行政院國家科學委員會補助專題研究計畫成果報告
※※※※※※※※※※※※※※※※※※※※※※※※※※
※
※
※
調控脊髓基因對於針刺鎮痛之影響
※
※
※
※※※※※※※※※※※※※※※※※※※※※※※※※※
計畫類別:■個別型計畫
□整合型計畫
計畫編號:NSC 90 - 2314 - B - 002 - 423
執行期間:
90 年
8 月
1
日至
91 年
7
月
31
日
計畫主持人:
孫
維
仁
共同主持人:
計畫參與人員:
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
執行單位:國立台大醫學院 麻醉科
中
華
民
國
91 年 10 月 22 日
Abstract
In the present study, we examined the effects of preoperative electroacupuncture (EA) at classical bilateral acupuncture points (Zusanli, also known as ST-36) on postoperative pain and opioid-related side effects. One hundred healthy consenting women undergoing lower abdominal surgery were randomly assigned to four treatment regimens: Group I (n = 25), control; Group II (n = 25), sham-EA (needle insertion without electrical stimulation); Group III (n = 25), low-EA (2 Hz of electrical stimulation); and Group IV (n = 25), high-EA (100 Hz of electrical stimulation). Electroacupuncture groups received needle insertion with or without electrical stimulation 20 minutes prior to anesthesia. All patients received patient-controlled analgesia (PCA) of morphine postoperation. Postoperative pain was evaluated by recording (1) the time of the first required analgesic, (2) the number of PCA demands, (3) the total amount of morphine required by PCA, and (4) patients’ VAS pain score. We found that the time of first analgesic requested was 10 min, 18 min, 28 min, and 28 min in the control, sham-, low-, and high-EA groups, respectively. During the first 24 h, the total amount of morphine required was decreased by 21%, 43% and 61% in the sham-, low- and high-EA groups, respectively. The incidence of nausea and dizziness during the
first 24 h after surgery was significantly reduced in both the low-EA and high-EA groups compared with the control and sham-EA groups. We also found that sham-EA exerts a beneficial effect with respect to its pain relieving quality but not the side effect profiles. Our findings demonstrates that preoperative treatment with low-EA and high-EA can reduce postoperative analgesic requirements and associated side effects in patients undergoing lower abdominal surgery.
Keywords:
Electroacupuncture; Postoperative pain; Patient-controlled analgesia; Visual analogue scale
1. Introduction
Acupuncture, the practice of inserting needles into the skin and deeper tissues along “meridians” to balance flows of bodily "energy” or “Xi”, has been widely used in China since 2500 BC (Wu, 1996). Though its role in various medical conditions remains largely controversial, recent evidence supports the worldwide use of acupuncture to relieve pain in clinical practice. Numerous studies have found that acupuncture activates multiple neurophysiological interactions, and thereby decreases nociceptive responses in animals receiving painful thermal, chemical, and electrical stimulations (reviewed by Mayer,
2000). Manual or electrical stimulation through needles induces a particular pattern of afferent activity in peripheral nerves, mainly Aβ, Aδ and possibly C-fibers. This excitation leads to activation of the endogenous pain inhibition system through multiple neuronal pathways (Basbaum and Field, 1984; Kaufman et al., 1984; Andersson and Lundeberg, 1995). One of the main consequences of acupuncture is the release of endogenous opioids, including β-endorphins, enkephalins, dynorphins, and endomorphins-1 (Promeranz and Chiu, 1976; Sjolund et al., 1977; He, 1987; Wang et al., 1990a; Wang et al., 1990b; Han et al., 1999), as well as non-opioid substances such as serotonin, norepinephrine, and possibly GABA (Cheng and Pomeranz, 1981; Pomeranz, 1996; Sandkuehler et al., 1997). In addition, animal and human studies have shown that diffuse noxious inhibitory controls (DNIC) may also be involved in underlying acupuncture mechanisms (Bing et al., 1990). DNICs are part of the biological pain control system whereby a spatially remote noxious conditioning stimulus can reduce the response to a subsequent noxious stimulus elsewhere (Le Bars et al., 1979; Le Bars et al., 1992).
Although acupuncture is widely used in humans, its applicability in various painful disorders is challenged due to its weak and variable analgesic effect, as well as by its concomitant placebo or hypnotic effect (Moret et al., 1991; Amanzio and Benedetti, 1999), or by the patient’s psychological expectation
(Thomas and Lundeberg, 1996). Studies have demonstrated that acupuncture is especially, though not exclusively, effective in myofascial pain (Melzack et al., 1977; Lewit, 1979), renal colic (Lee et al., 1992), angina pectoris (Richter et al., 1991), osteoarthritis of the knees (Christensen et al., 1992), tension headache (Vincent, 1990), and fibromyalgia (Deluze et al., 1992).
To date, few studies have investigated acupuncture’s effect on postoperative pain, and they have shown conflicting results (Galloway et al., 1984; Martelete and Fiori, 1985; Christensen et al., 1989; Christensen et al., 1993). A critical difference among these studies was the stimulation modality and the lack of sham control. None of these studies examined the effect of pre-stimulus acupuncture on postoperative pain and concomitant side effect profiles. Since acupoint stimulation has been widely used and proven to be effective in relieving profound nausea and vomiting caused by motion sickness and chemotherapy, electroacupuncture (EA) per se could potentially serve as an adjuvant for relieving opioid-related side effects during the postoperative period (Lee and Done, 1999). The present study was thus undertaken to evaluate whether preoperative application of different frequencies of EA stimulation can be effective in relieving postoperative pain, as well as postoperative opioid-related side effects.
2.1. Subjects
The study protocol was approved by the Hospital Research Committee. A total of 100 female patients were enrolled. After providing written informed consent, patients of ASA physical status I-II (American Society of Anesthesiology nomenclature) who were scheduled for abdominal hysterectomy were randomly divided into 4 groups of 25 each by a computer-generated randomization sequence: Group I received neither needle insertion nor electric stimulation (control); Group II received needle insertion but without electrical stimulation (sham EA); Group III received needle insertion with of 2 Hz stimulation (low-EA); and Group IV received needle insertion with 100 Hz stimulation (high-EA). The use of the PCA device (Lifecare PCA Plus II Infusor, Abbott Laboratories, IL) and the administration of EA were explained to each patient at the time of their preoperative visits. Patients with a history of opioid abuse, or significant cardiovascular, pulmonary, renal, hepatic or neurological disease were excluded.
2.2. Acupuncture
The acupuncture loci used were the bilateral Zusanli (also known as ST-36), which are located at one finger breadth below and anterior to the tibial tuberosity. We chose Zusanli because this point is traditionally considered to possess the most therapeutic effect on the lower abdomen. Two 30 gauge stainless steel acupuncture needles were inserted at the Zusanli point on both legs, with a distance
between needles of approximately 3 cm, i.e., one needle serving as the positive pole, and the other as the negative pole to allow for electrical stimulation of the selected point. After the patient reported the sensation of "De-Xi", a term used in acupuncture to describe a feeling of “heaviness” in the area surrounding the insertion locus, an electric current was delivered by a Functions Electrical Stimulator (Trio 300, I. T. O., Japan). Subjects and electrical equipment were placed such that subjects were unable to see any specifics regarding the type of current administered, and technicians maintained a normal persona to ensure that patients remained unaware of their grouping category. Electricity was generated as an output of constant current of 0.5 mA, 1 msec square pulse, at a maximal tolerable intensity (a strong, but not painful sensation as reported by the patient), and at 2 or 100 Hz depending on the group assignment. Sham EA included needle insertion with the indicator light on but with no actual current. All patients were subject to the respective treatment modality for 20 minutes before the induction of anesthesia.
2.3. Anesthesia and postoperative care
After removal of the needles, anesthesia was induced with i.v. thiopental 5 mg/kg and succinylcholine 2 mg/kg for tracheal intubation. Isoflurane in nitrous oxide 60% with oxygen 40% and an intermittent dose of atracurium were used for anesthesia maintenance without the use of opioids. Following surgery, all
patients were transported to the recovery room. The time interval of the patient’s first request for pain medication was recorded (either pethidine 1 mg/kg i.m. during the first hour, which was restricted to a single dose, or as recorded by PCA when no request was made during the first hour). At one hour post operation, the PCA system was connected to the patient. The PCA device was programmed to intravenously deliver 2 mg morphine as “on demand” doses with a minimum lockout interval of 10 min during the following 23 h.
2.4. Efficacy measures
As soon as the patient complained of initial pain, the first PCA dose was provided. The average pain using the 100 mm visual analog scale (VAS) were recorded at 30 min, and at 1, 1.5, 2, 4, 8, 16 and 24 h by an observer who had no knowledge of the patient’s group assignment. The number of PCA demands, including those made during lockout intervals, was recorded by a printout attachment for 24 h. No other analgesics were administered during the PCA control period. Heart rate, blood pressure, and SpO2 were recorded by a pulse oximeter every
30 min for the first 2 h and at 4 h intervals thereafter. At the end of 24 h test period, patients were asked if they had experienced any opioid-related adverse effects, including nausea, vomiting, dizziness, or pruritus, and their responses were recorded.
2.5. Data analysis
This sample size permitted the detection of an inter-group mean difference using a type I
error of 0.05 and a type II error of 0.2 (i.e.,
power=0.8). Patient’s age, weight, duration of anesthesia and duration of surgery, VAS score, PCA demands and doses delivered were analyzed with one-way ANOVA followed by Bonferroni post hoc test. Incidence of side effects was analyzed using the chi-square test. A P value of less than 0.05 was considered
statistically significant.
Results
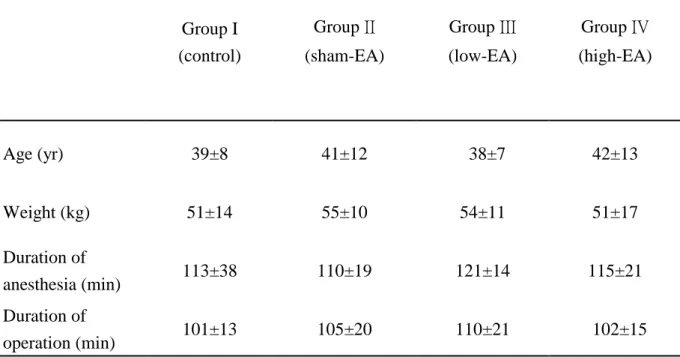
The demographic data listed in Table 1 shows no significant difference among the four groups. All enrolled patients completed the study period with no withdrawals. The time interval of the first request for analgesic was 10.6 min, 18.0 min, 27.9 min, and 28.1 min for the control, sham-EA, low -EA and high-EA, respectively. These intervals were all significantly longer than the control group, and the time intervals of both low- and high-EA groups were longer than the sham-EA group (Table 2). The number of PCA demands during the 24 h test period was significantly less in the high-EA (7.9±5.9) and low-EA (11.7±7.1) groups compared to that of the control (20.5±9.2) and the sham-EA (16.1±7.4) groups, as shown in Table 2. There were also highly significant differences in morphine delivered among the four groups, with the lowest dose used in the high-EA group (Table 2). Pain scores were not different among the four groups
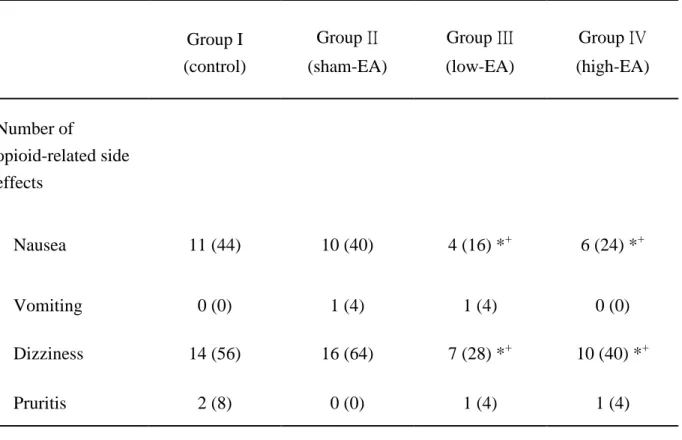
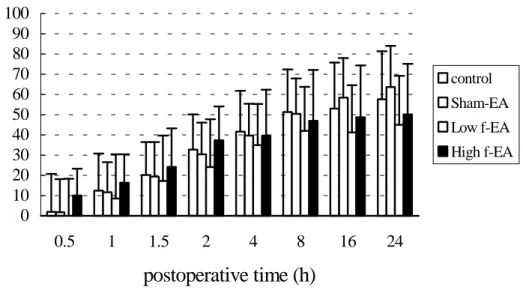
(Fig. 1); however, compared to the control group, the total amount of morphine required during the 24 h test period was reduced by 21%, 43% and 61% in the sham-EA, low-EA and high-EA groups, respectively. The incidence of nausea and dizziness was significantly lower in both the low- and high-EA groups compared to the other two groups (Table 3). No patient demonstrated any respiratory depression (respiratory rate < 10 min or SpO2 < 90%).
Discussion
We found that sham-, low-, and high-EA treatments prior to lower abdominal surgery significantly reduced the postoperative PCA morphine requirement, and that low- and high-EA decreased opioid-induced nausea and dizziness throughout the first postoperative day. We also found that high frequency EA stimulation produced better effects than low frequency stimulation. Our results were consistent with several other animal and clinical studies that have reported that EA stimulation improved analgesia during the acute phase of post-traumatic pain. EA has been widely used and well documented in tooth extraction (Ekblom et al., 1991; Ernst and Pittler, 1998) and in oocyte aspiration (Stener-Victorin et al., 1999). EA-induced analgesia after major surgery, however, remains controversial. Christensen et al. (1993) demonstrated that patients receiving EA before and during hysterectomy exhibited no reduction in their postoperative analgesic requirement or
pain ratings. The possible reasons for this discrepancy are multiple. Christensen et al. selected an array of acupoints; the needles were inserted after induction of anesthesia and remained in place throughout the surgical procedure; and in addition to EA, patients received a relatively high dose of pethidine for induction and maintenance of anesthesia. Any benefits of EA that may have been present were likely masked by the high level of pethidine used. This variation in methods vs. those used in the present study may explain the vastly different results reported. Wang et al. (1997) found significantly greater pain relief after lower abdominal surgery among patients receiving transcutaneous electrical nerve stimulation (TENS) applied at Hogu (LI-4) during the postoperative period. Wang’s study showed that both high- and low-frequency TENS reduced i.v. PCA hydromorphone requirement by 65% and 34%, respectively. Similar results were obtained in our study whereby the total number of PCA demands and the opioid analgesic dose requirements were markedly decreased in both high- and low-frequency EA groups. These findings imply that both EA and TENS can produce adequate postoperative pain relief, even though their underlying mechanisms are likely dissimilar.
In the present study, EA-induced analgesic effects between 2 Hz and 100 Hz were compared on the basis that low frequency (2 Hz) and high frequency (100 Hz) presumably
induce a differential release of enkephalins and dynorphins in both animals and humans (Chen and Han, 1992; Ulett et al., 1998). It has also been shown that the analgesic effect produced by low frequency stimulation is naloxone-reversible, while high frequency stimulation is not (Lee and Beitz, 1992; Guo et al., 1996). These results strongly suggest a distinct neuronal sensitization and characteristic spatial process in the central nervous system between these two frequencies. The primary difference between 2 Hz and 100 Hz stimulations is the number of electric pulses providing during a given period of time. It is estimated that patients in the high frequency group received a total of 20 times the number of electrical pulses than the low frequency group during the 20 min test period. Previous study suggested that the inhibitory magnitude and duration of neuronal response to painful C-fiber activation is a function of the number of preceding conditioning stimuli (Ness and Gebhart, 1991). This previous speculation is consistent with the results observed in our study.
The results of the present study also demonstrated that the opioid-sparing effect of EA is dependent on the frequency of the electrical stimulation. The morphine requirement after high frequency EA was decreased by 31% compared with the low EA group during the first 24 hours postoperation. This opioid-sparing effect not only results in a decrease in the incidence of nausea and
dizziness after surgery, but it may also increase the tolerability and availability of adequate analgesic effect among those who are susceptible to morphine overdose, e.g.,
debilitated or older patients. Furthermore, acupuncture per se has been shown to reduce
the incidence of nausea through its direct antiemetic effect. Several studies have shown that acupuncture can decrease postoperative nausea and vomiting, in addition to reducing postoperative pain (Lee and Done, 1999).
In the present study, we deliberately did not attempt to influence subjects’ expectation regarding the effectiveness of EA. However, it is important to keep in mind that neurophysiological and humoral events are related to psychological factors. Undoubtedly, sensory stimulation and particularly acupuncture has the potential to produce strong placebo effects. For example, while sham needle insertion showed no effect on opioid-related side effects, it did exert a moderate pain relieving effect. Indeed, acupuncture works by stimulating endogenous opioids and so, it appears, does the placebo effect (Amanzio and Benedetti 1999). To achieve optimal acupuncture therapy, physiological and psychological factors must interact in synergy, utilizing their respective endogenous mechanisms efficiently (Thomas et al., 1996). By utilizing two control groups in our study design, including PCA only and sham EA groups, we were able to very clearly distinguish between the purely placebo
elements involved vs. clear evidence of physiological effects.
In the present study we also demonstrated that preoperative application of 20 min EA, whether high or low frequency, effectively reduced the 24 hour postoperative morphine requirement. The concept of preemptive analgesia through the prevention of intense nociceptor activation and suppression of the subsequent hyperalgesic state has potentially dramatic implications for postoperative analgesia (Woolf and Chong, 1993; Sun et al., 1996). In animals, pretreatment with short-acting opioids or NMDA antagonists has been shown to inhibit spinal dorsal horn sensitization and nocifensive behaviors (Yamamoto and Yaksh, 1992). However, results reported from human studies involving preemptive analgesia in surgical situations are relatively less impressive than results shown in animal studies utilizing the same treatment schemes (Cousins et al., 2000). EA-produced analgesia generally lasts for up to two hours (Christensen et al., 1989; Ulett et al., 1998). Therefore, high- or low- frequency stimulation before surgical incision can be regarded as an alternative to conventional methods as a prestimulus analgesic modality. Whether EA is indeed useful as a preemptive analgesia requires further study that will require two additional treatment groups: one receiving both pre- and post-operative EA, and another groups receiving postoperative EA alone.
In conclusion, we found that preoperative
electroacupuncture is an adequate adjunct to PCA. Both high- and low-frequency electrical stimulation reduced the postoperative analgesic requirement. We found that high frequency electrical stimulation provided the best results. In addition, the use of EA also resulted in a decrease in the incidence of opioid-related side effects after lower abdominal surgery. Together, our findings demonstrate that further studies are warranted regarding the efficacy of EA in both managing pain and in treating opioid-related symptoms.
References
Amanzio M, Benedetti F.
Neuropharmacological dissection of placebo analgesia: expectation-activated opioid systems versus conditioning-activated specific subsystems. J Neurosci 1999;19:484-494.
Andersson S, Lundeberg T. Acupuncture - from empiricism to science: functional background to acupuncture effects in pain and disease. Med Hypotheses 1995; 45:271-281. Basbaum AI, Field HL. Endogenous pain
control systems: brainstem spinal pathways and endogenous circuitry. Ann Rev Neurosci 1984;7:309-338.
Bing Z, Villanueva L, Le Bars D. Acupuncture and diffuse noxious inhibitory controls: naloxone-reversible depression of activities of trigeminal convergent neurons. Neurosci 1990;37:809-818.
mechanism of electroacupuncture analgesia. Brain Res 1981; 215: 77-92.
Chen XH, Han JS. Analgesia induced by
electroacupuncture of different frequencies is mediated by different types of opioid
receptors: another cross-tolerance study. Behav Brain Res. 1992;47:143-149. Christensen BV, Juhl IU, Vilbeck H, Bulow
HH, Dreijer NC, Rasmunsen HF. Acupuncture treatment of severe knee osteoarthritis: a long-term study. Acta Anaesthesiol Scand 1992;36:519-525. Christensen PA, Noreng M, Andersen PE,
Nielsen JW. Electroacupuncture and postoperative pain. Br J Anaesth 1989; 62: 258-262.
Christensen PA, Rotne M, Vedelsdal R, Jensen RH, Jacobsen K, Husted C.
Electroacupuncture in anaesthesia for hysterectomy. Brit J Anaesth
1993;71:835-8.
Cousins MJ, Power I, Smith G. 1996 Labat lecture: pain--a persistent problem. Region Anesth Pain Med 2000;25:6-21.
Deluze CH, Bosia L, Zirbs A, Chantraine A, Vischer ThL. Electroacupuncture in fibromyalgia: results of a controlled trial. BMJ 1992;305:1249-1252.
Ekblom A, Hansson P, Thomsson M, Thomas M. Increased postoperative pain and consumption of analgesics following acupuncture. Pain 1991;44:241-7. Ernst E, Pittler MH. The effectiveness of
acupuncture in treating acute dental pain: a
systemic review. Br Dent J 1998;184:443-447.
Galloway DJ, Boyle P, Burns HJ, Davidson PM, George WD. A clinical assessment of
electroanalgesia following abdominal operations. Surg Gynecol Obstet 1984; 159: 453-456.
Gan TJ, Ginsberg B, Glass PS, Fortney J,
Jhaveri R, Perno R. Opioid-sparing effects of a low-dose infusion of naloxone in
patient-administered morphine sulfate. Anesthesiology. 1997;87:1075-81.
Guo HF, Tian J, Wang X, Fang Y, Hou Y, Han J. Brain substrates activated by
electroacupuncture of different frequencies (I): comparative study on the expression of oncogene c-fos and genes coding for three opioid peptides. Mol Brain Res
1996;43:157-166.
Han Z, Jiang YH, Wan Y, Wanh Y, Chang JK, Han JS. Endomorphine-1 mediates 2 Hz but not 100 Hz electroacupucnture analgesia in the rat. Neurosci Lett 1999;274:75-78. He LF. Involvement of endogenous opioid
peptides in acupuncture analgesia. Pain 1987;31:99-121.
Kaufman MP, Waldrop TG, Rybycki KJ, Ordway GA, Mitchell JH. Effects of static and rhythmic twitch contractions on the discharge of group III and IV muscle afferents. Cardiovasc Rec 1984;19:663-668. Le Bars D, Dickensson AN, Besson JM.
Diffuse noxious inhibitory controls (DNIC). II. Lack of effects on non-convergent
neurons, supraspinal involvement and theoretical implications. Pain
1979;6:305-327.
Le Bars D, Willer JC, De Broucker T.
Morphine blocks descending pain inhibitory controls in humans. Pain 1992;48:13-20. Lee A, Done ML. The use of
nonpharmacologic techniques to prevent postoperative nausea and vomiting: a meta-analysis. Anesth Analg.
1999;88:1362-1329.
Lee JH, Beitz AJ. Electroacupuncture modifies the expression of c-fos in the spinal cord induced by noxious stimulation. Brain Res 1992;577;80-91.
Lee YH, Lee WC, Chen MT, Huang JK, Chung C, Chang LS. Acupuncture in the treatment of renal colic. J Urol 1992;147:16-18. Lewit K. The needle effect in relief of
myofascial pain. Pain 1979;6:83-90.
Lewith GT. How effective is acupuncture in the management of pain? J R Coll Gen Pract 1984;34:275-278.
Luc Frenette. The acute pain service. Critical care clinics 1999;15:143-150.
Martelete M, Fiori AM. Comparative study of the analgesic effect of transcutaneous nerve stimulation (TNS); electroacupuncture (EA) and meperidine in the treatment of
postoperative pain. Acupunct Electrother Res 1985; 10:183-93.
Mayer DJ. Biological mechanisms of acupuncture. Prog Brain Res 2000;122:457-477.
Melzack R Stillwell DM, Fox EJ. Trigger points and acupuncture points for pain: correlations and implications. Pain 1977;3:3-23.
Moret V, Forster A, Laverrière MC, Lambert H, Gaillard RC, Bourgeois P, Haynal A,
Gemperle M, Buchser E. Mechanism of analgesia induced by hypnosis and acupuncture: is there a difference? 1991;45:135-140.
Ness TJ, Gebhart GF. Interactions between visceral and cutaneous nociception in the rat. II Noxious visceral stimuli inhibit cutaneous nociceptive neurons and reflexs. J
Neurophysiol 1991;66:29-39.
Pomeranz B, Chiu D. Naloxone blockade of acupuncture analgesia: endorphin implicated. Life Sci 1976; 19: 1757-1762.
Pomeranz B. Scientific research into acupuncture for the relief of pain. J Alt Complement Med 1996;2:53-60.
Richter A, Herlitz J, Hjalmarson A. Effect of acupuncture in patients with angina pectoris. Eur Heart J 1991;12:175-178.
Sandkuehler J, Chen JG, Cheng G, Randic M. Low frequency stimulation of afferent Aδ fibers induces long-term depression of primary afferent synapses with substantia gelatinosa neurons in the rat. J Neurosci 1997;17:6483-6491.
Siddik SM, Aouad MT, Jalbout MI, Rizk LB, Kamar GH, Baraka AS. Diclofenac and/or propacetamol for postoperative pain management after cesarean delivery in
patients receiving patient controlled analgesia morphine. Reg Anesth Pain Med 2001;26:310-5.
Sjolund B, Terenius L, Eriksson M. Increased cerebrospinal fluid levels of endorphins after electro-acupuncture. Acta Physiol Scand 1977; 100: 382-384.
Stener-Victorin E, Waldenstrom U, Nilsson L, Wikland M, Janson PO. A prospective randomized study of electroacupuncture versus alfentanil as anaesthesia during oocyte aspiration in in-vitro fertilization. Hum Repro 1999;14:2480-2484.
Sun WZ, Shyu BC, Shieh JY. Nitrous oxide or halothane, or both, fail to suppress c-fos expression in the rat spinal cord dorsal horn neurons after subcutaneous formalin. Br J Anaesth 1996;76:99-105.
Thomas M, Lundeberg T. Does acupuncture work? Pain clinic. Updates 1996;4:1-4. Tramer MR, Walder B. Efficacy and adverse
effects of prophylactic antiemetics during patient-controlled analgesia therapy: a
quantitative systematic review. Anesth Analg 1999;88:1354-61.
Ulett GA, Han S, Han JS. Electroacupuncture: Mechanisms and clinical application. Biol Psychiatry 1998;44:129-138.
Vincent CA. The treatment of tension headache by acupuncture: a controlled single case design with time series analysis. J Psychosom Res 1990;34:553-561. Wang B, Tang J, White PF, Naruse R,
Sloninsky A, Kariger R, Gold J, Wender RH.
Effect of the intensity of transcutaneous acupoint electrical stimulation on the
postoperative analgesic requirement. Anesth Analg. 1997;85:406-13.
Wang Q, Mao L, Han J. The arcuate nucleus of hypothalamus mediates low but not high frequency electroacupuncture analgesia in rats. Brain Res 1990a;513:60-66.
Wang Q, Mao L, Han J. The role of periaqueductal gray in mediation of
analgesia produced by different frequencies of electroacupuncture stimulation in rats. Int J Neurosci 1990b;53:167-172.
Woodhouse A, Mather LE. Nausea and Vomiting in the postoperative
patient-controlled analgesia environment. Anaesthesia 1997a;52:770-775.
Woodhouse A, Mather LE. The influence of age upon opioid analgesic use in the patient-controlled analgesia (PCA)
enviroment. Anaesthesia 1997b;52:949-955. Woolf CJ, Chong MS. Preemptive analgesia
-Treating postoperative pain by preventing the establishment of central sensitization. Anesth Analg 1993;77:362-79.
Wu JN. A short history of acupuncture. J Altern Complement Med 1996;2:19-21.
Yamamoto T, Yaksh TL. Comparison of the antinociceptive effects of pre- and
posttreatment with intrathecal morphine and MK801, an NMDA antagonist, on the formalin test in the rat. Anesthesiology. 1992;77:757-63.
Table 1. Demographic data for each of the four treatment groups. Group I (control) Group II (sham-EA) Group III (low-EA) Group IV (high-EA) Age (yr) 39±8 41±12 38±7 42±13 Weight (kg) 51±14 55±10 54±11 51±17 Duration of anesthesia (min) 113±38 110±19 121±14 115±21 Duration of operation (min) 101±13 105±20 110±21 102±15
Table 2. Postoperative analgesic requirements in each treatment group. Group I (control) Group II (sham-EA) Group III (low-EA) Group IV (high-EA)
Time for the first dose of pethidine after operation (min)
10.6 ± 5.9 18.0 ± 7.9* 27.9 ± 12.3**§ 28.1 ± 13.8** §
PCA demands in the first 24h 1 - 8 h 9.0 ± 3.6 7.0 ± 3.6* 5.1 ± 4.0**+ 3.3 ± 3.2**++§ 8 - 16 h 8.2 ± 5.3 5.8 ± 3.8 4.0 ± 2.6**+ 2.8 ± 2.1**++§ 16 - 24 h 3.2 ± 2.4 3.3 ± 2.1 2.6 ± 2.1 1.8 ± 1.6**++ Total in 24h 20.5 ± 9.2 16.1 ± 7.4 * 11.7 ± 7.1**+ 7.9 ± 5.9**++§ Morphine delivered (mg) 1 - 8 h 16.1 ± 7.1 12.8 ± 6.6* 9.2 ± 7.1**+ 6.1 ± 5.9 **++§ 8 - 16 h 15.5 ± 9.4 10.8 ± 7.7 * 7.6 ± 5.4**+ 5.4 ± 3.8 **++§ 16 - 24 h 6.5 ± 4.8 6.6 ± 4.1 5.0 ± 4.2 3.5 ± 3.2**++ Total in 24h 38.1 ± 16.0 30.2 ± 14.4* 21.8± 14.7**+ 15.0 ± 10.7**++§
Values are mean ± S.D. (n=25) *p<0.05, **p<0.01 versus Group I.
+
p<0.05, ++p<0.01 versus Group II.
§
Table 3. Postoperative side effects in the four treatment groups. Group I (control) Group II (sham-EA) Group III (low-EA) Group IV (high-EA) Number of opioid-related side effects Nausea 11 (44) 10 (40) 4 (16) *+ 6 (24) *+ Vomiting 0 (0) 1 (4) 1 (4) 0 (0) Dizziness 14 (56) 16 (64) 7 (28) *+ 10 (40) *+ Pruritis 2 (8) 0 (0) 1 (4) 1 (4)
Values are mean (%) *p<0.05, versus Group I.
+
0 10 20 30 40 50 60 70 80 90 100 0.5 1 1.5 2 4 8 16 24
postoperative time (h)
VAS
control Sham-EA Low f-EA High f-EA Figur e legendsFigure 1. Postoperative 24-h visual analogue scale (VAS, 0-100 mm) comparison. Open bars indicate control group; dotted bars, sham-EA; hatched bars, low EA; shaded bars, high EA.