帕金森病患於頭皮針灸治療前後大腦皮質動作準備電位與皮質應激性之變化;The Influence of Scalp Acupuncture on the Motor-related Cortical Potential and Cortical Excitability in Patients with Parkinson''s disease
52
0
0
全文
(2) 中國醫藥學院碩士班研究生 論文指導教授推薦書. 中國醫學研究所, 林 裕 欽 君所提之論文 帕金森病患於頭皮針灸治療前後大腦皮質動 作準備電位與皮質應激性之變化. ,係由本. 人指導撰述,同意提付審查。. 指導教授. 陳 光 偉. 中 華 民 國 九 十 六 年 七 月 四 日 ii.
(3) 中國醫藥學院碩士班研究生 論文口試委員審定書. 中國醫學研究所, 林 裕 欽 君所提之論文 帕金森病患於頭皮針灸治療前後大腦皮質動 作準備電位與皮質應激性之變化. ,經本委. 員會審議,認為符合碩士資格標準。 論文口試委員會. 委員. 林 昭 庚 張 芳 嘉 蔡 崇 豪 陳 光 偉. 所長. 高 尚 德. 中 華 民 國 九 十 六 年 七 月 四 日 iii.
(4) Contents. Chapter 1. Introduction……………………………………...……......... 1 Chapter 2. Literature and Research Review…………………...…......... 2 Scalp Acupuncture…………………………………………. 2 Parkinson's Disease…………………………………………5 Bereitschaftspotential..………………….…………………12 Cortical Excitability…………………………….………… 17 Chapter 3. Material and Methods………………................………….. 21 Subjects…………………………………………………… 21 Procedures of Motor-Related Cortical Potential (MRCP) and cortical excitability experimentation………..………...23 Statistical Analysis for data………………….…………….27 Chapter 4. Results………………………………………….…………. 28 Electroencephalographic data (MRCP analysis) ………… 28 Cortico-cortical inhibition (Cortical Excitability)………... 32 Chapter 5. Discussion………………………………………………… 37 Chapter 6. Conclusion…………………….………………………….. 41 References……………………………………………………………. 42 iv.
(5) Figures. Fig. 2.1.. The motor area………………………………………………. 3. Fig. 2.2.. The chorea-tremor area……………………………………… 4. Fig. 2.3.. Bereitschaftspotential………………………………………. 12. Fig. 3.1.. Following chart of acupuncture experimentation…………...23. Fig. 3.2.. Scalp points………………………………………………… 24. Fig. 3.3.. Following chart of On-Off experimentation……………….. 25. Fig. 4.1.. MRCPs before acupuncture in four PD patients…………… 28. Fig. 4.2.. MRCPs during acupuncture in four PD patients…………… 29. Fig. 4.3.. The MRCP during versus before acupuncture……………... 29. Fig. 4.4.. The average waveform of computed potentials though acupuncture treatment……………………………………… 30. Fig. 4.5.. All MRCPs before acupuncture in controls………………... 31. Fig. 4.6.. All MRCPs during acupuncture in controls……………….. 31. Fig. 4.7.. The MRCP during versus before acupuncture in controls… 31. Fig. 4.8.. Data of six PD patients in CCI…………………………….. 32. Fig. 4.9.. The data of last acupuncture in patient No.6………………. 33. Fig. 4.10. Data except the treatment with insufficient inhibition……... 33 Fig. 4.11. Data of five normal controls………………………………...34 Fig. 4.12. Data of six patients (on & off phases)……………………… 34 Fig. 4.13. The data of patient No.11…………………………………... 35 Fig. 4.14. Data except the treatment with insufficient inhibition (on & off phases)…………………………………………... 35 Fig. 4.15. Acupuncture inhibition in Parkinsonian patients excluding the treatment with insufficient inhibition versus normal controls……………………………………………………... 36 Fig. 4.16. Acupunctural inhibition versus Anti-parkisonian………….. 36. v.
(6) Tables. Table 2.1. Modified Hoehn and Yahr stages……………………………..6 Table 2.2. Terminologies for identifiable components of MRCP……... 13 Table 2.3. The generator sources of each MRCP components…………14 Table 2.4. Differential influence of various factors…………………… 15 Table 3.1. Clinical data from twelve Parkinsonian patients…………… 22 Table 5.1. Oxford Centre for Evidence-based Medicine Levels of Evidence……………………………………………………. 38. vi.
(7) 帕金森病患於頭皮針灸治療前後大腦皮質動作準備電位與皮質 應激性之變化 The Influence of Scalp Acupuncture on the Motor-related Cortical Potential and Cortical Excitability in Patients with Parkinson’s disease. YC JG FC GW. 研究生 共同指導教授. : 林裕欽 : 林昭庚 教授 張芳嘉 博士 指導教授 : 陳光偉 所長 中國醫藥大學中國醫學研究所. Lin Lin Chang Chen. 中文摘要 對於巴金森氏病人而言,因針灸的安全性且其與抗巴金森藥物無交互 作用,所以常作為輔助性的療法。然針灸對巴金森氏病人的臨床的療效 是有爭議的,而且少有用電生理的研究來評估針灸對巴金森氏病的引 響,是故設計此電生理試驗以衡量巴金森氏病人的頭皮針治療。 在本試驗中,我們使用皮質動作準備電位及皮質應激性(經成雙穿顱 磁刺激所誘發)為電生理評估的工具,對五位正常受試者與十二位巴金 森氏病人進行試驗。其中五位正常受試者與六位巴金森氏病人進行頭皮 針的試驗並分析前後電生理變化,而另六位巴金森氏病人接受服用抗巴 金森藥物前後的評估試驗。 經頭皮針的短暫治療後,六位巴金森氏病人並未在肢體活動獲得短期 的改善。但是在頭皮針的治療前後確有明顯的電生理改變,於正常受試 者中發現,其後期皮質動作準備電位於右側中央記錄有增強趨勢,且於 長間期成雙穿顱磁刺激中存在對皮質應激性抑制。而在巴金森氏病人 上,則於間期超過五毫秒的成雙穿顱磁刺激試驗中,頭皮針治療後明顯 的抑制治療前原有皮質應激性。. 關鍵字:頭皮針、針灸、巴金森氏病、皮質動作準備電位、皮質應激性 1.
(8) Chapter 1 Introduction Parkinson’s disease (PD) is one of the neurodegenerative disorders, which commonly causes disability among the elderly because of motor dysfunction. The clinical features of PD are mainly tremor, bradykinesia, rigidity and posture instability in a progressive course. [1,2]. . PD has existed worldwide. since the ancient time. In western views, the anti-parkinsonian drugs, such as levodopa, anticholinergics, dopamine agonists and monoamine oxidase inhibitors, have satisfactory efficacy in the initial treatment of PD. [3]. . But. they provide relatively little benefit during the progression of the disease and may cause the patient to develop unsatisfactory symptoms, which is due to the side effects of increased dosage and the long-term therapy [4]. Because of safety, negligible side effects and unknown interactions with medications, the acupuncture has been an alternative treatment for PD. [3]. .. After receiving acupuncture, the PD symptoms may relieve and the needed dosage of anti-parkinsonian medicine may decrease according to many experiences of staves in clinics. [4,5]. . Nevertheless, certain commentaries. consider that acupuncture is well tolerated but the symptoms of PD don’t improve other than sleep benefit. [6,7]. . The most of researchers evaluated the. therapeutic effects of acupuncture on PD by using the rating scales. [5,6,7]. ,. such as Webster's PD Rating Scale (WPDRS), Unified PD Rating Scale (UPDRS), Hoehn and Yahr (H & Y) score, Sickness Impact Profile (SIP), et cetera. [1,8]. . However, few studies evaluate the effects of acupuncture in PD. by electrophysiological methods, although the electromyogram (EMG). [9]. and auditory evoked brainstem potential have been applied in some of the studies [10]. Scalp acupuncture, a specialized acupuncture technique [11], is also known as a remedy for PD. [12]. . The purpose of this study was to. investigate whether scalp acupuncture induces change in the motor-related cortical potentials and cortical excitability before and during acupuncture. 1.
(9) Chapter 2 Literature and Research Review Scalp Acupuncture Scalp acupuncture is a modern acupuncture method and one of several specialized acupuncture techniques with a specific body location, taking its place alongside ear, nose, hand, foot, and wrist/ankle acupuncture. The more general acupuncture therapy is often called body acupuncture. The evolvement history [13] About the 1930s, the American neurosurgeon Wilder Penfield demonstrated that the human motor cortex also contains a spatial map of the body's musculature according to focal electrical stimulation. Also the somatic sensory map shows the same disproportions observed in the postcentral gyrus. Then it is noticed that a special area on cerebral cortex is responsible for certain function, such as motor, sensory and speech, etc. Around 1950s to 1970s, many China acupuncturists had researched the relation between scalp projection points and function of underlying special area on cerebral cortex. Then they found some effects on neurological or systemic diseases by using those points as acupoints (acupunctural points). During the 1970’s, scalp acupuncture was developed as a complete acupuncture system. Three major contributors to the development of this system, Jiao Shunfa, Fang Yunpeng, and Tang Songyan, each proposed different diagrams and groupings of scalp acupunctural points. Thus, scalp acupuncture is not really a single system, but a multiplicity of systems still in development, with a 30-year history of practical experience. A standard of nomenclature for acupuncture points has been developed (Regional Consultation Meeting on the Standardization of Acupuncture Nomenclature, Tokyo, May 1984), indicating 14 therapeutic 2.
(10) lines or zones based on a combination of the thoughts of the different schools of scalp acupuncture. However, it is often necessary to carefully review the zones relied upon by an individual practitioner, as few have adopted the unified pattern. So Zhu Mingqing developed a popular version of scalp acupuncture. In Zhu’s scalp acupuncture, 8 therapeutic zones are used [actually, 9 zones], and the manipulation is characterized by forceful, small-amplitude lifting and thrusting of the needle, associated with massage [of the body part to be affected] and physical and breathing exercises. The main localization of scalp points according to scalp acupuncture of Jiao Shunfa [11,13] Motor area: (seen on Figure 2.1) The point at 0.5cm posterior to the midpoint of the anterior-posterior line defines the upper limit of the motor area, and the lower limit intersects the eyebrow-occiput line at the anterior border of the natural hairline on the temple. The upper 1/5 represents the lower limbs and trunk, the middle 2/5 is response to the upper limbs and the lower 2/5 depicts the face. It is indicated for contralateral motor disturbance of the appropriate area.. Fig. 2.1. The motor area (from Ref. 12) 3.
(11) Sensory area: This is a line parallel to the motor area and is 1.5cm behind it. The sensory input to the lower limbs and trunk is represented on the upper 1/5, the middle 2/5 represents the upper limbs, and the lower 2/5 represents the face. It is response for contralateral sensory disturbances of the appropriate area, pain and migraine. Chorea-tremor area: (seen on Figure 2.2.) This area locates parallel to the motor area and is 1.5 cm toward the face. It is response for Parkinsonism, tremor and chorea from any cause. The needling stimulation to the contralateral area is helpful for unilateral disorder, and the stimulation to the bilateral areas for bilateral disorder.. Fig. 2.2. The chorea-tremor area (from Ref. 12). The therapy theory [11] Needle stimulation of these theoretical areas may result in altered blood flow and/or increased activity of the various areas lying deep or superficially within the brain. The basic principle, therefore, was that the stimulation of these appropriate scalp areas could result in changes in brain function. In general, the special areas on the scalp were related to underlying cerebral surfaces. 4.
(12) Parkinson's Disease (Idiopathic PD, Paralysis Agitans) James Parkinson is attributed with rendering the first cogent description of PD and identified the hallmark features of the illness through description of cases observed in the streets of London in his monograph, The Shaking Palsy (1817). Over time, the specific terms of PD and idiopathic PD have reserved for the clinical syndromes of asymmetrical parkinsonism, usually with rest tremor, in association with the specific pathological findings of loss of dopaminergic substantia nigra neurons with eosinophilic cytoplasmic inclusions (Lewy bodies). In 1959, Hornykiewicz discovered that ultimately led to highly effective pharmacotherapy with. L-dopa. and direct-acting. dopamine agonists (DAs). Epidemiology and Clinical Features In community-based series, PD accounts for more than 80% of all parkinsonism. [14]. , with a prevalence of about 357.9 per 100,000 and an. incidence of 28.7 per 100,000 per year in Taiwan[15]. PD is a disease of aging, showing a gradual increase in prevalence beginning after the age of 50 years and a steep increase in prevalence after age 60 years. Disease before the age of 30 years is very rare and often suggests a hereditary form of parkinsonism [14]. .. Typically the onset and progression of PD are gradual. The most common presentation is the rest tremor in one hand, often associated with decreased arm swing and shoulder pain. Bradykinesia and rigidity are often detectable on the symptomatic side, and midline signs, such as reduced facial expression or mild contralateral bradykinesia and rigidity, may be present. The disorder usually remains asymmetrical throughout much of its course. With progression of the illness, generalized bradykinesia may cause difficulty with arising from a chair or turning in bed. The gait and balance are progressively affected and falls may occur. The Hoehn and Yahr stage, first described before effective dopaminergic treatment became available, 5.
(13) accurately outlines the milestones in progression of the illness from mild unilateral symptoms through the end-stage nonambulatory state (Table 2.1) [14]. .. Table. 2.1. Modified Hoehn and Yahr stages Stage 0. No signs of disease. Stage 1. Unilateral disease. Stage 1.5. Unilateral plus axial involvement. Stage 2. Bilateral disease, without impairment of balance. Stage 2.5. Mild bilateral disease, with recovery on pull test. Stage 3. Mild to moderate bilateral disease; some postural instability; physically independent. Stage 4. Severe disability; still able to walk or stand unassisted. Stage 5. Wheelchair bound or bedridden unless aided. It is not difficult to diagnose a PD patient with unilateral or asymmetrical rest tremor, bradykinesia, and rigidity. The presence of this syndrome carries a positive predictive value of 92%, with a sensitivity of 90% [14]. The clinical diagnosis is usually according to UK Parkinson’s Disease Society Brain Bank clinical diagnostic criteria [2]. UK Parkinson’s Disease Society Brain Bank clinical diagnostic criteria: STEP 1. Diagnosis of Parkinsonian syndrome BRADYKINESIA (slowness of initiation of voluntary movement with progressive reduction in speed and amplitude of repetitive actions). And at least one of the following: a. muscular rigidity b. 4-6 Hz rest tremor c. postural instability not caused by primary visual, vestibular, cerebellar or proprioceptive dysfunction 6.
(14) STEP 2. Exclusion criteria for Parkinson’s disease History of repeated strokes with stepwise progression of parkinsonian features History of repeated head injury History of definite encephalitis Oculogyric crises Neuroleptic treatment at onset of symptoms More than one affected relative Sustained remission Strictly unilateral features after 3 years Supranuclear gaze palsy Cerebellar signs Early severe autonomic involvement Early severe dementia with disturbances of memory, language and praxis Babinski sign Cerebral neoplasm or communicating hydrocephalus on CT scan Negative response to large doses of levodopa (if malabsorption excluded) MPTP exposure STEP 3. Supportive prospective positive criteria for Parkinson’s disease. Three or more required for diagnosis of definite Parkinson’s disease Unilateral onset Rest tremor present Progressive disorder Persistent asymmetry affecting the side of onset most Excellent response (70-100%) to levodopa Severe levodopa-induced chorea Levodopa response for 5 years or more clinical course of 10 years or more. 7.
(15) Nonmotor symptoms are universal in PD and contribute prominently to declining quality of life. [14]. : Autonomic symptoms include reduced. gastrointestinal transit time with postprandial bloating and constipation, urinary urgency, disordered sweating, and orthostatic hypotension. Cognitive and behavioral changes are universal as well, involving impaired attention and executive dysfunction. Anxiety and mood disorders are common. Sleep disturbance is nearly universal in PD and is multifactorial, such as a variety of motor movements including restless legs and periodic leg movements, rapid eye movement (REM) sleep behavior disorder (RBD), and nightmares. Symptomatic Treatment [14] Anticholinergics. reduce. tremor. and. rigidity. without. effects. on. bradykinesia by antagonizing the effects of acetylcholine at muscarinic receptors postsynaptically to striatal interneurons. Its toxicity related to antagonism of acetylcholine at central and peripheral receptors results in confusion, blurred vision, dry mouth, constipation, and urinary retention. L-dopa develops adverse effects, including nausea, vomiting, orthostatic hypotension, sedation, confusion, sleep disturbance, alterations of dream phenomena, hallucinations, and dyskinesias. Its global antiparkinsonian efficacy is dramatic and predictable, so that a positive therapeutic response is used to define the disease itself. Amantadine has an antiparkinsonian mechanism to stimulate release of endogenous dopamine stores, to block reuptake of dopamine from the synaptic cleft, and to have anticholinergic properties. Dopamine agonists (DAs) cause side effects similar to those of L-dopa, although orthostatic hypotension, sleepiness, and hallucinations are more common or severe. DA monotherapy is associated with a very low incidence of dyskinesia. Wearing off is the most common type of motor fluctuation and is the predictable return of parkinsonism in advance of the next scheduled antiparkinsonian dose. On-off is the unpredictable reappearance of parkinsonism at a time when central levels of antiparkinsonian drugs are 8.
(16) expected to be within the target therapeutic range. Dose failure is the completed failure to develop a favorable effect in response to an incremental dopaminergic dose. Peak-dose dyskinesias are usually choreiform or stereotypical movements presenting at the peak of the therapeutic response. Etiology and pathology of PD in Chinese medicine [12] Many of clinical Features (as above described) in PD are typical signs and symptoms of internal wind(內風) associated with liver disharmony(因諸風 眩吊皆屬於肝) in Chinese medicine. PD usually occurs in patients over 50. years old. Chinese medicine believes that overwork, excessive sexual activity, improper diet and emotional stress are common and important causes for many diseases. If these causes last a long period of time they will eventually give rise to kidney deficiency. Furthermore, senility, the late stage of life, is characterised by decline of kidney essence (腎陰虛). This is why geriatric diseases always present with an underlying kidney deficiency pattern. As the liver and kidney share the same origin, kidney deficiency leads to both liver and kidney deficiency(肝腎兩虛). Malnourishment of the tendons due to this deficiency results in stirring of liver wind internally(肝風 內動). From a Chinese medicine perspective, the main manifestations and. age of onset of Parkinson’s disease indicate that the disease relates primarily to liver and kidney disharmony(肝腎失調) and liver wind(肝風). Pattern identification and treatment principles of PD in Chinese medicine [12] PD is characterised by signs and symptoms of liver wind. In clinical practice, this degenerative condition often overlaps with other chronic geriatric diseases, such as hypertension, high cholesterol, coronary artery disease, arteriosclerosis and diabetes. These are commonly associated with phlegm(痰) and blood stasis(血淤). In Chinese medicine, the pathogenesis of Parkinson’s disease includes both root deficiency and excessive manifestations such as wind(風), phlegm(痰), qi stagnation and blood stasis 9.
(17) (氣滯血淤). Patterns of PD are represented by a progressive continuum. from mild to severe. Qi and blood deficiency (氣血兩虛) begins the disease progression. Left untreated or aggravated, the condition often degenerates into deficiency of liver and kidney(肝腎兩虛). Wind-phlegm is then prone to obstruct the channels(風痰阻絡) leading to blood stasis with endogenous wind(內風). Finally, at the severe end of the spectrum, yin and yang both become deficient(陰陽兩虛). As a result, the general treatment principle is “nourishing yin and extinguishing wind”(滋陰熄風). Nourishing liver and kidney yin treats the root(滋養肝腎之陰為本) and extinguishing wind focuses on eliminating its manifestation(鎮肝熄風為標). “Invigorating blood and transforming phlegm” (活血卻痰) is an additional principle application because blood stasis and/or phlegm are patterns that appear often in this disease. The specific treatment plan will differ in different stages of the disease with different patients. Generally speaking, PD is a chronic disease requiring a long period of treatment with acupuncture and herbs in Chinese medicine. Acupuncture treatment of Parkinson’s disease [12] Body acupuncture [12] Main Points: Taixi KID-3, Ganshu BL-18, Taichong LIV-3, Ququan LIV-8, Sanyinjiao SP-6, Guanyuan REN-4, Fengchi GB-20, Fengshi GB-31 and Hegu L.I.-4. In this acupuncture prescription, Taixi KID-3, the yuan-source point of the kidney channel, is effective at nourishing kidney yin. Ganshu BL-18 and Ququan LIV-8, the back-shu point and he-sea point of the liver channel respectively, restore the liver function. These three points nourish kidney and liver yin to treat the root. The spleen and kidney are the root of post- and pre- heaven respectively, and thereby the source of liver yin. Sanyinjiao SP-6, the meeting point of the spleen, liver and kidney channels, and Guanyuan REN-4, the meeting point of the Conception vessel with the spleen, liver and kidney channels, can nourish the liver. Both REN-4 and 10.
(18) SP-6 strengthen the function of the first three points in treating the root. Fengchi GB-20 (Wind Pool) and Fengshi GB-31 (Wind Market) are points of the gall bladder channel which interiorly-exteriorly connects with the liver channel, and are effective at extinguishing liver wind. The modification [12,16]: For tremor and rigidity of the upper limbs, Quchi LI-11, Shousali LI-10, and Waiguan TE-5 may be added; for tremor and rigidity of the lower limbs, Yanglingquan GB-34, and Zusanli ST-36 may be added. [12]. ; Qihai REN-6 and Zusanli ST-36 may be added to increase. deficient qi and blood; Shenshu BL-23, Zhaohai KID-6 and Yanglingquan GB-34 may be added for pronounced liver and kidney yin deficiency; Yinglingquan SP-9 and Fenglong ST-40 may be added when the channels are obstructed by wind-phlegm; Geshu BL-17 and Xuehai SP-10 may be added for cases with blood stasis and endogenous wind [16]. Scalp acupuncture [12] The commonly used scalp locations are the chorea, motor, leg motor and sensory areas. Use the thoracic cavity area in cases with palpitations and chest oppression. The stomach area is effective for epigastric distention and reduced appetite. Scalp acupuncture is manipulated by rapidly twirling the needles at small amplitude in 200 times a minute for 2 minutes, and retaining the needles for 5 minutes. Moxibustion [12,17] Moxibustion is also used frequently in practice, especially for patterns involving yang qi deficiency. Dabao SP-15, Qimen LIV-14, Shenque REN-8 and Zusanli ST-36 are the most commonly used points for moxa treatment which is especially effective for the rigidity of muscles and limbs. [12]. .. Tanzhong CV-17, Zhongwan CV-12, and Tianshu ST-25 may be added, which are basic acupoints for treatment of brain diseases, and could be combined with Sanyinjiao SP-6 [4].. 11.
(19) Bereitschaftspotential (Movement-Related Cortical Potentials, MRCP) Since Kornhuber and Deecke (1964) made the first report of electroencephalographic (EEG) activity preceding self-initiated movement in humans, generally named as Bereitschaftspotential (BP), various source localization techniques in normal subjects and epicortical recordings in epilepsy patients have disclosed the generator mechanisms of each identifiable component of movement-related cortical potentials (MRCPs) to some extent. The initial slow segment of MRCP, generally named as Bereitschaftspotential (BP) or early BP, usually begins between 1.5 to 1 s before the movement onset [17] and is maximal at the midline centro-parietal area, symmetrically and widely distributed over the scalp regardless of the site of movement. About 500 ms before the movement onset. [17]. , there. appears the steeper negative slope called negative slop (NS') or late BP. Figure 2.3 shows averaged waveforms of 98 trials based on the scalp distribution of averaged data across 14 subjects by Shibasaki et al., and different terminologies have been proposed for identifiable components of MRCP seen in Table 2.2 [18].. 1. Early BP starts 1.7 s before the onset of the averaged, rectified EMG of the left wrist extensor muscle 2. Later negative slope (late BP) starts 300 ms before the EMG onset (contralateral to the movement) 3. N-10 or motor potential (MP) is a negative peak localized at the contralateral central area (C2) 4. N+50 or the frontal peak of motor potential (fpMP) is another negative peak occurring shortly after N-10 is localized over the midline frontal region (from Ref. 18) Fig. 2.3. Bereitschaftspotential 12.
(20) Table 2.2. Terminologies for identifiable components of MRCP (from Ref. 18) Pre-movement components Kornhuber and Deecke (1965) Vaughan et al. (1968) Shibasaki et al. BP (1980)a Dick et al. NS1 (1989) Lang et al. BP1 (1991) Tarkka and BP Hallett (1991) Kristeva et al. (1991)b Cui and BP1 Deecke (1999). Post-movement components. BP. PMP. MP. N1. P1. N2(?). N2(?). N-10. N+50. NS’ P-50. RAP P2 P+90. N+160. P+300. NS2 BP2 NS’ PMP isMP ppMP fpMP RF. MF BP2. MP. MEFI MEFII MEFIII PMPP. MEPI. PMF MEPII. a: Peak of each component, except for BP and NS’, was measured from the peak of averaged, rectified EMG. b: Based on movement-related magnetic fields.. Generator sources of MRCP [18] Early BP starts first in the supplementary motor area (SMA) including pre-SMA and SMA proper, and then shortly thereafter in the lateral premotor cortices bilaterally. About 500 ms prior to the movement onset the late BP (NS’) starts mainly in the contralateral M1 and premotor cortex. The current consensus on the generator sources of each MRCP components is summarized in Table 2.3. In self-paced repetition of simple movements at slow rate, the early slope (early BP) begins about 2 s before the movement onset in the pre-SMA with no site-specificity and in the SMA proper according to the somatotopic organization, and shortly thereafter in the lateral premotor cortex bilaterally again with relatively clear somatotopy. About 500 ms before the movement onset, another steeper negative slope (late BP or NS’) occurs in the contralateral M1 and lateral premotor cortex with precise somatotopy.. 13.
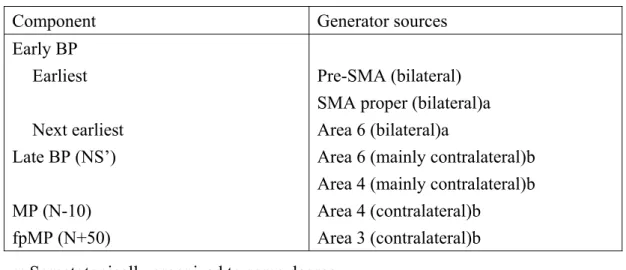
(21) Table 2.3. The generator sources of each MRCP components (from Ref. 18) Component. Generator sources. Early BP Earliest Next earliest Late BP (NS’) MP (N-10) fpMP (N+50). Pre-SMA (bilateral) SMA proper (bilateral)a Area 6 (bilateral)a Area 6 (mainly contralateral)b Area 4 (mainly contralateral)b Area 4 (contralateral)b Area 3 (contralateral)b. a: Somatotopically organized to some degree. b: Somatotopically organized precisely.. Influence factors and physiological implication of BP [18,19] The magnitude and time course of BP recorded in the self-paced condition are influenced by various factors such as level of intention, preparatory state, movement selection as to freely selected versus fixed, learning and skill acquisition, pace of movement repetition, praxis movement, perceived effort, force exerted, speed and precision of movement, discreteness and complexity of movement, and pathological lesions of various brain structures [18]. Within subjects, the reproducibility is high and there appears to be no systematic effect of practice on the BP. The BP may be absent in some subjects and age-related changes are minor [19]. One review article refers to more recent findings and summarizes the current consensus of this issue in Table 2.4 [18]. Larger amplitude of late BP is found, but not early BP, in the isolated movement of the middle finger as compared with the simultaneous movement of the two fingers. In spite of the fact that a larger number of muscles are involved in the two finger movement than in the single finger movement, the late BP is larger in the latter.. 14.
(22) Table 2.4. Differential influence of various factors (from Ref. 18) Differential influence of various factors on early and late BP in normal and pathological conditions Factors Early BP Late BP Level of intention. Larger a. Preparatory state Movement selection Praxis movement Learning Speed Precision Force Discreteness. Earlier onset a Larger Start parietally a Larger during learning a Later onset a No effect Larger a No effect. Complexity Parkinsonism Cerebellar lesion Dystonia Hemiparesis recovery Mirror movement. No effect Small Small No change No change No change. No effect. Larger Larger Larger No change Small Small Involved Involved. As for the factors in normal conditions, the effect is shown in a comparative form; the greater the factors, the larger or smaller the BP. a : Late BP not clearly distinguished.. Early BP is influenced by cognitive functions such as level of intention, preparatory state and movement selection, whereas the late BP is influenced by features of the movement itself, such as precision, discreteness and complexity. In pathological conditions, early BP is abnormal in PD, while late BP is abnormal in hemiparesis, dystonia and mirror movement. Both are abnormal in cerebellar lesions. This is consistent with the generator sources of each component; pre-SMA, SMA proper and lateral premotor area (area 6) bilaterally are in response for early BP and contralateral precentral cortex including area 6 and area 4 exhibit late BP [18]. In the Libet’s experiment, the timing of awareness of the conscious would occur much later than the BP onset. There are general interpretations for the complexity of the Libet’s experiment: first, there is a general decision to 15.
(23) move periodically in the beginning of the whole experiment; second, it is possible that the decision for each individual movement is made subconsciously and that consciousness is “switched on” about 200 ms before movement onset; third, this 200 ms interval gives time for consciousness to veto the movement [18]. BP in Parkinson’s Disease [19] Given the strong projection from basal ganglia to SMA, abnormalities of the BP in PD are expected. In an early observation, reduction of the BP was over the two precentral areas despite of preservation at the vertex. Early BP was smaller for patients with PD, compared to controls over frontal electrodes, whereas there were no significant differences for the late BP. In PD treated with thalamotomy, the patients lost previously present BP postoperatively. From findings in the patients with PD compared with age-matched controls, the size of the early BP amplitude was reduced in the patients whereas the peak amplitude was not different. Random-choice movements were associated with greater SMA activation than fixed ones from studying functional imaging in both PD patients and controls. However, PD did not increase their BP, particularly the earlier component, with the random movement task. Also the contingent negative variations (CNV) from PD patients were reduced over frontal cortical sites compared to controls and bilateral subthalamic nucleus stimulation could reduce the abnormalities. Levodopa treatment increased the amplitude of the early BP in both normals and patients with PD.. 16.
(24) Cortical Excitability The technique of focal transcranial magnetic stimulation (TMS) is usually used to evaluate the excitability of the motor cortex by different conditions, such as paired TMS, stimulation of somatosensory afferent and pairing peripheral stimulation with TMS. Intracortical (Cortico-cortical) inhibition Kujirai et al. reported that if two stimuli were given through the same coil over the motor cortex, a subthreshold conditioning stimulus suppresses the response of a larger suprathreshold stimulus when the interval between the stimuli is less than 5 ms regardless of facilitated responses at longer intervals for the test [20]. At an interstimulus interval (ISI) of 3 ms, the suppressed test responses were maximum during the intensity of conditioning stimuli at 0.8 times the resting motor threshold [20] or between 90 and 110 percentage of active motor threshold [21]. This interaction is due to the activation of circuits in the cerebral cortex: first, the intensity of the conditioning stimulus can be lower than that required to evoke any descending corticospinal volley; second, the conditioning stimulus has no effect on spinal H-reflexes, or responses to anodal electrical stimulation of the motor cortex; third, direct recordings from the spinal epidural space show that the conditioning stimulus reduces the size and number of descending corticospinal volleys evoked by the test shock. [22]. . The inhibitory neurotransmitter r-aminobutyric acid (GABA),. widespreaded throughout the cortex, may mediate the actions of inhibitory neurons controlling excitability to maintain organisation within the motor cortex [24]. So the initial inhibition from the conditioning stimulus is probably due to the local GABAergic neurones within the motor cortex [21] since it is affected by drugs that act on central GABAA receptors [22]. Therefore, paired transcranial magnetic stimulation (TCMS) is possible to test the excitability of intracortical inhibitory and excitatory elements.. 17.
(25) Inhibition from other areas of the brain connected to motor cortex [22] Transcallosal inputs are displayed while a single conditioning stimulus over the motor hand area of one cortex can affect the size of responses to a test pulse given over the opposite motor area. The major inhibition is beginning at an interstimulus interval of 6–7 ms, and lasts for 30 ms or more depending on the intensity of the conditioning stimulus. Transcallosal inhibitions are site-specific, being most prominent when homologous parts of each motor area are stimulated, and seem to depend on activation of neurones different to those involved in the contralateral MEP since the threshold for inhibition may differ from that of the contralateral MEP. This is consistent with the anatomical data that show the transcallosally projecting fibres originate in cortical layer III whereas the corticospinal neurones are found in layer V. Inputs from the cerebellum represent inhibitory maximum effect during transcranial electrical stimuli across the posterior parts of the mastoid process over the cerebellum which is contralateral to the motor cortex used to test. Inhibition begins about 5 ms after the conditioning stimulus and continues for 10 ms or more. However, the later part of the inhibitory effect is complex. The first 3 ms or so is a purely cortical effect from testing spinal excitability with H-reflexes and anodal electric stimulation of the motor cortex, probably produced by activation of a cerebello-cortical projection, but that later portions might be of mixed spinal and cortical origin. Magnetic stimulation, particularly with the large coils, is sometimes needed to obtain such effects from the cerebellum and often activates cervical nerve roots, resulting in complicate interpretation of the results. Modulation of the somatosensory afferent stimulation The short- and long-term changing afferent input by peripheral sensory stimulation can also influence motor cortical organization. Motor-evoked potentials evoked by TMS can be increased in the hand muscles innervated by the repetitively stimulated nerve, which is due to the increase of the 18.
(26) cortical excitability and doesn’t result from the stimulus-induced increases in the excitability of spinal motoneurones because of no alteration of F wave responses in the intrinsic hand muscles after prolonged nerve stimulation [24]. Also a prolonged nonpainful stimulation of peripheral nerves induced a long-term increase in excitability in the motor cortex representation of the corresponding muscles. [25]. . Above effects are also very specific and are. accompanied by topographic changes in the related representational cortical maps. Conversely, the stimulation of skin or muscle nociceptive fibres in the distal upper limb has an inhibitory effect on motor-evoked potentials (MEPs) evoked by TMS [26] that is specific to the muscles adjacent to the painful area, given that it is not present or becomes excitation in more proximal muscles. It had been shown to enhance excitability in the human motor cortex via interventional paired associative stimulation (IPAS), as dual stimuli consisting of motor point stimulation on the tested muscle paired with single TMS [27]. Following IPAS, the facilitation of motor-evoked potentials (MEPs) are significant, associated with an increase in the intracortical facilitation, although there is no significant difference in the level of intracortical inhibition [23]. The long-term potentiation-like mechanism may underlie the cortical plasticity induced by IPAS [28]. Cortical Excitability in PD The Abnormality of motor cortical inhibition in patients with PD was demonstrated by a significant decrease in the amount of corticocortical inhibition, which improved after L-dopa intake. Basal ganglia dysfunction in PD could decrease the excitability of cortical inhibitory circuits resulting in reduced ipsilateral corticocortical suppression as tested by TMS. A role of inhibitory connections within motor cortex is possible to focus activity onto appropriate neurons for a forthcoming movement, and then basal ganglia output may regulate shaping process [29]. Pallidotomy could modulate the cortical inhibitory circuitry in patients with PD because of obvious diminution of cortico-cortical inhibition at the ISI of 3 ms in Parkinsonian 19.
(27) patients 3 months after operation [30]. The motor-evoked potential amplitude in the tested hand muscle was not increased by IPAS in PD patients compared with healthy volunteers. The ratio of the motor-evoked potential amplitude before and after IPAS in PD-off patients increased after dopamine replacement. Thus, dopamine might contribute to the associative long-term potentiation-like effect in the motor cortex in PD patients [31].. 20.
(28) Chapter 3 Material and Methods Subjects All subjects underwent experimentation in Neuroscience Laboratory of the Neurology department in China Medical University hospital. The protocol was approved by the local Institutional Review Board. Five control volunteers (four men and one female, age from 28 to 36 with mean 33 y/o, without PD, other neurodegenerative disease, or the past history of intracranial disorders, such as stroke neurotaumatic hemorrhage, cerebral neoplasm, or etc., possibly causing sequent lesions) and twelve patients with PD were included in this study. Patients were recruited for the study during their routine outpatient visited to the Neurology department in China Medical University hospital. Only patients with idiopathic Parkinson’s disease stage I–III (according to UK Parkinson’s Disease Society Brain Bank clinical diagnostic criteria. [2]. , and Hoehn and Yahr. staging scale) were included in the study. Patients with atypical Parkinsonism or with exhibiting signs of cognitive impairment were excluded. Other exclusion criteria included (1) patients taking medication for anxiety, depression, psychosis, or other psychiatric disturbances; (2) prior history of stroke or dementia; (3) bleeding or coagulation disorders; (4) skin infections; (5) history of arrhythmias, pacemaker, or implanted defibrillator; (6) needle phobia. Twelve Parkinsonian patients were equally and randomly divided into two groups: six with the average age of 55.8 years were for acupuncture experimentation, and others with the average age of 59.2 years received on-off experimentation.. 21.
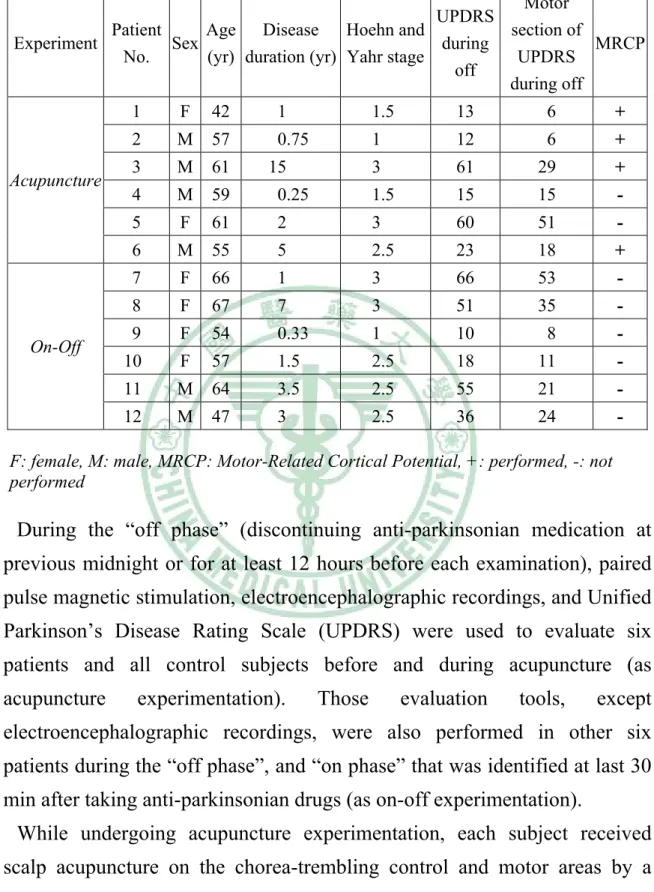
(29) Table 3.1. Clinical data from twelve Parkinsonian patients Motor UPDRS Patient Age Disease Hoehn and section of Experiment Sex during MRCP No. (yr) duration (yr) Yahr stage UPDRS off during off. Acupuncture. On-Off. 1. F. 42. 1. 1.5. 13. 6. +. 2. M. 57. 0.75. 1. 12. 6. +. 3. M. 61. 3. 61. 29. +. 4. M. 59. 0.25. 1.5. 15. 15. -. 5. F. 61. 2. 3. 60. 51. -. 6. M. 55. 5. 2.5. 23. 18. +. 7. F. 66. 1. 3. 66. 53. -. 8. F. 67. 7. 3. 51. 35. -. 9. F. 54. 0.33. 1. 10. 8. -. 10. F. 57. 1.5. 2.5. 18. 11. -. 11. M. 64. 3.5. 2.5. 55. 21. -. 12. M. 47. 3. 2.5. 36. 24. -. 15. F: female, M: male, MRCP: Motor-Related Cortical Potential, +: performed, -: not performed. During the “off phase” (discontinuing anti-parkinsonian medication at previous midnight or for at least 12 hours before each examination), paired pulse magnetic stimulation, electroencephalographic recordings, and Unified Parkinson’s Disease Rating Scale (UPDRS) were used to evaluate six patients and all control subjects before and during acupuncture (as acupuncture. experimentation).. Those. evaluation. tools,. except. electroencephalographic recordings, were also performed in other six patients during the “off phase”, and “on phase” that was identified at last 30 min after taking anti-parkinsonian drugs (as on-off experimentation). While undergoing acupuncture experimentation, each subject received scalp acupuncture on the chorea-trembling control and motor areas by a licensed Acupuncturist, and the treatment lasted approximately for one hour. All of the subjects completed the study and were given informed consents for the participation. 22.
(30) Procedures of Motor-Related Cortical Potential and cortical excitability experimentation Acupuncture experimentation Following chart of acupuncture experimentation (with EEG recording) First UPDRS III ▼ EEG recording (Fz, FCz, Cz, Pz, F3-F4, C3-C4, P3-P4) preceded by transcranial magnetic stimulation ▼ To insert gauge-32 filiform needles (1 cun ) to motor area and chorea-trembling in right vertex scalp. Scalp acupuncture (maintained > 30+ min) ▼ Repeated EEG recording followed by transcranial magnetic stimulation ▼ Second UPDRS III ▼ To remove needles from scalp Fig. 3.1. Following chart of acupuncture experimentation. 1. Before acupuncture Before electroencephalographic recording, the subjects were evaluated with UPDRS and paired pulse magnetic stimulation (described below). During electroencephalographic recording, they sited on a chair in front of the monitor displaying a gray cross in central area in a laboratory room with dimmed lights and should stay as quiet as possible to focus eyes on a point in front of them. Self-paced, brisk voluntary abduction of the right index a rate of every 4-5 seconds were performed sequentially and the surface electromyography (EMG) on the first dorsal interosseous (FDI of the experiment at index) were recorded simultaneously. This experiment was recorded more than 10 minutes at least. Not all patients received the electroencephalographic recording, except for two patients (Patient No. 4 and 5 seen in Table 3.1) although paired pulse magnetic stimulation was performed in all subjects. 23.
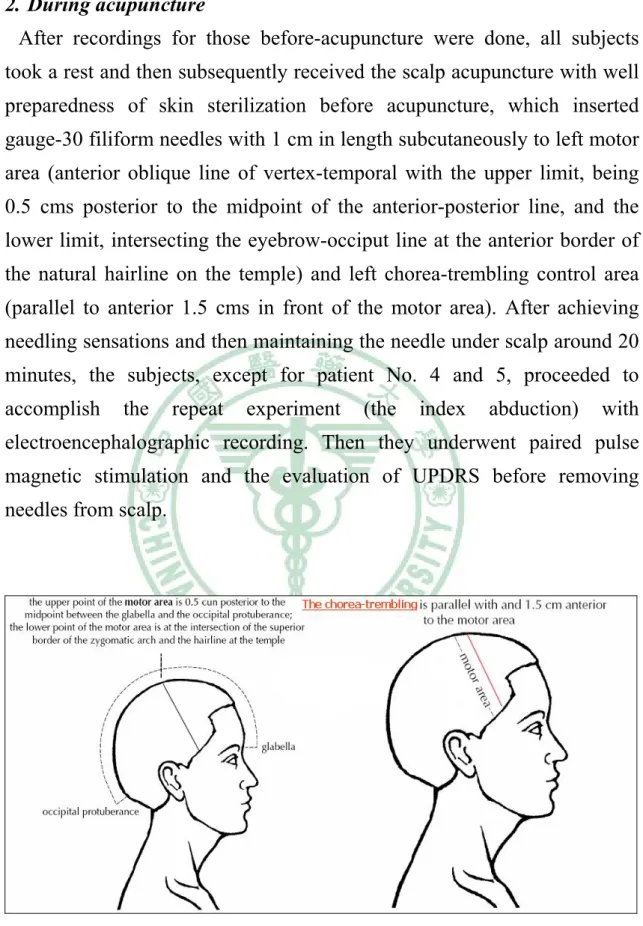
(31) 2. During acupuncture After recordings for those before-acupuncture were done, all subjects took a rest and then subsequently received the scalp acupuncture with well preparedness of skin sterilization before acupuncture, which inserted gauge-30 filiform needles with 1 cm in length subcutaneously to left motor area (anterior oblique line of vertex-temporal with the upper limit, being 0.5 cms posterior to the midpoint of the anterior-posterior line, and the lower limit, intersecting the eyebrow-occiput line at the anterior border of the natural hairline on the temple) and left chorea-trembling control area (parallel to anterior 1.5 cms in front of the motor area). After achieving needling sensations and then maintaining the needle under scalp around 20 minutes, the subjects, except for patient No. 4 and 5, proceeded to accomplish. the. repeat. experiment. (the. index. abduction). with. electroencephalographic recording. Then they underwent paired pulse magnetic stimulation and the evaluation of UPDRS before removing needles from scalp.. Fig. 3.2. Scalp points. 24.
(32) On-off experimentation Following chart of On-Off experimentation UPDRS in “off phase” ▼ First transcranial magnetic stimulation ▼ Taking anti-parkinsonian drugs led to “on phase”, at last 30 min later and identified by subjective and objective improvement ▼ Second transcranial magnetic stimulation Fig. 3.3. Following chart of On-Off experimentation. All experiment steps are similar to those in acupuncture experimentation, except electroencephalographic records and acupuncture treatment. The six patients received twice evaluations of paired pulse magnetic stimulation and UPDRS during the “off phase”, and “on phase”. The “on phase” is identified while subjective and objective improved in Parkinsonian symptoms at last 30 min after taking anti-parkinsonian drugs. In general, the interval of twice evaluations is more than 40 min. Electroencephalographic recording (MRCP) Ten. Ag/AgCl. electrodes. were. placed. on. the. scalp. for. the. electroencephalogram (EEG) recording with four electrodes on the midline (Fz, FCz, Cz, Pz) and three pairs of electrodes on the lateral sites (F3-F4, C3-C4, P3-P4). One electrode below the left outer canthus was set for the electro-oculogram (EOG) recording. The electrode impedance was below 5 kΩ. All electrodes were referenced to the linked earlobes and the signals were filtered with a band pass of 0.05 to 70 Hz (NeuroScan SynAmps, Neurosoft, Inc. Sterling, Va, USA). Surface EMG activity was recorded with a pair of electrodes taped over the first dorsal interosseous (FDI), rectified and filtered with a bandpass of 30-200 Hz. The signals were sampled in rate of 1 KHz for each channel. EEG, EOG, and EMG data were stored digitally for off-line analysis. We selected the epoch period from 2,000 msec before to 1,000 msec after EMG burst onset. Around 100 artifact-free EEG sweeps 25.
(33) of each experiment were averaged after precise alignment with the EMG burst onset. The baseline was corrected from the first 300 msec (2000 to 1700 msec prior to movement onset). The averaged waveforms, as Motor-Related Cortical Potential (MRCP), in the midline frontal (FCz & Fz), vertex (CZ), parietal (Pz) and lateral (F3-F4, C3-C4, P3-P4) area were obtained to determine the alterations among experiments before and during acupuncture. Paired pulse magnetic stimulation (cortico-cortical inhibition) Throughout the study, the subjects were awake and seated with their hands resting on the chair arms. Surface electromyogram (EMG) recording from the first dorsal interosseous (FDI) was made using silver/silver chloride electrodes in right hand. The EMG signals were amplified by Nicolet IIIP, filtered from 3 Hz to 2 KHz, digitized (sampling rate 1 kHz per channel), processed with CED 1401 plus (Cambridge Electronic Device, UK), and stored on a computer. The impedance between the cathode and anode was kept below 5 kΩ during the study. The motor cortex in left hemisphere was stimulated to use a MAGSTIM 200 (Whitland, Dyfed UK) with a figure-of-8 coil with external loop diameters of 9 cm, placed at the optimum scalp position to elicit motor responses in the contralateral FDI. Two different orientations of the stimulating coil over the motor strip were used, with the induced current flowing either in a latero-medial (LM) or in a posterior-anterior (PA) direction, and stimulating intensities were expressed as a percentage of the maximum output of the stimulator. Threshold is determined for both relaxed and tonically active muscle. Thresholds were defined as the stimulus intensity required to produce a motor evoked potential (MEP) of at least 100 μV peak-to-peak amplitude in at 50% of consecutive trials with the tested muscle at rest. Resting threshold was determined during complete electrical muscle silence; active threshold was determined during a tonic contraction of 5% maximum voluntary contraction.. 26.
(34) Two magnetic stimuli converged onto a Bistim module. [20]. (Whitland,. Dyfed, UK) were delivered through the same stimulating coil over the motor cortex. The study was performed with the target muscle at rest. Paired-pulse TMS (Conditioned stimulus) was performed with the first (conditioned) stimulus intensity, set 5% (of stimulator output) below the active threshold, and the second (test) stimulus, adjusted to evoke a muscle response over the relaxed FDI with a peak-to-peak amplitude of approximate 1 mV. Interstimulus intervals (ISIs) between 1 and 17 msec (2, 3, 4, 5, 6, 8, 11 and 16) were investigated. Conditioned and unconditioned stimuli were randomly intermixed, by programmed pulses from CED 1401 plus, and given every 10 s. At least 10 conditioned and 10 unconditioned trials were collected in each subject for each ISI. The peak-to-peak amplitudes of magnetic conditioned MEPs were compared with the average amplitudes of unconditioned MEPs and expressed as a percentage of the size of the amplitude of the unconditioned response. Statistical Analysis for data As early and late BP onset latencies were usually difficult to identify precisely and reliably, we measured the 1500 ms before the motor onset (MO) as a rough estimate of the (early) BP onset and 500 ms before MO as negative slow (NO’, late BP) onset [18,19]. By using Student's t tests, the three areas, one from 1500 ms to 500ms before MO, another forward 500 ms before MO and the last combining both, were compared before and during acupuncture. For each experimentation and groups, Student's t tests were also capable of measuring the alteration between responses in some ISIs of paired pulse magnetic stimulation before and during acupuncture, or during “off phase” and “on phase”. The parametric one-way analysis of variance (ANOVA) was used for the measure of difference among ISIs in each procedure of paired pulse magnetic stimulation. Significance was set at P< 0.05 for all tests. Data are expressed as means ±S.D. in the text and are illustrated as means ±S.E.M. 27.
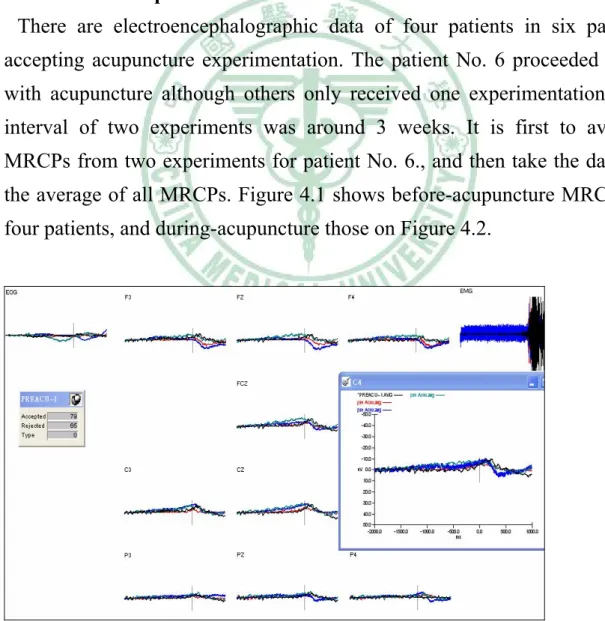
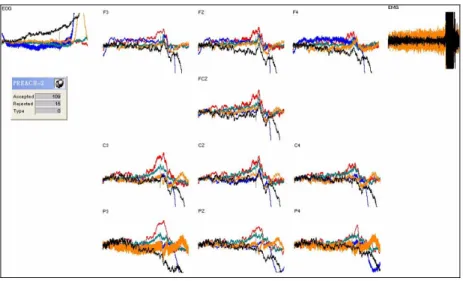
(35) Chapter 4 Results All patients didn’t feel predominant improvement in Parkinsinian symptoms through acupuncture although no advanced events developed. Also there were no differences in UPDRSIII (the motor section of UPDRS). Electroencephalographic data (MRCP analysis) In Parkinsonian patients: There are electroencephalographic data of four patients in six patients accepting acupuncture experimentation. The patient No. 6 proceeded twice with acupuncture although others only received one experimentation. The interval of two experiments was around 3 weeks. It is first to average MRCPs from two experiments for patient No. 6., and then take the data for the average of all MRCPs. Figure 4.1 shows before-acupuncture MRCPs of four patients, and during-acupuncture those on Figure 4.2.. Fig. 4.1. MRCPs before acupuncture in four PD patients 28.
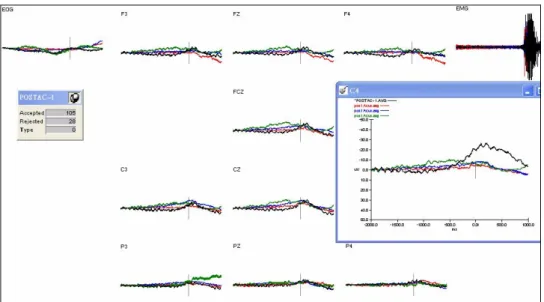
(36) Fig. 4.2. MRCPs during acupuncture in four PD patients. The average of MRCP during acupuncture was compared with before acupuncture (shown on Figure 4.3).. Fig. 4.3. The MRCP during (gray) versus before (black) acupuncture. For each electroencephalographic data from acupuncture experimentation, we subtracted the MRCPs before acupuncture from those during acupuncture to get certain computed potentials. Then we measured the areas of in three time intervals, one from 1500 ms to 500ms before MO (equal to 29.
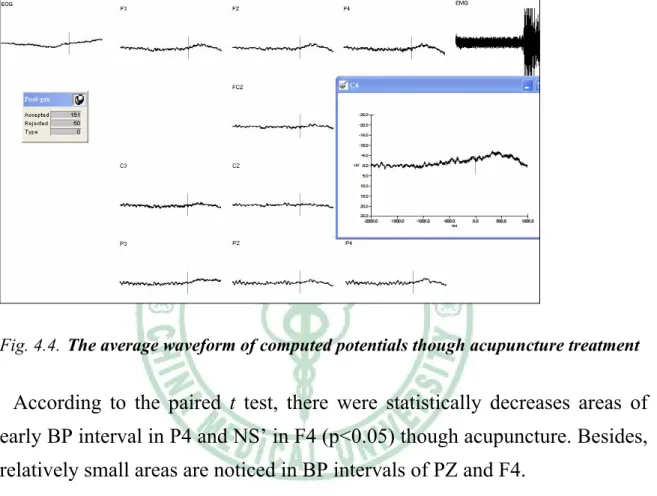
(37) the interval of early BP, named as early BP interval), another forward 500 ms before MO (equal to NS’ interval, named as NS’ interval) and the last combining both (equal to whole BP interval, named as BP interval), in order to test the alteration of MRCPs though acupuncture treatment. Figure 4.4 appears the average waveform from computed potentials of four patients.. Fig. 4.4. The average waveform of computed potentials though acupuncture treatment. According to the paired t test, there were statistically decreases areas of early BP interval in P4 and NS’ in F4 (p<0.05) though acupuncture. Besides, relatively small areas are noticed in BP intervals of PZ and F4. In normal controls: There was statistically increased area of the BP interval in C4 though acupuncture (p<0.05) that was associated with relatively enlargement in NS’ areas in CZ and C4. No markedly altered area was defected in any early BP interval. The electroencephalographic data of five volunteers MRCPs before and during acupuncture was presented on Figure 4.6 and 4.6, respectively, and the average comparison had shown on Figure 4.7. 30.
(38) Fig. 4.5. All MRCPs before acupuncture in controls. Fig. 4.6. All MRCPs during acupuncture in controls. Fig. 4.7. The MRCP during (gray) versus before (black) acupuncture in controls 31.
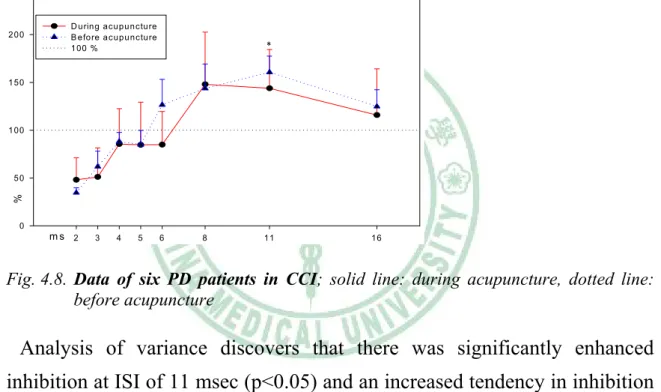
(39) Cortico-cortical inhibition (CCI) The effects of acupuncture in PD patients: Ipsilateral ortico-cortical inhibition was investigated over ISIs from 2 to 16 msec. A comparison between the mean data of response percentages before and during acupuncture from six patients was shown on Figure 4.8. Because of twice acupuncture in patient No. 6, it is first to average the mean of same ISIs within two experiments, later added to mean data with other patients. 2 50. 2 00. D uring acupu ncture B efore a cupu ncture 1 00 %. *. 1 50. 1 00. %. 50. 0. ms 2. 3. 4. 5. 6. 8. 11. 16. Fig. 4.8. Data of six PD patients in CCI; solid line: during acupuncture, dotted line: before acupuncture. Analysis of variance discovers that there was significantly enhanced inhibition at ISI of 11 msec (p<0.05) and an increased tendency in inhibition during the ISI at 6 msec whereas relatively less inhibition at ISI of 2 msec. We. identified. whether. one. treatment. was. sufficient. to. effect. cortico-cortical inhibition for a patient or not, according to calculating differences in response percentages at same ISIs and areas under curves, consisting of response percentage points at ISIs and lines between them. An insufficient effect was identified if there were diminishing area and response percentages at five ISIs or more after acupuncture or medicinal treatment. By this rule, last acupuncture of patient No. 6 failed to make sufficient effect on cortico-cortical inhibition (seen on Figure 4.9). 32.
(40) 500. 400. D uring a cup uncture 10 0% B efo re a cup uncture. 300. 200. %. 100. 0. ms 2. 3. 4. 5. 6. 8. 11. 16. Fig. 4.9. The data of last acupuncture in patient No.6; solid line: during acupuncture, dotted line: before acupuncture. After excluding data of acupunctural treatment with insufficient effect, we could establish new data of response percentages at all ISIs that were shown on Figure 4.10. 250. 200. During acupuncture 100 % Before acupuncture. *. *. 150. *. 100. %. 50. 0. ms 2. 3. 4. 5. 6. 8. 11. 16. Fig. 4.10. Data except the treatment with insufficient inhibition; solid line: during acupuncture, dotted line: before acupuncture. Significantly increased inhibition developed at ISIs of 6, 11 and 16 msec (p<0.05) regardless of the tendency to decrease inhibitory at ISI of 2 msec.. 33.
(41) In normal controls: We builded up a comparison between the data of response percentages before and during acupuncture from five volunteers shown on Figure 4.11. 250. 200. D u rin g a c u p u n c tu re B e fo re a c u p u n c tu re 100%. 150. 100. %. 50. 0. ms 2. 3. 4. 5. 6. 8. 11. 16. Fig. 4.11. Data of normal controls; solid line: during acupuncture, dotted line: before acupuncture. Although the curve of data during acupuncture went under the one before acupuncture after ISI of 4ms in vision of Figure 4.11, there is no statistically significant variance at all ISIs. Parkinsonian patients during On and Off phases: There was no statistically significant inhibition at all ISIs by a comparison between the means from six patients during on and off phases shown on Figure 4.12. 300. 250. 200. 150. 100. On O ff 100%. %. 50. 0. ms 2. 3. 4. 5. 6. 8. 11. 16. Fig. 4.12. Data of six patients (on & off phases); red: solid line: On phase, dotted line: off phase 34.
(42) But “on phase”, induced by anti-parkinsonian, in patient No. 11 developed an insufficient effect on cortico-cortical inhibition (seen on Figure 4.13) in accordance with described rules. So Figure 4.14 shows new data of ISIs after excluding that treatment with insufficient inhibition. 250. 200. 150. 100. 50. %. On 100% O ff. 0. ms. 2. 3. 4. 5. 6. 8. 11. 16. Fig. 4.13. The data of patient No.11 * 300. *. 200. 100. %. On O ff 100%. 0. ms. 2. 3. 4. 5. 6. 8. 11. 16. Fig. 4.14. Data except the treatment with insufficient inhibition (on & off phases); solid line: On phase, dotted line: off phase. Significantly inhibition builded at ISIs of 4 and 8 msec (p<0.05) with predominant tendency toward inhibition at 6 msec. Besides, curves of the data during “on phase” always went under those during “off phase” in visions of Figure 4.13 and 4.14. 35.
(43) Comparison of degrees in inhibition effect: We subtracted the mean before acupuncture or during “off phase” from those during acupuncture or “on phase” to get variance and to test degrees of inhibition effect. 100 A c u p u n c tu r e in h ib itio n in P a r k in s o n ia n p a tie n ts e x c lu d in g th e tr e a tm e n t w ith in s u ffic ie n t in h ib itio n z e r o lin e N o r m a l c o n tr o ls. 50. 0. -5 0. % -1 0 0. ms. 2. 3. 4. 5. 6. 8. 11. 16. Fig. 4.15. Acupuncture inhibition in Parkinsonian patients excluding the treatment with insufficient inhibition versus normal controls. Acupuncture inhibition started to affect responses at ISIs longer than 5 msec with comparison of even facilitation at short intervals (3 & 4 ms) in controls (dotted line on Fig. 4.15). Anti-parkisonian played an inhibitory role at all ISIs in PD, while were predominant at 6 and 8 msec (dotted line on Fig. 4.16). According to inhibitory findings of acupuncture in PD (solid lines on Fig. 4.15 & 4.16), there was relatively weaker inhibition at short intervals than anti-parkisonian effect. 100 A c u p u n c tu re in h ib itio n in P a rk in s o n ia n p a tie n ts e x c lu d in g th e tre a tm e n t w ith in s u ffic ie n t in h ib itio n z e ro lin e A n ti-p a rk is o n ia n in h ib itio n e x c lu d in g th e tre a tm e n t w ith in s u ffic ie n t in h ib itio n. 50. 0. -5 0. % -1 0 0. ms. 2. 3. 4. 5. 6. 8. 11. 16. Fig. 4.16. Acupunctural inhibition versus Anti-parkisonian (either excluding the treatment with insufficient inhibition) 36.
(44) Chapter 5 Discussion The use of alternative therapies is common in patients with Parkinson’s disease. Forty percent of patients reported the use of at least one form of alternative therapy in a systematic survey of 201 patients with Parkinson’s disease. Acupuncture was among the most frequently used treatment modalities. The majority of patients had not discussed the use of alternative treatments with their treating physician [7]. A non-blinded, pilot trial was conducted to assess the safety, tolerability and efficacy of acupuncture for the symptoms of Parkinson’s disease [6,7]. Twenty patients received 10 to 16 sessions of acupuncture therapy by a licensed acupuncturist. Broad batteries of tests were used to evaluate the response, including quantitative tests of motor function, UPDRS, H & Y, Beck Depression and Anxiety Inventories, and the Sickness Impact Profile (SIP). Although 85% of patients reported subjective improvement of individual symptoms, the only objective improvement of significance was in the sleep and rest subcategory of the SIP. Acupuncture was well tolerated, and no adverse effects were reported. There were no statistically significant differences in UPDRSIII, Parkinson's disease Questionnaire (PDQ-39 and PDQ-8 Summary Index) and Geriatric Depression Scale between controls and patients from a double-blind pilot study for evaluation of acupuncture in the treatment of Parkinson’s disease. [32]. . But the lasting periods of. acupuncture treatments (usual for 3 months) were longer in observational studies of groups of patients reported in the Chinese medical literature [5,10,12], and above trials had lack of individualization of the treatments. In our study, there was neither alteration in UPDRSIII, nor subjective improvement in motor symptoms for all patients through acupuncture although no any advanced event happened. But it does not demonstrate that there is no evidence of long-term benefit according to the result in our study that was 37.
(45) designed to evaluate short-term acupuncture effect. According to the evidence-based medicine levels of evidence by the work of Chris Ball, Dave Sackett, Bob Phillips, Brian Haynes, Sharon Straus, and Martin Dawes, our study is an individual case-control trial that only has the evidence of level 3b (seen in Table 5.1). However, the original design of this study was to focus on acupunctural mechanism and not only to evaluate acupunctural outcome. Table 5.1. Oxford Centre for Evidence-based Medicine Levels of Evidence Level. Therapy/Prevention, Aetiology/Harm SR (with homogeneity) of RCTs. 1b. Individual RCT (with narrow Confidence Interval). 1c. All or none. 2a. SR (with homogeneity) of cohort studies. 2b. Individual cohort study (including low quality RCT; e.g., <80% follow-up). 2c. "Outcomes" Research; Ecological studies. 3a. (with homogeneity) of case-control studies. 3b. Individual Case-Control Study. 4. Case-series (and poor quality cohort and case-control studies). 5. Expert opinion without explicit critical appraisal, or based on physiology, bench research or "first principles". * *. 1a. SR: systematic review; RCT: random control trial Produced by Bob Phillips, Chris Ball, Dave Sackett, Doug Badenoch, Sharon Straus, Brian Haynes, Martin Dawes since November 1998. By regulating energetic imbalances within the organism, the insertion of acupuncture needles in specific acupoints have a therapeutic benefit on nearby or distant organs via “meridians”(經絡), as a network of channels to connect functional organic systems according to the theory of the traditional Chinese medicine. According to recent neuropharmacological and neuroimaging data, many of the effects of acupuncture might be mediated by the activation of disease-related areas within the central nervous system. For example, different kinds of opioid neuropeptides are released by stimulation of analgesic acupoints, which may cause the activation of many areas of the 38.
(46) limbic ⁄ paralimbic systems involved in pain mediation. Furthermore, stimulation of eye-related and language-related acupoints has been shown to activate cortical areas implicated in vision, auditory and language processing, respectively [26]. If multiple brain areas are activated by acupuncture, this may be the consequence of the stimulation of somatosensory afferent fibres, produced by needle insertion. According to measuring MEP by TCM, Maioli. [26]. demonstrated that simple insertion of the acupuncture needle, which produces only a very mild, localized and short-lasting somatosensory stimulation, is sufficient to induce a significant modulation of excitability of the motor pathways that depart from the primary motor cortex; acupunctural effects can hardly be ascribed to nonspecific changes in whole-system excitability; changes in MEP amplitude following acupuncture depend on the stimulation point and the investigated muscle, and the elicited responses strongly depend on the needling point. Our study found similar discovery (not shown in above results) that MEPs were increased significantly in four controls through acupuncture but not in all Parkisonian patients. In controls, we found acupuncture inhibition started to affect responses in ISIs longer than 4 msec, and enhanced potentials were present in BP and NS’ intervals of EEG on the central scalp and right-side near vertex, not predominant in early BP intervals from any electrode recording. Although PD represented the dysfunction of early BP[18] and cortico-cortical inhibition at short ISIs less than 5 msec[29], scalp acupuncture didn’t play a role in the set of our data in regardless of relatively strong inhibition at ISIs longer than 5 msec in cortico-cortical inhibition by acupuncture. Therefore, short-term treatment of scalp acupuncture could not give our patients a great benefit on motor symptoms immediately. Lastly, we speculate that acupunctural inhibition at longer ISIs, more than 5 msec in paired pulse magnetic stimulation, may result from the somatosensory input of contra lateral sensory cortex via the stimulation of scalp acupuncture.. 39.
(47) In initial request, the scalp needle should be rotated about 200 times per minute during therapy approach. [11]. , which may give rise to strong. somatosensory stimulation in order to enhance certain activity in central nerve system, such as modulation of excitability of the motor pathways via organisational change within the motor and sensory cortex. In our study, scalp needles were maintained subcutaneously without other management after achieving needling sensations, which might be difficult to reach requested strength for acupuncture. The electro-acupuncture may be a stable tool instead of strong manual management and considered to be used in future study.. 40.
(48) Chapter 6 Conclusion Acupuncture is safe and well tolerated without adverse effects for alternative therapy in patients with Parkinson’s. It is an argument if (scalp) acupuncture improves motor symptoms of PD before of ambiguous evidences in clinical trials. All patients didn’t feel predominant improvement in Parkinsinian symptoms. Although our patients didn’t take any short-term benefit in Parkinsinian symptoms through scalp acupuncture, there were some electrophysical effects in distant for patients and normal controls. Therefore, it is essential to arrange further and long-term studies to ascertain physical mechanism for acupuncture.. 41.
(49) References 1.. Gelb DJ, Oliver E, Gilman S. Diagnostic criteria for Parkinson disease. Arch Neurol.1999;56:33-39. 2.. Calne DB, Snow BJ, Lee C. Criteria for diagnosing Parkinson's disease. Ann Neurol. 1992;32:125-127. 3.. Manyam BV, Sanchez-Ramos JR. Traditional and complementary therapies in Parkinson's disease. Adv Neurology. 1999;80:565-74.. 4.. He J, Wei H, Yuan C, Gu M, Chen R. Present situation and prospects of TCM treatment of Parkinson's disease. J Tradit Chin Med. 2004;24:308-314.. 5.. Zhuang X, Wang L. Acupuncture treatment of Parkinson's disease-a report of 29. J Tradit Chin Med. 2000;20:265-267.. 6.. Shulman LM, Wen X, Weiner WJ, Bateman D, Minagar A, Duncan R, and Konefal J. Acupuncture therapy for the symptoms of Parkinson's disease. Mov Disord. 2002;17:799-802. 7.. Rabinstein AA, Shulman LM. Acupuncture in clinical neurology. Neurologist. 2003;9:137-148. 8.. Liberini P. Parola S. Spano PF. Antonini L. Olfaction in Parkinson’s disease: methods of assessment and clinical relevance. J Neurol. 2000;247: 88-96. 9.. Huang WY. Influence of electric stimulation of scalp acupuncture on electromyogram in tremor pattern of Parkinson’s disease. Acta Univ Tradit Med Sin Pharmacol Shanghai. 2000;14:38-39. 10. Wang L, He C, Liu Y, Zhu L. Effect of acupuncture on the auditory evoked brain stem potential in Parkinson's disease. J Tradit Chin Med. 2002;22:15-17 11. Liu TH, Sadove MS. Scalp needle therapy - acupuncture treatment for central nervous system disorders. Am J Chin Med. 1974;2:261-269 12. Xue Y. The treatment of Parkinson's disease by acupuncture and herbal 42.
(50) medicine. J Tradit Chin Med. 2003;73: 7-10 13. Lu Shoukang. Scalp acupuncture therapy and its clinical application. J Tradit Chin Med. 1991;11(4):272-280. 14. Bradley WG, Daroff RB, Fenichel GM, Jankovic J. Neurology in Clinical Practice. Elsevier Ltd, Linacre, London 2004; pp. 2131-2138 15. Chen RC, Chang SF, Su CL, et al. Prevalence, incidence and mortality of PD: a door-to-door survey in Ilan county, Taiwan. Neurology 2001;57:1679-1686 16. Shi X. Dr. Shi Yanqing’s experience in acupuncture treatment of paralysis agitans. J Tradit Chin Med. 2004;24(3):188-1190 17. Iwatsuki H. The Relationship between Physical Parameters of Movement and Movement-Related Cortical Potential. J.Phys. Ther. Sci. 2000;12:39-42 18. Shibasaki H, Hallett M. What is the Bereitschaftspotential? Clin Neurophysiol. 2006;117:2341-2356 19. Colebatch JG. Bereitschaftspotential and Movement-Related Potentials: Origin, Significance, and Application in Disorders of Human Movement. Mov Disord. 2007;22(5):601-610 20. Kujirai T, Caramia MD, Rothwell JC, Day BL, Thompson PD, Ferbert A, Wore S, Asselman P. Corticocortical inhibition in human motor cortex. J. Physiol. 1993;471:501-519. 21. Ziemann U, Rothwell JC, Ridding MC. Interaction between intracortical inhibition and facilitation in human motor cortex. J. Physiol. 1996;496:873-881. 22. Rothwell JC. Connections to motor cortex from other areas of the brain studied with transcranial magnetic stimulation. Int. Congr. Ser. 2002;1226:45-52 23. Ridding MC, Taylor JL. Mechanisms of motor-evoked potential facilitation following prolonged dual peripheral and central stimulation in humans. J. Physiol. 2001;537(2):623-631. 43.
(51) 24. Ridding MC, Brouwer B, Miles TS, Pitcher JB, Thompson PD. Changes in muscle responses to stimulation of the motor cortex induced by peripheral nerve stimulation in human subjects. Exp Brain Res. 2000;131:135-143. 25. Charlton CS, Ridding MC, Thompson PD, Miles TS. Prolonged nerve stimulation induces persistent changes in excitability of human motor cortex. J. Neurol. Sci. 2003;208:79-85. 26. Maioli C, Falciati L, Marangon M, Perini S, Losio A. Short- and long-term modulation of upper limb motorevoked potentials induced by acupuncture. European Journal of Neuroscience. 2006; 23:1931-1938, 27. Stefan K, Kunesch E, Cohen LG, Beneke R, Classen J. Induction of plasticity in the human motor cortex by paired associative stimulation. Brain. 2000;123:572-584. 28. Stefan K, Kunesch E, Benecke R, Cohen LG, Classen J. Mechanisms of enhancement of human motor cortex excitability induced by interventional paired associative stimulation. Journal of Physiology. 2002;543(2):699-708 29. Ridding MC, Inzelberg R, Rothwell JC. Changes in excitability of motor cortical circuitry in patients with Parkinson’s disease. Ann Neurol. 1995;37:181-188 30. Tsai CH, Chang FC, Lu CS, Lee ST, Huang YT, Lu MK, Chen RS, Wu T, Lee JD, Weng YH, Chang HC. Pallidotomy effect on the cortical excitability in patients with severe Parkinson’s disease. Mov Disord. 2004;20(4):463-470 31. Yoshino U, Tatsuya M, Mamdouh AK, Hideyuki S, Hidemoto S, Akio I, Tahamina B, Faruque R, Takashi N, Hidenao F. Altered plasticity of the human motor cortex in Parkinson’s disease. Ann Neurol. 2006;59:60-71 32. Cristian A, Katz M, Cutrone E, Walker RH. Evaluation of Acupuncture in the Treatment of Parkinson’s Disease: A double-blind pilot study. Mov Disord. 2005;20(9):1185-1188. 44.
數據

+7
Outline
相關文件
6 《中論·觀因緣品》,《佛藏要籍選刊》第 9 冊,上海古籍出版社 1994 年版,第 1
[14] reported that when patients with osteomyelitis of the jaws were divided into two groups, the ones undergo- ing BP treatment and the others taking no BP, Actinomyces
large cystic, and expansile lesion :位在 left ramus of mandible,皮質骨有變薄的現象 - Provisional diagnosis: Ameloblastoma or odontogenic keratocyst. -
pylori in pathogenesis of oral mucosal lesions or ulcerations is still unclear, it seems that patients with oral lesions as leukoplakia and oral lichen planus, and concurrent
In cases of anterior intrabony maxillary midline lesions with cortical erosion, entities such as nasopalatine duct cyst, keratocystic odontogenic tumor, periapical in-
CT scans showed expansile and densely mineralized lesions in all four quadrants with the left posterior mandible showing a focal penetration of the buccal cortical bone..
Although Taiwan stipulates explicit regulations governing the requirements for organic production process, certification management, and the penalties for organic agricultural
A discussion of the Dapagli flozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) trial, the Effect of Sotagli flozin on Car- diovascular Events in Patients
