S72
0896-8608/08 $3.00 + .00 Copyright © 2008 International Society for Peritoneal Dialysis Printed in Canada. All rights reserved.
Proceedings of the 3rd Asian Chapter Meeting of the ISPD November 22 – 24, 2007, Hiroshima, Japan
Peritoneal Dialysis International, Vol. 28 (2008), Supplement 3
In Taiwan, peritoneal dialysis (PD) was launched in 1984.
Since then, the Taiwan Society of Nephrology (TSN) has taken the responsibility for supervising PD programs. All PD pro- grams are required to pass evaluations from the TSN before inception. Every new PD patient receives individual train- ing from a qualified PD nurse. The training, accompanied by a review test, is usually provided in the hospital during the week right after catheter implantation.
To evaluate the effect of the patient training program on PD outcomes, we designed a retrospective observation study and reviewed the post-training tests of 100 new PD patients.
The post-training test has 10 parts: anatomy and physiol- ogy, overview of chronic kidney disease, overview of PD, complications of peritonitis and exit-site infection, diet control, cardiovascular complications, PD skills and proce- dures, aseptic techniques, management of peritonitis, and routine tasks. The relationship between the post-training test scores and peritonitis was analyzed.
Results showed that risk of peritonitis is not related to the post-training test score. However, based on our experi- ences, we believe that PD patient training should be length- ened and repeated periodically as suggested by the International Survey of Peritoneal Dialysis Training Pro- grams. Training on certain issues such as the signs and symp- toms of peritonitis should be especially enhanced.
Perit Dial Int 2008; 28(S3):S72–S75 www.PDIConnect.com
KEY WORDS: Patient training; peritonitis.
T
raining patients to perform peritoneal dialysis (PD) safely is crucial for the success of the modality.Many studies have showed the importance of PD train- ers and training programs (1, 2). In Taiwan, PD was launched in 1984. Currently, about 95 PD centers op- erate nationwide, serving 4305 PD patients. In the early
TRAINING OF PERITONEAL DIALYSIS PATIENTS—TAIWAN’S EXPERIENCES
Tzen-Wen Chen,1 Szu-Yuan Li,2 Jinn-Yang Chen,2 and Wu-Chang Yang2
Nephrology,
1Department of Medicine, Taipei Medical University Hospital, Taipei Medical University; and Nephrology,
2Department of Medicine, Taipei Veterans General Hospital and School of Medicine,
National Yang-Ming University, Taipei, Taiwan
Correspondence to: Tzen-Wen Chen, Nephrology, Department of Medicine, Taipei Medical University Hospital, No.
252, Wu Hsing Street, Taipei 110 Taiwan.
stages, nephrologists in Taiwan were extremely careful in selecting candidates for PD because of a relative lack of experience with the modality. Today, they follow the guidelines from the Taiwan Society of Nephrology (TSN) to prescribe the dose of PD.
The TSN is in charge of supervising PD programs.
New programs are required to pass TSN evaluations, which include assessments not only of the quality of the facilities, but also of the nephrologists and nurses.
Because nurses play a prime role in patient training, qualified nurses are essential (3–6). To become quali- fied, nurses must take a 4-day training course, which is held by the TSN, and must pass the examination af- terward. In addition, the nurse must take 2 months of clinical training in a TSN-authorized PD training center.
Worldwide, PD patient training programs are not uniform, and so outcomes cannot be used to evalu- ate the training. To determine whether training ob- jectives in Taiwan have been met, we studied post-training tests in a single center. We reviewed the questionnaires of 100 new PD patients in the Taipei Veterans General Hospital (VGH) during the years 2001 – 2007.
PATIENTS AND METHODS
Standardized training is usually provided in the hospital during the week after catheter implantation.
It consists of lectures, printed materials, practice of the procedures of fluid exchange, exit-site care, iden- tification of the signs and symptoms of peritonitis and complications, and troubleshooting. A qualified PD nurse spends 25 – 40 hours to train each new PD patient during hospitalization. Patients first prac- tice exchange skills with a PD doll or a PD apron be- fore being allowed to use the techniques on their own catheters. The nurse-to-patient ratio is 1:1 during the training course.
by on May 20, 2011 www.pdiconnect.comDownloaded from
S73
CHEN et al. PD TRAINING IN TAIWAN
PDI JUNE 2008 – VOL. 28, SUPPL 3 PROCEEDINGS OF THE 3RD ASIAN CHAPTER MEETING OF THE ISPD
Following the training, the takes a post-training test consisting of 10 parts:
• Anatomy and physiology
• Overview of chronic kidney disease (CKD)
• Overview of PD
• The complications of peritonitis and exit-site infections
• Diet control
• Cardiovascular complications
• PD skills and procedures
• Aseptic techniques
• Management of peritonitis
• Routine tasks
We included 100 new PD patients (42 men, 58 women) from 2001 to 2007 in the study. Tables 1 and 2 show the characteristics of the patients and the causes of renal disease leading to dialysis. All patients received either continuous ambulatory PD (n = 71) or automated PD (n = 29) with standard PD fluid. Peritonitis and exit- site infection events that occurred during the study period were retrieved from medical charts. Post-training test scores were used to analyze the outcomes of peri- tonitis and exit-site infection.
RESULTS
Table 3 shows the overall test scores for the patients.
The questions with the lowest accuracy rate in each category were these:
• in anatomy and physiology, the normal urine amount (60%);
• in overview of CKD, the definition of CKD (74%);
• in overview of PD, the success factors in PD (16%);
• in the complications of peritonitis and exit-site in- fections, the catheter cuff function (39%);
• in diet control, potassium-rich food (7%);
• in cardiovascular complications, the definition of systolic and diastolic pressures (57%);
• in PD skills and procedures, the meaning of drain volume (38%);
• in aseptic techniques, the correct method of hand- washing (57%);
• in management of peritonitis, fibrin in dialysate (36%); and
• in routine tasks, the total quantity of monthly dia- lysate exchanges (5%).
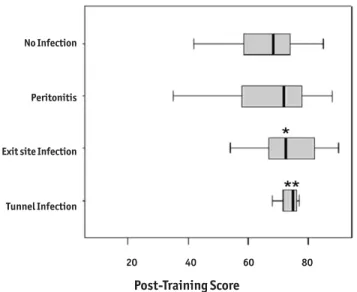
During the study period, 19 episodes of peritoni- tis, 18 episodes of exit-site infection, and 3 episodes of tunnel infection occurred.
The scores of the groups with a college or senior high school education were both significantly higher than the scores of the group with a primary school education only (p = 0.048 and p = 0.038 respectively).
Patients with a lower education level tended to score fewer points in the post-training test (Figure 1). How- ever, the risk for peritonitis was not related to the post- training scores (p = 0.8). Surprisingly, patients with exit-site infection or tunnel infection achieved higher post-training scores (Figure 2; p = 0.036 and p = 0.043 respectively). Apparently, pathophysiologic factors remain influential.
DISCUSSION
Peritonitis is the main cause of hospitalization, tech- nique failure, and even mortality in PD patients. The leading cause of peritonitis is contamination during a PD exchange. Training patients to perform PD safely is thus critical for success of the modality.
Since the 1990s, many published articles have tried to determine the most appropriate approach to PD patient training (3–5). In 1994, the International So- ciety for Peritoneal Dialysis (ISPD) Publications Com- mittee published recommended training requirements TABLE 1
Characteristics of the Study Patients
Sex (men/women) 42/58
Mean age (years) 52.7±16.1
Treatment model (CAPD/APD) 71/ 29
Mean duration on PD (months) 38.4
nKt/V 2.17±0.55
Albumin (g/dL) 3.8±0.5
CAPD = continuous ambulatory peritoneal dialysis; APD = auto- mated peritoneal dialysis; PD = peritoneal dialysis; nKt/V = normalized Kt/V.
TABLE 2
Causes of Renal Failure Leading to Dialysis
Cause Patients (%)
Chronic glomerulonephritis 31
Diabetic nephropathy 24
Hypertensive nephropathy 7
Tubulointerstitial disease 11
Polycystic kidney disease 5
Lupus nephritis 10
Others 10
by on May 20, 2011 www.pdiconnect.comDownloaded from
S74
CHEN et al. PD TRAINING IN TAIWAN
PROCEEDINGS OF THE 3RD ASIAN CHAPTER MEETING OF THE ISPD JUNE 2008 – VOL. 28, SUPPL 3 PDI
for nephrology nurses, including specific objectives for theory and practical skills (3), yet standards for patient training were absent. Finally, in 2006, the ISPD made recommendations for PD training (6). The arti- cle, in the form of a literature review, also set guide- lines. However, specific teaching materials, duration of training, and methods of teaching the patient are still lacking or are only opinions.
In Taiwan, the nurse plays the key role in PD patient training, which usually starts right after PD catheter implantation. As soon as the first training program ends, the patient receives a test. The nurse corrects the
answers and re-teaches the patient accordingly until the patient truly understands the concepts and skills of PD and is able to perform the modality safely.
After an extensive survey of PD centers in the United States, Canada, South America, Netherlands, and Hong Kong, Bernardini et al. concluded that there was no correlation between training time or home visits and the peritonitis rate in adult patients (1). Our study reached similar findings.
In the current study, the risk of peritonitis was not related to post-training test scores, education levels, or occupations. Several explanations for those results
TABLE 3
Post-Training Test Results for 100 New Peritoneal Dialysis (PD) Patients
Questions (n) Answered correctly
(n) (%)
Anatomy and physiology 7 541 77.3
Overview of CKD 7 606 86.8
Overview of PD 9 572 63.6
Complications (peritonitis and exit-site infections) 12 763 63.6
Diet control 10 569 56.9
Cardiovascular complications 10 739 73.9
Skills and procedures of PD 15 1133 75.5
Aseptic technique 8 638 79.8
Management of peritonitis 7 437 62.4
Routine work 9 607 67.4
TOTAL 94 — 70.3
CKD = chronic kidney disease.
Figure 1 — Distribution of scores based on educational attain- ment. Patients with a college or senior high school education achieved significantly higher scores than did the patients with only a primary school education (* p = 0.048 and ** p = 0.038 respectively). More highly educated patients achieved higher post-training test scores.
Figure 2 — Distribution of scores based on occurrence of infec- tions. Scores for patients with peritonitis were not significantly different from scores for patients without infectious complica- tions (p = 0.8). Scores for patients with exit-site or tunnel infection (or both) were significantly higher (* p = 0.036 and
** p = 0.043 respectively).
Post-Training Score
30 40 50 60 70 80 90 20 40 60 80
College
Senior high school
Junior high school
Primary school
No Infection
Peritonitis
Exit site Infection
Tunnel Infection
Post-Training Score
by on May 20, 2011 www.pdiconnect.comDownloaded from
S75
CHEN et al. PD TRAINING IN TAIWAN
PDI JUNE 2008 – VOL. 28, SUPPL 3 PROCEEDINGS OF THE 3RD ASIAN CHAPTER MEETING OF THE ISPD
are possible. First, the post-training test score dem- onstrates learning ability rather than execution abil- ity. Patients with a higher education level can learn concepts quickly, and thus achieve higher scores. How- ever, successful PD relies heavily on aseptic procedures during exchanges.
In the Taipei VGH, nurses retrained patients after the post-training test to make sure that every new PD patient was able to perform the exchange procedure correctly. The training duration ranged from 25 to 45 hours depending on the individual patient. With pro- longed training time, even patients with a minimum educational background can perform PD accurately.
That finding might explain the results of an interna- tional survey of pediatric training (7) that related longer training time with lower peritonitis rates in pediatric patients (p < 0.01).
Another important explanation is that PD training is only a preliminary step in reducing the risk of peri- tonitis. Continuous education and retraining, proper hand-washing techniques, personal hygiene, exit-site care, and use of antibiotic ointment are also crucial for the prevention of contamination. Beside contamina- tion during exchanges, the immunity status of the patient, transmural migration, and obstetric and other factors can also lead to PD peritonitis.
In our study, all possible causes of peritonitis were reviewed. Inappropriate aseptic exchange technique was the cause in 37% of cases (n = 7). Another 37% of cases (n = 7) were related to diarrhea, and in 21% of the cases (n = 4), the cause was unknown.
Patient training can minimize the risk of contamina- tion-induced infections, but aseptic technique does not help to decrease transmural peritonitis. Every PD patient therefore needs to know very well the early symptoms and signs of peritonitis and other complications.
CONCLUSIONS
The learning abilities of patients, as translated into test scores, does not correlate with the risk for perito- nitis in our observation. The post-training test helps to evaluate the learning process and provides immedi- ate feedback to the learner. With repeated and suffi- ciently long training, even patients with a minimum educational background can perform PD techniques precisely. Given that many factors other than exchange contamination can induce peritonitis, training regard- ing certain problems—especially the signs and symp- toms of peritonitis—should be enhanced.
REFERENCES
1. Bernardini J, Price V, Figueiredo A, Riemann A, Leung D.
International survey of peritoneal dialysis training programs. Perit Dial Int 2006; 26:658–63.
2. Borràs M, Sorolla C, Carrera D, Martín M, Villagrassa E, Fernández E. Patients with learning difficulties: outcome on peritoneal dialysis. Adv Perit Dial 2006; 22:116–18.
3. Recommendations of the International Society for Peritoneal Dialysis for training requirements of nephrology trainees and nurses. Perit Dial Int 1994; 14:117–20.
4. Blake PG, Breborowicz A, Han DS, Joffe P, Korbet SM, Warady BA on behalf of the International Society for Peritoneal Dialysis Standards and Education Subcommittee.
Recommended peritoneal dialysis curriculum for nephrology trainees. Perit Dial Int 2000; 20:497–502.
5. Neville A, Jenkins J, Williams JD, Craig KJ. Peritoneal dialysis training: a multisensory approach. Perit Dial Int 2005;
25(Suppl 3):S149–51.
6. Bernardini J, Price V, Figueiredo A. Peritoneal dialysis patient training, 2006. Perit Dial Int 2006; 26:625–32.
7. Holloway M, Mujais S, Kandert M, Warady BA. Pediatric peritoneal dialysis training: characteristics and impact on peritonitis rates. Perit Dial Int 2001; 21:401–4.
by on May 20, 2011 www.pdiconnect.comDownloaded from