Correlation of Tourette Syndrome and Allergic Disease:
Nationwide Population-Based Case-Control Study
Yu-Tzu Chang, MD,* Yu-Fen Li, PhD, MPH,† Chih-Hsin Muo, MS,‡ Shih-Chieh Chen, MD,§
Zheng-Nan Chin, MD,* Huang-Tsung Kuo, MD, PhD,* Hung-Chih Lin, MD,*
储
Fung-Chang Sung, PhD, MPH,†‡ Chang-Hai Tsai, MD, PhD,*¶ I-Ching Chou, MD*#
ABSTRACT: Objective:Linkage between allergy and increased immune response activation in Tourette syn-drome (TS) has been reported. We performed a matched case-control study to evaluate correlation between allergic diseases and TS. Methods: Data in this case-control study were from the Taiwan National Health Insurance Research Database. The sample comprised 845 2- to 18-year-old patients with newly diagnosed TS in 2003–2007 and 3378 controls frequency matched with cases on age, sex, and urbanization level. Uncon-ditional logistic regression estimated odds ratios (ORs) and 95% confidence intervals (CIs) of the association between allergic disease (e.g., allergic rhinitis, atopic dermatitis, asthma, and allergic conjunctivitis), the number of allergic comorbidities, and TS. Results: The majority (76.0%) of incident TS cases were boys; the 4 allergic diseases strongly correlated with higher risk of TS. In a model simultaneously considering all 4 allergic diseases, subjects with allergic rhinitis showed double the risk of TS (adjusted ORⴝ 2.18, 95%CI 1.83–2.59;
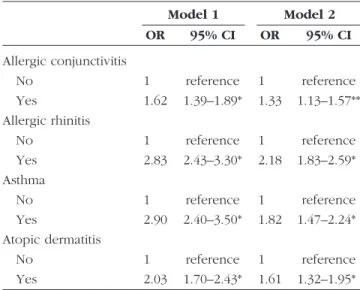
p <0.0001); adjusted ORs were 1.82, 1.61, and 1.33, respectively, for asthma (95% CI 1.47–2.24; p < 0.0001), dermatitis (95%CI 1.32–1.95; p < 0.0001), and allergic conjunctivitis (95% CI 1.13–1.57; p < 0.001). Risk increased with number of comorbidities (p < 0.0001); this association was positively modified by age (p < 0.0001). Conclusions: Our data showed significant correlation between allergic diseases and TS. Risk also increased with number of allergic comorbidities and with age. Further studies on the mechanism of neuro-immunology of TS are required.
(J Dev Behav Pediatr 32:000 –000, 2011) Index terms: Tourette syndrome, allergy, neuroimmunology.
T
ourette syndrome (TS) is a neuropsychiatric disorder characterized by the presence of involuntary motor and phonic tics that grow stronger and then become weaker. In this heterogeneous disorder, genetic, environmental, immunological, and hormonal factors interact to estab-lish vulnerability. Immune and nervous systems have delicate, complex, and dynamic interaction, both in healthy and diseased individuals.1 Mounting evidencesuggests that besides affording communication between immune cells, specific cytokines play a role in signaling
the brain to produce neurochemical, neuroendocrine, neuroimmune, and behavioral changes.2–5 Cytokines
may act as neuromodulators and immunomodulators;2
the signaling may be part of a generalized and compre-hensive mechanism to mobilize resources in the face of physical and/or psychological stress and to maintain homeostasis. On the clinical level, advances in cytokine research have helped us understand pathophysiology of medical conditions and identification of new treat-ments.6These developments are particularly relevant to
immune-related disorders such as infection, allergy, au-toimmune disease, and cancer. Neurobiological research has revealed several possible alternations; evidence points to immune dysregulation as involved in pathogen-esis of tic disorders.
Likewise, environmental factors triggering immune response have been proposed for a subgroup of patients with TS and pediatric-onset obssessive-compulsive disor-der (OCD). Possibility of such a link is partly based on similarity of TS to Sydenham chorea, which occurs after group A -hemolytic streptococcal infections.7– 8 In
brief, immunological research indicates that infections like pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections may induce or reinforce tics and associated features in susceptible in-dividuals, possibly via abnormal humoral immune
re-From the *Children’s Medical Center, China Medical University Hospital; †De-partment of Public Health, China Medical University, ‡Management Office for Health Data, China Medical University Hospital; §Division of Pediatric Immunol-ogy, Children’s Medical Center, China Medical University Hospital;储School of Chinese Medicine, College of Chinese Medicine, China Medical University; ¶De-partment of Healthcare Administration, Asia University; #Graduate Institute of Integrated Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan.
Received April 2010; accepted October 2010.
This study was supported partly by the National Science Council, Executive Yuan, Taiwan, Republic of China, grants NSC 95-2625-Z-039-002, NSC 96-2625-Z-039-003, and NSC 97-2625-M-039-003; China Medical University Hospital grant 1MS1; and Taiwan Department of Health Clinical Trial and Research Center for Excellence grant DOH99-TD-B-111-004.
Address for reprints: I-Ching Chou, MD, Children’s Medical Center, China Med-ical University Hospital, No. 2, Yuh-Der Road, North District, Taichung 40447, Taiwan; e-mail: [email protected].
Copyright © 2011 Lippincott Williams & Wilkins
Original Article 1 AQ: A AQ: J AQ: K AQ: L
sponse directed against self-tissue antigens.8 –14 Linkage
between group A -hemolytic streptococcal infections and onset or worsening of pediatric OCD, TS, and tic disorders has been corroborated by cross-sectional8 –10
and longitudinal11–12reports.
Association of allergies with TS has been described in literature.15–19Ho et al15cited patients who show clinical
evidence of allergy in the Multiple Allergens Simulta-neous Tests positive group (56.9%) of patients with TS as displaying a significant difference from controls. Preva-lence of allergy in patients with TS has proven signifi-cantly higher than in the general population. However, after comparing 247 patients with TS with selected con-trols, Comings and Comings20concluded that no
signif-icant difference in frequency of allergies between these groups existed.
To calculate association between allergy and TS, we hypothesize the role of allergy in TS and performed nationwide population-based case-control study to cor-relate rhinitis, asthma, atopic dermatitis, and conjuncti-vitis with TS.
MATERIALS AND METHODS
Study Subjects
We gleaned data from the National Health Research Institutes Dataset established in January 1996. The Na-tional Health Insurance program of Taiwan is an island-wide system established by the Bureau of National Health Insurance of the Department of Health. Imple-mented as of March 1995, it had a coverage rate of over 99% in 2007 (http://www.nhi.gov.tw). This dataset con-sisted of insurance claims by 10,000,000 individuals ran-domly selected among all insured individuals in 2005. These claims, retrospectively collected since 1996 and prospectively recorded up to 2007, contained basic de-mographic information on insured residents (sex, age, region, and so on), along with medical records (includ-ing inpatient and ambulatory visits). We used the Inter-national Classification of Disease, Ninth Revision (ICD-9) to define status of Tourette syndrome (TS) in individuals aged 2 to 18 years. We identified 845 incident cases as newly diagnosed patients with TS (ICD-9: 307.2) in 2003–2007. In each case, 4 controls were matched for age, sex, and urbanization level among children with no history of TS. Using 1:m case-control studies is to increase the power and to control possible confound-ing. As the statistical efficiency does not gain much when m ⬎4, we decide to conduct a 1:4 matched case-control study. Urbanization level was defined ac-cording to population density (persons/km2) for each
township and district (Department of Statistics, Ministry of the Interior, Executive Yuan of the Republic of China, http://sowf.moi.gov.tw/stat/year/list.htm). Number of matchable controls came out too short—3378 controls included in analysis. We identified the status of each subject’s allergic conjunctivitis (ICD-9: 372.05, 37.210, and 372.14), allergic rhinitis (ICD-9: 477), asthma (ICD-9: 493 and 494), and atopic dermatitis (ICD-9: 691) during
the study period. Cumulative effect of multiple allergic comorbidities was evaluated by the number of allergic comorbidities.
Statistical Analysis
Chi-square and t-tests rated the difference between case and control groups. The odds ratio (OR) and 95% confidence interval (CI) were estimated using uncondi-tional logistic regression with adjustment of confound-ers. The mutually adjusted model tested all 4 allergic diseases simultaneously, while adjusting for sex, age, and urbanization. Analyses were performed by SAS software version 9.1 (SAS Institute Inc., Carey, NC), and signifi-cance level was set at 0.05.
RESULTS
Among 845 incident cases diagnosed with Tourette syndrome (TS) in 2003–2007, the majority was boys (76.0%) with a mean age of 8.37 (SD⫽ 2.97) years (Table 1). Compared with matched controls, cases were more prone to allergic conjunctivitis (64.6% vs 53.0%), allergic rhinitis (58.1% vs 32.9%), asthma (26.0% vs 10.8%), and atopic dermatitis (26.6% vs 15.2%). Adjusted logistic re-gression analysis of TS and associated factors are pre-sented in Table 2. Model 1 refers to multivariate logistic regression of each comorbidity, adjusted for sex, age, and urbanization. Model 2 serves as a mutually adjusted model. Four allergic diseases positively correlated with risk of TS. In the model simultaneously considering all 4 allergic diseases, subjects with allergic rhinitis showed more than twice the risk of TS (adjusted odds ratio [OR]⫽ 2.18, 95% confidence interval [CI] 1.83–2.59; p⬍ 0.0001); adjusted ORs were 1.82, 1.61, and 1.33, respectively, for asthma (95% CI 1.47–2.24; p⬍ 0.0001), dermatitis (95% CI 1.32–1.95; p⬍ 0.0001), and allergic conjunctivitis (95% CI 1.13–1.57; p⬍ 0.001).
Individuals can simultaneously manifest several aller-gic comorbidities; we thus rated cumulative effect by counting allergic comorbidities each individual suffered, adjusted for age, sex, and urbanization level. Risk in-creased with number of comorbidities, exhibiting an OR of 1.74 (95% CI 1.62–1.87; p ⬍ 0.0001). However, cu-mulative effect was positively modified by age (p ⬍ 0.0001; Fig. 1). For individuals without indexed allergic diseases, TS risk decreased with age (adjusted OR ⫽ 0.96, 95% CI 0.92–1.01; p⫽ 0.08) but increased with age (adjusted OR⫽ 1.06, 95% CI 1.04–1.09 per year and per indexed allergic disease; p⬍ 0.0001) for individuals with indexed allergic diseases, especially among those with 3 or 4 allergies, as depicted in Figure 1. Relative to a 10-year-old patient without allergic diseases, a 15-year-10-year-old patient with allergic diseases displayed 40 times the risk.
DISCUSSION
The connection between the immune system and neu-ropsychiatric disease has become increasingly clear.20More
and more studies suggest immune abnormality as associ-ated with Tourette syndrome (TS): e.g., autoimmune
re-AQ: B T1, AQ:C T2, AQ:D F1
sponses, altered cytokine profiles, and correlations of in-flammatory mediators with symptom exacerbation. This study revealed people with allergic diseases like rhinitis, asthma, and conjunctivitis at risk for TS, which increased
with comorbidities and with age. Association between al-lergy and TS has been mentioned in previous studies. In 1999, Ho et al stated that 64% of their patients with TS proved atopic,20showing prevalence of allergy in patients
with TS definitely higher than in the mainstream
popula-Figure 1. A statistical graph representing the relative risk (in terms of odds ratio) for Tourette syndrome as age increases by the number of allergic diseases (p for interaction ⬍0.0001). The reference group is individuals with no allergic disease at a certain age.
Table 2. Associations Between Risk Factors and Tourette Syndrome, OR, and 95% CI Model 1 Model 2 OR 95% CI OR 95% CI Allergic conjunctivitis No 1 reference 1 reference Yes 1.62 1.39–1.89* 1.33 1.13–1.57** Allergic rhinitis No 1 reference 1 reference Yes 2.83 2.43–3.30* 2.18 1.83–2.59* Asthma No 1 reference 1 reference Yes 2.90 2.40–3.50* 1.82 1.47–2.24* Atopic dermatitis No 1 reference 1 reference Yes 2.03 1.70–2.43* 1.61 1.32–1.95*
OR, odds ratio; CI, confidence interval. Model 1: each comorbidity adjusted for sex, age, and urbanization; Model 2: mutually adjusted. *p⬍ 0.0001; **p⬍ 0.001.
Table 1. Comparisons in Sociodemographic Factors and Comorbidities Between Cases with Tourette Syndrome and Controls
Total (nⴝ 4223) Tourette Syndrome p
No (nⴝ 3378) Yes (nⴝ 845) Age (yr) .98 Mean 8.38 8.38 8.37 SD 2.96 2.96 2.97 Sex .99 Girls 1015 (24.0) 812 (24.0) 203 (24.0) Boys 3208 (76.0) 2566 (76.0) 642 (76.0) Urbanization .99 Mean 7063 7064 7060 SD 6094 6094 6097 Comorbidity Allergic conjunctivitis ⬍.0001 No 1887 (44.7) 1588 (47.0) 299 (35.4) Yes 2336 (55.3) 1790 (53.0) 546 (64.6) Allergic rhinitis ⬍.0001 No 2621 (62.1) 2267 (67.1) 354 (41.9) Yes 1602 (37.9) 1111 (32.9) 491 (58.1) Asthma ⬍.0001 No 3637 (86.1) 3012 (89.2) 625 (74.0) Yes 586 (13.9) 366 (10.8) 220 (26.0) Atopic dermatitis ⬍.0001 No 3486 (82.6) 2866 (84.8) 620 (73.4) Yes 737 (17.5) 512 (15.2) 225 (26.6)
Tourette syndrome⫽ International Classification of Diseases, Ninth Revision (ICD-9) code: 307.2; allergic conjunctivitis ⫽ ICD-9-code: 372.05, 372.10, and 372.14; allergic rhinitis⫽ ICD-9 code: 477; asthma ⫽ ICD-9 code: 493 and 494; atopic dermatitis ⫽ ICD-9 code: 691. Values are presented as n (%) unless otherwise indicated.
tion. Allergens in food may play a role in both allergic disease and TS, which may be alleviated by avoiding de-monstrable offending dietary factors. Evidence that certain foods could enhance production of a specific neurotrans-mitter has also been reported.1,21–23 By reviewing 3300
patients with TS, Bruun21stated that in his clinical
experi-ence, symptom exacerbation is often associated with sea-sonal allergic responses or ingestion of allergens in foods, as well as by medication used to treat allergies. Allergic diseases are more chronic in winter than in summer; in addition, these may improve during puberty. Course of these diseases is similar to tic disorders that grow stronger and then become weaker. Finegold16reported 4 patients
with TS showing higher serum IgE levels and positive skin test. He stated that symptoms of patients with TS may mimic allergies or combine with allergic illness. He sug-gested linkage between these 2 disorders. In 1986, Mandell reported 80% incidence of allergy in investigations of pa-tients with TS,23linking allergy and TS.
Allergic disease may lead to stress for patients. Psy-chosocial stress has emerged as a powerful predictor of future tics, obssessive-compulsive disorder (OCD), and depressive symptom severity.24 Other environmental
triggers (infection, stress, allergen, and so on) involve the dopamine release system,24 –27 increasing cytokine
and autoantibody release, whose interactions with the central nervous system may be involved with the onset or worsening of tics and obsessive-compulsive symp-toms.24 Animal studies prove that immunosuppression
elicited by stressor can be modified by drugs influencing serotonin and dopaminergic systems. The authors view stress-induced alternation of immune response as arising from changed neurochemical patterns of the brain and disturbance of the mechanism via psychoneuroimmuno-modulation.28Furthermore, stress could aggravate
symp-toms of TS and allergies.18,24,29 This may be the reason
why more allergic comorbidity means higher risk of TS, as exhibited in this study.
Interpretations of our study have some limitations. Children with TS often suffer tics along with concomi-tant psychopathologies: attention-deficit-hyperactivity, mood disorders, OCD, episodic outbursts, learning diffi-culties, sleep disturbance, and other behavioral prob-lems. Clinical impact on affected patients is quite signif-icant and can presumably get more scrutiny in their care and pediatric visits as compared with control subjects. Risk of controls to develop allergic disorder may be underestimated, because children with minor allergic disorder may not go to pediatric clinics.
CONCLUSION
Incidence of allergic diseases are correlated with occurrence of Tourette syndrome (TS). Possible im-munopathogenic mechanisms in TS include genetic expression, immune response, the role of cytokine, environmental influence, or stress-related responses. Nevertheless, although the precise mechanism is largely unknown at present, available evidence points
to allergic disease affecting individuals with tic disor-ders. Ongoing large-scale longitudinal studies could provide definite answers to this intriguing topic. REFERENCES
1. Kerr D, Krishnan C, Pucak ML, Carmen J. The immune system and neuropsychiatric diseases. Int Rev Psychiatry. 2005;17:443– 449. 2. Kronfol Z, Remick DG. Cytokines and the brain: implications for
clinical psychiatry. Am J Psychiatry. 2000;157:683– 694. 3. Rothwell NJ. Cytokine in the Nervous System.Georgetown, TX:
PG Landes; 1996;47–71.
4. Ransohoff RM, Benveniste EN, eds. Cytokines and the CNS. Boca Raton, FL: CRC Press; 1996.
5. Plotnikoff N, Murgo A, Faith R, Good R, eds. Cytokines: Stress and Immunity. Boca Raton, FL: CRC Press; 1999.
6. Kunkel SL, Remick DG, eds. Cytokines in Health and Disease. New York, NY, Marcel Dekker; 1992.
7. Kiessling LS, Marcotte AC, Culpepper L. Antineuronal antibodies in movement disorders. Pediatrics. 1993;92:39 – 43.
8. Swedo SE, Leonard HL, Garvey M, et al. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: clinical description of the first 50 cases. Am J Psychiatry.1998;155:264 –271.
9. Cardona F, Orefici G. Group A streptococcal infections and tic disorders in an Italian pediatric population. J Pediatr. 2001;138: 71–75.
10. Church AJ, Dale RC, Lees AJ, Giovannoni G, Robertson MM. Tourette’s syndrome: a cross sectional study to examine the PANDAS hypothesis. J Neurol Neurosurg Psychiatry. 2003;74: 602– 607.
11. Murphy ML, Pichichero ME. Prospective identification and treatment of children with pediatric autoimmune neuropsychiatric disorder associated with group A streptococcal infection (PANDAS). Arch Pediatr Adolesc Med. 2002;156:356 –361. 12. Luo F, Leckman JF, Katsovich L, et al. Prospective longitudinal
study of children with tic disorders and/or obsessive-compulsive disorder: relationship of symptom exacerbations to newly acquired streptococcal infections. Pediatrics. 2004;113:e578 – e585.
13. Hoekstra PJ, Anderson GM, Limburg PC, Korf J, Kallenberg CG, Minderaa RB. Neurobiology and neuroimmunology of Tourette’s syndrome: an update. Cell Mol Life Sci. 2004;61:886 – 898. 14. Trifiletti RR, Packard AM. Immune mechanisms in pediatric
neuropsychiatric disorders. Tourette’s syndrome, OCD, and PANDAS. Child Adolesc Psychiatr Clin N Am. 1999;8:767–775. 15. Ho CS, Shen EY, Shyur SD, Chiu NC. Association of allergy with
Tourette’s syndrome. J Formos Med Assoc. 1999;98:492– 495. 16. Finegold I. Allergy and Tourette’s syndrome. Ann Allergy. 1985;
55:119 –121.
17. Kim H, Moote W, Mazza J. Tourette’s syndrome in patients referred for allergy evaluation. Ann Allergy Asthma Immunol. 1997;79:347–349.
18. Freeman RD, Connolly JE, Baird PA. Tourette’s syndrome: update. Can Med Assoc J. 1984;130:1554 –1557.
19. Jankovic J: Tics and Tourette’s syndrome. In: Tolosa E, Koller WC, Gershanik OS, et al, eds. Differential Diagnosis and Treatment of Movement Disorders. Boston, MA: Butterworth-Heinemann, 1998;99 –108.
20. Comings DE, Comings BG. A controlled study of Tourette syndrome. VI. Early development, sleep problems, allergies, and handedness. Am J Hum Genet. 1987;41:822– 838.
21. Bruun RD. Gilles de la Tourette’s syndrome. An overview of clinical experience. J Am Acad Child Psychiatry. 1984;23:126 – 133.
22. Wurtman RJ. Effects of foods on the brain. Possible implications for understanding and treating Tourette Syndrome. Adv Neurol. 1992;58:293–301.
23. Allergy and Tourette’s syndrome. Ann Allergy. 1986;56:507–508.
AQ: E
AQ: F
AQ: G
24. Martino D, Dale RC, Gilbert DL, Giovannoni G, Leckman JF. Immunopathogenic mechanisms in tourette syndrome: A critical review. Mov Disord. 2009;24:1267–1279.
25. Robertson MM. The Gilles de la Tourette syndrome: the current status. Br J Psychiatry. 1989;154:147–169.
26. Kurlan R. Hypothesis II: Tourette’s syndrome is part of a clinical spectrum that includes normal brain development. Arch Neurol. 1994;51:1145–1150.
27. Hyde TM, Weinberger DR. Tourette’s syndrome. A model neuropsychiatric disorder. JAMA. 1995;273:498 –501. 28. Idova G, Cheido M, Devoino L. Modulation of the immune
response by changing neuromediator systems activity under stress. Int J Immunopharmacol. 1997;19:535–540.
29. Gustafsson PA, Bjorksten B, Kjellman NI. Family dysfunction in asthma: a prospective study of illness development. J Pediatr. 1994;125:493– 498.