國立臺灣大學工學院暨醫學院醫學工程學系 博士論文
Department of Biomedical Engineering College of Engineering and College of Medicine
National Taiwan University Doctoral Dissertation
應用脈衝式超音波熱治療與氯喹強化癌症奈米藥物治療
Enhancing Cancer Tumor Treatment of Nanomedicine with Pulsed-wave Ultrasound Hyperthermia and Chloroquine
江季峰
Chi-Feng Chiang
指導教授:林文澧 博士 Advisor: Win-Li Lin, Ph.D.
中華民國 108 年 10 月
October 2019
致謝
感謝指導教授林文澧老師多年來的悉心指導,不只指引研究 方向,更以身作則示範了不停探索新研究主題的做學問態度。
感謝聖凱學長、為中、芷君學姊,在研究和實驗方面提供了 許多寶貴建議與技術指導。感謝梁博欽醫師伉儷在研究及生 活方面提供的各種協助。也感謝實驗室學弟妹們在事務上的 分擔幫忙,讓我在博士生涯最後幾年能專心致力於研究上。
感謝我的家人們,從我決定棄醫從研的時候開始,一直以來 都無條件地支持我。
最後,也是最感謝的,是我親愛的妻子齡齡。沒有妳的陪伴、
鞭策、與鼓勵,這篇論文肯定無法完成。
摘要
熱治療結合化療藥物為一有效之腫瘤治療策略,能強化奈米藥物穿透進入腫 瘤組織並強化其療效。本研究分為兩部分,第一部分探討脈衝式超音波熱治療是 否可增強 PEGylated liposomal doxorubicin (PLD) 對於轉移乳癌模式之療效。本實 驗使用小鼠乳癌細胞 4T1 種植於 BALB/c 小鼠腦部,以活體影像系統追蹤腫瘤成 長。腫瘤植入後六天,投予 PLD 並於腫瘤區域施打脈衝式超音波熱治療。實驗結 果顯示脈衝式超音波熱治療可增加 PLD 於腫瘤區域之累積。此外,化療藥物 PLD 加上脈衝式超音波熱治療能有效抑制腫瘤之生長,而免疫染色及細胞凋亡測試亦 佐證其效用。此研究證實應用脈衝式超音波熱治療能促進化療藥物有效進入腦腫 瘤組織並達到治療之效果。
第二部分則結合脈衝式超音波熱治療與自噬抑制劑 chloroquine (CQ) 以進一 步強化奈米藥物之療效並抑制腫瘤之復發。自噬作用在腫瘤細胞經常扮演重要的 存活機制,因此抑制自噬作用是一可能之腫瘤輔助治療策略。本實驗使用小鼠乳 癌細胞 4T1 種植於 BALB/c 小鼠皮下,於腫瘤植入後第五天投予 PLD 與 CQ,
並於腫瘤局部施打脈衝式超音波熱治療,之後觀察腫瘤的生長變化並追蹤其復 發。實驗結果證實 CQ 能更加強化脈衝式超音波與奈米藥物對腫瘤的抑制效果,
並且能延緩腫瘤復發的時間。免疫染色與西方點墨法也證實了 CQ 對腫瘤細胞能 有效抑制自噬作用。此研究證實結合脈衝式超音波熱治療與 CQ 能更加強化奈米 藥物之抗腫瘤效果,並能長期抑制腫瘤復發。
關鍵詞: 脈衝式超音波熱治療,奈米藥物,doxorubicin,氯喹,自噬抑制,癌症,
腫瘤
Abstract
Chemotherapeutic agents and hyperthermia are known to have synergistic effect in cancer treatment. Focused ultrasound sonication enhances the delivery of nanodrug into tumor and strengthens the efficacy of thermo-chemotherapy.
In the first part of our study, we investigated the enhancing effect of pulsed-wave ultrasound hyperthermia (pUH) on the delivery and therapeutic efficacy of PEGylated liposomal doxorubicin (PLD) for brain metastasis of breast cancer. Murine breast cancer cells 4T1 were implanted into mouse striatum as a metastatic brain tumor model, and the tumor growth was monitored with in vivo imaging system (IVIS). The mice were intravenously injected with PLD followed by transcranial pUH or continuous ultrasound hyperthermia (cUH) treatment on day-6 after tumor implantation. The amounts of doxorubicin accumulated in the normal brain and tumor tissues were measured with fluorometry. The tumor growth responses for the control, pUH, PLD, PLD+cUH, and PLD+pUH groups were evaluated with IVIS. The PLD distribution and cell apoptosis were assessed with immunofluorescence staining. The results showed that pUH significantly enhanced the PLD delivery into brain tumors and the tumor growth was further inhibited by PLD+pUH without damaging the sonicated normal brain tissues.
This indicates that low-dose transcranial pUH is a promising method to selectively enhance nanodrug delivery and improve the brain tumor treatment.
In the second part of our study, we combined pUH and an autophagy inhibitor chloroquine (CQ) to further strengthen the antitumor efficacy of PLD and postponed the recurrence of tumor. Autophagy often serves as an important surviving mechanism for cancer cells, therefore inhibiting autophagy has been considered as an adjuvant
anti-cancer strategy. In this study, BALB/c mice implanted with subcutaneous 4T1 tumor were used as an animal tumor model. On Day 5 after tumor implantation, tumor-bearing mice received intravenous injection of PLD (10 mg/kg) plus 15-minute on-tumor pUH and were then fed with CQ (50 mg/kg daily) thereafter. It was shown that prolonged suppression of tumor growth was attained with PLD+pUH+CQ treatment, whereas in PLD+pUH group tumors quickly recurred after an initial inhibition.
Immunohistochemical staining and Western blotting showed that autophagy of cancer cells was blocked for the mice receiving CQ. This study proves that PLD+pUH+CQ is a promising strategy to treat cancer for a sustained inhibition.
Keywords: pulsed-wave ultrasound hyperthermia, nanodrug, doxorubicin, chloroquine, autophagy inhibition, cancer, tumor
Contents
口試委員審定書 ... i
致謝 ... ii
中文摘要 ...iii
Abstract ... iv
Contents ... vi
List of Figures ... x
List of Tables ... xv
Chapter 1. Background & Objectives ... 1
1.1 Difficulties in cancer treatment ... 1
1.2 Cancer nanomedicine ... 2
1.2.1 Preferential accumulation due to EPR effect ... 2
1.2.2 Prolonged circulation time of PEGylated liposomes ... 3
1.2.3 Synergy between hyperthermia and of nanomedicine ... 4
1.3 Ultrasound Hyperthermia ... 4
1.3.1 Thermal effect of ultrasound ... 5
1.3.2 Ultrasound hyperthermia-enhanced drug delivery ... 6
1.3.3 Non-thermal effects of ultrasound ... 6
1.4 Autophagy inhibition in cancer treatment ... 7
1.5 Objectives ... 8
1.6 Thesis outline... 8
Chapter 2. Pulsed-wave Ultrasound Hyperthermia Selectively Facilitates the Delivery of PEGylated Liposomal Doxorubicin and Improves the Antitumor Efficacy against Brain Metastasis of Breast Cancer ... 10
2.1 Introduction ... 10
2.2 Materials and Methods ... 12
2.2.1 PEGylated liposomal doxorubicin (PLD)... 12
2.2.2 In vitro investigation of PLD accumulation in cancer cells enhanced by ultrasound ... 13
2.2.3 Preparation of tumor cells and the brain tumor model ... 14
2.2.4 Focused ultrasound (FUS) system and pulsed-waved FUS hyperthermia14 2.2.5 Experimental grouping ... 15
2.2.6 Quantification of PLD entering the normal brain and tumor tissues ... 15
2.2.7 Measurement of tumor growth by in vivo imaging system (IVIS) and mouse survival ... 16
2.2.8 Immunofluorescence and PLD distribution ... 16
2.2.9 TUNEL assay ... 17
2.2.10 Statistical analysis ... 17
2.3 Results ... 18
2.3.1 Pulsed-wave ultrasound better enhances PLD delivery into tumor cells 18 2.3.2 Low-dose pulsed-wave ultrasound hyperthermia enhances the antitumor action in brain tumors ... 18
2.3.3 PLD delivery to normal brain and tumor tissues by low-dose pulsed-wave/continuous-wave ultrasound hyperthermia ... 19
2.3.4 Immunofluorescence detection of PLD deposition ... 20
2.3.5 TUNEL staining for apoptotic cancer cells in the tumors ... 20
2.4 Discussion... 21
2.5 Conclusions ... 24 Chapter 3. Pulsed-wave Ultrasound Hyperthermia Enhanced Nanodrug Delivery
Combined with Chloroquine Exerts Effective Antitumor Response and
Postpones Recurrence ... 35
3.1 Introduction ... 35
3.2 Materials and Methods ... 37
3.2.1 Chemical Reagents ... 37
3.2.2 Tumor cells ... 37
3.2.3 In vitro fluorescence assay of PLD internalization by 4T1 cells with or without CQ ... 37
3.2.4 MTT Cytotoxicity Assay ... 38
3.2.5 In vivo tumor model ... 39
3.2.6 Animal treatment experiment ... 39
3.2.7 Histopathological Examination and Immunohistochemical Study ... 40
3.2.8 TUNEL Assay ... 41
3.2.9 Western Blotting ... 42
3.2.10 Statistical analysis ... 42
3.3 Results ... 43
3.3.1 In vitro fluorescence assay of PLD internalization by 4T1 cells with or without CQ ... 43
3.3.2 MTT Cytotoxicity Assay ... 43
3.3.3 Combination treatment of PLD+pUH and CQ inhibited cancer tumor growth and delayed its recurrence ... 43
3.3.4 Immunohistochemical study proved autophagy of tumor cells blockaded by CQ administration ... 44
3.3.5 TUNEL assay showed apoptosis increased by PLD+pUH, not by CQ .. 45
3.3.6 Western Blotting ... 45
3.4 Discussion... 46
3.5 Conclusions ... 50
Chapter 4. Summary and Future Work ... 63
References ... 65
List of Figures
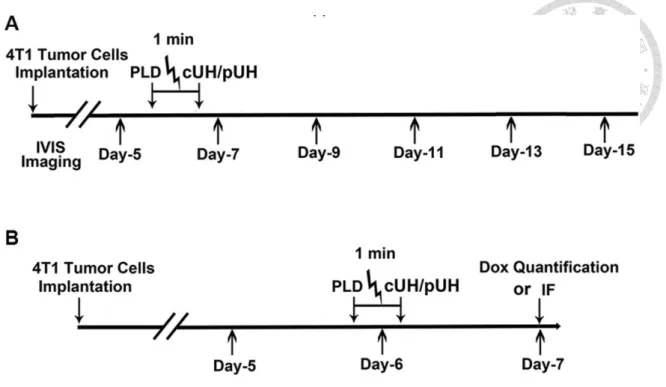
Figure 2-1. Typical temperature responses were measured at the focal zone with continuous wave or pulsed-wave ultrasound sonication over time.. ... 26 Figure 2-2. (A) Time course for the therapeutic experiments. 4T1 cancer cells were
implanted on day 0, and the treatments were performed on day 6 with PLD injection, and/or continuous-wave ultrasound hyperthermia (cUH) or pulsed-wave ultrasound hyperthermia (pUH). IVIS imaging was performed on day 5, 7, 9, 11, 13 and 15. (B) Schedule for doxorubicin (Dox) quantification or immunofluorescence (IF) after different therapeutics. ... 27 Figure 2-3. Immunofluorescence staining for in vitro investigation of PEGylated
liposomal doxorubicin (PLD) up-taken by 4T1 breast tumor cells with or without ultrasound sonication. Fluorescence staining of tumor cells was performed 2 h after different therapeutics: 1) control: no treatment; 2) PLD:
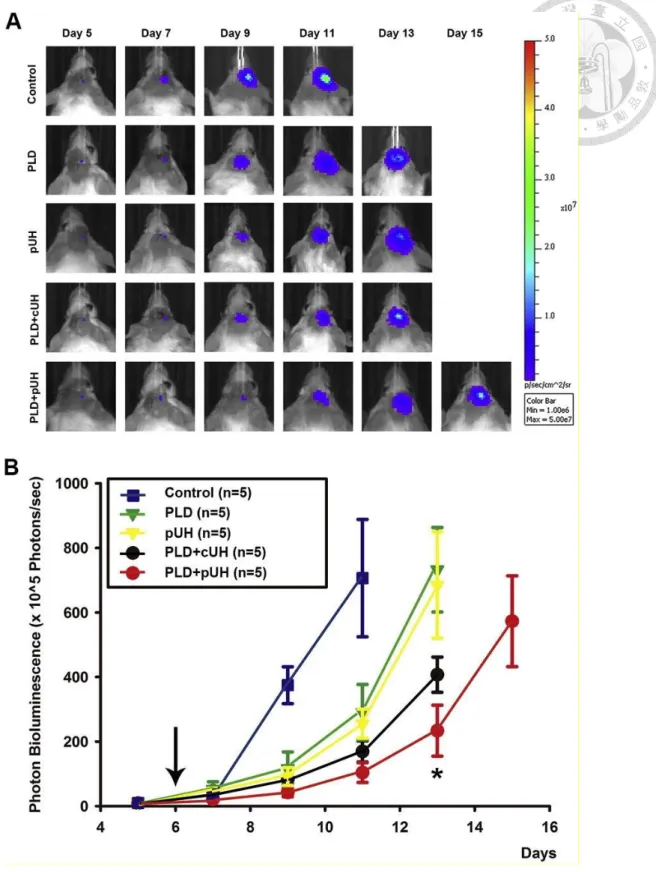
PLD alone; 3) PLD + cU: PLD plus continuous-wave ultrasound sonication; 4) PLD + pU: PLD plus pulsed-wave ultrasound sonication. A dose of 3 μg/ml PLD was used in this experiment and the sonication duration was 3 min for both continuous- and pulsed-wave ultrasound with the same acoustic power (0.4 W). Red, blue and green colors represent PLD, cell nuclei and cell membrane, respectively. Scale bar = 200 μm ... 28 Figure 2-4. (A) Representative IVIS imaging and (B) bioluminescent signal
quantification of mouse brain tumors from day 5 to day 15 after tumor implanted. Mice were implanted with luciferase-expressing 4T1-luc2 breast cancer cells in the brains. Bioluminescent signals were quantified using an IVIS imaging system. Treatment was executed on day 6 after tumors
implanted, and images were obtained every other day. There were five groups:
Control (no treatment), PLD, pUH (pulsed-wave ultrasound hyperthermia), PLD + cUH (continuous-wave ultrasound hyperthermia), and PLD + pUH. A dose of 3.5 mg/kg PLD was used and the ultrasound parameters used were shown in Table 1. The arrow indicates the time point for different therapeutics performed. Note that PLD + pUH markedly inhibited the brain tumor growth.
Data are presented as mean ± SEM (n = 5 for each group). *Represents p <
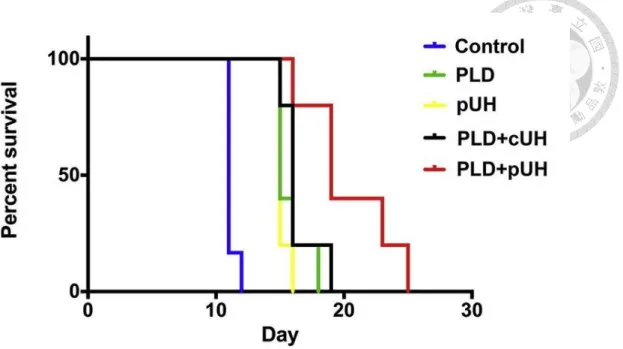
0.05, the comparison between the PLD + pUH group and the PLD + cUH group. . ... 29 Figure 2-5. Kaplan-Meier survival curves of tumor-bearing mice with different
therapeutics. PLD + pUH significantly increased the lifespan of tumor-bearing mice. ... 31 Figure 2-6. Doxorubicin concentrations in tumor and normal brain tissues for mice
with/without continuous-wave ultrasound hyperthermia (cUH) or pulsed-wave ultrasound hyperthermia (pUH). Mice were implanted with 4T1-luc2 murine breast cancer cells on day 0 and were injected with a dose of 5 mg/kg PLD with/without transcranial cUH or pUH on day 6 after tumor implanted. Note that pUH significantly enhanced the accumulation of PLD in the tumor tissues than cUH. In addition, both cUH and pUH did not elevate the PLD concentration in the normal brain tissues. Data are presented as mean
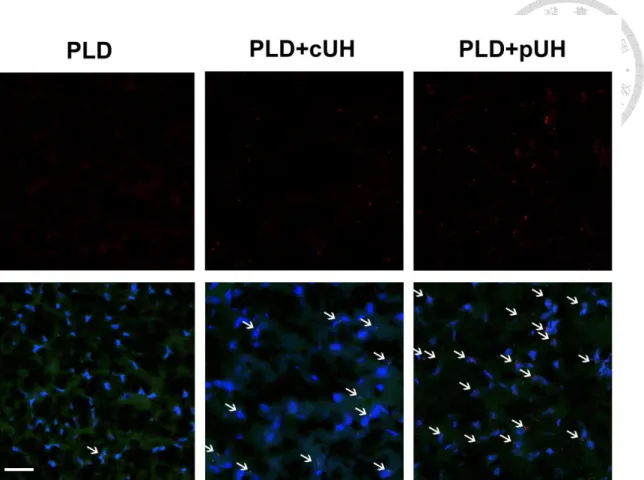
± SEM (n = 5 for each group). *Represents p < 0.05 ... 32 Figure 2-7. Immunofluorescence staining in the tumor regions after different
therapeutics. Mouse brains were implanted with 4T1-luc2 tumor cells and the treatments were performed 6 days after tumors implanted. In these experiments, a dose of 15 mg/kg PLD was i.v. injected. The mice were
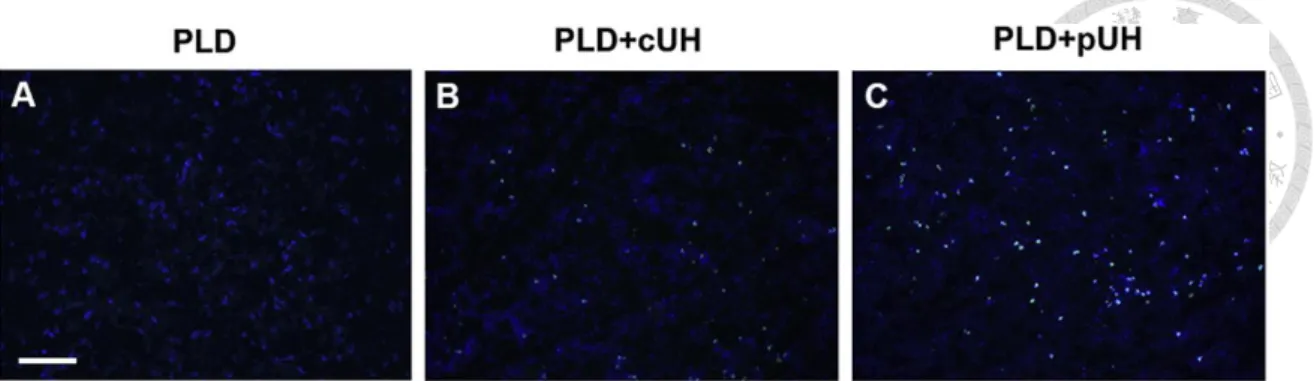
sacrificed 24 h after the treatment and then the brain tissues were stained with DAPI to visualize the tumor cell nuclei (blue) and with PKH67 to show the cell membrane (green). Tumors treated with PLD + pUH had the strongest red fluorescence expression and the deposition of doxorubicin was near the cell nuclei. Scale bars: 50 μm. ... 33 Figure 2-8. TUNEL staining was used to detect apoptotic cells in tumor tissues. Mouse
brains were implanted with 4T1-luc2 tumor cells and the treatments were performed 6 days after tumors implanted. A dose of 3.5 mg/kg PLD was i.v.
administered for these experiments. The mice were then sacrificed 24 h after the treatments and then brain tumor slices were obtained for staining. Tumor slices were firstly stained with terminal TUNEL (green) and then with DAPI to visualize the tumor cell nuclei (blue). The strong apoptotic signal was observed in the PLD + pUH group. Scale bar: 100 μm. ... 34 Figure 3-1. The scheme of PEGylated Liposomal Doxorubicin (PLD) + pulsed-wave
Ultrasound Hyperthermia (pUH) + chloroquine (CQ) in cancer treatment.. 51 Figure 3-2. Time schedule of treatment experiment. PEGylated Liposomal Doxorubicin
(PLD) was given intravenously on Day 5 after tumor implantation.
Pulsed-wave ultrasound hyperthermia (pUH) was administered 10~15 minutes after PLD administration. Then mice were orally fed chloroquine (CQ) dissolved in drink water daily till experiment end. ... 52 Figure 3-3. (A) Fluorescent microscopic images of 4T1 murine breast cancer cells in
vitro treated with PLD+CQ+H or PLD+H. Doxorubicin (red) distribution with respect to nuclei (blue, stained with Hoechst 33342 dye) were shown. (B) Mean fluorescent intensity of doxorubicin with respect to nucleus region area.
Abbreviation: H: hyperthermia. ns: not significant. ... 53
Figure 3-4. MTT Cytotoxicity Assay. The cell viability was reduced by PLD with hyperthermia in a dose-dependent manner. The addition of CQ (10μM) further potentiated the cytotoxicity of PLD+H comparing to the counterpart without CQ. **: p<0.01, ***: p<0.001. Abbreviation: H=hyperthermia ... 54 Figure 3-5. (A) Representative photographs of tumor for each group. Region encircled
by dashed line indicated tumor. Scale bar=1cm. (B) The response of subcutaneous 4T1 murine breast cancer to different treatment:
PLD+pUH+CQ, PLD+pUH, CQ, and control groups. * denotes p<0.05, and
** denotes p<0.01 between PLD+pUH+CQ and PLD+pUH, respectively. . 55 Figure 3-6. The Kaplan-Meier survival plot for PLD+pUH+CQ, PLD+pUH, CQ, and
control groups. ... 57 Figure 3-7. Histological examinations with hematoxylin-eosin staining for each
experimental group. Scale bar = 100 μm. ... 58 Figure 3-8. Immunohistochemical stain for LC3 (brown stain) for each experimental
group. LC3 accumulation reflects late-stage inhibition of autophagy. Greatly increased accumulation of LC3 was observed in both PLD+pUH+CQ and CQ groups, whereas slightly increase in the PLD+pUH group, and nearly no accumulation in the control group. Scale bar = 100 μm. ... 59 Figure 3-9. (A) Fluorescent microscopic images of TUNEL assay for each experimental
group. Apoptotic signals (green) were much more enhanced in PLD+pUH+CQ group and PLD+pUH group. Scale bar = 200 μm. (B) The fluorescent intensities for each experimental group were quantified and analyzed for statistical significance. **: p<0.01. ***: p<0.001. ns: not significant. ... 60 Figure 3-10. Western blot for LC3 for each experimental group. Increased expression of
LC3-II was observed in PLD+pUH+CQ group and CQ group, reflecting the late-stage autohphagy inhibition by CQ. LC3 expression was slightly reduced in PLD+pUH group comparing to control group. ... 62
List of Tables
Table 2-1. Ultrasound parameters used in the in vivo experiments to perform continuous-wave ultrasound hyperthermia (cUH) or pulsed-wave ultrasound hyperthermia (pUH). ... 25
Chapter 1. Background & Objectives
1.1. Difficulties in cancer treatment
Cancer is a devastating threat to human health, causing the second leading number of death worldwide and responsible for an estimated 9.6 million deaths in 2018.
Globally, about one in six deaths is due to cancer.
Several characteristics owned by cancer cells make them quite distinct from normal cells [1,2]. One of the most symbolic feature of cancer cells is its limitless replicative potential. Malignant cells proliferate dysregulated and form neoplasms that continue to grow. Besides, they also gain the ability to break basement membrane and invade adjacent tissue. Cancer cells can even travel via blood stream or lymphatic vessels for long distance to faraway sites where they may succeed in founding new colonies.
Recent studies indicate that cancer is not merely a collection of relatively homogenous malignant cells, but a complex structure which involves many types of cell, including endothelial cells, inflammatory cells, and stroma cells, etc. [2] This tumor microenvironment supports tumor growth and protects them from being attacked by host immune system. The sophisticated environment of cancer makes treating cancer a difficult challenge.
Furthermore, a small fraction of neoplastic cells, termed cancer stem cells (CSC), even aggravate the problem. Like normal tissue stem cells, CSCs may self-renew as well as spawn more differentiated descendent cells which forms the most part of bulk tumor.
CSCs are capable of initiating a tumor even in very scarce numbers. Due to their relative quiescence in mitotic activity, CSCs have higher resistance to chemotherapy and radiotherapy, which often preferentially kill fast-dividing cells. Their persistence may be
responsible for the recurrence of cancer and make long-term cure of disease a challenging task.
1.2. Cancer nanomedicine
Chemotherapy remains the mainstream non-surgical treatment strategy against many types of cancer. Chemotherapeutic drugs target the signature characteristic of cancer cells by interrupting their division, hence malignant cells are no longer allowed to replicate limitlessly. However, the lack of specificity of conventional chemotherapeutic drugs limits their usefulness. A lot of chemotherapeutic drugs pose toxicity to normal organs, suppress immune system, and induce various adverse effects.
These side effects not only impact on patients’ life quality but also affect the feasible therapeutic dose, resulting in nonoptimal treatment.
The advance of nanotechnology provides a new opportunity to solve this problem [3,4,5]. By proper designing, nanoparticles can deliver chemotherapeutic drugs into cancer cells more efficiently and more specifically while minimizing the toxicity to normal cells. Nanomedicine can even simultaneously carry multiple functional moieties to facilitate chemotherapeutic drugs. Furthermore, nanomedicine possesses the potential to overcome drug resistance, since nanoparticles can bypass P-glycoprotein efflux pump, one of the main drug resistance mechanisms [5,6].
Nanoparticles used for cancer therapy can be made from a variety of materials, including polymers, liposomes, inorganic materials, etc. However, only a limited number of liposomes and polymer nanoformulations were clinically approved.
1.2.1. Preferential accumulation due to EPR effect
that of molecular drug, which is mainly driven by diffusion. Nanomedicine preferentially accumulates in neoplastic tissues because of the enhanced permeability and retention (EPR) effect [2,7,8].
The EPR effect results from two key characteristics of the neoplastic tissues, the leaky vasculature and impaired lymphatic drainage [7,8]. Blood vessels in normal tissues are well-structured and lined by tight endothelial cells, which prevent nanoparticles from travelling through endothelium into tissue. However, in neoplastic tissue, the vasculature is structurally chaotic and defective in endothelial lining, thereby enabling nano-sized particles to pass through endothelial defects. Furthermore, the lack of functional lymphatic drainage allows nanoparticles to retain within tumor tissue for longer durations without being cleared. The EPR effect provides a way to preferentially deliver chemotherapeutic moieties into tumor while minimizing the adverse effects to normal tissue damage.
1.2.2. Prolonged circulation time of PEGylated liposomes
Despite the advantage of EPR effect, nanomedicine suffers from another problem.
Nanoparticles entering circulation system are rapidly cleared by mononuclear phagocyte system (MPS) and quickly removed from blood stream, therefore they do not persist long enough to be delivered to target organ in sufficient dose [9].
To overcome such issue, long-circulating liposomes were invented. These liposomes carry long and flexible chains of hydrophilic polymers, e.g. poly-(ethylene glycol) (PEG), on their outer surface. The PEG chains occupy the peri-liposomal space and sterically exclude other macromolecules from getting close. Consequently, the binding of blood plasma opsonins to the liposome surface are hindered, and it renders these PEGylated liposomes ‘stealth’ to the surveillance of MPS [10]. The
pharmacokinetic half-life of stealth liposomes is hence greatly prolonged compared to conventional liposomes [11]. Stealth technology not only extends the circulation time of liposomes, but also changes their bio-distribution. PEGylated liposomes had a less uptake by liver and spleen while showed a higher plasma concentration as compared to conventional liposomes.
1.2.3. Synergy between hyperthermia and nanomedicine
Hyperthermia has been used in the treatment of many kinds of cancer for centuries [12,13]. Mildly elevating tissue temperature and maintaining it for several minutes can increase the blood flow and vascular permeability in the heated tumor region [14]. In addition, the uptake of chemotherapeutic drugs may be enhanced when cancer cells are placed at 43℃ [15]. The delivery and uptake of nanomedicine at the target region can then be greatly enhanced using localized mild hyperthermia.
Furthermore, hyperthermia has been known to have synergistic effect with chemotherapeutic agents [15,16] or ionizing radiation [17]. Cancer cells can repair potentially lethal damage after exposure to chemotherapeutic drugs at 37℃, but at 43℃
the repair ability was greatly hindered. Therefore, hyperthermia and chemotherapeutic nanomedicine can complement each other and form a good combination.
1.3. Ultrasound Hyperthermia
Ultrasound is a mechanical wave with frequencies higher than the audible range of human (20 kHz or greater). It oscillates and penetrates tissues, and is capable of carrying acoustic energy. Due to noninvasiveness and nonionizing radiation, ultrasound is widely used in medical applications, either as a diagnostic tool or therapeutic use.
1.3.1. Thermal effect of ultrasound
The effects of ultrasound dealt to biological tissues can be divided into two categories, thermal effects and non-thermal effects. Thermal effects result from the absorption of acoustic energy by tissues, and then the absorbed energy is converted into heat and it raises the temperature of tissues. A mild rise in temperature of biological tissues results in upregulated cellular metabolism and increase in blood flow, whereas a high rise in temperature can denature proteins and eventually cause coagulative necrosis.
Different temperature rises lead to different clinical applications, e.g. mild temperature rises in adjuvant hyperthermia therapy, high temperature rises in ablation therapy, etc.
Cancer cells are more vulnerable to ultrasound exposure than normal cells [18].
Ultrasound can directly kill or sensitize cancer cells to stresses such as chemotherapeutic drugs or X-ray irradiation [19], and synergistic effects are observed when the temperature of cancer cells rises [20]. In addition, it has been reported that apoptosis was induced in several leukemia and lymphoma carcinoma cell lines in vitro by high-intensity pulsed ultrasound [21], low-intensity pulsed ultrasound [22], and ultrasound in combination with hyperthermia [23].
Along with the direct effects on tissues or cells, ultrasound hyperthermia can also activate host’s immune system to fight against cancer. Hyperthermia induces anti-tumor immune response through complex mechanisms. It increases the expression of several potential tumor antigens, including MHC class I, heat shock proteins, and exosomes.
Hyperthermia also stimulates immune cells, such as nature killer cells, CD8+ T cells, and dendritic cells. Along with these, the trafficking of immune cells between lymphoid organs and tumor are improved [12].
Ultrasound induced-hyperthermia was found to be more advantageous over other heating modalities due to its non-invasiveness and ability to penetrate into deep tissues
[24,25]. By tailoring transducer design, the acoustic energy of ultrasound can be precisely focused onto a very compact region even if the target is deeply located within body.
1.3.2. Ultrasound hyperthermia-enhanced drug delivery
During ultrasound sonication, the blood flow, elasticity and metabolic processes of the heated tumor are increased [26]. These effects facilitate the drug accumulation in the heated tumor region and improve the drug uptake by cancer cells through the release from thermal-sensitive forms [27] and/or through the membrane permeability modulation, especially for those cancer cells expressing multi-drug resistance [28]. The study of our group proved that short-time focused ultrasound hyperthermia (UH) could noninvasively enhance the permeability of BTB in the sonicated brain tumor region [29].
The results suggested that ultrasound sonication enhanced the delivery of PEGylated liposomal doxorubicin (PLD) into brain tumors and improved the treatment efficacy without damaging adjacent normal brain tissues.
1.3.3. Non-thermal effects of ultrasound
Non-thermal effects of ultrasound are usually associated with radiation force, acoustic streaming, and cavitation. Acoustic streaming and radiation pressure influence fluid and particle motion, causing convective microflow that can permeate cellular membrane and send particles into cells. Besides, ultrasound causes cavitation in the presence of gas-containing microbubbles. Cavitation is the oscillation of microbubbles in response to the pressure wave of ultrasound. Microbubbles repeatedly expand then contract, and may collapse violently when they grow beyond their critical sizes. The collapse, known as inertial cavitation, creates a brief but strong shockwave and causes
local a temperature rise. Additionally, free radicals are generated during cavitation by pyrolysis of molecules present inside collapsing microbubbles [30]. These phenomena can be utilized in several biomedical applications, such as blood-brain barrier disruption and sonodynamic therapy.
Pulsed-wave ultrasound was reported to further promote ultrasound-induced cancer cell apoptosis [31]. The pulse repetition frequency (PRF) might play a key role in ultrasound-induced biological and chemical effects [32]. Combination of doxorubicin and pulsed-wave ultrasound (PRF: 100 Hz) has been demonstrated its synergistic effects in cell killing and apoptosis enhancement in human lymphoma cells [16].
1.4. Autophagy inhibition in cancer treatment
Autophagy is a crucial catabolic process in maintaining homeostasis of cellular environment. It turns over old proteins and organelles and recycles cellular components [33,34]. Autophagy also plays an important role in cancer pathophysiology. The role of autophagy seems to be bi-directional depending on circumstances: it prevents cancer development, but helps established cancer to survive from stress and threats [33,34,35,36,37,38]. Therefore, autophagy inhibition has been investigated as an evolving strategy to fight against advanced cancer [37,38,39].
Among autophagy inhibitors, chloroquine (CQ) and its analogue hydroxychloroquine (HCQ) are the most widely used drugs. They inhibit lysosomal acidification and cause a late-stage blockade in autophagy [37]. In addition, CQ was reported to possess multiple anti-cancer mechanisms other than autophagy inhibition, such as targeting against cancer stem cells (CSC) [40] and inducing tumor vessel normalization [41]. There were several ongoing clinical trials using CQ (or HCQ) additional to conventional chemotherapeutic agents to treat various kinds of cancer,
including colorectal cancer, glioblastoma, and pancreatic cancer [38].
1.5. Objectives
The aim of present study is to develop an effective strategy capable of long-lastingly suppressing tumor growth and preventing cancer relapse. We implemented pulsed-wave ultrasound hyperthermia (pUH) to facilitate the delivery and activity of anti-cancer nanodrug against tumors. In addition, we utilized chloroquine to inhibit autophagy of cancer cells in order to prevent tumor recurrence.
The first part of study assesses the application of pUH to enhance the delivery and efficacy of anti-cancer nanodrug and evaluate treatment effectiveness in an intracranial brain metastatic tumor model.
The second part of study investigates the combination treatment of PLD with pUH and a constant CQ administration to successfully treat tumors, prevent tumor recurrence, and improve a disease-free survival.
1.6. Thesis outline
This dissertation is organized in four chapters. Chapter 1 provides an introduction of main topics to be addressed in this thesis. The application of cancer nanomedicine and enhanced delivery with ultrasound hyperthermia are briefly reviewed. Furthermore, the role of chloroquine, an autophagy inhibitor, in cancer treatment is introduced.
Finally, the motivation and purpose of the thesis are described.
Chapter 2 focuses on the application of pulsed-wave ultrasound hyperthermia (pUH) to enhance the delivery and efficacy of PLD. The experiment setups in this study include in vitro fluorescent assay assessing PLD deposition, in vivo PLD quantification,
tumor growth evaluation with IVIS in an intracranial brain metastatic tumor model, and survival analysis.
Chapter 3 focuses on the addition of constant CQ administration along with PLD and pUH, to further improve the anti-tumor efficacy and prolong the disease-free survival. The experimental methods in this section include in vitro fluorescent assay investigating PLD internalization, MTT assay, Western blotting, immunohistochemistry study, and tumor growth in a subcutaneous tumor model.
Finally, Chapter 4 summarizes the research highlights of our studies and addresses the future work.
Chapter 2. Pulsed-wave Ultrasound Hyperthermia Selectively Facilitates the Delivery of PEGylated Liposomal Doxorubicin and Improves the Antitumor Efficacy against Brain
Metastasis of Breast Cancer
2.1. Introduction
Elevating tissue temperature to a mild range and maintaining for several minutes can increase blood flow and drug absorption in the heated region [42]. Drug delivery and uptake at the target region can then be enhanced using localized mild hyperthermia.
Ultrasound is a mechanical energy and it is a proved modality able to improve the tumor treatment outcome. Inhibition of many malignant tumors by hyperthermia alone [13] or in combination with other modalities was reported decades ago. Synergistic response was well-known when it came with ionizing radiation [17] and in combination with some chemotherapeutic agents [15]. Ultrasound induced-hyperthermia was also investigated [24] and found to be more beneficial than other heating modalities due to its facility in controlling focal power and tissue attenuation coefficient for deep tumor targeting [25].
Despite the fact that the blood-tumor barrier (BTB) is more permeable than the blood-brain barrier (BBB), the efficacy of systemic chemotherapy for the treatment of brain tumor is still hindered by BTB from achieving the therapeutic levels. It is also worth mention that the selectivity and heterogeneity of the BTB permeability blocks many chemotherapeutic agents from effectively accumulating in the target [43].
Therefore, it is necessary to develop powerful approaches to improve the delivery of
therapeutic agents to the target region with minimizing the side effects of critical tissues.
Short-time focused ultrasound hyperthermia (UH) could noninvasively enhance the permeability of BTB in the sonicated brain tumor region [29]. The results suggested that ultrasound sonication represented a feasible approach for enhancing PLD delivery into brain tumors and improved the treatment efficacy without damaging the normal brain tissues. It also reported that pulsed-wave ultrasound could promote ultrasound-induced cancer cell apoptosis [31]. The pulse repetition frequency (PRF) might play a key role in ultrasound-induced biological and chemical effects [32]. Combination of doxorubicin and pulsed-wave ultrasound (PRF: 100 Hz) has been demonstrated its synergistic effects in cell killing and apoptosis enhancement in human lymphoma cells [16].
Ultrasound can be a non-invasive, highly precise and deeply penetrating mechanical wave and has the potential to destroy tumor cells. For cancer therapy, ultrasound can directly kill or sensitize cancer cells to upcoming stresses, such as anticancer drugs or X-irradiation [19], and the synergistic effect also occurs when cancer cells suffer temperature rise [20]. This indicates that thermal effect is one of the key factors for ultrasound cancer treatment. During ultrasound sonication, the blood flow, elasticity and metabolic processes of the heated tumor are increased [26]. These would enhance the accumulation of drug in the heated tumor and the drug uptake for cancer cells through the release from thermal-sensitive forms [27] and/or through the membrane permeability modulation, especially for those cancer cells displaying multidrug resistance [28]. Therapeutic ultrasound was developed to deliver drugs and genes to a variety of tissues [44,45,46] and locations, such as tumors [47,48], cardiac tissues [49,50], and brain [51]. The alternate compressions and rarefactions of ultrasound produce a slight oscillation of fluid and tissues, which might increase cell membrane permeability [52] and molecular transport by altering molecular motion [53].
Cancer cells were more prone to be killed by ultrasound exposure than normal cells [18]. For cancer therapy, low-intensity ultrasound has been used via specific pathway interactions, such as sonoporation therapy [54], enhancing chemotherapy, gene therapy [16], and apoptotic therapy [55]. It has been recently reported that apoptosis was induced in several leukemia and lymphoma carcinoma cell lines in vitro by high-intensity pulsed ultrasound [21], low-intensity pulsed ultrasound [22], and ultrasound in conjunction with hyperthermia [23].
The aim of the present study was to develop pulsed-wave low-dose ultrasound hyperthermia and evaluate its treatment effectiveness for brain tumors. To determine whether pulsed-wave ultrasound was effective to deliver PLD into the sonicated tumor cells, we arranged an in vitro test for tumor cells exposed to ultrasound sonication under a constant temperature condition. Then, we arranged a focused ultrasound transducer to produce pulsed-wave/continuous-wave low-dose ultrasound hyperthermia in the target brain tumor after an I.V. PLD injection. We followed up the tumor growth response and measured the PLD depositions in brain and tumor tissues one day after the PLD injection with/without ultrasound hyperthermia.
2.2. Materials and Methods
2.2.1. PEGylated liposomal doxorubicin (PLD)
The PLD used in this study was a commercialized product, Lipo-Dox® purchased from Taiwan Tung Yang Biopharm Company Ltd. It contains 2 mg/mL doxorubicin and 14 mol/mL phospholipids. Its lipid composition is DSPC, cholesterol, and PEG-DSPE (molar ratio 3:2:0.3). The average particle size of the PLD is about 100 nm and its elimination half-life is 65 h.
2.2.2. In vitro investigation of PLD accumulation in cancer cells enhanced by ultrasound
Murine 4T1-luc2 breast cancer cells (ATCC® CRL-2539TM) expressing firefly luciferase (luc2 vector) were cultured in Dulbecco’s Modified Eagle’s Medium (DMEM) supplemented with 10% heat-inactivated fetal bovine serum (FBS), and penicillin (100 U/mL)/streptomycin (100 μg/mL) in 10 cm tissue culture plates in a 5% CO2-containing incubator at 37 °C. Bioluminescence activity was confirmed using fluorometer. Cell number and viability were calculated using a hemocytometer and trypan blue exclusion.
To investigate PLD uptake by tumor cells, 106 4T1-luc2 cells with 1 mL PBS were loaded in an Eppendorf tube and prepared to receive ultrasound sonication. A dose of 3 μg/mL PLD was added to the Eppendorf tube before sonication. Ultrasound sonication was generated by a 500-kHz, single-element focused transducer (H104MR; Sonic Concepts, Bothell, WA, USA) with a diameter of 64 mm and a curvature radius of 62 mm. The radiofrequency signal was supplied by a function generator (33120A; Agilent, Palo Alto, CA, USA), and then the signal was amplified by a radiofrequency power amplifier (75A250A; Amplifier Research, Souderton, PA, USA). The acoustic wave was transmitted to the Eppendorf tube directly by a removable cone filled with degassed water. This experiment was composed of four groups: control (without PLD), PLD alone, PLD + cU (continuous-wave ultrasound), and PLD + pU (pulsed-wave ultrasound). For the PLD + pU group, a pulse repetition frequency (PRF) of 1000 Hz and a duty cycle of 50% were used. The sonication duration was 3 min and the acoustic power was 0.4 W for both the PLD + cU and PLD + pU groups. After sonication, tumor cells were incubated in a 12-well plate for 2 h in an incubator. An inverted fluorescence microscopy (Axiovert 200 M; Carl Zeiss Ltd., Oberkochen, Germany) was used to observe the PLD distribution in tumor cells after ultrasound sonication.
2.2.3. Preparation of tumor cells and the brain tumor model
All the experimental protocols were approved by the Institution of Animal Care and Use Committee, College of Medicine, National Taiwan University. Eight-week-old female BALB/c mice were housed with a 12-h light/dark cycle and allowed free access to water and standard diet. The mice were anesthetized by 1–3% isoflurane during the tumor implantation surgery. A total of 2 × 104 of 4T1-luc2 tumor cells suspended in 2 μL of phosphate buffered saline (PBS) were slowly injected at a rate of 2 μL/min into the right caudate putamen (0.5 mm anterior and 2.0 mm lateral to the bregma at a depth of 3 mm from the dura) over a 1-min duration. The needle was stayed for 5 min and then withdrawn for 1 min. The incision was sewn up with 6-0 polydioxanone suture.
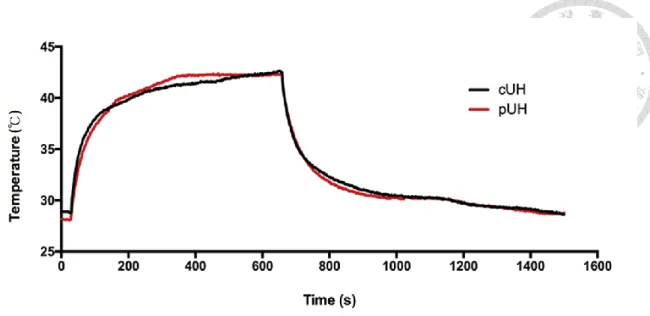
2.2.4. Focused ultrasound (FUS) system and pulsed-waved FUS hyperthermia Ultrasound was generated by a 500-kHz single-element focused transducer whose half-maximum pressure amplitude diameter and length of the focal zone were 3 mm and 8 mm, respectively. The radiofrequency signal was supplied by a function generator and then the signal was amplified by a radiofrequency power amplifier. The FUS was precisely targeted using a stereotaxic apparatus (Stoelting, Wood Dale, IL, USA). The center of the focal spot was approximately 3 mm below the cone tip. In the experiments, we used two types of ultrasound parameters to achieve ultrasound hyperthermia. Table 2-1 shows the detail of the parameters used for continuous-wave ultrasound hyperthermia (cUH) and pulsed-wave ultrasound hyperthermia (pUH). Fig. 2-1 shows the temperature responses at the focal zone measured with T-type thermocouple during cUH and pUH. The cumulated thermal doses (CEM43°C) for both cUH and pUH are less than 2 min.
2.2.5. Experimental grouping
The in vivo experiments included two parts: part 1, tumor growth responses to various therapeutics (Fig. 2-2A); and part 2, quantification or immunofluorescence of PLD in normal brain and tumor tissues (Fig. 2-2B). Totally 55 mice were used for the PLD quantification and treatment studies. To examine the treatment efficacy, we used 25 mice randomly divided into five groups: 1) control (n = 5), 2) PLD alone (n = 5), 3) pUH alone (n = 5), 4) PLD + cUH (n = 5), and 5) PLD + pUH (n = 5). To quantify the amount of PLD deposited in the normal brain and tumor tissues, we used 30 mice randomly divided into six groups: 1) normal brain without hyperthermia (n = 5), 2) normal brain with cUH (n = 5), 3) normal brain with pUH (n = 5), 4) brain tumor without hyperthermia (n = 5), 5) brain tumor with cUH (n = 5), and 6) brain tumor with pUH (n = 5). The PLD was injected as a bolus (5 mg/kg) approximately 1 min before ultrasound hyperthermia.
2.2.6. Quantification of PLD entering the normal brain and tumor tissues
To investigate whether doxorubicin delivery was enhanced by continuous-wave or pulsed-wave ultrasound hyperthermia, a dose of 5 mg/kg PLD was administered through the tail vein on day 6 after tumor implantation with or without hyperthermia. To flush the PLD in the cerebral vessels, the brain was perfused with normal saline via a transcardial method 24 h after the PLD administration. The amounts of doxorubicin deposited in tissues were then quantified as our previous study [29]. To correct for background fluorescence, the samples were compared with standard curve data from the fluorescence emission of known amounts of doxorubicin added to acidified isopropanol extracts of homogenized tumor tissue from untreated mice. The concentration of doxorubicin was measured using a fluorometer (excitation at 470 nm and emission at
590 nm) (SpectraMax M2; Molecular Devices, Sunnyvale, CA, USA).
2.2.7. Measurement of tumor growth by in vivo imaging system (IVIS) and mouse survival
The mice were anesthetized with isoflurane and then D-luciferin (Gold Biotechnology Inc., St Louis, MO, USA) was intraperitoneally injected (150 mg/kg) at 10 min before imaging. The mice were imaged with an IVIS® Spectrum, and bioluminescent signals were quantified using Living Image 3.0 (Caliper Life Sciences, Alameda, CA, USA). Images were taken every other day starting from day 5 and continuing up to day 15 after tumor implantation. The treatment was performed on day 6 after tumor implantation when the measured bioluminescent value reached approximately 106 photons/s. The survival time of tumor-bearing mice was also evaluated. The survival data were analyzed by using log-rank test in the Kaplan-Meier analysis method and summarized by a means of median survival times with their 95%
confidence intervals.
2.2.8. Immunofluorescence and PLD distribution
Immunofluorescence staining was accomplished on day 7 post-implantation. The mice were sacrificed, perfused with saline and then phosphate buffer containing 4%
paraformaldehyde to fix the brain tissues. The brains were immersed with 4%
paraformaldehyde at 4 °C overnight, and then moved to 30% sucrose solution at 4 °C for 2 days. The brains were sequentially sliced to a thickness of 20 μm. Three representative slices for the maximal tumor area were taken for each group. For immunofluorescence analysis, tissue slices were pretreated with 4% formaldehyde and permeabilized with 20 μg/mL proteinase K and 0.2% Triton X-100 in PBS. The slides
were then mounted with a solution containing blue 4’,6-diamidino-2-phenylindole (DAPI) (Sigma, St Louis, MO, USA) and labeled with the PKH67 Green Fluorescent Cell Linker Kit (Sigma, St. Louis, MO). Doxorubicin fluorescent detection was carried out with a green excitation/red emission filter using a confocal microscope (Axio Imager A1; Carl Zeiss Ltd., Oberkochen, Germany). All images were captured using the same exposure time. The pictures were merged using AxioVision Rel. 4.8 software (Carl Zeiss Ltd., Oberkochen, Germany).
2.2.9. TUNEL assay
Tumor sections were processed for the terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) assay using a DeadEnd Fluorometric TUNEL system (Promega, Madison, WI, USA) following the manufacturer’s instructions. Briefly, the slides were fixed with 4% formaldehyde and permeabilized with 20 μg/mL proteinase K and 0.2% Triton X-100 in PBS. The slides were then labeled with a TdT reaction mixture for 60 min in a 37 °C incubator and mounted with a mounting solution containing DAPI. Fluorescence images of apoptotic cells (green) and cell nuclei (blue) were obtained using a confocal microscope with the fluorescein isothiocyanate-DAPI setting. All images were captured using the same exposure time. The pictures were also merged using AxioVision Rel. 4.8 software.
2.2.10. Statistical analysis
All values are displayed as mean ± SEM (standard error of the mean). The results were analyzed with one-way analysis of variance with the post hoc Dunnet test.
Statistical significance was defined as p < 0.05. Calculations were processed on a personal computer using SPSS version 20.0 (SPSS Inc., Chicago, Illinois, USA).
2.3. Results
2.3.1. Pulsed-wave ultrasound better enhanced PLD delivery into tumor cells To investigate the effect of ultrasound sonication on PLD delivery into tumor cells, we utilized fluorescence microscopy to detect the PLD distribution. Fig. 2-3 showed that PLD delivery was enhanced by both pulsed-wave and continuous-wave ultrasound, and it displayed that pulsed-wave ultrasound could produce a much higher PLD deposition in tumor cells than continuous-wave ultrasound.
2.3.2. Low-dose pulsed-wave ultrasound hyperthermia enhanced the antitumor action in brain tumors
To investigate the effect of low-dose focused ultrasound hyperthermia (UH) on the anti-cancer action of PLD for brain tumor-bearing mice, a single treatment was executed on day 6 after tumor implantation. Tumor progression was then evaluated by an in vivo imaging system (IVIS) every other day starting from day 5. A dose of 3.5 mg/kg PLD was injected through tail vein before ultrasound hyperthermia. Fig. 2-4A showed the representative images of the bioluminescent signals, indicating that the photons increased exponentially in the control group. The PLD group and the pulsed-wave UH (pUH) alone group had a similar tumor growth pattern. In addition, the signal pattern for the PLD + cUH group (PLD plus continuous-wave UH (cUH)) showed a better inhibition of tumor growth than the PLD and pUH groups. As compared with the PLD + pUH group, the tumor inhibition was markedly better for PLD + pUH than PLD + cUH.
Fig. 2-4B showed the results of the temporal bioluminescent response, indicating that the tumors treated with PLD + pUH were significantly inhibited on day 13 as compared with the PLD + cUH group. On day 15, the brain tumors in the other treatment groups
skull would lead to overestimated photon intensities, and hence there was only the PLD + pUH group shown on day 15.
Fig. 2-5 showed the survival response of the brain tumor-bearing mice treated with different therapeutics. The treatment with PLD + pUH led to a significantly improved survival time for the tumor-bearing mice, as compared with the control, PLD, pUH, and PLD + cUH groups. The median survival times for the mice treated with PLD, pUH, PLD + cUH or PLD + pUH were 16, 16, 17, 22 days, respectively, much longer than the control group (11 days). The prolonged survival time for the pUH group (same survival time as the PLD group) indicated that low-dose pulsed-wave focused ultrasound hyperthermia could damage brain tumors and result in a longer survival time than the control group. The prolonged survival time of the PLD + pUH group indicated that low-dose pulsed-wave ultrasound hyperthermia could both damage brain tumors and effectively enhance PLD delivery into the sonicated tumor cells/tissues to achieve the best anti-tumor activity.
2.3.3. PLD delivery to normal brain and tumor tissues by low-dose pulsed-wave/continuous-wave ultrasound hyperthermia
Fluorometry was used to measure the doxorubicin from the PLD deposited in the normal brain and tumor tissues for the mice with/without low-dose continuous-wave/pulsed-wave ultrasound hyperthermia. Fig. 2-6 showed the concentration of doxorubicin in the normal brain and tumor tissues 24 h after an injection of 5 mg/kg PLD. The doxorubicin concentration was significantly greater in the tumors treated with PLD + pUH than those in the tumors treated with PLD + cUH or PLD alone. This suggested that low-dose pulsed-wave ultrasound hyperthermia had the ability to significantly increase the PLD transport into the sonicated tumor tissues. This
figure also showed that there was no obvious difference of the PLD concentration in normal brain tissues among these three groups.
2.3.4. Immunofluorescence detection of PLD deposition
Fluorescence microscopy was used to study the deposition of the fluorescent PLD in tumor tissues for the PLD, PLD + cUH, and PLD + pUH groups 24 h after PLD injection. Labeling marker PKH67 (green color) was used to identify the cell membrane.
Fig. 2-7, the results of immunofluorescence staining for tumor tissues, showed that the tumor sections for the PLD + pUH group had a more enriched doxorubicin (red color) accumulation than those for the PLD and PLD + cUH groups. The doxorubicin depositions were consistent with the quantification results of brain tumor tissues (Fig.
2-6).
2.3.5. TUNEL staining for apoptotic cancer cells in the tumors
To further assess the antitumor effect, TUNEL staining was performed to detect apoptotic cells in the tumors. Fig. 2-8 showed that the PLD + pUH group had the strongest TUNEL-positive signal among the PLD, PLD + cUH, and PLD + pUH groups, indicating that there were much more apoptotic cancer cells by applying a low-dose pulsed-wave ultrasound hyperthermia after PLD injection.
2.4. Discussion
In this study, we demonstrated in the in vitro study that short-time pulsed-wave ultrasound (pU) could enhance the PLD delivery into breast cancer cells more effectively than continuous-wave ultrasound (cU) under the same acoustic power and sonication duration (Fig. 2-3). In addition, we also showed in the in vivo study that low-dose pulsed-wave ultrasound hyperthermia (pUH) could result in a higher deposition of PLD in brain tumors than continuous-wave ultrasound hyperthermia (cUH) under the same acoustic power and sonication duration (Fig. 2-6 and Fig. 2-7). The combined effects of pulsed-wave ultrasound and ultrasound hyperthermia significantly improve the PLD delivery into the sonicated tumor tissues and cancer cells to produce a boosted cytotoxicity to inhibit the tumor growth (Fig. 2-4B and Fig. 2-8) and produce a higher survival for brain tumor-bearing mice (Fig. 2-5).
In a fluid or soft tissues, ultrasound propagates as a longitudinal wave of alternate compressions and rarefactions and it may cause direct mechanical effects on the sonicated tissues and cells. The alternate compressions and rarefactions of ultrasound may produce a slight oscillation of fluid and tissues, which might increase cell membrane permeability [32] and molecular transport by altering molecular motion [42].
In addition, a phenomenon called acoustic streaming occurs when the momentum of the sound waves transfers to an absorbing fluid, thus generating convective flow in the direction of the propagating ultrasonic waves. These phenomena may enhance cell membrane permeability and the transport of nanodrug into the sonicated cells to produce a higher concentration of PLD in the cancer cells as shown in Fig. 2-3 (the difference between the PLD group and the PLD + cU group).
There are several mechanisms whereby ultrasound sonication may be involved in drug delivery with/without the presence of microbubbles. In this study, we employed
focused ultrasound to produce localized hyperthermia and modulated the ultrasound as a pulsed-wave form with a pulse repetition frequency (PRF) of 1000 Hz without an injection of microbubbles. This pulsed-wave ultrasound would produce a repetitive radiation pressure with a gradient around several Pa/mm on the sonicated tumor tissues and cancer cells. As a result, this repetitive radiation pressure would make the sonicated tumor tissues and cancer cells moving forwards and backwards. This may be the main reason for the in vitro experimental results showing that pulsed-wave ultrasound (pU) can produce a better cell membrane permeability and transport of nanodrug into the cancer cells to have a higher concentration of PLD in the sonicated cancer cells as shown in Fig. 2-3 (the difference between the PLD + cU group and the PLD + pU group). Similarly, pulsed-wave ultrasound hyperthermia improves the transport of PLD into the sonicated tumor tissues and gives an impact on the cancer cell membranes to have a better delivery of PLD into cancer tumors as shown in Fig. 2-4. Here, we demonstrated that the combined effects of pulsed-wave ultrasound and low-dose ultrasound hyperthermia could significantly improve the nanodrug delivery into the sonicated tumor and cancer cells to boost the cytotoxicity and the inhibition of tumor growth as shown in Fig. 2-4, Fig. 2-6 (the difference between the PLD + cUH group and the PLD + pUH group). Further study is necessary to optimize the ultrasound parameters, such as PRF, duty cycle, etc. and to visually examine the impact of pU on cell membrane functions.
The mechanical effects of alternate compressions and rarefactions of ultrasound sonication on the cell membrane may cause membrane deformation, poration, or sometimes lysis even in the absence of transient cavitation [32,56]. It reported that tumor suppressor protein, p53, might affect the integrality of the cell membranes. Tumor cells lacking functional p53 would show lower elasticity and higher deformability [57],
and their membrane might be much more sensitive to a pulsed-wave ultrasound with a repetitive radiation pressure of a gradient around several Pa/mm during sonication. In Fig. 2-4, the pUH group exhibits a similar therapeutic response as the PLD alone group and this phenomenon might relate to the impact of pulsed-wave ultrasound on the sonicated cancer cells. In addition, ultrasound sonication may affect the cell cycle progression temporarily at early time points (first 12 h post sonication) and then diminish by 24 h [58]. In this study, in vitro experimental results (Fig. 2-3) and in vivo experimental results (Fig. 2-6, Fig. 2-7) demonstrated that pulsed-wave ultrasound has an additional mechanical effect on the cancer cell membrane to result in a better accumulation of PLD in the sonicated cancer cells and tumor tissues than conventional continuous-wave ultrasound. The above causes might be the reasons of the better therapeutic efficacy for pUH than cUH under the same acoustic power and sonication duration.
Doxorubicin concentrations in tumor and normal brain tissues (Fig. 2-6) showed that there was no significant difference of PLD deposition in the sonicated normal brain tissues for both cUH and pUH. It is well-known that an intact blood-brain barrier prevents chemotherapeutics entering the parenchyma, and in this study the maximum temperature rise (∼43 °C) and the resulting thermal dose (CEM43°C < 2 min) for both cUH and pUH were much lower than the threshold values (48 °C, CEM43°C = 12.8 min) for thermally induced blood-brain barrier disruption and brain tissue damage [59].
Hence, this type of low thermal dose ultrasound sonication would not produce any damage to the normal brain tissues or increase nanodrug delivery into the sonicated normal brain tissues. On the other hand, the BTB/BBB in the brain tumor tissue is partially leaky due to the invading of tumor cells into the brain parenchyma to alter vascular permeability. As the brain tumor grows, the enhanced permeability and
retention (EPR) effect occurs but this effect in brain tumors is still weak. Ultrasound hyperthermia can locally increase the sonicated brain tumor temperature, leading to increased perfusion, vascular permeability, and interstitial micro-convection in the heated tumor region; and hence both cUH and pUH have an enhanced PLD deposition in the sonicated tumor region. In this study, the experimental results further demonstrated that pulsed-wave ultrasound hyperthermia not only could heat brain tumors but also could make BTB more permeable for the PLD delivery into the sonicated tumors to achieve a significantly better therapeutic efficacy.
2.5. Conclusions
The blood-brain barrier/blood-tumor barrier (BBB/BTB) is an obstacle for the delivery of chemotherapeutic agents to the brain tumor. In this study, both in vitro and in vivo experimental results demonstrated that pulsed-wave ultrasound and low-dose
ultrasound hyperthermia could significantly enhance the PLD delivery into the sonicated cancer cells and tumor tissues than conventional continuous-wave ultrasound and ultrasound hyperthermia under the same acoustic power and sonication duration without damaging normal brain tissues. The results indicate that this pulsed-wave ultrasound hyperthermia technology can be very useful in delivering nanodrugs for the treatment of various types of brain cancer tumors.
Table 2-1. Ultrasound parameters used in the in vivo experiments to perform continuous-wave ultrasound hyperthermia (cUH) or pulsed-wave ultrasound hyperthermia (pUH).
Continuous-wave Ultrasound Hyperthermia (cUH)
Pulsed-wave Ultrasound Hyperthermia (pUH)
Frequency (MHz) 0.5 0.5
Peak Negative
Pressure (MPa) 0.97 1.37
Pulse Repetition
Frequency (Hz) N/A 1000
Duty Cycle (%) 100 50
Duration (min) 10 10
Acoustic Power (W) 2.22 2.22
Figure 2-1. Typical temperature responses were measured at the focal zone with continuous wave or pulsed wave ultrasound sonication over time.
Figure 2-2. (A) Time course for the therapeutic experiments. 4T1 cancer cells were implanted on day 0, and the treatments were performed on day 6 with PLD injection, and/or continuous-wave ultrasound hyperthermia (cUH) or pulsed-wave ultrasound hyperthermia (pUH). IVIS imaging was performed on day 5, 7, 9, 11, 13 and 15. (B) Schedule for doxorubicin (Dox) quantification or immunofluorescence (IF) after different therapeutics.
Figure 2-3. Immunofluorescence staining for in vitro investigation of PEGylated liposomal doxorubicin (PLD) up-taken by 4T1 breast tumor cells with or without ultrasound sonication. Fluorescence staining of tumor cells was performed 2 h after different therapeutics: 1) control: no treatment; 2) PLD: PLD alone; 3) PLD + cU: PLD plus continuous-wave ultrasound sonication; 4) PLD + pU: PLD plus pulsed-wave ultrasound sonication. A dose of 3 μg/ml PLD was used in this experiment and the sonication duration was 3 min for both continuous- and pulsed-wave ultrasound with the same acoustic power (0.4 W). Red, blue and green colors represent PLD, cell nuclei and cell membrane, respectively. Scale bar = 200 μm.
Figure 2-4. (A) Representative IVIS imaging and (B) bioluminescent signal quantification of mouse brain tumors from day 5 to day 15 after tumor implanted. Mice were implanted with luciferase-expressing 4T1-luc2 breast cancer cells in the brains.
Bioluminescent signals were quantified using an IVIS imaging system. Treatment was
executed on day 6 after tumors implanted, and images were obtained every other day.
There were five groups: Control (no treatment), PLD, pUH (pulsed-wave ultrasound hyperthermia), PLD + cUH (continuous-wave ultrasound hyperthermia), and PLD + pUH. A dose of 3.5 mg/kg PLD was used and the ultrasound parameters used were shown in Table 1. The arrow indicates the time point for different therapeutics performed. Note that PLD + pUH markedly inhibited the brain tumor growth. Data are presented as mean ± SEM (n = 5 for each group). *Represents p < 0.05, the comparison between the PLD + pUH group and the PLD + cUH group.
Figure 2-5. Kaplan-Meier survival curves of tumor-bearing mice with different therapeutics. PLD + pUH significantly increased the lifespan of tumor-bearing mice.
Figure 2-6. Doxorubicin concentrations in tumor and normal brain tissues for mice with/without continuous-wave ultrasound hyperthermia (cUH) or pulsed-wave ultrasound hyperthermia (pUH). Mice were implanted with 4T1-luc2 murine breast cancer cells on day 0 and were injected with a dose of 5 mg/kg PLD with/without transcranial cUH or pUH on day 6 after tumor implanted. Note that pUH significantly enhanced the accumulation of PLD in the tumor tissues than cUH. In addition, both cUH and pUH did not elevate the PLD concentration in the normal brain tissues. Data are presented as mean ± SEM (n = 5 for each group). *Represents p < 0.05.
Figure 2-7. Immunofluorescence staining in the tumor regions after different therapeutics. Mouse brains were implanted with 4T1-luc2 tumor cells and the treatments were performed 6 days after tumors implanted. In these experiments, a dose of 15 mg/kg PLD was i.v. injected. The mice were sacrificed 24 h after the treatment and then the brain tissues were stained with DAPI to visualize the tumor cell nuclei (blue) and with PKH67 to show the cell membrane (green). Tumors treated with PLD + pUH had the strongest red fluorescence expression and the deposition of doxorubicin was near the cell nuclei. Scale bars: 50 μm.
Figure 2-8. TUNEL staining was used to detect apoptotic cells in tumor tissues. Mouse brains were implanted with 4T1-luc2 tumor cells and the treatments were performed 6 days after tumors implanted. A dose of 3.5 mg/kg PLD was i.v. administered for these experiments. The mice were then sacrificed 24 h after the treatments and then brain tumor slices were obtained for staining. Tumor slices were firstly stained with terminal TUNEL (green) and then with DAPI to visualize the tumor cell nuclei (blue). The strong apoptotic signal was observed in the PLD + pUH group. Scale bar: 100 μm.
Chapter 3. Pulsed-wave Ultrasound Hyperthermia Enhanced Nanodrug Delivery Combined with Chloroquine Exerts
Effective Antitumor Response and Postpones Recurrence
3.1. Introduction
Autophagy is a catabolic process that turns over old proteins and organelles, allows cells to recycle cellular components and provides required energy [33,34]. It is a key component in maintaining homeostasis of cellular environment. Autophagy also plays a crucial role in cancer pathophysiology. It is believed that autophagy prevents cancer development, but helps cancer cells within an already established tumor to survive from stress and threats [33,34,35,36,37,38]. Therefore, autophagy inhibition has been investigated as an evolving strategy to fight against advanced cancer [37,38,39].
Chloroquine (CQ) and its analogue hydroxychloroquine (HCQ) are widely used anti-malarial drugs. They inhibit lysosomal acidification and hence block the formation of autophagosome as well [37]. In addition to autophagy inhibition, CQ was reported to possess multiple mechanisms to fight against cancer, including targeting against cancer stem cells (CSC) [40] and inducing tumor vessel normalization [41]. The link between CQ and cancer can be traced to 1980s, a malaria suppression program carried out in Tanzania utilizing CQ were found accompanied with a significant decline in Burkitt's lymphoma within the period of CQ distribution program [60]. There were several ongoing clinical trials using CQ (or HCQ) additional to conventional chemotherapeutic agents to treat various kinds of cancer, including colorectal cancer, glioblastoma, and pancreatic cancer [38].
Hyperthermia has been used to treat many kinds of cancer for decades, either
monotherapy or in combination with other anti-cancer therapy. The synergistic effect between hyperthermia and chemotherapeutic agents such as doxorubicin was well-known [15]. Furthermore, localized hyperthermia increases blood flow and vascular permeability in the heated tumor region, and therefore enhances the delivery of nanodrug into cancer cells [26]. Ultrasound was investigated as a modality to induce hyperthermia and was found advantageous over other thermal sources for its noninvasiveness and penetrating ability into deep tissues [25].
Previous studies [29,61] showed that short-time pulsed-wave ultrasound hyperthermia (pUH) not only enhanced the delivery of PLD but also elicited inhibitory effect directly on cancer cells. However, in some cases the cancer tumors were macroscopically destroyed by the combined therapy of PLD+pUH, they still recurred several days or weeks after the treatment.
The aim of present study was to investigate an effective strategy to successfully treat tumor, prevent tumor recurrence, and improve the disease-free survival. We evaluated the combination treatment of PLD+pUH with constant CQ administration to see if it successfully suppressed tumor growth and prevented recurrence. The concept of therapy and design of experiment was schemed in Figure 3-1 and Figure 3-2, respectively. We found that pUH enhanced PLD delivery in combination with CQ could persistently suppress 4T1 tumor growth and postpone its recurrence.