Mortality among psychiatric patients in Taiwan
—Results from a universal National
Health Insurance programme
Yi-Hua Chen
a, Hsin-Chien Lee
b,c, Herng-Ching Lin
d,⁎
a
School of Public Health, Taipei Medical University, Taipei, Taiwan
bDepartment of Psychiatry, Taipei Medical University Hospital, Taipei, Taiwan c
School of Medicine, Department of Psychiatry, Taipei Medical University, Taipei, Taiwan
d
School of Health Care Administration, Taipei Medical University, Taipei, Taiwan
a b s t r a c t
a r t i c l e i n f o
Article history:
Received 21 February 2008 Received in revised form 24 July 2008 Accepted 31 July 2008
Keywords: Mortality
National Health Insurance Psychiatric inpatient
This study investigated 6-year follow-up mortality rates and cause of death for persons younger than 45 years old with a history of hospitalisation for major psychiatric disorders after the introduction of the National Health Insurance (NHI). Linkage data combining death certificates with Taiwan NHI research claims data were used. The study cohort was comprised all patients under the age of 45 years, who had been hospitalised for major psychiatric disorders in 1998. Patients agedb45 years undergoing an appendectomy were selected as a control group. Cox proportional hazard regressions were performed to compute the adjusted 6-year hazard ratios. For patients with schizophrenia, major depression, or bipolar disorder, the adjusted risks of dying during the follow-up period were significantly 4.614, 3.707 and 3.866, respectively, times higher than that for appendectomy patients. The adjusted hazard ratios of non-natural dying during the follow-up period were significantly 16.316, 14.626 and 8.481 times for female patients with schizophrenia, major depression, and bipolar disorder, respectively, as high as for female appendectomy patients. The continuing excess mortality among psychiatric patients, from both natural and unnatural causes, still remains even after implementation of a NHI.
© 2008 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Over the years, studies have consistently reported higher mortality
rates among psychiatric patients of both genders, in various countries and
ethnic groups, especially among younger patients and speci
fically during
the
first year after admission (
Black et al., 1985; Casadebaig and Quemada,
1991; Chen et al., 1996; Räsänen et al., 2003
). Despite some studies
reporting a distinct decline in excess mortality (
Sims, 1987; Casadebaig
and Quemada, 1991
), others have observed a persistent or even widening
disparity in health outcomes between the general population and
psychiatric patients (
Lawrence et al., 2003; Räsänen et al., 2003
).
Compared with the general population, excess mortality among
psychiatric patients is attributed to both natural and unnatural causes
of death (e.g., suicide and accidents). Higher risk of suicide was
reported for schizophrenic, manic, and depressive patients, especially
among male patients with affective disorders during the
first decade
after a psychiatric hospitalisation (
Tsuang, 1978
). Although similar
patterns of death from natural causes (e.g., cardiovascular diseases
and lung diseases) were reported comparing psychiatric groups and
the general population, an elevated risk of mortality was documented
among mentally ill people (
Tsuang and Woolson, 1978; Corten et al.,
1988; Mortensen and Juel, 1990, 1993
).
Consistent with this picture, higher mortality, both natural and
unnatural deaths, among psychiatric inpatients in Taiwan has likewise
been reported (
Chen et al., 1996
). Using a nationwide cohort of
Taiwanese psychiatric inpatients admitted between 1987 and 1988,
inclusive,
Chen et al. (1996)
reported a higher 6-year mortality rate for
psychiatric inpatients (i.e., standardized mortality ratios of 3.1 for men
and 4.8 for women) compared with the general population.
Mortality studies have contributed considerably as indicators of
health-care quality for inpatient and outpatient services (
Tsuang and
Simpson,1985; Hewer et al.,1995
). It is often asked whether equal access
to health services including specialised medical procedures has been
achieved for a population in general (
Corten et al.,1991
). Many countries
with advanced economies provide universal health insurance coverage
to achieve more equal health-care access and to improve the health of
the general population. In Taiwan, before 1995, about 57% of the people
were insured through three separate programmes, the Labor, the
Government Employee, and the Farmers' Insurance Programs. In March
Psychiatry Research 178 (2010) 160–165⁎ Corresponding author. School of Health Care Administration, College of Medicine, Taipei Medical University, 250 Wu-Hsing St., Taipei 110, Taiwan. Tel.: +886 2 2736 1661x3613; fax: +886 2 2738 4831.
E-mail address:[email protected](H.-C. Lin).
0165-1781/$– see front matter © 2008 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.psychres.2008.07.023
Contents lists available at
ScienceDirect
Psychiatry Research
1995, Taiwan initiated its National Health Insurance (NHI) programme
to
finance health care for all citizens. Taiwan's NHI has a unique
combination of characteristics: universal coverage, a single-payer
payment system with the government as the sole insurer, very low
out-of-pocket copayments, comprehensive bene
fits, unrestricted access
to any medical institution of the patient's choice and a wide variety of
providers including primary care physicians. The NHI also covers the
cost of medication.
Although there are limited studies available, positive effects of
universal health insurance on health and health-care use have been
observed (
Decker and Remler, 2004
). Some researchers have
indicated that changes in a health-care system might contribute to a
decline in the tendency to excess mortality among psychiatric patients
(
Tsuang and Simpson, 1985; Sims, 1987
). Following the
implementa-tion of the NHI in 1995, a signi
ficant change in health-seeking
behaviours and health resources use could be anticipated. It is thus of
interest to re-examine the mortality rates among psychiatric patients
in Taiwan following implementation of the NHI.
In this study, we investigated mortality among psychiatric patients
in a universal National Health Insurance programme in Taiwan. The
6-year follow-up mortality rates and causes of death for persons
younger than 45 years with a history of hospitalisation for a major
psychiatric disorder following the introduction of the NHI were
investigated, using data that combines death certi
ficates with Taiwan
NHI research claims data.
2. Methods 2.1. Database
The hospitalisation data used in this study were obtained from the National Health Insurance Research Dataset (NHIRD) for the years 1996–98 inclusive, as published by the National Health Research Institute in Taiwan. The dataset includes all claims data from Taiwan's National Health Insurance (NHI) programme implemented as a means of financing health care for all Taiwanese citizens. As of April 2005, the NHI program had over 21 million enrollees, representing around 96% of the island's population (Chen et al., 2007). The NHI's reimbursement system ties a hospital's reimbursement level to its patient severity profile. To deter diagnosis upcoding, the NHI Bureau implements routine sample cross-checks of each hospital's claims with its medical charts, followed by punitive measures for coding infractions. Fines for fraudulent diagnosis reporting are generally 100 times the value of the false claim. As a result, hospitals' interests are best served by accurate coding of diagnoses and services provided. It is generally believed that the NHI's checks and balances foster accurate coding, although there have not been sensitivity and specificity studies to document its coding accuracy. Since this dataset is for the purpose of claims, no missing data is likely. As one of the largest databanks of medical/health information in the world, the NHIRD offers a unique opportunity to compare mortalities among young patients admitted to psychiatric departments.
In this study, the date of death was obtained from the 1998–2004 ‘cause of death’ datafile published by the Department of Health (DOH) in Taiwan. The ‘cause of death’ file provides details on marital status, the dates of births and deaths, place of legal residence, underlying cause of death (ICD-9-CM code), and employment status. Given that there is mandatory registration of all deaths in Taiwan, this data should be particularly accurate and comprehensive. The NHIRD was linked to the‘cause of death’ datafile with the assistance of the DOH in Taiwan.
2.2. Study sample
The study cohort consisted of all patients under the age of 45 years who had been hospitalised for schizophrenia (any ICD-9-CM 295 code other than 295.7 for schizoaffective disorder), major depression (296.2X and 296.3X), or bipolar disorder (296.0X, 296.4X, 296.5X, 296.6X, 296.7X, 296.80 or 296.89) between January and December 1998, because patients younger than 45 years are at higher risk of excess mortality (Casadebaig and Quemada, 1991; Meloni et al., 2006). To avoid the potential confounding factors of institutionalisation and chronicity (Cuijpers and Smit, 2002), those who had been hospitalized for schizophrenia, bipolar disorder, or major depression or were under any psychiatric treatment for schizophrenia during the previous 2-year period (1996–97) were excluded from the study cohort. In addition, patients agedb45 years undergoing an appendectomy in 1998 with an ICD-OP code of 47.0 as the primary operative procedure were selected as a control group, since data on the general population are not available from the NHIRD. The reason for selecting appendectomy patients as the control group was that patients undergoing appendec-tomies are relatively indistinguishable from the general population. No statistically significant differences were found between the control cohort and the general population in Taiwan with regard to either gender (P N 0.05) or age (P N 0.05).
Appendectomy patients were, however, excluded if they had ever been diagnosed as having any major psychiatric disorder at the time of their recruitment.
In total, 26 374 eligible patients were ultimately selected for this study, including 5515 suffering from schizophrenia, 555 from major depression, and 1581 from bipolar disorder, as well as 18 754 who had undergone an appendectomy. Follow-up of each individual patient was undertaken from recruitment until the end of 2004, with all patients identified from administrative data to determine whether any had died. Both natural and unnatural causes of deaths were examined, with unnatural causes including suicides, accidents, and homicides, while all other deaths were defined as due to natural causes (Honkonen et al., 2008).
The regression modeling also adjusted for sociodemographic variables including age (b18, 18–24, 25–34, and ≥35 years), gender, medical co-morbidities, level of urbanisation and the geographic location of the community in which the patient resided (northern, central, eastern and southern Taiwan). Details on co-morbid medical disorders, including hypertension, diabetes, renal disease, and chronic obstructive pulmonary disease (COPD), were also extracted from the claims data at the time of the index discharge, because these conditions may exacerbate the risk of mortality.
The urbanisation levels in Taiwan consist of seven strata, with level 1 referring to the ‘most urbanised’ communities and level 7 referring to the ‘least urbanised’ communities, according to standards published by the Taiwanese National Health Research Institute. However, given that there were only very small numbers of schizophrenia cases in levels 5, 6 and 7, these three levels were combined into a single group, which was thereafter referred to as level 5.
2.3. Statistical analysis
The SAS statistical package (SAS System for Windows, version 8.2) was used to perform the statistical analyses in this study. Pearsonχ2
tests were used to examine differences in sociodemographic characteristics, co-morbid medical disorders, and the risk of stroke development among the four cohorts (schizophrenia, major depression, bipolar disorder and appendectomy). The 6-year survival rate was then estimated using the Kaplan–Meier method, with the log-rank test used to examine differences among cohorts. Cox proportional hazard regressions were also carried out as a means of computing the adjusted 6-year hazard ratios, following adjustment for the variables above. Finally, hazard ratios (HRs) are presented along with the 95% confidence intervals (95% CIs), adopting a significance level of 0.05 (Pb0.05) for this study.
3. Results
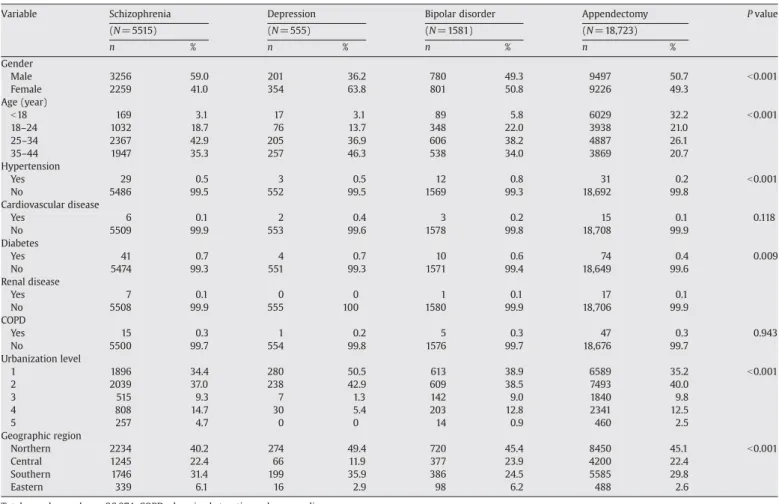
Of the total sample of 26 374 patients under the age of 45 years,
52.1% were male, 30.6% were aged between 25 and 34 years and 0.3%
had conditions complicated by hypertension, 0.1% by cardiovascular
diseases, 0.5% by diabetes, 0.1% by renal diseases and 0.3% by COPD.
Details of the distribution of demographic characteristics and
co-morbid medical disorders for the sampled patients are provided in
Table 1
by disorder type.
Compared to the appendectomy patients, patients with major
depression were more likely to be female, aged between 35 and
44 years, with conditions complicated by diabetes, residing in
more-urbanized communities and in northern Taiwan at the time of the
index discharge (all P b0.001).
Table 1
also shows that there were
signi
ficant differences in the distributions of gender (Pb0.001), age
(P b 0.001), hypertension (P b 0.001), diabetes (P = 0.009),
urbaniza-tion level (P b 0.001), and geographic region (P b0.001).
The log-rank test indicated that patients with schizophrenia, major
depression, and bipolar disorder had signi
ficantly lower 6-year
survival rates compared with appendectomy patients (P b 0.001).
The 6-year survival rate, crude HRs, and adjusted HRs of mortality for
the four cohorts are presented in
Table 2
, which reveals that 6.8%, 5.8%,
5.6% and 1.2% of patients with schizophrenia, major depression,
bipolar disorder, and an appendectomy, respectively, died during the
6-year follow-up period. For patients with schizophrenia, major
depression or bipolar disorder, the risks of dying during the
follow-up period were 6.113 (95% CI = 5.169
–7.230, Pb0.001), 5.191 (95%
CI = 3.580
–7.526, P b0.001), and 4.952 (95% CI = 3.864–6.347,
P b 0.001) times that for appendectomy patients, respectively. After
adjusting for patient's age, gender, co-morbidities, urbanization level,
and geographic region, the relationships still remained; for patients
with schizophrenia, major depression, or bipolar disorder, the risks of
dying during the follow-up period were 4.614 (95% CI = 3.870
–5.500,
P b 0.001), 3.707 (95% CI = 2.544–5.401, P b 0.001), and 3.866 (95%
CI = 3.003
–4.978, Pb0.001) times that for appendectomy patients,
respectively. For female patients with schizophrenia, major
depres-sion, or bipolar disorder, the adjusted HRs of dying were all higher
than those for male patients.
Table 2
also shows the HRs by natural and non-natural deaths.
Surprisingly, the adjusted HRs of dying of non-natural causes during
the 6-year follow-up period were 16 316 (95% CI = 9.877
–26.952,
P b 0.001), 14 626 (95% CI = 6.909–30.962, P b 0.001) and 8 481 (95%
CI = 4.357
–16.513, Pb0.001) times for female patients with
schizo-phrenia, major depression and bipolar disorder, respectively, as high
as for female appendectomy patients.
Table 3
describes proportionate mortality by disorder type. Not
surprisingly, over 25% (out of total deaths) of patients with
schizophrenia, major depression, or bipolar disorder died of suicide.
In comparison, only 7.9% (out of total deaths) of patients undergoing
an appendectomy committed suicide. Patients with major depression
or bipolar disorder did not have a signi
ficantly higher rate of death due
to circulatory or respiratory diseases than those undergoing an
appendectomy.
4. Discussion
This is the
first report on mortality among psychiatric patients,
who were fully insured, in a universal NHI programme in Taiwan. An
important
finding is that despite the implementation of the NHI in
1995, providing universal health-care resources to all citizens,
mortality remained high and 6-year survival rates were signi
ficantly
lower for psychiatric patients, with females constituting a higher risk
group. Compared with appendectomy patients, the adjusted hazard
ratios were signi
ficantly elevated among schizophrenic, depressive
and manic patients during a 6-year follow-up period, with a higher
ratio of deaths by unnatural causes.
Excess mortality among psychiatric patients has been previously
reported, with overall standardized mortality ratios of psychiatric to
general populations in different regions and countries, ranging from
approximately 1.5
–3.1 for males and 1.9–4.8 for females (
Brook, 1985;
Wood et al., 1985
). Consistent with those reports, increased mortality,
from both natural and non-natural causes, was still apparent among
major psychiatric patients in the 6-year follow-up period. The
prevalence of certain physical illnesses is also higher among
psychiatric patients. For example,
Johannessen et al. (2006)
reported
an elevated level of hypertension in bipolar patients, and our study
also observed a higher tendency to hypertension and diabetes among
patients with schizophrenia and affective disorders. As regional
differences have been observed in incidence of schizophrenia (
Schelin
et al., 2000
), we found that the distribution of psychiatric inpatients
was associated with urbanisation level and geographic region, with
depressive people living mainly in the most urbanised communities.
Comparing our study results with those reported before the NHI era
in Taiwan, no declining mortality trend was identi
fied. Before the
introduction of the NHI,
Chen et al. (1996)
recruited a cohort of
psychiatric inpatients from 1987 to 1988 and followed them up for
6 years to the end of 1993. Despite applying various sampling methods,
our
finding of excess mortality among psychiatric inpatients after the
implementation of the NHI appears consistent with that from the
preceding period.
Researchers have proposed that universal health insurance might
increase health care use among both young and elderly populations
(
Card et al., 2004; Decker and Remler, 2004
). Findings from the NHI in
Table 1Demographic characteristics and comorbid medical disorders of schizophrenia, major depression, bipolar disorder, and appendectomy patients in Taiwan in 1998.
Variable Schizophrenia Depression Bipolar disorder Appendectomy P value
(N = 5515) (N = 555) (N = 1581) (N = 18,723) n % n % n % n % Gender Male 3256 59.0 201 36.2 780 49.3 9497 50.7 b0.001 Female 2259 41.0 354 63.8 801 50.8 9226 49.3 Age (year) b18 169 3.1 17 3.1 89 5.8 6029 32.2 b0.001 18–24 1032 18.7 76 13.7 348 22.0 3938 21.0 25–34 2367 42.9 205 36.9 606 38.2 4887 26.1 35–44 1947 35.3 257 46.3 538 34.0 3869 20.7 Hypertension Yes 29 0.5 3 0.5 12 0.8 31 0.2 b0.001 No 5486 99.5 552 99.5 1569 99.3 18,692 99.8 Cardiovascular disease Yes 6 0.1 2 0.4 3 0.2 15 0.1 0.118 No 5509 99.9 553 99.6 1578 99.8 18,708 99.9 Diabetes Yes 41 0.7 4 0.7 10 0.6 74 0.4 0.009 No 5474 99.3 551 99.3 1571 99.4 18,649 99.6 Renal disease Yes 7 0.1 0 0 1 0.1 17 0.1 No 5508 99.9 555 100 1580 99.9 18,706 99.9 COPD Yes 15 0.3 1 0.2 5 0.3 47 0.3 0.943 No 5500 99.7 554 99.8 1576 99.7 18,676 99.7 Urbanization level 1 1896 34.4 280 50.5 613 38.9 6589 35.2 b0.001 2 2039 37.0 238 42.9 609 38.5 7493 40.0 3 515 9.3 7 1.3 142 9.0 1840 9.8 4 808 14.7 30 5.4 203 12.8 2341 12.5 5 257 4.7 0 0 14 0.9 460 2.5 Geographic region Northern 2234 40.2 274 49.4 720 45.4 8450 45.1 b0.001 Central 1245 22.4 66 11.9 377 23.9 4200 22.4 Southern 1746 31.4 199 35.9 386 24.5 5585 29.8 Eastern 339 6.1 16 2.9 98 6.2 488 2.6
Taiwan also indicated that discrepancies in access to health care were
indeed signi
ficantly reduced after a National Health Insurance
programme with comprehensive coverage was initiated (
Chen et al.,
2007
). Although we anticipated that higher health-care use would be
associated with better health outcomes, our study was unable to
find
evidence of reduced mortality among psychiatric patients. Some prior
studies have obtained similar results,
finding that although health
insurance coverage might improve self-reported health status (
Card
et al., 2004
), mortality remained intact (
Card et al., 2004; Chen et al.,
2007
).
Several plausible reasons might explain this
finding. First, 6-year
mortality might not be a suf
ficiently sensitive index for assessing the
effects of a health-care system on health outcomes. The NHI program
has only recently been implemented for that long, and mortality rates
are established based upon lifetime investment in health.
Second, although the NHI in Taiwan was reported to promote
greater healthcare use of both inpatient and outpatient services
signi
ficantly among low- and middle-income groups, more than
among the higher-income class, whether similar patterns can be
observed for discrepancies between psychiatric and general
popula-tions remains a question. As reported by
Kisely et al. (2007)
, mentally
ill persons with circulatory disease (including ischaemic heart disease
and stroke), especially those who had been psychiatric inpatients,
were signi
ficantly less likely to undergo specialised or
revascularisa-tion procedures. Psychiatric illness was associated with reduced
access to some medically necessary procedures, even in a universal
health-care system aimed at producing equality in service delivery.
Furthermore, psychiatric patients' motivation towards recovery and
compliance with treatment might be involved in the quality of
healthcare they receive.
Third, access to or use of health-care services might not be the
main determinant of health. Other factors, including environment,
lifestyle, or health behaviors are also substantial in in
fluencing a
person's health status (
Marmot and Wilkinson, 1999
). These factors
cannot be directly modi
fied by the introduction of the NHI.
Aside from implementation of the NHI, various factors might help
explain the reasons why psychiatric patients possess higher mortality
risk from both natural and unnatural causes of deaths. Psychiatric
patients may receive poorer quality health care (
Hewer et al., 1995
),
including insuf
ficient diagnosis or treatment of their physical illnesses
(
Corten et al., 1991
). Patients might be limited in their ability to
recognize and communicate physical disturbances to others. Some
demographic, urbanisation, or hazardous health behaviours might
contribute to these differences. For example, higher cardiovascular
morbidity and mortality among depressive patients might possibly be
due their looser control of hypertension (
Davidson et al., 2000
).
Lifestyle, such as alcohol or tobacco use, less physical activity, and
unhealthy eating habits may play a part in the proportionately higher
numbers of deaths (
Brown et al., 2000; Cuijpers and Smit, 2002
).
Factors associated with patients' speci
fic psychiatric symptoms or
side-effects of psychotropic drugs might also be involved in the excess
mortality among persons with mental illness (
Appleby et al., 2000;
Zarate and Patel, 2001
).
Further, higher suicides rates and incidence of accidental deaths
due to hazardous activities were considered to be responsible for
increased numbers of death by unnatural causes. Approximately, 28%
of the excess mortality might be attributed to suicide and 12% to
accidents among schizophrenic patients (
Brown, 1997
). Proportionate
mortality from suicide in our sample was high. Based upon reports
from Department of Health, Executive Yuan, Taiwan, suicide rates rose
from 9.97 (per 100 000) in 1998 to 15.31 (per 100 000) in 2004 among
the general population in Taiwan, with an even higher rise among
psychiatric patients. Further, previous studies have shown that
underreporting of suicide is commonplace (
Dijkhuis et al., 1994;
Wang and Chou, 1997
). Possible reasons for the growing trend might
include increased economic burdens, psychological distress,
unem-ployment rates, psychiatric problems (e.g., alcohol use, major
depression) and other psychosocial situations (e.g., high divorce
rate) (
Yip, 1996; Wang and Chou, 1997
).
Several limitations of this study merit attention. First, typical
concerns associated with mortality analysis include the quality,
extensiveness, and accuracy of death certi
ficates and death registries
Table 2Six-year survival rates and hazard ratios by disorder type.
Variable Six-year
survival rate
Crude hazard ratio/95% confidence interval (CI)
Adjusted hazard ratioa/95% CI All deaths Total Disorder type Schizophrenia 93.2 6.113 (5.169–7.230)*** 4.614 (3.870–5.500)*** Major depression 94.2 5.191 (3.580–7.526)*** 3.707 (2.544–5.401)*** Bipolar disorder 94.5 4.952 (3.864–6.347)*** 3.866 (3.003–4.978)*** Appendectomy 98.9 1.000 1.000 Male Disorder type Schizophrenia 93.2 4.807 (3.890–5.940)*** 3.477 (2.791–4.329)*** Major depression 92.0 5.664 (3.376–9.501)*** 3.786 (2.245–6.385)*** Bipolar disorder 93.1 4.844 (3.538–6.633)*** 3.733 (2.713–5.135)*** Appendectomy 98.5 1.000 1.000 Female Disorder type Schizophrenia 93.3 8.504 (6.451–11.210)*** 6.925 (5.158–9.299)*** Major depression 95.5 5.687 (3.315–9.757)*** 4.619 (2.659–8.023)*** Bipolar disorder 95.8 5.275 (3.517–7.910)*** 4.406 (2.905–6.681)*** Appendectomy 99.2 1.000 1.000 Natural deaths Total Disorder type Schizophrenia 96.2 4.977 (4.018–6.166)*** 3.457 (2.780–4.342)*** Major depression 97.7 2.975 (1.651–5.361)*** 1.897 (1.048–3.434)* Bipolar disorder 97.1 3.843 (2.749–5.373)*** 2.844 (2.025–3.996)*** Appendectomy 99.2 1.000 1.000 Male Disorder type Schizophrenia 96.6 4.105 (3.112–5.416)*** 2.802 (2.109–3.722)*** Major depression 96.8 3.496 (1.529–7.997)*** 2.145 (0.933–4.932) Bipolar disorder 97.2 3.647 (2.338–5.690)*** 2.710 (1.729–4.247)*** Appendectomy 99.1 1.000 1.000 Female Disorder type Schizophrenia 96.9 6.353 (4.530–8.909)*** 4.584 (3.194–6.577)*** Major depression 98.5 2.901 (1.250–6.732)* 1.980 (0.843–4.652) Bipolar disorder 97.7 4.200 (2.520–6.997)*** 3.220 (1.906–5.439)*** Appendectomy 99.4 1.000 1.000 Non-natural deaths Total Disorder type Schizophrenia 96.3 9.444 (7.244–12.312)*** 7.945 (6.007–10.509)*** Major depression 96.1 9.827 (6.057–15.943)*** 8.276 (5.050–13.563)*** Bipolar disorder 96.8 7.934 (5.535–11.372)*** 6.737 (4.658–9.743)*** Appendectomy 99.6 1.000 1.000 Male Disorder type Schizophrenia 96.3 6.558 (4.750–9.053)*** 5.129 (3.653–7.201)*** Major depression 94.8 9.322 (4.747–18.304)*** 7.050 (3.554–13.988)*** Bipolar disorder 95.7 7.682 (4.982–11.846)*** 6.263 (4.019–9.760)*** Appendectomy 99.4 1.000 1.000 Female Disorder type Schizophrenia 96.2 16.974 (10.505–27.337)*** 16.316 (9.877–26.952)*** Major depression 96.9 14.029 (6.764–29.096)*** 14.626 (6.909–30.962)*** Bipolar disorder 98.0 8.941 (4.666–17.134)*** 8.481 (4.357–16.513)*** Appendectomy 99.8 1.000 1.000 *P b 0.05; ***P b 0.001. a
Hazard ratios were adjusted for patient's age, gender, medical comorbidity (including hypertension, diabetes, renal disease, and chronic obstructive pulmonary disease), urbanization, and geographical location.
(
Martin, 1985; Flanders, 1992
). Because of the mandatory registration
of all deaths in Taiwan, data from the death registry should be
particularly accurate and comprehensive and are thus the most
appropriate data available for mortality analysis. Meanwhile, although
ICD-9-CM codes were used consistently throughout our study period,
the possibility of changes in coding practices on death certi
ficates
should be considered when interpreting trends in natural and
non-natural deaths. In spite of the
fluctuation of non-natural deaths by
various methods, there has been a steady rise in natural deaths which
may re
flect no obvious attitudinal changes in coding practices on
death certi
ficates over the study period. However, because of the fact
that claims and death certi
ficates were used to define the diagnosis in
this study, the potential bias related to the reliability of diagnoses
existed. Second, the reliability and validity of the NHI claims data and
over- and under-diagnoses should be considered. To deter upcoding,
the NHI Bureau routinely performs sample cross-checks of each
hospital's claims with its medical charts, followed by punitive
measures for coding infractions. It generally accepted that the NHI's
checks and balances promote appropriate coding. However, the
reliability of diagnoses might vary among different psychiatric
disorders, with diagnostic accuracy being higher for schizophrenia
than for major depression (
Chien et al., 2007
). Lower diagnostic
accuracy might attenuate the mortality gap slightly between patients
with major depression and the general population.
Third, social stigmas might lead some patients to deny symptoms.
Because of possible under-representation of psychiatric inpatients in
this study, excess mortality among psychiatric patients might slightly
be under-estimated. Further, the use of psychiatric inpatients might
favour the recruitment of more physically vulnerable persons, because
psychiatric patients with physical illness might be more likely to be
hospitalised than those with mental disorders alone. Finally, this study
was unable to investigate the effects of such risk factors as patients'
socioeconomic status, marital status, education, and family history of
psychiatric conditions related to mortality. Data regarding concurrent
use alcohol, tobacco or other substances were not available.
The continuing excess mortality among psychiatric patients from
both natural and unnatural causes and across different categories of
mental illnesses highlights the ongoing signi
ficance of this problem.
Even after implementation of a universal health-care system in Taiwan
that is free at the point of delivery, this issue remains. Thus, a signi
ficant
next step would be to evaluate the quality of medical care received by
psychiatric patients, ascertaining its weaknesses so that further
improvements can be made. Whether inequitable access to some
medically necessary procedures exists for psychiatric patients under the
NHI and developing strategies to reduce these disparities warrant future
investigation. Consistently high rates of unnatural deaths, especially for
female patients, are warning signals of de
ficiencies in psychiatric
services. More deaths from unnatural causes occur particularly during
or shortly after a psychiatric hospitalisation, reinforcing the need for
more intensive care or follow-up during this period. Routine monitoring
of the side effects of different types and doses of psychotropic
prescriptions, compliance with the medication regimen, and
encoura-ging healthier behaviors and lifestyles deserve special and constant
attention.
Our study supports the continuing development of strategies to
ef
ficiently reduce death rates, such as improvements in health-care
quality, promoting use of medical services, and keeping track of
disturbing psychotic or physical symptoms among psychiatric
patients. Regular monitoring of mortality trends among psychiatric
patients and the effect of the NHI program on death rates should
continue.
Acknowledgements
This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health, Taiwan and managed by the National Health Research Institutes. The interpretations and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health or the National Health Research Institutes.
References
Appleby, L., Thomas, S., Ferrier, N., Lewis, G., Shaw, J., Amos, T., 2000. Sudden unexplained death in psychiatric in-patients. British Journal of Psychiatry 76, 405–406.
Black, D.W., Warrack, G., Winokur, G., 1985. Excess mortality among psychiatric patients. The Iowa Record-Linkage Study. Journal of the American Medical Association 253, 58–61.
Brook, O.H., 1985. Mortality in the long-stay population of Dutch mental hospitals. Acta Psychiatrica et Neurologica Scandinavica 71, 626–635.
Brown, S., 1997. Excess mortality of schizophrenia. A meta-analysis. British Journal of Psychiatry 171, 502–508.
Brown, S., Inskip, H., Barraclough, B., 2000. Causes of the excess mortality of schizophrenia. British Journal of Psychiatry 177, 212–217.
Card, D., Dobkin, C., Maestas, N., 2004. The impact of nearly universal insurance coverage on health care utilization and health: evidence from Medicare. NBER Working Paper Series, vol. 13065.
Casadebaig, F., Quemada, N., 1991. Changes in mortality among psychiatric inpatients, 1968–1982. Social Psychiatry and Psychiatric Epidemiology 26, 78–82.
Chen, W.J., Huang, Y.J., Yeh, L.L., Rin, H., Hwu, H.G., 1996. Excess mortality of psychiatric inpatients in Taiwan. Psychiatry Research 62, 239–250.
Chen, L., Yip, W., Chang, M.C., Lin, H.S., Lee, S.D., Chiu, Y.L., Lin, Y.H., 2007. The effects of Taiwan's National Health Insurance on access and health status of the elderly. Health Economics 16, 223–242.
Chien, I.C., Kuo, C.C., Bih, S.H., Chou, Y.J., Lin, C.H., Lee, C.H., Chou, P., 2007. The prevalence and incidence of treated major depressive disorder among National Health Insurance enrollees in Taiwan, 1996 to 2003. Canadian Journal of Psychiatry 52, 28–36. Table 3
Proportionate mortality by disorder type (N = 34,157).
Cause of deaths (ICD-9-CM codes 001-999) Schizophrenia Depression Bipolar disorder Appendectomy Total
(n = 377) (n = 32) (n = 88) (n = 216) (n = 713)
n (%) n (%) n (%) n (%) n (%)
Infectious and parasitic diseases (001–139) 8 (2.1) 0 (0.0) 2 (2.3) 1 (0.5) 11 (1.5)
Neoplasms (140–239) 26 (6.9) 0 (0.0) 12 (13.6) 56 (25.9) 94 (13.2)
Endocrine, nutritional and metabolic disease and immunity disorders (240–279) 11 (2.9) 0 (0.0) 3 (3.4) 10 (4.6) 24 (3.4)
Diseases of blood and blood-forming organs (280–289) 0 (0.0) 0 (0.0) 1 (1.1) 0 (0.0) 1 (0.1)
Diseases of the nervous system and sense organs (320–389) 3 (0.8) 0 (0.0) 1 (1.1) 8 (3.7) 12 (1.7)
Disease of the circulatory system (390–459) 30 (8.0) 1 (3.1) 1 (1.1) 18 (8.3) 50 (7.0)
Diseases of the respiratory system (460–519) 15 (4.0) 1 (3.1) 2 (2.3) 5 (2.3) 23 (3.2)
Disease of the digestive system (520–579) 26 (6.9) 5 (15.6) 10 (11.4) 26 (12.0) 67 (9.4)
Diseases of the genitourinary system (580–629) 1 (0.3) 0 (0.0) 1 (1.1) 3 (1.4) 5 (0.7)
Disease of the skin and subcutaneous tissue (680–709) 3 (0.8) 0 (0.0) 1 (1.1) 1 (0.5) 5 (0.7)
Disease of the musculoskeletal system and connective tissue (710–739) 0 (0.0) 0 (0.0) 0 (0.0) 1 (0.5) 1 (0.1)
Congenital anomalies (740–759) 3 (0.8) 0 (0.0) 0 (0.0) 0 (0.0) 3 (0.4)
Symptoms, signs, and ill-defined conditions (780–799) 33 (8.8) 3 (9.4) 4 (4.6) 10 (4.6) 50 (7.0)
Injury and poisoning (800–999) 69 (18.3) 6 (18.8) 17 (19.3) 50 (23.2) 142 (19.9)
Suicide (E950–E959) 101 (26.8) 11 (34.4) 24 (27.3) 17 (7.9) 153 (21.5)
Complications of pregnancy, childbirth, and the puerperium (630–679) 0 (0.0) 0 (0.0) 0 (0.0) 1 (0.5) 1 (0.1)
Corten, P., Ribourdouille, M., Dramaix, M., 1991. Premature death among outpatients at a community mental health center. Hospital and Community Psychiatry 42, 1248–1251.
Corten, P., Ribourdouille, M., Hermann, P., Rorsman, B., Sims, A., 1988. Epidemiological survey of the“natural” mortality in psychiatry. Acta Psychiatrica Belgica 88, 349–371.
Cuijpers, P., Smit, F., 2002. Excess mortality in depression: a meta-analysis of community studies. Journal of Affective Disorder 72, 227–236.
Davidson, K., Jonas, B.S., Dixon, K.E., Markovitz, J.H., 2000. Do depression symptoms predict early hypertension incidence in young adults in the CARDIA study? Coronary artery risk development in young adults. Archives of Internal Medicine 160, 1495–1500.
Decker, S., Remler, D., 2004. How much might universal health insurance reduce socioeconomic disparities in health? A comparison of the US and Canada. NBER Working Paper Series, vol. 10715.
Dijkhuis, H., Zwerling, C., Parrish, G., Bennett, T., Kemper, H.C., 1994. Medical examiner data in injury surveillance: a comparison with death certificates. American Journal of Epidemiology 139, 637.
Flanders, W.D., 1992. Inaccuracies of death certificate information. Epidemiology 3, 3–5. Hewer, W., Rössler, W., Fätkenheuer, B., Löffler, W., 1995. Mortality among patients in psychiatric hospitals in Germany. Acta Psychiatrica et Neurologica Scandinavica 91, 174–179.
Honkonen, H., Mattila, A.K., Lehtinen, K., Elo, T., Haataja, R., Joukamaa, M., 2008. Mortality of Finnish acute psychiatric hospital patients. Social Psychiatry and Psychiatric Epidemiology 43 (8), 660–666.
Johannessen, L., Strudsholm, U., Foldager, L., Munk-Jørgensen, P., 2006. Increased risk of hypertension in patients with bipolar disorder and patients with anxiety compared to background population and patients with schizophrenia. Journal of Affective Disorder 95, 13–17.
Kisely, S., Smith, M., Lawrence, D., Cox, M., Campbell, L.A., Maaten, S., 2007. Inequitable access for mentally ill patients to some medically necessary procedures. Canadian Medical Association Journal 176, 779–784.
Lawrence, D.M., Holman, C.D., Jablensky, A.V., Hobbs, M.S., 2003. Death rate from ischaemic heart disease in Western Australian psychiatric patients 1980–1998. British Journal of Psychiatry 182, 31–36.
Marmot, M., Wilkinson, R.G., 1999. Social Determinants of Health. Oxford University Press, Oxford, UK.
Martin, R.L., 1985. Methodological and conceptual problems in the study of mortality in psychiatry. Psychiatric Developments 3, 317–333.
Meloni, D., Miccinesi, G., Bencini, A., Conte, M., Crocetti, E., Zappa, M., Ferrara, M., 2006. Mortality among discharged psychiatric patients in Florence, Italy. Psychiatry Services 57, 1474–1481.
Mortensen, P.B., Juel, K., 1990. Mortality and causes of death in schizophrenic patients in Denmark. Acta Psychiatrica et Neurologica Scandinavica 81, 372–377.
Mortensen, P.B., Juel, K., 1993. Mortality and causes of death in first admitted schizophrenic patients. British Journal of Psychiatry 163, 183–189.
Räsänen, S., Hakko, H., Viilo, K., Meyer-Rochow, V.B., Moring, J., 2003. Excess mortality among long-stay psychiatric patients in northern Finland. Social Psychiatry and Psychiatric Epidemiology 38, 297–304.
Schelin, E.M., Munk-Jørgensen, P., Olesen, A.V., Gerlach, J., 2000. Regional differences in schizophrenia incidence in Denmark. Acta Psychiatrica et Neurologica Scandinavica 101, 293–299.
Sims, A., 1987. Why the excess mortality from psychiatric illness? British Medical Journal (Clinical Research Ed.) 294, 986–987.
Tsuang, M.T., 1978. Suicide in schizophrenics, manics, depressives, and surgical controls. A comparison with general population suicide mortality. Archives of General Psychiatry 35, 153–155.
Tsuang, M.T., Woolson, R.F., 1978. Excess mortality in schizophrenia and affective disorders. Do suicides and accidental deaths solely account for this excess? Archives of General Psychiatry 35, 1181–1185.
Tsuang, M.T., Simpson, J.C., 1985. Mortality studies in psychiatry. Should they stop or proceed? Archives of General Psychiatry 42, 98–103.
Wang, C.S., Chou, P., 1997. An analysis of unnatural deaths between 1990 and 1994 in A-Lein, Taiwan. Injury 28 (3), 203–208.
Wood, J.B., Evenson, R.C., Cho, D.W., Hagan, B.J., 1985. Mortality variations among public mental health patients. Acta Psychiatrica et Neurologica Scandinavica 72, 218–229. Yip, P.S., 1996. Suicides in Hong Kong, Taiwan and Beijing. British Journal of Psychiatry
169 (4), 495–500.
Zarate, C.A., Patel, J., 2001. Sudden cardiac death and antipsychotic drugs: do we know enough? Archives of General Psychiatry 58, 1168–1171.