ORIGINAL ARTICLE
A observational study of the efficacy and safety
of capecitabine versus bolus infusional 5-fluorouracil
in pre-operative chemoradiotherapy for locally advanced
rectal cancer
Chin-Fan Chen&Ming-Yii Huang&Chih-Jen Huang&
Chan-Han Wu&Yung-Sung Yeh&Hsiang-Lin Tsai&
Cheng-Jen Ma&Chien-Yu Lu&Shun-Jen Chang&
Ming-Jenn Chen&Jaw-Yuan Wang
Accepted: 24 November 2011 / Published online: 19 January 2012 # Springer-Verlag 2012
Abstract
Background and objectives This study is to evaluate the safety and efficacy of preoperative radiotherapy (RT) combined with bolus infusional 5-fluorouracil (5-FU) or oral capecitabine in patients with locally advanced rectal cancer (LARC). Materials and methods Seventy-four patients were retro-spectively analyzed. Twenty-seven patients were treated with 5-FU (350 mg/m2 IV bolus) and leucovorin (20 mg/ m2IV bolus) for 5 days/week during week 1 and 5 of RT. Forty-seven patients were treated with capecitabine
(850 mg/m2, twice daily for 5 days/week). Both groups received the same RT course (45–50.4 Gy/25 fractions, 5 days/week, for 5 weeks). Patients underwent surgery in 6 weeks after completion of the chemoradiotherapy. Data of the observational study were collected.
Results Grade 3 or 4 toxicities occurred in 40.7% (5-FU) and 19.1% (capecitabine) of the patients (P00.044). Six patients in the 5-FU group (22.2%) and six patients in the capecitabine group (14%) achieved complete response. Pri-mary tumor (T) downstaging were achieved in 51.9%
(5-C.-F. Chen
:
Y.-S. YehDepartment of Emergency Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan
M.-Y. Huang
:
C.-J. HuangDepartment of Radiation Oncology, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan
M.-Y. Huang
:
C.-J. HuangDepartment of Radiation Oncology, Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
C.-H. Wu
Department of Medical Research, Fooyin University Hospital, Pingtung, Taiwan
H.-L. Tsai
Division of General Surgery Medicine, Department of Surgery, Kaohsiung Medical University Hospital,
Kaohsiung Medical University, Kaohsiung, Taiwan
H.-L. Tsai
School of Medical and Health Sciences, Fooyin University, Kaohsiung, Taiwan
C.-J. Ma
:
J.-Y. Wang (*)Division of Gastrointestinal and General Surgery,
Department of Surgery, Kaohsiung Medical University Hospital, Kaohsiung Medical University,
No. 100 Tzyou 1st Road, Kaohsiung 807, Taiwan
e-mail: [email protected] J.-Y. Wang
e-mail: [email protected] C.-Y. Lu
Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital,
Kaohsiung Medical University, Kaohsiung, Taiwan
C.-Y. Lu
Department of Internal Medicine, Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
FU) and 69.8% (capecitabine) of the patients. The patholog-ical ypT0-2 stage was 40.7% (5-FU) and 67.4% (capecita-bine) (P00.028).
Conclusions In consideration of the better ypT0-2 down-staging rate, less severe toxicities, and no need for indwell-ing intravenous device on oral capecitabine regimen, the administration of oral capecitabine with RT may be a more favorable option in the neoadjuvant treatment for LARC.
Keywords Preoperative chemoradiation . Rectal cancer . Capecitabine . 5-FU
Introduction
Since the randomized phase III study conducted by the German Rectal Cancer Study Group showing the advan-tages including lower acute toxicity, lower local recurrence rate, and improved sphincter preservation in comparison with postoperative chemoradiotherapy, preoperative concur-rent chemoradiotherapy (CCRT) has been suggested for patients with locally advanced rectal cancer (LARC) [1]. Since then, 5-fluorouracil (5-FU) and leucovorin (LV) has been the standard chemotherapy in combination with radio-therapy (RT) in the neoadjuvant treatment of LARC [2]. Because of the disadvantages of infusional 5-FU (either continuous or bolus infusion) including the need for in-dwelling catheters with potential complications (infection, bleeding, thrombosis, etc.) [3], oral fluoropyrimidine has been gradually used as an alternative in this situation.
Capecitabine is an oral fluoropyrimidine carbamate pro-drug of 5-FU. It is converted to 5-FU via three steps, including involvement of the thymidine phosphorylase (TP) at the final step [4]. Capecitabine does not only provide a convenient method of administration without the
complications of venous access indeed but also has the characteristics of tumor-selective generation of 5-FU be-cause of higher levels of TP in tumor tissue than in adjacent normal tissue [5]. In addition, a synergistic effect has been found between capecitabine and RT. Sawada et al. [6] con-firmed that RT increases the TP level in tumor cells, thereby upregulating the enzyme's activity. This leads to a more effective conversion of capecitabine to 5-FU within tumor cells, thus improving the drug's efficacy. Therefore, the aim of this study was to retrospectively compare capecitabine and 5-FU regarding the efficacy and safety of two different chemotherapy regimens (bolus infusional 5-FU/LV vs. oral capecitabine) combined RT in the preoperative treatment of patients with LARC, with the additional analysis on low-lying tumors (tumor located≦5 cm from the anal verge).
Materials and methods
Patients
Between November 2006 and June 2011, 74 patients with LARC (T3/T4 disease or any clinical positive N-stage) located within 10 cm from the anal verge receiving preop-erative concurrent chemoradiotherapy (CCRT) were en-rolled in this study. The study was approved by the ethics committee of the Kaohsiung Medical University Hospital. Baseline assessment before initiation of CCRT included complete medical history and physical examination, colono-scopy, tumor biopsy, pelvic and abdominal computed to-mography (CT), endorectal ultrasonography (ERUS) (if clinically feasible), and/or pelvic magnetic resonance imag-ing (MRI). Complete laboratory tests included a complete blood cell count, liver function tests, electrolytes, creatinine, albumin, and carcinoembryonic antigen (CEA). All patients
S.-J. Chang
Faculty of Medicine, College of Medicine, Kaohsiung Medical University,
Kaohsiung, Taiwan
M.-J. Chen (*)
Department of Surgery, Chi-Mei Medical Center, 901 Chung Hwa Road,
Yung Kang, Tainan 710, Taiwan e-mail: [email protected]
M.-J. Chen
Department of Sports Management,
College of Leisure and Recreation Management, Chia Nan University of Pharmacy and Science, Tainan, Taiwan
J.-Y. Wang
Cancer Center, Kaohsiung Medical University Hospital, Kaohsiung Medical University,
Kaohsiung, Taiwan C.-F. Chen
:
S.-J. ChangGraduate Institute of Clinical Medicine, College of Medicine, Kaohsiung Medical University,
Kaohsiung, Taiwan J.-Y. Wang
Graduate Institute of Medicine, College of Medicine, Kaohsiung Medical University,
Kaohsiung, Taiwan J.-Y. Wang
Department of Medical Genetics, College of Medicine, Kaohsiung Medical University,
had Eastern Cooperative Oncology Group (ECOG) perfor-mance statuse2, with ages between 18 and 85 years and adequate hematological, liver, and renal function.
Chemotherapy
In this study, patients were divided into two groups accord-ing to the use of different regimens of chemotherapy. Of the 74 patients, 27 patients were treated with 5-FU (350 mg/m2 IV bolus) and leucovorin (20 mg/m2IV bolus) on days 1 through 5 and days 21 through 25 fractions of the radiother-apy (RT). Forty-seven patients were treated with capecita-bine (850 mg/m2, twice daily, 5 days per week, during the days when RT was administered). The first daily dose of capecitabine was given 2 h before radiotherapy and the second dose was 8 to 10 h later.
Radiotherapy
Radiation was delivered via 6- and 10-MV photons by use of a three-field technique (posterior and both laterals) in most patients. Treatment was planned via computerized dosimetry, and a dose of 1.8 Gy per fraction was prescribed to cover the planning target volume. Radiotherapy was delivered 5 days per week, once per day, at 1.8 Gy/day. Pelvic radiotherapy consisted of 45 Gy in 25 fractions over a period of 5 weeks, which was followed by a boost dose of 5.4 Gy administered in three fractions to the primary tumor by two lateral fields. The clinical target volume contained the primary tumor, the mesorectum, the presacral space, and the lymph nodes, which included the perirectal, presacral, internal iliac, and/or external iliac nodes as indicated. For the whole-pelvis field, the superior border was located at the L5–S1 interspace, and the inferior border was located 3 to 4 cm below the primary tumor. The lateral border was located 1.5 cm outside of the true bony pelvis. For the lateral fields, the posterior margin was 1.5 cm behind the anterior bony sacral margin, and the anterior border generally com-prised anterior acetabulum. The radiation therapy technique administered to patients in the two groups was identical.
Patients were evaluated weekly during the course of CCRT to assess the acute toxicity and compliance of patients. Blood tests were taken each time and consisted of complete blood cell count and differential count. The toxic-ity was monitored by use of the National Cancer Institute Common Toxicity Criteria, version 3.0 (http://ctep.cancer. gov/reporting/ctc.html; accessed in December 2010). Che-motherapy and/or radiotherapy were withheld if any chemotherapy-related grade 3 or 4 toxicity was noted, and appropriate dose adjustment was undertaken thereafter. Che-motherapy was restarted at an 80% dose if toxicity levels resolved and was stopped if grade 3 or 4 toxicity was noted
again after adjustment of the dosage. If grade 3 or 4 toxicity was clearly related to radiotherapy, for example, radiation dermatitis, local therapy was administered and chemothera-py was not stopped.
Surgery
Patients underwent surgery 6 weeks after completion of the CCRT. Total mesorectal excision technique was performed in all patients, and extended visceral resection was per-formed in clinically T4 patients. Anal sphincter-sparing surgery was performed when possible, with primary anas-tomosis and/or temporary diverting colostomies. The char-acteristics of each patient, the adverse events and the response after the chemoradiotherapy were recorded. Safety was mainly assessed by the proportion of patients who experienced grade 3 or 4 toxicity. Efficacy was assessed by determining the pathological complete response (pCR) rate and tumor downstaging rate. A pathologic complete response was defined as the absence of any viable residual tumor cell in the resected primary tumor and adjacent lymph nodes. The determination for downstaging was based on the comparison between the clinical TNM stage before the initiation of CCRT and the postoperative histopathological TNM stage. The primary endpoints were the pCR, tumor downstaging, and sphincter preservation rate after the pre-operative CCRT. The secondary endpoints were the acute toxicities during CCRT.
Statistical analysis
All data were statistically analyzed using the Statistical Package for the Social Sciences, version 17.0 (SPSS Inc., Chicago, IL). Independent t test was used for comparison of continuous variables. Categorical data were analyzed by Pearson Chi-Square test or Fisher's exact test (two-sided), and either of these was used to compare the parameters between the two regimens when appropriate. A P value less than 0.05 was considered to be significant statistically.
Results
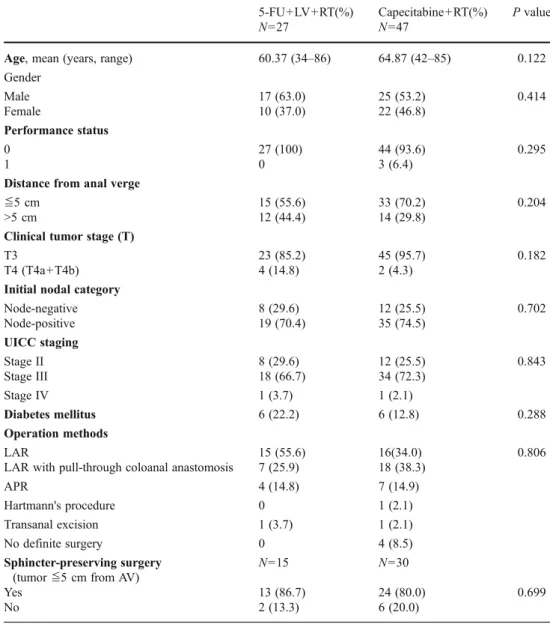
Seventy-four patients with LARC and receiving pre-operative CCRT were analyzed retrospectively and their characteristics are summarized in Table1. All patients had a good initial performance status (ECOG performance status grading system 0–1) before initiation of the CCRT. Mean age was 60.37 years (34–86) in the 5-FU group and 64.87 years (42–85) in the capecitabine group (P00.122). More male patients in the 5-FU group (63.0%) in compar-ison with those in the capecitabine group (53.2%) were
noted, but this difference was not statistically significant (P00.414). The two groups were well matched for clinical T stage, node metastasis, distance of tumor to anal verge, and underlying diabetes mellitus disease.
Toxicities
The acute toxicities encountered are listed in Table 2. All patients in both groups were assessable for toxicities. The most common overall adverse events encountered in this study were diarrhea (5-FU vs. capecitabine, 77.8% vs. 53.2%, P00.036), followed by anemia (22.2% vs. 12.8%, P00.288) and radiation dermatitis (11.1% vs. 31.9%, P0 0.053). Fortunately, most of these adverse events could be abated by medications. In grade 3 or grade 4 (grade 3+), acute toxicities developing during the CCRT was 40.7% in the 5-FU group and 19.1% in the capecitabine group (P0 0.044). The main grade 3+ adverse events encountered in
these patients were diarrhea (5-FU vs. capecitabine, 25.9% vs. 17.0%, P00.359), leukopenia (7.4% vs. 0%, P00.130), ane-mia (3.7% vs. 2.1%), and radiation dermatitis (7.4% vs. 0%, P00.130). Among all the patients in the study, no patient needed to stop the chemoradiotherapy because of any intoler-able acute toxicity. Three patients suffered from grade 3+ acute toxicities and needed hospitalization, but they recovered uneventfully after adequate conservative treatment.
Sphincter preservation
After completion of CCRT, all the 27 patients in the 5-FU group and 43 of the 47 patients (91.5%) in the capecitabine group underwent definitive surgery. Four patients in the capecitabine group refused surgery after CCRT and were excluded from the assessment of pathological response and sphincter preservation. The types and numbers of surgical resections performed in both 5-FU and capecitabine groups
Table 1 Characteristics of the studied patients
5-FU 5-fluorouracil, LV leuco-vorin, RT radiotherapy, AV anal verge 5-FU+LV+RT(%) N027 Capecitabine +RT(%) N047 P value
Age, mean (years, range) 60.37 (34–86) 64.87 (42–85) 0.122 Gender Male 17 (63.0) 25 (53.2) 0.414 Female 10 (37.0) 22 (46.8) Performance status 0 27 (100) 44 (93.6) 0.295 1 0 3 (6.4)
Distance from anal verge
o5 cm 15 (55.6) 33 (70.2) 0.204
>5 cm 12 (44.4) 14 (29.8)
Clinical tumor stage (T)
T3 23 (85.2) 45 (95.7) 0.182
T4 (T4a+T4b) 4 (14.8) 2 (4.3)
Initial nodal category
Node-negative 8 (29.6) 12 (25.5) 0.702 Node-positive 19 (70.4) 35 (74.5) UICC staging Stage II 8 (29.6) 12 (25.5) 0.843 Stage III 18 (66.7) 34 (72.3) Stage IV 1 (3.7) 1 (2.1) Diabetes mellitus 6 (22.2) 6 (12.8) 0.288 Operation methods LAR 15 (55.6) 16(34.0) 0.806
LAR with pull-through coloanal anastomosis 7 (25.9) 18 (38.3)
APR 4 (14.8) 7 (14.9)
Hartmann's procedure 0 1 (2.1)
Transanal excision 1 (3.7) 1 (2.1)
No definite surgery 0 4 (8.5)
Sphincter-preserving surgery (tumoro5 cm from AV)
N015 N030
Yes 13 (86.7) 24 (80.0) 0.699
were: low anterior resection (LAR), 22 vs. 34 (including pull through coloanal anastomosis, 7 vs. 18); abdominoperineal resection (APR), 4 vs. 7; Hartmann's procedure, 0 vs. 1, and transanal full-thickness excision, 1 vs. 1. Fifteen of 27 patients in the 5-FU group and 30 of 43 patients in the capecitabine group had low-lying tumors (tumor located≦5 cm from the anal verge). Among these patients, 13 of the 15 patients (86.7%) in the 5-FU group and 24 of the 30 patients (80%) in the capecitabine group were able to undergo sphincter-sparing procedure (P00.699).
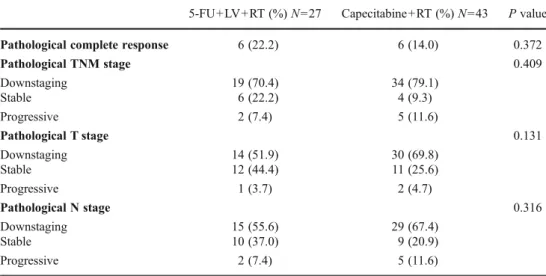
Pathological response
The objective pathologic response is summarized in Tables3 and 4. Twenty-seven patients in the 5-FU group and 43 patients in the capecitabine group were enrolled for evaluation of the pathological response. The histopathologic stage of
resected specimens in both groups was as follows: stage I in 11.1% vs. 33.3%; stage II in 25.9% vs. 12.8%; stage III in 37.0% vs.35.9%; and stage IV in 3.7% vs. 2.6%. Pathological complete response was achieved in 22.2% (5-FU group) and 14.0% (capecitabine group) (P00.372). By comparing clini-cal and postoperative histopathologic stages, downstaging of TNM stage was achieved in 19 of 27 patients (70.4%) in the 5-FU group and 34 of 43 patients (79.1%) in the capecitabine group (P00.409). Primary tumor (T) and node (N) down-staging were achieved in 51.9% vs.55.6% (5-FU group) and 69.8% vs. 67.4% (capecitabine group) of the patients (T downstaging, P00.131; N downstaging, P00.316).
Perioperative morbidity and mortality
Three of 27 patients (11.1%) in the 5-FU group in compar-ison with one of the 43 patients (2.3%) in the capecitabine
Table 2 Acute toxicities during preoperative chemoradiotherapy
5-FU 5-fluorouracil, LV leuco-vorin, RT radiotherapy
5-FU+LV+RT (%) N027 Capecitabine +RT (%) N047 P value
Grade 3 or 4 toxicities 11 (40.7) 9 (19.1) 0.044 Nausea/vomiting 0.309 Grade 1 0 4 (8.5) Grade 2 2 (7.4) 4 (8.5) Diarrhea 0.036 Grade 1 1 (3.7) 8 (17.0) Grade 2 13 (48.1) 9 (19.1) Grade 3 7 (25.9) 8 (17.0) 0.359 Grade 4 0 0 Constipation 0.550 Grade 1 0 1 (2.1) Grade 2 2 (7.4) 0 Leukopenia 0.550 Grade 2 0 1 (2.1) Grade 3 2 (7.4) 0 0.130 Anemia 0.288 Grade 1 5 (18.5) 2 (4.3) Grade 2 0 3 (6.4) Grade 3 0 1 (2.1) Grade 4 1 (3.7) 0 Thrombocytopenia Grade 2 1 (3.7) 0 Frequency/urgency 0.411 Grade 1 0 4 (8.5) Grade 2 1 (3.7) 2 (4.3) Dermatitis 0.053 Grade 1 1 (3.7) 11 (23.4) Grade 2 0 (0) 4 (8.5) Grade 3 2 (7.4) 0 0.130 Hand-foot syndrome Grade 2 0 1 (2.1)
group suffered from anastomotic leakage after the definite surgery (P00.291). Of the four patients with anastomotic leakage, two have to receive computed tomography-guided drainage of the pelvic abscess, another one received conser-vative treatment with total parenteral nutrition and antibiot-ics, and the last one underwent transverse colostomy for fecal diversion. All four patients made an uneventful recov-ery after the treatments. Besides, 25 patients underwent pull-through coloanal anastomosis in the study. Among the 25 patients, neither anastomotic leakage nor fistula was ob-served. Three patients (12%) encountered anastomotic ste-nosis and required anal bougination in the follow-up time. In consideration of the functional outcome, 20 of the 25 patients (80%) had bowel frequency at about 1–2 bowel movement per day. Another three patients (12%) had 3–5 bowel movements per day. The last two patients (8%)
suffered from incontinence problems (incontinent of flatus in one patient, incontinent of liquid stool and flatus in another) after taking down the ileostomy and restoring the bowel continuity. Neither life-threatening complications nor any treatment-related death occurred postoperatively in the study.
Comparison of efficacy and toxicities with previous studies
Table 5 summarizes the efficacy of previously published studies using preoperative RT combined with either bolus 5-FU or capecitabine in the treatment of patients with LARC. It shows pCR rates ranging from 10% to 13% in bolus 5-FU regimen versus 7% to 30.2% in capecitabine regimen [7–21]. Additionally, tumor downstaging rates were 70.5% in bolus 5-FU regimens in comparison with
Table 3 Correlation between the clinical T stage and patho-logical T stage (%)
5-FU 5-fluorouracil, LV leuco-vorin, RT radiotherapy
5-FU+LV+R/T N027
ypT0 ypT1 ypT2 ypT3 ypT4a ypT4b Total
cT1 0 0 0 0 0 0 0 cT2 0 0 0 0 0 0 0 cT3 7 (25.9) 0 4 (14.8) 11 (40.7) 0 1 (3.7) 23 (85.2) cT4a 0 0 0 1 (3.7) 0 0 1 (3.7) cT4b 0 0 0 2 (7.4) 0 1 (3.7) 3 (11.1) Total 7 (25.9) 0 4 (14.8) 14 (51.9) 0 2 (7.4) 27 Capecitabine N043
ypT0 ypT1 ypT2 ypT3 ypT4a ypT4b Total
cT1 0 0 0 0 0 0 0 cT2 0 0 0 0 0 0 0 cT3 7 (16.3) 2 (4.7) 20 (42.6) 10 (23.3) 1 (2.3) 1 (2.3) 41 (95.3) cT4a 0 0 0 0 0 0 0 cT4b 0 0 0 1 (2.3) 1 (2.3) 0 2 (4.7) Total 7 (16.3) 2 (4.7) 20 (46.5) 11 (25.6) 2 (4.7) 1 (2.3) 43
Table 4 Response after preop-erative chemoradiotherapy in patients with LARC
LARC locally advanced rectal cancer, 5-FU 5-fluorouracil, LV leucovorin, RT radiotherapy
5-FU+LV+RT (%) N027 Capecitabine +RT (%) N043 P value Pathological complete response 6 (22.2) 6 (14.0) 0.372
Pathological TNM stage 0.409 Downstaging 19 (70.4) 34 (79.1) Stable 6 (22.2) 4 (9.3) Progressive 2 (7.4) 5 (11.6) Pathological T stage 0.131 Downstaging 14 (51.9) 30 (69.8) Stable 12 (44.4) 11 (25.6) Progressive 1 (3.7) 2 (4.7) Pathological N stage 0.316 Downstaging 15 (55.6) 29 (67.4) Stable 10 (37.0) 9 (20.9) Progressive 2 (7.4) 5 (11.6)
Table 5 Summary of efficacy of 5-FU or capecitabine based preoperative chemoradiotherapy in patients with LARC
Bolus infusional 5-FU +LV
Case number Dose of 5-FU (mg/m2/day) Dose of RT pCR (%) Sphincter preservation (%) for distal rectal tumor Tumor down-staging (%)
Minsky et al. [7] 25 325+LV 20 mg/m2/day × 5 days/week, on first and fourth weekfof RT
46.8 Gy in 25 fractions × 5 days/week × 5 week, 3.6 Gy boost
12 N
Mohiuddin et al. [8] 21 1,000 mg/m2during
day1–4 and day 28–32 of RT
45 to 60 Gy in 25 fractions, 5 days/week × 5 week
10 N
Grann et al. [9] 72 325+LV 20 mg/m2/day
× 5 days/week, on first and fifth week of RT
46.8 Gy in 25 fractions, 5 days/week × 5 week, 3.6 Gy boost 13 89 N Bosset et al. [10] (EORTC 22921) 506 350+LV 20 mg/m2/day × 5 days/week, on first and fifth week of RT
45 Gy in 25 fractions, 5 days/week × 5 week N N N Gerard et al. [11] (FFCD 9203) 375 350+LV 20 mg/m2/day, × 5 days/week, on first and fifth week of RT
45 Gy in 25 fractions 5 days/week × 5 week
11.4 N
Kim et al. [12] 127 500+LV 20 mg/m2/day
× 5 days/week, on first and fifth week of RT
45 Gy in 25 fractions, 5 days/week × 5 week, 5.4 Gy boost
11.4 42.1 70.5
Current study (2011) 27 350+LV 20 mg/m2/day × 5 days/week, on first and fifth week of RT
45–50.4 Gy in 25 fractions, 5 days/week × 5 week
22.2 86.7 70.4
Oral capecitabine
Case Number Dose of capecitabine Dose of RT pCR (%) Sphincter Preservation (%) for distal rectal tumor
Tumor Down-staging (%)
Kim et al. [12] 97 825 mg/m2twice daily,
for 14 days followed by a 7-day rest period
45 Gy in 25 fractions, 5 days/week × 5 week, 5.4 Gy boost 22.2 66.7 86.7 Yerushalmi et al. [13] 43 825 mg/m2twice daily, 5 days/week on RT day 45 Gy in 25 fractions, 5 days/week × 5 week, 5.4 Gy boost 30.2 N 76.7
Das et al. [14] 89 825 mg/m2twice daily, 5 days/week (65.2%) and 7 days/week (34.8%) on RT day 45 Gy in 25 fractions, 5 days/week × 5 week, 0–7.5 Gy boost 21 N 52.0
De Paoli et al. [15] 53 825 mg/m2twice daily, 7 days/week on RT day
45 Gy in 25 fractions, 5 days/week × 5 week, 5.4 Gy boost
24 59 57
Desai et al. [16] 30 665 mg/m2twice daily,
7 days/week × 6 weeks
45 Gy in 25 fractions, 5 days/week × 5 week, 5.4 Gy boost
11 10.5 78.3
Craven et al. [17] 70 900 mg/m2twice daily,
5 days/week on RT day
45 Gy in 25 fractions, 5 days/week × 5 week
9.2 N 41
Dunst et al. [18] 96 825 mg/m2twice daily,
7 days/week for the duration of RT
50.4 Gy,daily 1.8 Gy × 5–6 week, 5.4 Gy boost for T4 lesions
7 N 61.0
Elwanis et al. [19] 43 825 mg/m2twice daily, 5 days/week on RT day
45 Gy in 25 fractions, 5 days/week × 5 week
9.3 31.3 74.4 Marsh et al. [20] 17 825 mg/m2twice daily,
7 days/week on RT day
A total of 50.4/55.2 Gy for T3/T4 lesions. Twice daily fractions of 1.2 Gy, 5 days/week
18.8 63.6 81.3
Chan et al. [21] 34 825 mg/m2twice daily,
5 days/week on RT day
44 Gy in 22 fractions, 5 days/week × 5 week, 6 Gy boost
20.5 23 59
Current study. (2011) 43 850 mg/m2twice daily, 5 days/week on RT day
45–50.4 Gy in 25 fractions, 5 days/week × 5 week
14.0 80 79.1
5-FU 5-fluorouracil; LARC locally advanced rectal cancer, LV leucovorin, RT radiotherapy, pCR pathological complete response, N not reported, AV anal verge
the range of 41% to 86.7% in the capecitabine regimen [12– 21]. Despite the comparable results in the capecitabine group, the pCR rate in the 5-FU group in our study seemed to be slightly higher than that in other studies. Concerning the incidence of grade 3+ diarrhea and the phenomenon that severe leukopenia occurred more frequently in patients receiving bolus 5-FU; both were similar to other studies (Table 6, grade 3+ diarrhea, 9.5–22.8% in the 5-FU group and 0–25% in the capecitabine group, grade 3+ leukopenia, 0–18% in the 5-FU group and 0–4% in the capecitabine group) [7,9–21], in spite of our 5-FU group showing a slight increase in grade 3+ diarrhea compared to others.
Discussion
In patients with distal rectal tumors, the goal of preoperative radiotherapy alone or combined with chemotherapy is to downstage the tumor and allow for a sphincter-sparing surgical procedure, thereby improving quality of life and possibly prognosis [1]. Both continous infusional and bolus infusional 5-FU/LV are acceptable treatment regimen for patients with LARC according to NCCN (National Com-prehensive Cancer Network) guideline (http://www.nccn.
org/professionals/physician_gls/f_guidelines.asp). However, continuous infusion at a scheduled dose per day, either in week 1 and 5 or during the complete radiotherapy, required an intravenous device for each patient. Therefore, bolus infusional 5-FU/LV is used more common than continuous infusion in Taiwan. In this study, we compared the efficacy and acute toxicities during preoperative chemoradiother-apy (bolus infusional 5-FU/LV or oral capecitabine com-bined with concomitant RT) for patients with LARC. The pCR rate was 22.2% in the bolus 5-FU group and 14.0% in the capecitabine group, and TNM downstaging rate was 70.4% in the 5-FU group and 79.1% in the capecitabine group. Therefore, the 5-FU group showed grossly compa-rable efficacy with the capecitabine group in our study. However, the pathological ypT0-2 stage was 40.7% (5-FU) and 69.8% (capecitabine) (P00.028). The pathologi-cal node-negative rate was 59.3% (5-FU) and 69.8% (cape-citabine), respectively (P00.367). With matched clinical T stage, more patients treated with the capecitabine group achieved a higher pathological ypT0-2 stage after CCRT than those with the 5-FU group. Additionally, Hofheinz et al. [22] also showed that capecitabine group achieved higher ypT0-2 stage after CCRT in their randomized trial for patients with LARC, of which was comparable with our results. Because the previous literature have mentioned
Table 6 Summary of grade 3 or 4 acute toxicities during preoperative 5-FU or capecitabine based chemoradiotherapy in patients with LARC (%)
Grade 3 or 4 toxicities Diarrhea Leukopenia Anemia Thrombocytopenia Radiation dermatitis
Hand-foot syndrome Bolus infusional 5-FU +LV (%)
Mohiuddin et al. [8] N 9.5 0 0 0 0 0 Grann et al. [9] 24 11 18 0 1 0 0 Bosset et al. [10] (EORTC 22921) 13.9 RGrade 2, 37.6 NC Gerard et al. [11] (FFCD 9203) Non-hematologic 13.5, overall 14.9 N Kim et al. [12] N 22.8 7.9 0 1.6 11.8 0 Current study. (2011) 40.7 25.9 7.4 3.7 0 7.4 0 Oral capecitabine (%) Kim et al. [12] N 11.3 0 0 0 3.1 6.2 Yerushalmi et al. [13] 14.0 2 0 N 0 5 2 Das et al. [14] 5.6 4.5 1.1 0 0 0 0 De Paoli et al. [15] 11.3 2 4 4 2 4 4 Desai et al. [16] 26.7 20 0 0 0 3.3 3.3 Craven et al. [17] N 4.3 N Dunst et al. [18] N 7 N 1.1 0 Elwanis et al. [19] 0 0 0 0 0 0 0 Marsh et al. [20] 25.0 25 0 0 0 0 0 Chan et al. [21] 8.8 8.8 0 0 0 0 0 Current study. (2011) 19.1 17.0 0 2.1 0 0 0
that downstaging towards a ypT0-2 stage after neoadjuvant CCRT in patients with rectal cancer correlates well with a favorable prognosis [23,24], the findings may also help us to predict a possibility of better outcome in the capecita-bine group in the study.
All grade 3 or 4 toxicities during the preoperative CCRT was 40.7% in the 5-FU group and 19.1% in the capecitabine group (P00.044). Thus, our result showed the capecitabine group with less grade 3+ toxicities in comparison with the 5-FU group. Moreover, diarrhea was the most common non-hematologic grade 3+ toxicities encountered in both groups (5-FU vs. capecitabine, 25.9% vs. 17.0%). Among the grade 3 + hematologic toxicities, leukopenia was noted only in the 5-FU group in our study. Both Hoff et al. and Scheithauer et al. [25,26] had mentioned that capecitabine was less toxic than infusional 5-FU when administered to patients with advanced colorectal cancer. Kim et al. [12] conducted a retrospective study comparing the efficacy and toxicity of bolus 5-FU (500 mg/m2/day) versus capecitabine (825 mg/m2twice daily) in combination with preoperative RT in patients with rectal cancer, a higher incidence of grade 3+ diarrhea and leukopenia was also noted in their 5-FU group (5-FU vs. capecitabine, diarrhea 22.8% vs. 11.3%, leukopenia 7.9% vs. 0%), of which was in consistence with our results. Besides, no grade 3 hand foot syndrome was noted in our study compared with 0–6.2% in the literature [12–16,18–21], and only one patient in the capecitabine group encountered grade 2 toxicity. Fortunately, this could be easily managed without interruption of the CCRT. Both patients with grade 3 radiation dermatitis in our study were low-lying rectal tumors (tumor located≦5 cm from the anal verge). Because more patients with low-lying rectal tumors were in the capecitabine group (5-FU vs. capecitabine, 55.6% vs. 70.2%), this could explain that more radiation dermatitis adverse events occurred in the capecitabine group (11.1% vs. 31.9%).
In our study, 91.5% patients in the capecitabine group and all in the 5-FU group underwent definite surgery after CCRT. Of the 15 patients (5-FU) and 30 patients (capecita-bine) who were clinically judged on initial survey to require an APR (tumor located≦5 cm from the anal verge) and one major goal of CCRT treatment was sphincter preservation, 86.7% (13/15) and 80.0% (24/30) of patients were able to undergo sphincter-sparing operations, respectively. No sig-nificant difference was found in the rates of sphincter pres-ervation between the two groups. Tumor downstaging and pCR after neoadjuvant CCRT is closely related to sphincter preservation in patients with low-lying rectal cancer. In our study, all six patients with low-lying rectal cancer achieving pCR after CCRT (three in the 5-FU group, three in the capecitabine group) could receive sphincter-sparing opera-tion, whereas the previous studies showed sphincter preser-vation rates of 42.1–89% in patients receiving bolus 5-FU regimen and 10.5–66.7% in those receiving capecitabine
regimen [9,10,12,15,16,19–21], of which was in consis-tence with our results.
Of the 25 patients who received preoperative CCRT and underwent pull-through coloanal anastomosis for restoring bowel continuity, the median bowel movements were two times per day in the postoperative follow-up time, and this is similar to results of the study conducted by Nathanson et al. [27]. In contrast with one patient in the capecitabine group, three patients with anastomotic leakage were noted in the 5-FU group (P00.291) and all of them received LAR without a diverting colostomy. Of the 36 patients who had low-lying rectal cancer and underwent sphincter-sparing operation, 19 had a temporary diverting colostomy. None of the 19 patients with a temporary diverting colostomy in com-parison with three of the remaining 17 patients (17.6%) without a temporary diverting colostomy suffered from anastomotic leakage (P00.095). By reviewing the litera-ture, Huh et al. [28] also reported their experience about 6.1% anastomotic leakage rate in patients with low rectal cancer treated by preoperative concurrent chemoradiation and subsequent LAR (no diverting stoma) in comparison with 0% in those without receiving preoperative chemoradiation, there-fore suggesting diverting stoma should be made in patients with low rectal cancer who are preoperatively radiated. We believe that more evidence from other studies is still needed for surgeons to determine whether routine diverting colosto-my is necessary in surgical management of low-lying rectal cancer after chemoradiation.
There are some limitations in this retrospective study. First, the sample size in the study was relatively smaller, and this factor may make the study unable to detect small, but clinically important differences between the two groups. Second, there are only response rates but no survival rates in the limited up period; we still need a longer follow-up time of patients in both grofollow-ups to analyze the survival difference between the two groups.
In summary, our results showed that both 5-FU/LV and capecitabine, combined with concomitant RT, are well acceptable preoperative treatment in patients with LARC. Both regimens showed a comparable efficacy, as mea-sured by pathologic complete response, TNM downstag-ing, and sphincter preservation rate. However, the possible complications related to the intravenous device, the less pathological ypT0-2 downstaging rate and the higher grade 3+ toxicities on bolus 5-FU/LV regimen, we suggest that the use of oral capecitabine combined with RT may be a more favorable choice in the neoadjuvant treatment for LARC.
Acknowledgements This study was supported by grants from the Excellence for Cancer Research Center Grant through the funding by Department of Health, Executive Yuan, Taiwan, Republic of China (DOH101-TD-C-111-002) and the Kaohsiung Medical University Hospital (KMUH98-8I04).
References
1. Sauer R, Becker H, Hohenberger W, Rödel C, Wittekind C, Fietkau R, Martus P, Tschmelitsch J, Hager E, Hess CF, Karstens JH, Liersch T, Schmidberger H, Raab R (2004) Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 351:1731–1740
2. Klaassen RA, Nieuwenhuijzena GA, Martijn H, Rutten HJ, Hospers GA, Wiggers T (2004) Treatment of locally advanced rectal cancer. Surg Oncol 13:137–147
3. Di Carlo I, Pulvirenti E, Mannino M, Toro A (2010) Increased use of percutaneous technique for totally implantable venous access devices. Is it real progress? A 27-year comprehensive review on early complications. Ann Surg Oncol 17(6):1649–1656
4. Walko CM, Lindley C (2005) Capecitabine: A Review. Clin Ther 27:23–44
5. Schüller J, Cassidy J, Dumont E, Roos B, Durston S, Banken L, Utoh M, Mori K, Weidekamm E, Reigner B (2000) Preferential activation of capecitabine in tumor following oral administration in colorectal cancer patients. Cancer Chemother Pharmacol 45:291– 297
6. Sawada N, Ishikawa T, Sekiguchi F, Tanaka Y, Ishitsuka H (1999) X-ray irradiation induces thymidine phosphorylase and enhances the efficacy of capecitabine (Xeloda) in human cancer xenografts. Clin Cancer Res 5:2948–2953
7. Minsky BD, Cohen AM, Enker WE, Saltz L, Guillem JG, Paty PB, Kelsen DP, Kemeny N, Ilson D, Bass J, Conti J (1997) Preopera-tive 5-FU, low-dose leukovorin, and radiation therapy for locally advanced and unresectable rectal cancer. Int J Radiat Oncol Biol Phys 37(2):289–295
8. Mohiuddin M, Regine WF, John WJ, Hagihara PF, McGrath PC, Kenady DE, Marks G (2000) Preoperative chemoradiation in fixed istal rectal cancer: dose time factors for pathological complete response. Int J Radiat Oncol Biol Phys 46:883–888
9. Grann A, Feng C, Wong D, Saltz L, Paty PP, Guillem JG, Cohen AM, Minsky BD (2001) Preoperative combined modality therapy for clinically resectable uT3 rectal adenocarcinoma. Int J Radiat Oncol Biol Phys 49:987–995
10. Bosset JF, Collette L, Calais G, Mineur L, Maingon P, Radosevic-Jelic L, Daban A, Bardet E, Beny A, Ollier JC, EORTC Radiotherapy Group Trial 22921 (2006) Chemotherapy with preoperative radio-therapy in rectal cancer. N Engl J Med 355(11):1114–1123 11. Gerard JP, Conroy T, Bonnetain F, Bouché O, Chapet O,
Closon-Dejardin MT, Untereiner M, Leduc B, Francois E, Maurel J, Seitz JF, Buecher B, Mackiewicz R, Ducreux M, Bedenne L (2006) Preoperative radiotherapy with or without concurrent fluorouracil and leucovorin in T3-4 rectal cancers: results of FFCD 9203. J Clin Oncol 24:4620–4625
12. Kim JS, Kim JS, Cho MJ, Yoon WH, Song KS (2006) Comparison of the efficacy of oral capecitabine versus bolus 5-FU in preoper-ative radiotherapy of locally advanced rectal cancer. J Korean Med Sci 21:52–57
13. Yerushalmi R, Idelevich E, Dror Y, Stemmer SM, Figer A, Sulkes A, Brenner B, Loven D, Dreznik Z, Nudelman I, Shani A, Fenig E (2006) Preoperative chemoradiation in rectal cancer: retrospective comparison between capecitabine and continuous infusion of 5-fluorouracil. J Surg Oncol 93(7):529–533
14. Das P, Lin EH, Bhatia S, Skibber JM, Rodriguez-Bigas MA, Feig BW, Chang GJ, Hoff PM, Eng C, Wolff RA, Delclos ME, Krishnan S, Janjan NA, Crane CH (2006) Preoperative chemo-radiotherapy with capecitabine versus protracted infusion 5-fluorouracil for rectal cancer: a matched-pair analysis. Int J Radiat Oncol Biol Phys 66(5):1378–1383
15. De Paoli A, Chiara S, Luppi G, Friso ML, Beretta GD, Del Prete S, Pasetto L, Santantonio M, Sarti E, Mantello G, Innocente R,
Frustaci S, Corvò R, Rosso R (2006) Capecitabine in combination with preopera- tive radiation therapy in locally advanced, resect-able, rectal cancer: a multicentric phase II study. Ann Oncol 17 (2):246–251
16. Desai SP, El-Rayes BF, Ben-Josef E, Greenson JK, Knol JA, Huang EH, Griffith KA, Philip PA, McGinn CJ, Zalupski MM (2007) A phase II study of preoperative capecitabine and radiation therapy in patients with rectal cancer. Am J Clin Oncol 30(4):340– 345
17. Craven I, Crellin A, Cooper R, Melcher A, Byrne P, Sebag-Montefiore D (2007) Preoperative radiotherapy combined with 5 days per week capecitabine chemotherapy in locally advanced rectal cancer. Br J Cancer 97(10):1333–1337
18. Dunst J, Debus J, Rudat V, Wulf J, Budach W, Hoelscher T, Reese T, Mose S, Roedel C, Zuehlke H, Hinke A (2008) Neoadjuvant capecitabine combined with standard radiotherapy in patients with locally advanced rectal cancer. Strahlenther Onkol 184:450–456 19. Elwanis MA, Maximous DW, Elsayed MI, Mikhail NN (2009)
Surgical treatment for locally advanced lower third rectal cancer after neoadjuvant chemoradiation with capecitabine: prospective phase II trial. World J Surg Oncol 7:52
20. Marsh RW, George TJ, Siddiqui T, Mendenhall WM, Zlotecki RA, Grobmyer S, Hochwald S, Chang M, Larson B, King J (2010) A Phase II trial of neoadjuvant capecitabine combined with hyper-fractionated accelerated radiation therapy in locally advanced rec-tal cancer. Am J Clin Oncol 33(3):251–256
21. Chan AK, Wong AO, Jenken DA (2010) Preoperative capecitabine and pelvic radiation in locally advanced rectal cancer—is it equiv-alent to 5-FU infusion plus leukovorin and radiotherapy? Int J Radiat Oncol Biol Phys 76:1413–1419
22. Hofheinz R, Wenz F, Post S, Matzdorff A, Laechelt S, Mueller L, Link H, Moehler M, Burkholder I, Hochhaus A (2009) Capecita-bine versus 5-fluorouracil -based (neo-)adjuvant chemoradiother-apy for locally advanced rectal cancer: safety results of a randomized, phase III trial. J Clin Oncol 27(15s), 2009 (suppl; abstr 4014), 2009 ASCO Annual Meeting
23. Hoff PM, Ansari R, Batist G, Cox J, Kocha W, Kuperminc M, Maroun J, Walde D, Weaver C, Harrison E, Burger HU, Osterwalder B, Wong AO, Wong R (2001) Comparison of oral capecitabine versus intra-venous fluorouracil plus leucovorin as first-line treatment in 605 patients with metastatic colorectal cancer: results of a randomized phase III study. J Clin Oncol 19(8):2282–2292
24. Reerink O, Verschueren RCJ, Szabo BG, Hospers GAP, Mulder NH (2003) A favourable pathological stage after neoadjuvant radioche-motherapy in patients with initially irresectable rectal cancer corre-lates with a favourable prognosis. Eur J Cancer 39:192–195 25. Rullier A, Laurent C, Capdepont M, Vendrely V, Bioulac-Sage P,
Rullier E (2010) Impact of tumor response on survival after radio-chemotherapy in locally advanced rectal carcinoma. Am J Surg Pathol 34:562–568
26. Scheithauer W, McKendrick J, Begbie S, Borner M, Burns WI, Burris HA, Cassidy J, Jodrell D, Koralewski P, Levine EL, Marschner N, Maroun J, Garcia-Alfonso P, Tujakowski J, Van Hazel G, Wong A, Zaluski J, Twelves C, X-ACT Study Group (2003) Oral capecitabine as an alternative to i.v. 5-fluorouracil-based adjuvant therapy for colon cancer: safety results of a ran-domized, phase III trial. Ann Oncol 14:1735–1743
27. Nathanson DR, Espat NJ, Nash GM, D'Alessio M, Thaler H, Minsky BD, Enker W, Wong D, Guillem J, Cohen A, Paty PB (2003) Evaluation of preoperative and postoperative radiotherapy on long-term functional results of straight coloanal anastomosis. Dis Colon Rectum 46(7):888–894
28. Huh JW, Park YA, Sohn SK (2007) A diverting stoma is not necessary when performing a handsewn coloanal anastomosis for lower rectal cancer. Dis Colon Rectum 50:1040–1046