行政院國家科學委員會專題研究計畫 成果報告
引痛點酚注射療法對肌膜疼痛症引痛點敏感度的影響(2/2)
計畫類別: 個別型計畫
計畫編號: NSC93-2314-B-006-009-
執行期間: 93 年 08 月 01 日至 94 年 07 月 31 日 執行單位: 國立成功大學醫學系復健醫學科
計畫主持人: 陳若佟
報告類型: 完整報告
處理方式: 本計畫可公開查詢
中 華 民 國 94 年 10 月 31 日
中文摘要
肌膜疼痛症為最常見的肌肉疼痛疾病,其罹患的人數很多且再發率相當高,往往嚴重 影響患者日常工作及生活品質。其特徵為在肌肉緊張帶上有一特定敏感的引痛點 (Myofascial Trigger Point) ,如果在引痛點上給與機械性刺激,可以誘發局部抽搐反應及 投射遠方肌肉的引傳痛。引痛點內含有多個活化小點且於此可記錄到具特徵化的自發性 電位活動,目前學者認為此自發性電位活動乃是一種不正常的終板雜訊電位(End-plate Noise),而引痛點的病生理機轉在於因肌肉傷害造成不正常運動神經終板,並於此處有 過多的乙醯膽鹼釋放。引痛點注射療法為目前臨床上治療肌膜疼痛症最快速有效的治療 方法,但對嚴重肌膜疼痛症患者效果可能很短暫。酚(Phenol)已使用於臨床幾十年, 之前 多用於治療肌肉痙攣及嚴重疼痛, 未曾用於肌膜疼痛症之治療。本試驗之目的就是要應 用洪氏(Hong)引痛點多小點注射法來研究引痛點酚注射療法對肌膜疼痛症引痛點敏感度 的影響,以進一步改善對嚴重肌膜疼痛症患者之治療。
實驗對象為 7 位嚴重肌膜疼痛症患者,於患者肌膜引痛點內搜尋敏感小點的終板雜訊 電位,當紀錄到終板雜訊電位後即做引痛點酚注射療法,即注射約一滴的酚(5% aqua phenol),並紀錄此終板雜訊電位於注射藥物後隨時間的變化;對照組施於其他的引痛點 並重複以上之步驟,但注射生理食鹽水。實驗分析以終板雜訊電位平均積分值(averaged integrated value, AIV)做為量化引痛點敏感度的參數。
實驗結果顯示:5 位患者合併有輕微至中度感覺異常的現象。所有 7 位嚴重肌膜疼痛 症患者實驗組 normalized AIV 均較對照組小,且結果具統計學意義。由 two-way ANOVA 分析得知,實驗組平均 normalized AIV 為 0.2550.089,而對照組平均 normalized AIV 為 0.9600.112,二者差異具統計學意義。其它臨床評估亦顯示患者的引痛點於酚注射 後,其疼痛分數、壓痛敏感度及壓痛耐受度均有明顯改善,但組織柔順度則無明顯改善。
結論:引痛點酚注射療法可有效的降低引痛點敏感度。
關鍵詞:肌筋膜疼痛症、引痛點、自發性電位活動、終板雜訊電位、酚注射療法 Abstract
Myofascial pain syndrome (MPS) is the most common cause of painful muscular dysfunction in clinics. Myofascial trigger point (MTrP), a hyperirritable spot within a palpable taut band of skeletal muscle, is the primary characteristic of MPS. Referred pain and local twitch response can be elicited by mechanical stimulus to the MTrP. Simons and others have proposed that MTrPs basically represent a neuromuscular disease associated with dysfunction of motor end-plates. Hong has also demonstrated that there are multiple active loci within an MTrP area, in which end-plate noise is shown in electromyography. Clinically, MTrP injection has been often used as an effective and valuable procedure to inactivate an active MTrP, and subsequently relieve the pain and tightness of the muscle involved in myofascial pain syndrome. However, some of the chronic MPS patients may become very severe that little clinical effectiveness can be gained from any form of therapy. Although Phenol has been widely employed to relieve both pain and spasticity, it has not been used in the treatment of MPS. Our hypothesis was that MTrP injection with phenol is useful in diminishing the sensitivity of MTrP, leading to effective pain relief of refractory MPS patients. The aim of this study was to apply electrophysiological signal analysis in quantitatively characterizing the change of end-plate noise for MTrP injection with phenol.
Clinical application of MTrP injection with phenol to severe MPS patients refractory to other form of MTrP therapy was conducted. Seven (4 female and 3 male) chronic MPS patients who had active MTrPs with severe spontaneous pain and muscle tightness in the
skeletal muscles were included in this study. The MTrPs of individual patient were randomly assigned to the experimental and control groups. The MTrPs in the experimental group received MTrP injection with phenol, while the MTrPs in the control group received MTrP injection with normal saline. Electromyography with needle electrodes was used to record end-plate noise from the active loci within the MTrP. After a train of end-plate noise was recorded from the active locus, one drop of 5% aqueous phenol was pushed into the active locus. The active recording needle electrode was kept at the same locus for the continuous recording of end-plate noise after phenol injection for about 3 minutes. Control study was conducted on other MTrP following the same procedure except that normal saline instead of phenol was used for MTrP injection. The average integrated value [AIV] of end-plate noise was statistically analyzed for comparing the treatment effect. Other clinical parameters, such as numerical analog pain scale, pressure pain threshold, pressure pain tolerance, and tissue compliance were also evaluated on the human subjects.
Mild to moderate paresthesia was reported in 5 of the subjects. All subjects demonstrated significantly lower normalized AIV in the treatment side compared to the control [P<0.05].
The results of two-way ANOVA showed that the mean of normalized AIV in treatment group [0.255 ± 0.089] was significantly [P<0.05] lower than that of control [0.960 ± 0.112]. MTrP injection with phenol was effective in diminishing the sensitivity of MTrP. Normalized data of the numerical analog pain scale, pressure pain threshold, and pressure pain tolerance showed statistical significance after phenol injection as compared to the control. There was no significantly difference in the normalized tissue compliance data between two groups.
Keywords: Myofascial Pain Syndrome, Myofascial Trigger Point, Spontaneous Electric Activity, End-plate Noise, Phenol
前言:
Myofascial pain syndrome (MPS) is the most common cause of painful muscular dysfunction in clinics. Myofascial trigger point (MTrP), a hyperirritable spot within a palpable taut band of skeletal muscle, is the primary characteristic of MPS. Referred pain and local twitch response can be elicited by mechanical stimulus to the MTrP. Simons and others have proposed that MTrPs basically represent a neuromuscular disease associated with dysfunction of motor end-plates. Hong has also demonstrated that there are multiple active loci within an MTrP area, in which end-plate noise is shown in electromyography. Clinically, MTrP injection has been often used as an effective and valuable procedure to inactivate an active MTrP, and subsequently relieve the pain and tightness of the muscle involved in myofascial pain syndrome. However, some of the chronic MPS patients may become very severe that little clinical effectiveness can be gained from any form of therapy. Although Phenol has been widely employed to relieve both pain and spasticity, it has not been used in the treatment of MPS.
研究目的:
Our hypothesis was that MTrP injection with phenol is useful in diminishing the sensitivity of MTrP, leading to effective pain relief of refractory MPS patients. The aim of this study was to apply electrophysiological signal analysis in quantitatively characterizing the change of end-plate noise for MTrP injection with phenol.
文獻探討:
Phenol has been widely employed to relieve both pain and spasticity. Phenol is a benzene ring with one hydroxyl group substituted for a hydrogen ion. It was first isolated in 1834 and was introduced to medicine as an antiseptic by Lister in 1867. In its pure state it consists of colorless crystals with a characteristic odor, which melt at 38C. It is soluble in water at room temperature in a ratio of 1:15 (6.7%) while high concentrations have to be warmed. Applied directly to tissue in concentrations of 5% or more in water, it causes protein coagulation and necrosis. It is conjugated by the liver and other tissues to phenyl compounds, oxidized to quinol compounds, or to carbon dioxide and water, and excreted by the kidney as various conjugated derivatives. Phenol is highly soluble in glycerine and released from it slowly, an advantage in injection that allows for limited spread and highly localized tissue fixation. It is more potent in water than in oil, with intermediate strength in glycerine.
Many variables can influence the effect of phenol block, including the concentration and volume of phenol injected, the length of time phenol is in contact with the tissue, localization and selection of block sites, and application techniques. Phenol has been applied to peripheral nerves and muscles at variable concentrations and using multiple techniques (e.g., intraneural injection, perineural injections, or intramuscular injections). Location of the nerves was achieved with sheathed needles and a stimulator. Initial reports suggested that phenol caused selective damage to small nerve fibers and the gamma motor fibers. Later studies, however, demonstrated that phenol at concentrations of 1-7% caused indiscriminate damage to efferent and afferent nerve fibers. The degree of damage correlates directly with concentration and total amount used. At concentrations less than 1%, phenol appears to have a local anesthetic effect, which is fully reversible. Peripheral neurolysis with phenol for pain has been reported with good results. Rose and Kelly in 1969, treating non-malignant shoulder pain, reported good results of suprascapular blocks with 3% phenol, with no mention of complications.
Mehta and Ranger in 1971 presented 103 patients with intractable abdominal pain due to sensory branch entrapment along the rectus sheath. After trying local anesthetic injections, then local anesthetic plus steroid, they had begun using 2-3 ml of 5% aqueous phenol at the trigger point, after pinpointing it with a stimulator and a sheathed needle. Eighty-two of these
patients answered a follow-up letter. Seventy percent were improved. There was no mention of painful paresthesia. In an effort to avoid unpleasant sensory effects, the technique of locating and blocking motor points was developed. It has been reported by Cain et al., Khalili and Benton, and Halpern and Meelhuysen. The technique consists of exploring the skin over a muscle first with a surface stimulating electrode. Then, when a point is found that produces maximal muscle response with minimal stimulation, this point is explored with a Teflon-sheathed needle until the intramuscular point of greatest sensitivity is located; here the phenol is injected. There may be several such motor points per muscle. There were no complications other than transient local soreness reported.
Although Phenol has been widely employed to relieve both pain and spasticity, it has not been used in the treatment of MPS. The advantages of MTrP injection with phenol are that it is safe, low cost, long duration, gives immediate results and may be repeated as necessary.
研究方法:
Clinical application of MTrP injection with phenol to severe MPS patients refractory to other form of MTrP therapy were conducted. Seven (4 female and 3 male) chronic MPS patients who have active MTrPs with severe spontaneous pain and muscle tightness in the skeletal muscles were included in this study. The MTrPs of individual patient were randomly assigned to the experimental and control groups. The MTrPs in the experimental group received MTrP injection with phenol, while the MTrPs in the control group received MTrP injection with normal saline.
Muscles studied included the upper trapezius, levator scapula, rhomboid, and infraspinatus muscles. All recordings were performed with the subjects conformably sitting on a chair or lying supine in bed. All subjects were awake and relaxed. For end-plate noise recording in an MTrP region, an insulated (Teflon-coated) needle with an exposed tip was used. The needle was attached to a syringe for the following MTrP injection and was connected to channel 1 of a 4-channel Viking EMG System (Nicolet Biomedical Inc., Madison, WI ). The recording needle electrode was inserted into an MTrP area for searching the end-plate noise. The control needle electrode was inserted into the nearby normal muscle fibers and connected to channel 2. The reference electrode common to both channels 1 and 2 and the ground electrode was attached to the adjacent skin. The sensitivity of recording was set at 0.02mV per division and the sweeping speed of screen was set at 10msec per division.
The active recording needle electrode was inserted gently and slowly through the least possible distance (usually 1-2 mm) into the MTrP region to search for the end-plate noise.
When a train of end-plate noise was recorded from an active locus of the MTrP, one drop of phenol was pushed into the active locus. The active recording needle electrode was kept at the same locus for the continuous recording of end-plate noise after phenol injection for about 3 minutes. After 8 advancements of the needle in one track, the needle was pulled out to the original insertion depth and reinserted in a slightly different direction. This procedure was repeated again to explore a total of 24 thrusts. Control study was conducted on other MTrP following the same procedure except that normal saline instead of phenol was used for MTrP injection.
The effectiveness of MTrP injection with phenol was validated by using signal analysis of end-plate noise recorded from human MTrP. The raw data of 1-second end-plate noise was recorded by electromyography, and then rectified and integrated to calculate the average integrated value (AIV) of end-plate noise for time domain analysis, and statistical analysis was applied to determine any significance of the phenol injection effects. Other clinical parameters, such as numerical analog pain scale, pressure pain threshold, pressure pain tolerance, and tissue compliance were also evaluated on the human subjects.
結果與討論:
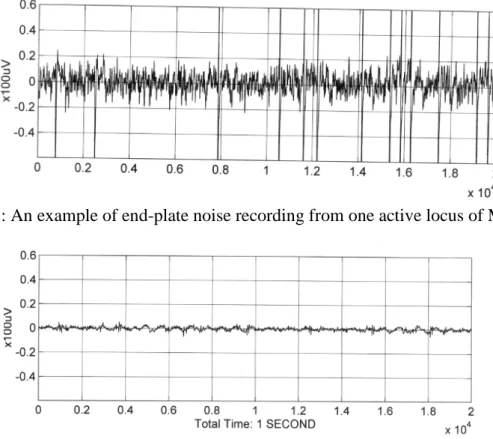
In this study, electrophysiological characteristics of end-plate noise recorded from multiple loci of MTrPs of skeletal muscle of human were investigated by using digital signal processing. The end-plate noise consisted of continuous, noise-like action potentials (5 to 50V), accompanied by intermittent large-amplitude spikes (100 to 600V) (Fig. 1). If the recording needle was advanced or withdrawn as little as 1mm away from the tiny active loci, it could not record the electrical activity. Usually there were several active loci with evidencing end-plate recording in an MTrP region. The control needle electrode in the nearby normal muscle fibers of a non-MTrP region showed no end-plate noise (Fig. 2). The magnitude of resting activity signals was less than 1V.
Mild to moderate paresthesia was reported in 5 of the subjects. All 7 subjects demonstrated significantly lower normalized AIV in the treatment side compared to the control [P<0.05].
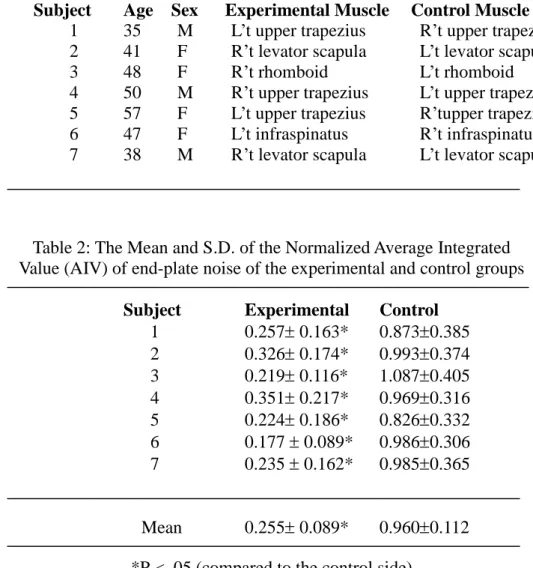
The results of two-way ANOVA showed that the mean of normalized AIV in treatment group [0.255 ± 0.089] was significantly [P<0.05] lower than that of control [0.960 ± 0.112] (Table 3). Normalized data of the numerical analog pain scale, pressure pain threshold, and pressure pain tolerance showed statistical significance after phenol injection as compared to the control.
There was no significantly difference in the normalized tissue compliance data between two groups.
Fig 1: An example of end-plate noise recording from one active locus of MTrP.
Fig 2: EMG recording from the control site of normal muscle at rest.
Table 1: Basic data of the subjects
Subject Age Sex Experimental Muscle Control Muscle 1 35 M L’t upper trapezius R’t upper trapezius 2 41 F R’t levator scapula L’t levator scapula
3 48 F R’t rhomboid L’t rhomboid
4 50 M R’t upper trapezius L’t upper trapezius 5 57 F L’t upper trapezius R’tupper trapezius 6 47 F L’t infraspinatus R’t infraspinatus 7 38 M R’t levator scapula L’t levator scapula
Table 2: The Mean and S.D. of the Normalized Average Integrated Value (AIV) of end-plate noise of the experimental and control groups
Subject Experimental Control 1 0.2570.163* 0.8730.385 2 0.3260.174* 0.9930.374 3 0.2190.116* 1.0870.405 4 0.3510.217* 0.9690.316 5 0.2240.186* 0.8260.332 6 0.1770.089* 0.9860.306 7 0.2350.162* 0.9850.365
Mean 0.2550.089* 0.9600.112
*P < .05 (compared to the control side)
Table 3: The Mean and S.D. of the numerical analog pain scale, pressure pain threshold, pressure pain tolerance and tissue compliance
of the experimental and control groups (Normalized data) Experimental Control Numerical Analog Pain Scale 0.3750.163* 0.8750.213 Pressure Pain Threshold 2.1860.759* 1.3570.582 Pressure Pain Tolerance 1.6780.523* 0.9950.412 Tissue Compliance 1.0640.245 1.1120.267
*P < .05 (compared to the control side)
It was concluded that MTrP injection with phenol is effective in diminishing the sensitivity of MTrP. The outcome of this research would provide fundamental information to improve understanding of MTrP; more important, it is expected to beneficial to effective treatment options for the severe MPS patients.
References
1. Burkel WE, McPhee M: Effect of phenol injection into peripheral nerve of rat: electron microscope studies. Arch Phys Med Rehabil. 51:391-397;1970.
2. Halpern D: Histologic studies in animals after intramuscular neurolysis with phenol. Arch Phys Med Rehabil. 58:438-443;1977.
3. Nathan PW, Scott GG: Intrathecal phenol for intractable pain: safty and dangers of the method. Lancer. 1:1096-1100;1965.
4. Rose DL, Kelly CR: Shoulder pain. Suprascapular nerve block in shoulder pain. J Kans Med Soc. 70:135-136;1969.
5. Wood KM: The use of phenol as a neurolytic agent: a review. Pain. 5:205-229;1978.
計劃成果自評
本試驗之目的就是要應用洪氏(Hong)引痛點多小點注射法來研究酚注射療法對肌膜疼 痛症引痛點敏感度的影響,以進一步改善對嚴重肌膜疼痛症患者之治療。由於酚注射療 法仍有可能會造成感覺異常的副作用,故實驗對象局限為嚴重肌膜疼痛症患者,且對其 他治療方法療效不佳者。於實驗步驟中,我們使用洪氏(Hong)引痛點注射法來減少所注 射的酚總量,以期能盡量降低感覺異常的副作用。然而 7 位患者中仍有 5 位患者合併有 輕微至中度感覺異常的現象,因此我們認為對肌膜疼痛症患者之酚注射治療應相當小心 且保守,最好保留給非常嚴重且對其他治療方法療效不佳的患者。而這也是為何實驗對 象人數較原先計畫少的原因。
由實驗結果顯示:所有 7 位嚴重肌膜疼痛症患者實驗組 normalized AIV 均較對照組 小,且結果具統計學意義。其它臨床評估亦顯示患者的引痛點於酚注射後,其疼痛分數、
壓痛敏感度及壓痛耐受度均有明顯改善,但組織柔順度則無明顯改善。結論:引痛點酚 注射療法可有效的降低引痛點敏感度,但感覺異常仍是最需克服的的副作用。