An Approach to Cross-Hospital Emergency Medical Service Support
Yen-Chun Lin 1 , Albert Jeng* , and Chun-I Huang
[email protected], [email protected], [email protected]
Department of Computer Science and Information Engineering, National Taiwan University of Science and Technology
*Department of Information Management, Kao Yuen Institute of Technology
Abstract
Objective: It is a great challenge to collect the medical records fast enough for physicians to provide definitive care to save emergency department (ED) patients. This paper describes an approach to fast collection of ED patients’ medical records in Taiwan. ED patients’ survival rate can thus be increased.
Setting: Emergency care in Taiwan.
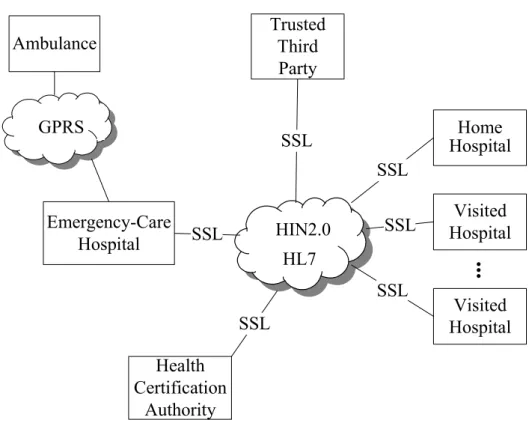
Methods: State-of-the-art information technologies and standards are useful in collecting ED patients’ medical records before they arrive at the hospital. Our approach considers preventing medical records from unauthorized disclosure or modification. The information technologies and infrastructures taken into account are as follows. Radio Frequency Identification systems can provide superior identity authentication of patients. With the implementation of General Packet Radio Service, Global System for Mobile Communications networks can connect to the Internet to transfer data. The Healthcare Institution Cards issued to hospitals by the Healthcare Certification Authority of Taiwan are used for mutual authentication between hospitals. The Health Level Seven protocol with Secure Sockets Layer can be used for secure exchange, management, and integration of clinical data to provide interoperability between healthcare information systems. The Health Information Network 2.0 can be the physical media to transmit information.
Result: A distributed architecture for rapid collection of medical records, especially those of ED patients’, is proposed. The architecture integrates existing healthcare resources in Taiwan. An ambulance can acquire the identification of a patient and transmits it to the hospital. An ED physician can then collect the patient’s medical records early enough, even before the patient arrives at the hospital.
Conclusion: The system helps reduce ED patients’ critical consultation time and is particularly beneficial to unconscious patients.
1. Introduction
The earlier we provide definitive care to critically ill and injured patients, the better progress they may have.
Since emergency department (ED) patients may have to go through the sickness/injury severity classification, medical records inquiry, and vital sign measurements, it may take a longer time than 15 minutes before the patients can be properly taken care of [1]. In general, it is a great challenge to collect the medical records fast enough for physicians to provide definitive care to save ED patients.
This paper proposes a fast medical record collection system, which reconciles with the fact that each hospital maintains its own patients’ medical records. State-of-the-art information technologies and standards are taken into account to collect patients’ medical information before they arrive at the hospital. ED patients’
survival rate can thus be increased.
1