-expression in the late stage disease before
chemotherapy is correlated with the drug resistance. Caveolin-1 may be one
component of mechanisms in multidrug resistance and may serve as a therapeutic
target for preventing multidrug resistance.
Reference:
1. Nishio, K., Nakamura, T., Koh, Y., Suzuki, T., Fukumoto, H., and Saijo, N.
Drug resistance in lung cancer. Curr Opin Oncol, 11: 109-115, 1999.
2. Anderson, R. G. W. and Jacobson, K. A Role for Lipid Shells in Targeting
Proteins to Caveolae, Rafts, and Other Lipid Domains. Science, 296:
1821-1825, 2002.
3. Engelman, J. A., Chu, C., Lin, A., Jo, H., Ikezu, T., Okamoto, T., Kohtz, D. S.,
and Lisanti, M. P. Caveolin-mediated regulation of signaling along the p42/44
MAP kinase cascade in vivo. A role for the caveolin-scaffolding domain.
4. Engelman, J. A., Wykoff, C. C., Yasuhara, S., Song, K. S., Okamoto, T., and
Lisanti, M. P. Recombinant Expression of Caveolin-1 in Oncogenically
Transformed Cells Abrogates Anchorage-independent Growth. J. Biol. Chem.,
272: 16374-16381, 1997.
5. Zundel, W., Swiersz, L. M., and Giaccia, A. Caveolin 1-mediated regulation of
receptor tyrosine kinase-associated phosphatidylinositol 3-kinase activity by
ceramide. Mol Cell Biol, 20: 1507-1514, 2000.
6. Podar, K., Tai, Y. T., Cole, C. E., Hideshima, T., Sattler, M., Hamblin, A.,
Mitsiades, N., Schlossman, R. L., Davies, F. E., Morgan, G. J., Munshi, N. C.,
Chauhan, D., and Anderson, K. C. Essential role of caveolae in interleukin-6-
and insulin-like growth factor I-triggered Akt-1-mediated survival of multiple
myeloma cells. J Biol Chem, 278: 5794-5801, 2003.
7. Wu, D., Foreman, T. L., Gregory, C. W., McJilton, M. A., Wescott, G. G., Ford,
O. H., Alvey, R. F., Mohler, J. L., and Terrian, D. M. Protein kinase cepsilon
has the potential to advance the recurrence of human prostate cancer. Cancer
Res, 62: 2423-2429, 2002.
8. Lavie, Y., Fiucci, G., and Liscovitch, M. Upregulation of caveolin in multidrug
resistant cancer cells: functional implications. Adv Drug Deliv Rev, 49:
9. Lavie, Y., Fiucci, G., and Liscovitch, M. Up-regulation of caveolae and
caveolar constituents in multidrug-resistant cancer cells. J Biol Chem, 273:
32380-32383, 1998.
10. Yang, C. P., Galbiati, F., Volonte, D., Horwitz, S. B., and Lisanti, M. P.
Upregulation of caveolin-1 and caveolae organelles in Taxol-resistant A549
cells. FEBS Lett, 439: 368-372, 1998.
11. Lavie, Y. and Liscovitch, M. Changes in lipid and protein constituents of rafts
and caveolae in multidrug resistant cancer cells and their functional
consequences. Glycoconj J, 17: 253-259, 2000.
12. Galbiati, F., Volonte, D., Engelman, J. A., Watanabe, G., Burk, R., Pestell, R.
G., and Lisanti, M. P. Targeted downregulation of caveolin-1 is sufficient to
drive cell transformation and hyperactivate the p42/44 MAP kinase cascade.
Embo J, 17: 6633-6648, 1998.
13. Lee, S. W., Reimer, C. L., Oh, P., Campbell, D. B., and Schnitzer, J. E. Tumor
cell growth inhibition by caveolin re-expression in human breast cancer cells.
Oncogene, 16: 1391-1397, 1998.
14. Ho, C. C., Huang, P. H., Huang, H. Y., Chen, Y. H., Yang, P. C., and Hsu, S. M.
Up-regulated caveolin-1 accentuates the metastasis capability of lung
1647-1656, 2002.
15. Belanger, M. M., Roussel, E., and Couet, J. Up-regulation of caveolin
expression by cytotoxic agents in drug-sensitive cancer cells. Anticancer
Drugs, 14: 281-287, 2003.
16. Belanger, M. M., Roussel, E., and Couet, J. Caveolin-1 Is Down-Regulated in
Human Lung Carcinoma and Acts as a Candidate Tumor Suppressor Gene.
Chest, 125: 106S-, 2004.
17. Hinrichs, J. W., Klappe, K., Hummel, I., and Kok, J. W. ATP-binding cassette
transporters are enriched in non-caveolar detergent-insoluble
glycosphingolipid-enriched membrane domains (DIGs) in human
multidrug-resistant cancer cells. J Biol Chem, 279: 5734-5738, 2004.
18. Liscovitch, M. and Lavie, Y. Multidrug resistance: a role for cholesterol efflux
pathways? Trends in Biochemical Sciences, 25: 530-534, 2000.
19. Davidson, B., Goldberg, I., Givant-Horwitz, V., Nesland, J. M., Berner, A.,
Bryne, M., Risberg, B., Kopolovic, J., Kristensen, G. B., Trope, C. G., van de
Putte, G., and Reich, R. Caveolin-1 expression in ovarian carcinoma is MDR1
independent. Am J Clin Pathol, 117: 225-234, 2002.
20. Bist, A., Fielding, P. E., and Fielding, C. J. Two sterol regulatory element-like
low density lipoprotein free cholesterol. Proc Natl Acad Sci U S A, 94:
10693-10698, 1997.
21. Fielding, P. E. and Fielding, C. J. Plasma membrane caveolae mediate the
efflux of cellular free cholesterol. Biochemistry, 34: 14288-14292, 1995.
22. Fielding, C. J., Bist, A., and Fielding, P. E. Caveolin mRNA levels are
up-regulated by free cholesterol and down-regulated by oxysterols in
fibroblast monolayers. Proc Natl Acad Sci U S A, 94: 3753-3758, 1997.
23. Fielding, C. J., Bist, A., and Fielding, P. E. Intracellular cholesterol transport in
synchronized human skin fibroblasts. Biochemistry, 38: 2506-2513, 1999.
24. Fielding, C. J. and Fielding, P. E. Intracellular cholesterol transport. J Lipid
Res, 38: 1503-1521, 1997.
25. Liu, J., Lee, P., Galbiati, F., Kitsis, R. N., and Lisanti, M. P. Caveolin-1
expression sensitizes fibroblastic and epithelial cells to apoptotic stimulation.
Am J Physiol Cell Physiol, 280: C823-835, 2001.
26. Shack, S., Wang, X. T., Kokkonen, G. C., Gorospe, M., Longo, D. L., and
Holbrook, N. J. Caveolin-induced activation of the phosphatidylinositol
3-kinase/Akt pathway increases arsenite cytotoxicity. Mol Cell Biol, 23:
2407-2414, 2003.
anchorage-independent growth, anoikis and invasiveness in MCF-7 human
breast cancer cells. Oncogene, 21: 2365-2375, 2002.
28. Timme, T. L., Goltsov, A., Tahir, S., Li, L., Wang, J., Ren, C., Johnston, R. N.,
and Thompson, T. C. Caveolin-1 is regulated by c-myc and suppresses
c-myc-induced apoptosis. Oncogene, 19: 3256-3265, 2000.
29. Nix, M. and Stoffel, W. Perturbation of membrane microdomains reduces
mitogenic signaling and increases susceptibility to apoptosis after T cell
receptor stimulation. Cell Death Differ, 7: 413-424, 2000.
30. Li, L., Ren, C. H., Tahir, S. A., Ren, C., and Thompson, T. C. Caveolin-1
maintains activated Akt in prostate cancer cells through scaffolding domain
binding site interactions with and inhibition of serine/threonine protein
phosphatases PP1 and PP2A. Mol Cell Biol, 23: 9389-9404, 2003.
31. Li, L., Yang, G., Ebara, S., Satoh, T., Nasu, Y., Timme, T. L., Ren, C., Wang, J.,
Tahir, S. A., and Thompson, T. C. Caveolin-1 mediates testosterone-stimulated
survival/clonal growth and promotes metastatic activities in prostate cancer
cells. Cancer Res, 61: 4386-4392, 2001.
Western blotting revealed caveolin-1 expression in BEAS-2B cells, but little
expression in A549. After exposure to different cytotoxic drugs including cisplatin
and gemcitabine, up-expression of caveolin-1 in A549 was found. Expression of
caveolin-1 was higher in high dose cytotoxic drug and longer exposure time. Staining
of α-tubulin was used as control.
Figure 2.
Immunohistochemical staining for caveolin-1. A. Negative or faint staining of
caveolin-1 in tumor cells from the patient who was response to chemotherapy.
Positive staining of endothelial cells as internal control (arrow). B. Cancer cell
chemotherapy.
Figure 3.
Comparison of overall survival curves for patients with caveolin-1-positive and
Table 1. Relationship between Clinicopathologic Features and Caveolin-1 Expression in Biopsy Specimens of Non-small Cell Lung Cancer
Characteristic Caveolin-1 (-) No. of Patients (%) Cavelin-1 (+) No. of Patients (%) P value Age 57.9± 13 62.7 ± 14 0.14 Gender Male 34 (82.9) 7 (13.1) 1 Female 27 (84.4) 5(15.6) Stage Ⅲb 11 (91.7) 1 (8.3) 0.68 Ⅳ 50 (82) 11 (18) Cell Type Adenocarcinoma 39 (84.8) 7 (15.2) 0.75 Others 22 (81.5) 5(18.5) Chemotherapy response Progress disease 12 (63.2) 7(36.8) 0.01§ Others 49 (90.7) 5(9.3) § Significance
Table 2. Analysis of parameters including caveolin-1 immunoreactivity and other clinical prognostic factors in 73 patients with advance lung cancer
Cog Regression
Factors
Hazard Ratio(95%CIa)
P
Caveolin-1b 3.516 (1.686-7.331) 0.0008* Age 0.994 (0.975-1.012) 0.4952 Gender 1.264 (0.759-2.103) 0.3681 Pathologyc 1.038 (0.614-1.756) 0.8882 Stage 1.499 (0.776-2.897) 0.2286a CI, confidence interval b Cut-off value: 30%
c Adenocarcinoma vs. non adenocarcinoma