Original Article
Strategies for Diabetes Self-Care Intervention and Education in Elderly Patients with Suboptimal Controlled Type 2
Diabetes: A Pilot Study
Ting-Wen Chia RN, CDE
1, Chien-Ning Huang MD, PhD
2,3, Ching-Ru Li RN, CDE
4, Yueh-Chu Wu RN, CDE
4, Yu-Tze Lin RN, CDE
4, Yi-Sun Yang, MD PhD
2,31 Department of Nutrition, Chung Shang Medical University Hospital, Taichung, Taiwan
2 Division of Endocrinology and Metabolism, Department of Internal Medicine, Chung Shang Medical University Hospital, Taiwan
3 Institute of Medicine, School of Medicine, Chung Shan Medical University, Taichung, Taiwan
4 Department of Nursing, Chung Shang Medical University Hospital, Taiwan
Introduction
In aging societies diabetes is an important health issue. About 20% of people aged 65 and above have diabetes (1- 2) and this proportion is expected to
increase rapidly in the coming decades. Diabetes is a chronic disease that requires a multitude of daily self-management decisions and complex care activities. Among patients with chronic disease, there is growing interest in “self-management” programs (3). Diabetes self-management education (DSME), a complex health intervention, is generally effective for enhancing self-care behaviors, improving glycemic control, lowering health care costs, and improving quality of life (4-6).
Older adults with diabetes are at greater risk than those without diabetes for several common geriatric syndromes, such as polypharmacy, cognitive impairment, sarcopenia, injurious falls, and
* Correspondence to: Yi-Sun Yang
Division of Endocrinology and Metabolism, Department of Internal Medicine, Chung Shan Medical University Hospital, Chung Shan Medical University, 110 Sec. 1, Jianguo N. Road, Taichung 40201, Taiwan.
Tel: +886-4-24739595 ext. 34711 Fax: +886-4-24739220
E-mail: [email protected]
The aim of this pilot study is to test the hypothesis that different diabetes self-management strategies can improve glycemic control in elderly patients with diabetes. Patients with suboptimal glycemic control were selected from outpatient clinic and randomly assigned to (1) breakfast meal-replacement;
(2) peer-support; and (3) group session only groups. HbA1c reductions of 0.8% and 1.01% were noted from the baseline value to 12 weeks in the meal-replacement and peer-support groups, respectively. In addition, greater body weight reduction was observed in the meal replacement and peer-support groups.
This reduction was associated with not only nutritional knowledge improvement but also decreased daily carbohydrate intake. A combination of conventional disease management education and peer- support or breakfast meal-replacement was found to be useful in elderly diabetic patients in terms of their ongoing diabetes self-care. Such combinations are easy to implement and effective for achieving glycemic control.
Keywords: meal replacement, peer support, type 2 diabetes, group education, diabetes self- management education
persistent pain (7-9). These conditions may impact older adults’ diabetes-related self-care tasks (10) and their ability to maintain the timing and content of meals. Some elderly diabetic patients find it difficult to understand conventional dietary and nutritional education based on food exchange lists (11). Even if they do understand such a system, they may have difficulty changing their daily eating habits (12). Thus, clinicians and diabetes educators need to simplify diabetes management strategies for elderly patients.
From previous studies on diabetes education interventions, patients have difficulty maintaining intervention responses over an extended period (13-14). One possible reason is that patients who struggle with self-management and glycemic control need more structured strategies to help them develop and maintain lifestyles and behaviors over the long term (15).
A rational approach may be the reinforcement of diabetes education or development of simple skills to maintain self-care behaviors at different points throughout the course of their diabetes. However, few well-designed randomized controlled trials have examined the value of reinforcing diabetes self-care or the best method of reinforcement.
One method is telephone-based peer support using protocols with predefined processes, treatment targets, and regular feedback (16-17). Peer support has the potential to address barriers to successful diabetes self-management, as well as to emphasize sustained behavioral change (18-19). Moreover, studies have demonstrated that meal replacement is an alternative dietary approach for improving blood glucose control (20- 21). Re-organizing nutritional strategies to provide a simple meal plan can facilitate high compliance with dietary regimens on a lifelong basis (22). Thus, meal replacement is easier to understand, teach, and implement than other approaches.
To test the hypothesis that different models for reinforcing diabetes self-management can improve glycemic control in elderly patients with diabetes, we carried out a pilot study with change in glycated hemoglobin (HbA1c) as the primary outcome.
Methods
The eligibility criteria were diagnosis of type 2 diabetes according to 2016 ADA criteria, age
≥ 60 years, body mass index (BMI) ≥ 24 kg/
m2, and HbA1c ≥ 8.0 %. Exclusion criteria were dementia, cancer, or other severe disease that might interfere with participation. This study was conducted between January and December 2016 in the Department of Endocrinology and Metabolism of Chung Shan Medical University Hospital in Taiwan. The Institutional Review Board of this hospital approved this study, which was conducted according to Declaration of Helsinki guidelines (IRB-CS13227). Informed consent was obtained from all participants in this study.
All participants received a structured DSME program. This program was delivered in a four- hour session, in a group format, with each group consisting of 5-10 patients, facilitated by a certified diabetes nurse educator. The themes delivered were:
1. Understanding the factors involved in managing diabetes and its complications; 2. Understanding healthy eating and being active; 3. Living with diabetes; and 4. Self-monitoring of blood glucose.
After the structured DSME program, participants were randomly assigned to one of three groups: 1) meal-replacement; 2) peer-support, and 3) group session only (Figure 1). Randomization was based on a single sequence of random assignments. A random number table was compiled from computer- generated random numbers.
Subjects in the meal-replacement group were instructed to consume a 300 kcal/day breakfast with diabetes-specific nutritional formula and choice of one serving of bread, cereal, or rice for 6 weeks. The diabetes-specific nutritional formula (Glucerna®, Abbott Nutrition) was a low-glycemic index liquid meal of 250 ml, containing 214 calories, 47.3% carbohydrates, 20% protein, and 32.7% fat. It was provided every week to ensure adherence. The peer-support group received a two-hour training course in peer communication skills following the group session. Training was conducted by diabetes nurse educator and focused on empathic listening, positive thinking, appropriate questioning, clarification of values and life goals, problem solving, and assertiveness.
Peer support one-on-one meetings were held to
listen to and discuss concerns. In addition, weekly support was provided via telephone call or message.
Participants in this group were asked to record every phone call or message sent in a logbook, which was reviewed by a diabetes educator every week to ensure compliance. For group session only group, no further instruction was given following the initial 4-hour group session. During the study period, no adjustments to prescribed medications were made, unless urgent (hyperglycemia, fasting blood glucose > 300 mg/dl or hypoglycemia glucose < 70 mg/dl).
The primary endpoint was HbA1c change from baseline to 12 weeks. Changes in body weight, blood pressure, fasting plasma glucose, lipid levels, nutritional knowledge, nutritional behavior, and diet were surveyed as secondary endpoints.
Nutritional knowledge test was comprised of 10 questions, with a total score of 10 points. The higher the score, the higher the nutritional knowledge.
There were 16 questions on the eating behavior test, with a total score of 80 points. The higher the score, the better the eating behavior.
Demographic data, medical history, laboratory
data, and food records were collected at baseline and subsequent visits. Dietary intake was evaluated using the patient’s three-day food records at baseline and 12 weeks.
Statistical analysis
Continuous variables are presented as mean
± standard deviation (SD) for the descriptive characteristics of the patients in each group.
Categorical variables are presented as percentages.
The differences between baseline and 12-week measurements determined the changes within each educational setting for most of the study variables, with paired Student’s t-tests and one-way ANOVA used to examine the data among the three groups.
χ2 tests were applied to comparisons of categorical variables between treatment arms and at 12-weeks and two sample t-tests were applied to comparisons of continuous variables.
Results
The 60 participants, 20 in each group, who completed the 12-week trial were included in the Figure. 1 Study design
Structured group education (4-hours):
1. Understanding the factors involved in managing diabetes and its complications;
2. Understanding healthy eating and being active;
3. Living with diabetes;
4. Self-monitoring of blood glucose
Peer-support Group session only
Meal-replacement
Diabetes-specific nutritional supplement
for 6 weeks at breakfast: 300kcal/day
At least one phone call or message every 7
days for 6 weeks To follow: Self-monitoring
of blood glucose, body weight, physical activity,
and diet reminders
Management of diabetes on a day-to-day basis
Figure. 2 Study flow chart for intervention Meal-replacement
(n=20) Group session only
(n=20) Not meeting inclusion criteria (n=6)
Declined to participate (n=2)
Peer-support (n=20) Randomized
(n=60)
Assessed Eligibility (n=68) HbA1c ≥ 8%
BMI > 24 kg/m2 Age > 60y
At 12 weeks
Primary end point: HbA1c change from baseline to 12 weeks. Secondary end points: body weight, blood pressure, fasting plasma glucose,
lipid levels, nutritional knowledge, nutritional behavior, and diet.
No treatment adjustment
Follow- up Analysis
Allocation
Enrolled
Excluded
Figure. 3A Changes in HbA1c in the three groups from
baseline to 12 weeks Figure. 3B Changes in body weight in the three groups from baseline to 12 weeks
analyses (Figure 2). Baseline characteristics are shown in Table 1. There were significant changes in HbA1c in the meal-replacement and peer- support groups (Figure 2A). Reductions in HbA1c of 0.8% and 1.01% from baseline values were noted in meal-replacement and peer-support groups, respectively. Mean HbA1c decreased from 8.6%
±1.3% to 7.7% ± 0.8% and from 8.5% ± 2.0% to 7.5% ± 7.5% in meal-replacement and peer-support groups, respectively. In the group session only
group, mean HbA1c decreased from 8.5% ± 1.1 % to 8.3% ± 0.9% (P=0.693). At the end of the study period, there were significant differences in body weight reduction among the groups. Mean body weight decreased from 64.2 ± 12.7 kg to 62.8 ± 12.1 kg and from 65.4 ± 8.0 kg to 64.4 ± 8.3 kg in meal- replacement and peer-support groups, respectively (Figure 2B). In group session only group, the mean body weight changed from 68.4 ± 13.2 kg to 68.6 ± 12.5 kg (P=0.473). The comparisons of Table 1. Baseline Characteristics of Study Participants
Age, years
Educational level Gender (Men)
Illiterate
Duration of diabetes (years) Elementary school
Junior high school and above
Family history of diabetes (yes)
DBP (mmHg) Weight (kg) SBP (mmHg)
FPG (mg/dl) HbA1c (%)
LDL-cholesterol (mg/dl) Triglycerides (mg/dl) HDL-cholesterol (mg/dl)
Group session only (n = 20)
10 (50)
9 (45)
10 (50) 12.4±10.4
8.5±1.1 97.9±28.0
6 (30)
42.6±14.6 65.2±1.4
5 (25)
68.4±13.2 130.5±20.5
72.7±12.3 181.2±84.6
123.3±73.9 Peer-support
(n = 20)
9 (45) 66.4±1.5
11 (60) 5 (20)
10 (50) 4 (20)
65.4±8.0 138.3±18.0
71.5±8.5 158.4±58.1
174.8±136.9 12.5±8.4
8.5±2.0 101.7±33.3
42.5±11.7 Meal-replacement
(n = 20)
8 (40) 65.8±1.3
10 (50) 6 (30)
8 (40) 4 (20)
64.2±12.7 144.3±19.6
75.2±11.0 177.6±51.0
176.5±173.0 12.6±6.2
8.6±1.3 95.4±22.8
44.1±11.3
p
0.825 0.246
0.774 0.840
0.628 0.094 0.544 0.509
0.378 0.998
0.957 0.785
0.904
Nutritional knowledge (score) Total-cholesterol (mg/dl)
Nutritional behavior (score) Energy (kcal/day)
Carbohydrate (g/day) Protein (g/day) Fat (g/day)
1600.5±237.3 210.1±37.7
57.2±12.9 173.5±38.8
5.8±1.5 50.1±10.3
61.3±13.2 178.4±35.3
6.1±1.8 48.9±10.6
65.0±11.9 1737.1±219.5
227.4±40.2
63.1±13.8 173.6±38.4
5.9±2.1 49.0±12.7
65.0±11.6 1693.5±149.4
225.7±38.1
67.0±14.3
0.927 0.901 0.754
0.572 0.116 0.321
0.091 Data expressed as mean ± standard deviation (SD) or percentage in parentheses.
SBP, systolic blood pressure; DBP, diastolic blood pressure; FPG, fasting plasma glucose.
Table 3. Change in knowledge and behavior among groups. Nutritional knowledge Nutritional behavior Energy (kcal/day) Carbohydrate (g/day) Protein (g/day) Fat (g/day)
Meal-replacement 0.003 0.000 0.1330.000 0.069P1 0.000 64.6±8.8 1446.1±129.7 60.5±7.5167.9±25.3 59.1±10.112 weeks 9.2±1.0 49.0±12.7 1693.5±149.4 65.0±11.6225.7±38.1 67.0±14.3Baseline 5.9±2.1
Peer-support 0.010 0.025 0.0580.043 0.018P1 0.000 60.3±6.8 1532.8±191.4 60.6±8.0202.8±28.7 54.6±12.112 weeks 8.4±1.2 48.9±10.6 1735.2±213.9 65.0±11.9227.4±40.2 63.1±13.8Baseline 6.1±1.8
Group session only 0.007 0.014 0.9980.000 0.521P2 0.000 0.001 0.400 0.3310.331 0.331P1 0.000 56.1±8.8 1617.6±200.9 60.6±13.1209.6±37.4 56.5±13.2112 weeks 6.8±1.2 50.1±10.3 1600.5±237.3 61.3±13.2210.1±37.7 57.2±12.9Baseline 5.8±1.5 Values are means ± SEM. P1: differences within groups; P2: differences between groups
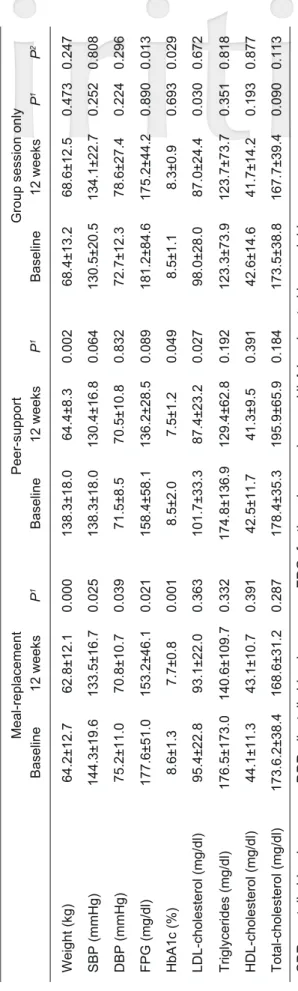
Table 2. Comparisons of blood pressure, fasting plasma glucose, and lipid levelsamong groups Weight (kg) SBP (mmHg) DBP (mmHg) FPG (mg/dl) HbA1c (%) LDL-cholesterol (mg/dl) Triglycerides (mg/dl) HDL-cholesterol (mg/dl) Total-cholesterol (mg/dl)
Meal-replacement 0.025 0.039 0.0010.021 0.332 0.391 0.287P1 0.000 0.363
133.5±16.7 70.8±10.7 7.7±0.8153.2±46.1 140.6±109.7 43.1±10.7 168.6±31.2
12 weeks 62.8±12.1 93.1±22.0
144.3±19.6 75.2±11.0 8.6±1.3177.6±51.0 176.5±173.0 44.1±11.3 173.6.2±38.4
Baseline 64.2±12.7 95.4±22.8
Peer-support 0.064 0.832 0.0490.089 0.192 0.391 0.184P1 0.002 0.027
130.4±16.8 70.5±10.8 7.5±1.2136.2±28.5 129.4±62.8 41.3±9.5 195.9±65.9
12 weeks 64.4±8.3 87.4±23.2
138.3±18.0 71.5±8.5 8.5±2.0158.4±58.1 174.8±136.9 42.5±11.7 178.4±35.3
Baseline 138.3±18.0 101.7±33.3
Group session only 0.808 0.296 0.0290.013 0.818 0.877 0.113P2 0.247 0.672
0.252 0.224 0.6930.890 0.351 0.193 0.090
P1 0.473 0.030
134.1±22.7 78.6±27.4 8.3±0.9175.2±44.2 123.7±73.7 41.7±14.2 167.7±39.4
12 weeks 68.6±12.5 87.0±24.4
130.5±20.5 72.7±12.3 8.5±1.1181.2±84.6 123.3±73.9 42.6±14.6 173.5±38.8
Baseline 68.4±13.2 98.0±28.0
SBP, systolic blood pressure, DBP, diastolic blood pressure; FPG, fasting plasma glucose, HbA1c, glycated hemoglobin Values are means ± SD.
P1: differences within groups; P2: differences between groups
blood pressure, fasting plasma glucose, and lipid levels among groups are shown in Table 2. At the 12-week examination, the three groups reported significantly beneficial changes in nutritional knowledge and behavior. The meal-replacement group improved the most, followed by the peer- support and group session only groups (p< 0.001 between groups). In regards to diet, daily caloric, carbohydrate, protein, and fat content is shown in Table 3. A significant reduction was noted in total daily caloric and carbohydrate intakes in meal- replacement and peer-support groups, compared to group session only group (p < 0.05), with this reduction most prominent in the meal-replacement group.
Overall, compliance was good. About 90% of the peer-support group made a phone call or sent a message every week. Moreover, meal-replacement consumption rate as reported by participants was around 86%.
Discussion
In this study, we examined the use of peer- support and meal-replacement after traditional DSME group session in elderly patients with suboptimal controlled diabetes. The results showed greater improvements in HbA1c, weight, and dietary behavior in the peer-support and meal- replacement groups compared to group session only group. Roughly 20% of all adults aged over 65 have diabetes (1,2). How to best provide diabetes self- management support to this group remains unclear due to limited randomized controlled trial data (1,2).
Older adults are often underrepresented in diabetes education interventions due to subtle changes in their functional, cognitive, and psychosocial statuses, which may affect diabetes self-care (23).
As a result, evidence-based guidelines for this age group are not well established.
A recent analysis of the benefits to older adults with diabetes (aged 60–75 years) of self-management interventions, suggested that older adults receive equal glycemic benefits, when compared with younger adults, from participation in group or individual self-management educational programs (24).
Group education is the most common form of DSME. These educational programs are usually delivered in multiple sessions, such as five 2-h sessions over 6 weeks. However, it has been found that few participants attend all sessions. Unmet personal preferences (e.g. parking, timing) are a barrier to continuous attendance (25). Another study showed that older age and the presence of mental health conditions or other medical comorbidities are associated with low attendance (26). Therefore, developing a simple and effective educational program for the elderly is mandatory. Although physical and mental capacities may have deteriorated in older adults, they still retain the ability to learn and to manage their diabetes.
A single session of DSME with reinforcing of self-care through peer-support or meal-replacement may help elderly patients improve their day-to- day self-management of diabetes. As shown in our study, nutritional knowledge improved in the three groups. However, at 12 weeks, only meal- replacement and peer-support group had better glycemic control and reduced daily carbohydrate intake. Therefore, knowledge alone is not sufficient for good metabolic control.
Continuous behavioral change requires behavioral, educational, psychosocial, or clinical support. In our study, the peer-support concept is of the psychosocial type and meal-replacement is of the clinical type.
Our findings show agreement with the use of meal replacements as a nutritional strategy for glycemic control in type 2 diabetes. They are also consistent with the findings of an earlier study that demonstrated that one meal replacement per day results in HbA1c reduction of 0.6% at 12 weeks (27).
Moreover, they are consistent with most studies on peer-support interventions. According to a systematic review, although studies on peer-support are generally heterogeneous in terms of setting, intervention, study design, length of follow-up, and outcome measures, the average HbA1c reduction is around 0.5% (95% CI, 0.25%-0.70%) (28). The number of participants in this study was relatively small. However, the overall compliance was good, reflecting the feasibility of such interventions for the elderly.
The duration of this study was 12 weeks.
Although this could be considered reasonably long for dietary intervention, a larger sample and a longer follow-up are needed to show whether peer- support intervention or meal replacement has longer term effects on maintaining glycemic control.
During the study period, unless there was severe hyperglycemia or hypoglycemia, no adjustment of prescribed medications was allowed. We recorded a low percentage of prescription adjustment (~5%).
Activity may also affect glycemic status and body weight. However, we did not measure activity in this study, which may have impacted on the results.
In conclusion, using different models for reinforcing diabetes self-management strategies, such as peer-support or meal-replacement, can improve glycemic control in elderly patients with diabetes.
Conflicts of interest
YS Yang has received research grants from Chung Shan Medical University Hospital. CT Wen, CN Huang, Edy Kornelius, CR Li, YC Wu, and YT Lin declare no conflicts of interest.
Acknowledgment
We would like to thank all the patients, physicians, and diabetes educators who collaborated on this study. This study was funded by Chung Shan Medical University Hospital (CSH-2016-A-015).
References
1. Tseng CH, Chong CK, Heng LT, Tseng CP, Tai TY. The incidence of type 2 diabetes mellitus in Taiwan. Diabetes Res Clin Pract 2000;50 Suppl 2:S61-4.
2. Centers for Disease Control and Prevention.
National Diabetes Statistics Report 2017.
3. Lorig KR, Sobel DS, Ritter PL, Laurent D, Hobbs M. Effect of a self-management program on patients with chronic disease. Eff Clin Pract 2001;4(6):256-62.
4. Yang YS, Wu YC, Lu YL, Kornelius E, Lin YT, Chen YJ, et al. Adherence to self-care behavior
and glycemic effects using structured education. J Diabetes Investig 2015;6(6):662-9.
5. Li R, Zhang P, Barker LE, Chowdhury FM, Zhang X. Cost-effectiveness of interventions to prevent and control diabetes mellitus: a systematic review.
Diabetes Care 2010;33(8):1872-94.
6. Lalic NM, Lalic K, Jotic A, Stanojevic D, Zivojinovic D, Janicijevic A, et al. The Impact of Structured Self-Monitoring of Blood Glucose Combined With Intensive Education on HbA1c Levels, Hospitalizations, and Quality-of- Life Parameters in Insulin-Treated Patients With Diabetes at Primary Care in Serbia: The Multicenter SPA-EDU Study. J Diabetes Sci Technol 2017;11(4):746-52.
7. Cukierman T, Gerstein HC, Williamson JD.
Cognitive decline and dementia in diabetes-- systematic overview of prospective observational studies. Diabetologia 2005;48(12):2460-9.
8. Noale M, Veronese N, Cavallo Perin P, Pilotto A, Tiengo A, Crepaldi G, et al. Polypharmacy in elderly patients with type 2 diabetes receiving oral antidiabetic treatment. Acta Diabetol 2016;53(2):323-30.
9. Wang T, Feng X, Zhou J, Gong H, Xia S, Wei Q, et al. Type 2 diabetes mellitus is associated with increased risks of sarcopenia and pre-sarcopenia in Chinese elderly. Sci Rep 2016;6:38937.
10. Kirkman MS, Briscoe VJ, Clark N, Florez H, Haas LB, Halter JB, et al. Diabetes in older adults. Diabetes Care 2012;35(12):2650-64.
11. Takahashi M, Araki A, Ito H. [Development of a new method for simple dietary education in elderly individuals with diabetes mellitus]. Nihon Ronen Igakkai Zasshi 2002;39(5):527-32.
12. Bloomgarden ZT, Karmally W, Metzger MJ, Brothers M, Nechemias C, Bookman J, et al.
Randomized, controlled trial of diabetic patient education: improved knowledge without improved metabolic status. Diabetes Care 1987;10(3):263- 72.
13. Norris SL, Lau J, Smith SJ, Schmid CH, Engelgau MM. Self-management education for adults with type 2 diabetes: a meta-analysis of the effect on glycemic control. Diabetes Care 2002;25(7):1159- 71.
14. Norris SL, Engelgau MM, Narayan KM. Effectiveness of self-management training in type 2 diabetes: a systematic review of randomized controlled trials.
Diabetes Care 2001;24(3):561-87.
15. Beverly EA, Fitzgerald SM, Brooks KM, Hultgren BA, Ganda OP, Munshi M, et al. Impact of reinforcement of diabetes self-care on poorly controlled diabetes: a randomized controlled trial.
Diabetes Educ 2013;39(4):504-14.
16. Chan JC, Sui Y, Oldenburg B, Zhang Y, Chung HH, Goggins W, et al. Effects of telephone-based peer support in patients with type 2 diabetes mellitus receiving integrated care: a randomized clinical trial. JAMA Intern Med 2014;174(6):972- 81.
17. Heisler M, Vijan S, Makki F, Piette JD. Diabetes control with reciprocal peer support versus nurse care management: a randomized trial. Ann Intern Med 2010;153(8):507-15.
18. Simmons D, Cohn S, Bunn C, Birch K, Donald S, Paddison C, et al. Testing a peer support intervention for people with type 2 diabetes: a pilot for a randomised controlled trial. BMC Fam Pract 2013;14:5.
19. Caro JF, Fisher EB. A solution might be within people with diabetes themselves. Fam Pract 2010;27 Suppl 1:i1-2.
20. Li D, Zhang P, Guo H, Ling W. Taking a low glycemic index multi-nutrient supplement as breakfast improves glycemic control in patients with type 2 diabetes mellitus: a randomized controlled trial. Nutrients 2014;6(12):5740-55.
21. Stenvers DJ, Schouten LJ, Jurgens J, Endert E, Kalsbeek A, Fliers E, et al. Breakfast replacement with a low-glycaemic response liquid formula in patients with type 2 diabetes: a randomised clinical trial. Br J Nutr 2014;112(4):504-12.
22. Imai S, Matsuda M, Hasegawa G, Fukui M, Obayashi H, Ozasa N, et al. A simple meal plan of 'eating vegetables before carbohydrate' was more effective for achieving glycemic control than an exchange-based meal plan in Japanese patients with type 2 diabetes. Asia Pac J Clin Nutr 2011;20(2):161-8.
23. Munshi M, Grande L, Hayes M, Ayres D, Suhl E, Capelson R, et al. Cognitive dysfunction is associated with poor diabetes control in older adults. Diabetes Care 2006;29(8):1794-9.
24. Beverly EA, Fitzgerald S, Sitnikov L, Ganda OP, Caballero AE, Weinger K. Do older adults aged 60-75 years benefit from diabetes behavioral interventions? Diabetes Care 2013;36(6):1501-6.
25. Winkley K, Stahl D, Chamley M, Stopford R, Boughdady M, Thomas S, et al. Low attendance at structured education for people with newly diagnosed type 2 diabetes: General practice characteristics and individual patient factors predict uptake. Patient Educ Couns 2016;99(1):101- 7.
26. Cauch-Dudek K, Victor JC, Sigmond M, Shah BR. Disparities in attendance at diabetes self- management education programs after diagnosis in Ontario, Canada: a cohort study. BMC Public Health 2013;13:85.
27. Leader NJ, Ryan L, Molyneaux L, Yue DK.
How best to use partial meal replacement in managing overweight or obese patients with poorly controlled type 2 diabetes. Obesity (Silver Spring) 2013;21(2):251-3.
28. Patil SJ, Ruppar T, Koopman RJ, Lindbloom EJ, Elliott SG, Mehr DR, et al. Peer Support Interventions for Adults With Diabetes: A Meta- Analysis of Hemoglobin A1c Outcomes. Ann Fam Med 2016;14(6):540-51.