科技部補助專題研究計畫成果報告 期末報告
藥物基因組學分析強直性脊柱炎患者 TNFα-受體阻滯劑治 療的反應預測
計 畫 類 別 : 個別型計畫
計 畫 編 號 : NSC 102-2314-B-040-017-
執 行 期 間 : 102 年 08 月 01 日至 103 年 07 月 31 日 執 行 單 位 : 中山醫學大學醫學研究所
計 畫 主 持 人 : 魏正宗 共 同 主 持 人 : 張偉嶠
處 理 方 式 :
1.公開資訊:本計畫涉及專利或其他智慧財產權,1 年後可公開查詢 2.「本研究」是否已有嚴重損及公共利益之發現:否
3.「本報告」是否建議提供政府單位施政參考:否
中 華 民 國 103 年 10 月 31 日
中 文 摘 要 : 僵直性脊椎炎是一種慢性脊椎及關節發炎性疾病,遺傳因 素,特別是 HLA-B27 基因及 HLA-B60 基因是最主要的致病基 因。
本研究主要調查 HLA-B27 基因及 HLA-B60 基因的交互作用,
同時比較這兩個基因在僵直性脊椎炎病人及正常控制組之基 因型差異。研究納入 471 位僵直性脊椎炎病人及 558 位年 齡、性別配對正常之臺灣人為控制組。基因型的檢定以 PCR 測定。
結果顯示,與 B27 陰性/B60 陰性之控制組來比較,發現 B27 陽性-B60 陰性之族群罹患僵直性脊椎炎的勝算比為 152 倍;
而 B27 陽性/B60 陽性之族群罹患僵直性脊椎炎之族群勝算比 高達 201 倍。將此兩個基因以結合分析之統計模式,計算出 的相對過多危險值 R1RI 為 64%。貢獻比例(AP)為 0.23,協同 指數(S)為 1.3。
結論: HLA-B27 及 HLA-B60 的基因交互作用增加臺灣人族群 罹患僵直性脊椎炎之可能性
中文關鍵詞: 僵直性脊椎炎,基因交互作用, HLA-B27, HLA-B60 英 文 摘 要 : Ankylosing spondylitis (AS) is a form of chrnic
inflammatory spondyloarthritis (SpA) that causes pain and stiffness in spines or joints. HLA-B27 and HLA- B60 have been reported as major genetic risk factors of AS. To test whether the interaction between HLA- B60 and HLA-B27 can serve as a better predictor of AS, 471 patients with AS and 558 healthy subjects were genotyped in a Taiwanese population. Combined risk factors were investigated to test the biological interaction. Our results indicated that the relative risk (RR) for HLA-B27+/HLA-B60? was 152 (85% CI 91 to 255) and it increased to 201 (95% CI 85 to 475) in HLA-B27+/HLA-B60+ patients (compare with HLA-
B27?/HLA-B60? as reference). Combinational analysis of two risk factors (HLA-B27+/HLA-B60+) showed a relative excess risk due to interaction (RERI) of 47%, attributable proportion (AP) of 0.23 and a synergy index (S) of 1.3. In conclusion, genetic interaction between HLA-B60 and HLA-B27 increased risk of AS in a Taiwanese population.
英文關鍵詞: Ankylosing spondylitis, gene interaction, HLA-B27, HLA-B60
1
Interaction between HLA-B60 and HLA-B27 as a predictor of ankylosing spondylitis in a Taiwanese population
1Division of Allergy, Immunology and Rheumatology, Department of Medicine, Chung Shan Medical University Hospital, Taichung, Taiwan; 3Institute of Medicine, Chung Shan Medical University, Taichung, Taiwan; 3Department of Clinical Pharmacy, School of Pharmacy, Taipei Medical University, Taipei, Taiwan; 4 Master Program for Clinical Pharmacogenomics and Pharmacoproteomics, School of Pharmacy, Taipei Medical University, Taipei, Taiwan.
5Institute of Medicine, Chung Shan Medical University, Taichung, Taiwan; 6Department of Rheumatology, Leiden University Medical Center, Leiden, The Netherlands; and
7Department of Pharmacy, Taipei Medical University-Wanfang Hospital, Taipei, Taiwan.
*Ya-Feng Wen, James Cheng-Chung Wei, Wong Sung-Ching Henry and Yu-Wen Hsu contributed equally to this work.
2
Abstract
Ankylosing spondylitis (AS) is a form of chrnic inflammatory spondyloarthritis (SpA) that causes pain and stiffness in spines or joints. HLA-B27 and HLA-B60 have been reported as major genetic risk factors of AS. To test whether the interaction between HLA-B60 and HLA-B27 can serve as a better predictor of AS, 471 patients with AS and 558 healthy subjects were genotyped in a Taiwanese population. Combined risk factors were investigated to test the biological interaction. Our results indicated that the relative risk (RR) for HLA- B27+/HLA-B60− was 152 (85% CI 91 to 255) and it increased to 201 (95% CI 85 to 475) in HLA-B27+/HLA-B60+ patients (compare with HLA-B27−/HLA-B60− as reference).
Combinational analysis of two risk factors (HLA-B27+/HLA-B60+) showed a relative excess risk due to interaction (RERI) of 47%, attributable proportion (AP) of 0.23 and a synergy index (S) of 1.3. In conclusion, genetic interaction between HLA-B60 and HLA-B27 increased risk of AS in a Taiwanese population.
3
Introduction
Ankylosing spondylitis (AS) is a rheumatoid rheumatic disease leading to pain, stiffness and possible fusion of spinal segments. It is considered as a chronic, inflammatory disorder and affects sacroiliac joints, lumbar spine, and peripheral joints1. Progression of disease in AS patients often leads to limited of mobility, functional impairment and finally affects the patients’ well-being2. Prevalence of AS in men is higher than in women3, while the pathological mechanisms of AS remain unclear.
A genome-wide association study (GWAS) conducted by The Australo-Anglo-American Spondyloarthritis Consortium (TASC) revealed the association of HLA-B27, IL-23 and IL-1 genes to AS5. Another GWAS in Han populations also confirmed the important role of HLA- B27 in AS 6. Although HLA-B27 gene is the best-known genetic susceptibility marker for AS, it only explain for 16% of the genetic variability in AS7. Associations between AS and the HLA-B27 gene and HLA-B60 gene have also been revealed8. In addition, Wei et al., showed that HLA-B60 is a risk factor for HLA-B27 negative patients9.
In 2013, epistasis between HLA-B27 and HLA-B60 has been reported to associate with increased risk of AS in Caucasians, with a very high relative excess risk10. However, the role of genetic interaction between HLA-B27 and HLA-B60 in Asia population remains unknown.
In this study, we investigated the correlation between HLA-B27 and HLA-B60 and the risk of AS. We also further tested whether HLA-B27 and HLA-B60 interaction contributes to the disease severity of AS in a Taiwanese population.
4
Materials and Methods Subject recruitment
The patients with AS and the healthy subjects were from the Chung Shan Medical University Hospital. AS patients who met the New York AS diagnosis criteria were recruited to participate. Our study was approved by the institutional review boards of the hospital.
Informed consent was obtained before any data were collected from the subjects. The Bath AS Disease Activity Index (BASDAI), Bath AS Functional Index (BASFI), and Bath AS Global (BAS-G) which evaluate disease activity, physical function, and global well-being is collected by questionnaire. Modified Chinese versions of the BASDAI, BASFI, and BAS-G showed good intra-class correlations and Cronbach’s alpha values.
DNA extraction and HLA Genotyping
DNA of blood cells were extracted by first treating them with 0.5% sodium dodecylsulfate lysis buffer and then protease K (1 mg/ml) to digest nuclear proteins for 4 h at 60 °C. Total DNA was harvested using a Gentra (Qiagen, Valencia, CA) extraction kit followed by 70% alcohol precipitation. DNA purification from buffy coat was carried out by using the Gentra Puregene Blood Kit (Qiagen, Valencia, CA, USA). HLA-B60 was genotyped by using the TaqMan® Allelic Discrimination Assay (Applied Biosystems, Foster City, CA).
A 96-well micro-plate with an ABI9700 Thermal Cycler (Applied Biosystems) is used to perform polymerase chain reaction (PCR). After PCR, fluorescence was detected and analyzed by StepOne software vers. 2.2.2 (Applied Biosystems)10. The genotype of HLA-B27 was assessed by flow cytometry as previously described11.
Data analysis
For interaction between two antigens associated with AS, HLA-B27 and HLA-B60, patients and controls were re-categorised into four strata: HLA-B27 positive or negative and
5
HLA-B60 positive or negative. With the disease risk in the HLA-B27 negative and HLA-B60 negative stratum as the reference, the ratio of the increase of risk for disease, the relative risk (RR), for the stratum with HLA-B60 but not HLA-B27 was calculated. Similarly, the RR was calculated for patients with HLA-B27 without HLA-B60. The sum and product of the increases in RR together with the background effect were then compared with the RR of the combined joint effect, that is, the RR for AS with HLA-B27 and HLA-B60 relative to the RR of AS without HLA-B27 or HLA-B60. The prevalence of AS in Taiwan is less than 0.5% and this justifies a rare disease assumption thereby equating ORs with RRs.
Interaction, defined as the deviation from additivity, was evaluated by three measures:
relative excess risk due to interaction (RERI), the attributable proportion (AP) due to interaction and the synergy index (S). These measures indicate significant interaction if they differ from 0 (RERI and AP) or 1 (synergy index). RERI can be interpreted as the excess risk due to interaction relative to the risk without exposure. AP is interpreted as the AP of disease that is due to interaction among persons with both exposures. The synergy index can be interpreted as the excess risk from exposure (to both exposures) when there is interaction, relative to the excess risk from exposure (to both exposures) without interaction. To obtain the parameter estimates needed for calculating these three measures, a logistic regression model was fitted12. The Statistical Package for the Social Sciences (SPSS), V. 20.0 (SPSS, Chicago, Illinois, USA), was used to analyse the data. In all tests, p values less than 0.05 were considered significant.
6
Results
As shown in Table 1, a total of 1028 subjects were recruited including 471 patients with AS, and 558 healthy subjects. The number of male in AS patients and control subjects was 320 (67.9%) and 435 (78.0%). The mean of age in both groups were 39.0 years. HLA- B27 and HLA-B60 genotype data were collected from both patients and control subjects. 431 (91.5%) AS patients and 133 (23.8%) control subjects were HLA-B27+. Besides, the number of HLA-B60+ was 102 (21.7%) and 69 (12.4%), respectively.
We further assessed the independent effect and gene-gene interaction effect of HLA- B27 and HLA-B60 to AS susceptibility by categorizing our samples into four groups: HLA- B27+/HLA-B60+, HLA-B27+/HLA-B60-, HLA-B27-/HLA-B60+, HLA-B27-/HLA-B60-.
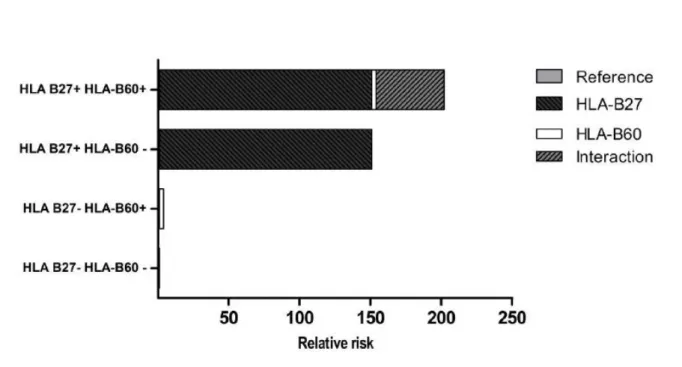
Samples with HLA-B27-/HLA-B60- were considered as reference. As the prevalence of AS is relatively rare in Asian (0.167%), odds ratio was calculated to substitute relative risk in this study. Figure 1 showed that both HLA-B27 and HLA-B60 were disease-susceptibility gene for AS, with odds ratio (OR) 152 (95% confidence interval (CI) 91 to 255, fisher’s-exact p=0.0072) and OR 2.9 (95% CI 1.4 to 6.0, fisher’s exact p=1.222×10-157) respectively. With HLA-B27−/HLA-B60− as the reference, patient who carried both HLA-B27 and HLA-B60 (HLA-B27+/HLA-B60+) showed a high susceptibility to AS, with the OR increased to 201 (95% CI 85 to 475, fisher’s exact p=2.5007×10-69).
To confirm the independent effect of HLA-B27 and HLA-B60 to AS susceptibility, logistic regression analysis was performed. Results indicated that three genetic risk factor combinations were independent risk factor for AS (HLA-B27+/HLA-B60+ and HLA-B27 + /HLA-B60 –: P<0.001 and HLA-B27 – /HLA-B60 +: P=0.0038) (Table 2).
The risk for AS in HLA-B27+/HLA-B60+ exceeded the sum of the risks (201 >
(152+2.9)) in HLA-B27−/HLA-B60+ and HLA-B27+/HLA-B60− (Figure 1) but not the product of the risks (201 < (152×2.9)). Calculated biological interaction measures showed a
7
departure from additivity of the two risk factors combined (HLA-B27+/HLA-B60+) with a RERI of 47%, AP of 0.23 and S of 1.3. These results confirmed the gene-gene interaction effect between HLA-B27 and HLA-B60 in Taiwanese population.
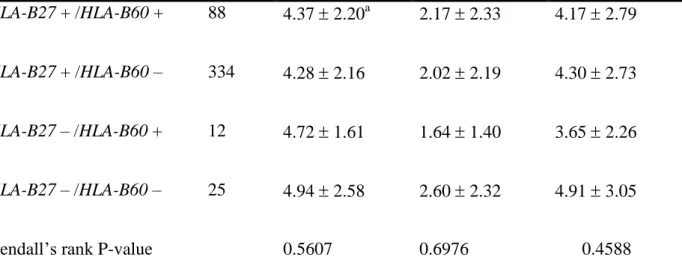
In order to investigate the association between HLA antigens and AS severity, further analysis was conducted. We investigated whether HLA-B27 or HLA-B60 associated with clinical phenotypes including Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functional Index (BASFI), and Bath Ankylosing Spondylitis Global Index (BAS-G), which represent disease activity, physical function, and global well-being respectively. Although interaction effect between HLA-B27 and HLA-B60 to AS susceptibility has been detected, no association between HLA-B27 or HLA-B60 and AS disease severity was observed (Table 3).
8
Discussions
Susceptibility to autoimmune disease like AS is inherited as a polygenic trait, and is characterized by abnormal immune activation. HLA has been known to involve in the antigen recognition process and is a well-known susceptibility factor for the pathogenesis of AS.
HLA-B27 is considered as the major susceptibility factor of AS8,12-13. HLA-B27 is a highly polymorphic gene, with 105 subtypes: HLA-B*27:01 to HLA-B*27:10614-15. Indeed, comparison of HLA-B27–/HLA-B60– group and HLA-B27+/HLA-B60– group (Figure 1), our results confirmed that HLA-B27 plays an important role in the Taiwanese AS patients.
HLA-B27 and HLA-B60 genes are located on chromosome 6p21.3, both coding proteins involve in antigen presenting function. HLA present endogenous antigens to T-cells and further trigger the autoimmune responses. Recent studies suggested that peptide motifs of HLA-B60 may different from HLA-B2716-18, thus these HLA-B subtypes might involve in different antigen-triggered pathologic pathways. To measure biological interaction between HLA-B27 and HLA-B60, we calculated three parameters that measure the departure from additivity of risk effects of each risk factor, i.e. RERI, the relative excess risk due to attributable to HLA-B27 and HLA-B60 interaction; AP[AB]: the proportion of AS among those with both exposures that is attributable to HLA-B27 and HLA-B60 interaction; and synergy index, which measures the interaction between two risk factors expressed as the ratio of relative excess risk for the combined effect of the risk factors and the sum of the relative excess risks for each separate effect of the two risk factors. These three indices were calculated from risk ratio. Under the criteria that disease prevalence was rare (the mean AS prevalence was 0.167 in Asia19). The value of odds ratio would approximate the value of risk ratio. Thus in our study, odds ratio were calculated to estimate the value of risk ratio, and
9
further, calculate the value of RERI, AP and S. Our results showed a departure from additivity of the two risk factors combined (HLA-B27+/HLA-B60+) with a RERI of 47%, AP of 0.23 and S of 1.3.
Consistent with the Floris A van Gaalen et al (2012) study, our study confirmed that HLA-B60 can be used as an independent risk factor for AS susceptibility. In addition, it showed a strong biological interaction effect with HLA-B27. However, the difference between two studies is that our results showed that the risk ratio attributed by HLA-B27 is greater than that of HLA-B60, suggesting that HLA-B27 remains the most important genetic predictor on AS susceptibility in a Taiwanese population. While HLA-B60 displays a minor additive role. Because of the difficulties in early diagnosis of AS in Taiwan, our study revealed a possibility to the implementation of combining HLA-B60 with HLA-B27 screen in clinical practice.
Despite the strong correlation between HLA-B27 and HLA-B60 to the AS susceptibility, no correlation between HLA-B27, HLA-B60 and clinical manifestations of AS, i.e. BASDAI, BASFI, and BAS-G was observed in this study. Indeed, similar findings were observed in acrophage migration inhibitory factor (MIF) gene polymorphism22. MIF is associated with the susceptibility but not severity of polyarthritis22. In short, HLA-B27 and HLA-B60 are strong genetic determinant of susceptibility to AS. Therefore, combination of these two HLA antigens can be applied as a potential clinical tool to detect the risk of AS.
10
Conclusions
In summary, we revealed that HLA-B60 is a risk factor for AS in Taiwanese population.
We also confirmed the biological interaction effect between HLA-B27 and HLA-B60 in AS susceptibility in Taiwanese population, which is consistence with Caucasians population.
Furthermore, we have shown that polymorphism between HLA-B27 and HLA-B60 antigens are associated with susceptibility to, but not severity of AS. As a result, in the Taiwanese population individuals with the HLA-B27+/HLA-B60+ genotype have a greatly increased risk of developing AS.
ACKNOWLEDGEMENTS
Supported by the Seminar Project of New Hiring Professor from Taipei Medical University, Taiwan, ROC (TMU101-AE4-B14) and National Science Council, Taiwan, ROC (NSC101- 2628-B038-001-MY2)
11
References:
1. Braun J et al. Ankylosing spondylitis. Lancet. 2007 Apr 21;369(9570):1379-90.
2. Madsen OR et al. Reproducibility of the Bath Ankylosing Spondylitis Indices of disease activity (BASDAI), functional status (BASFI) and overall well-being (BAS-G) in anti- tumour necrosis factor-treated spondyloarthropathy patients. Clin Rheumatol. 2010 Aug;29(8):849-54
3. Calin A et al. Impact of sex on inheritance of ankylosing spondylitis: a cohort study.
Lancet. 1999 Nov 13;354(9191):1687-90.
4. Duftner C et al. Prevalence, clinical relevance and characterization of circulating cytotoxic CD4+CD28- T cells in ankylosing spondylitis. Arthritis Res Ther. 2003;5(5):R292-300.
5. Australo-Anglo-American Spondyloarthritis Consortium (TASC) et al. Genome-wide association study of ankylosing spondylitis identifies non-MHC susceptibility loci. Nat Genet. 2010 Feb;42(2):123-7.
6. Lin Z et al. A genome-wide association study in Han Chinese identifies new susceptibility loci for ankylosing spondylitis. Nat Genet. 2011 Dec 4;44(1):73-7.
7. Khan MA et al. Genetic aspects of ankylosing spondylitis. Best Pract Res Clin Rheumatol.
2002 Sep;16(4):675-90.
8. Brewerton DA et al. Ankylosing spondylitis and HLA-B27. Lancet. 1973 Apr 28;1(7809):904-7.
9. Wei JC et al. HLA-B60 and B61 are strongly associated with ankylosing spondylitis in HLA-B27-negative Taiwan Chinese patients. Rheumatology (Oxford). 2004 Jul;43(7):839- 42.
12
10. van Gaalen FA et al. Epistasis between two HLA antigens defines a subset of individuals at a very high risk for ankylosing spondylitis. Ann Rheum Dis. 2013 Jun;72(6):974-8. doi:
10.1136/annrheumdis-2012-201774.
11 Chou CT et al. The detection of the HLA-B27 antigen by immunomagnetic separation and enzyme-linked immunosorbent assay-comparison with a flow cytometric procedure. J Immunol Methods. 2001 Sep 1;255(1-2):15-22.
11. Schlosstein L et al. High association of an HL-A antigen, W27, with ankylosing spondylitis. N Engl J Med. 1973 Apr 5;288(14):704-6.
12. Andersson, T.et al. Calculating measures of biological interaction. Eur J Epidemiol 20, 575-9 (2005).
13. Brown MA. Breakthroughs in genetic studies of ankylosing spondylitis. Rheumatology (Oxford). 2008 Feb;47(2):132-7.
14. Khan MA. Polymorphism of HLA-B27: 105 subtypes currently known. Curr Rheumatol Rep. 2013 Oct;15(10):362.
15. Gran JT et al. Clinical, epidemiologic, and therapeutic aspects of ankylosing spondylitis.
Curr Opin Rheumatol. 1998 Jul;10(4):292-8.
16. Weiss EH et al. Molecular biology of the HLA-B27 locus. Br J Rheumatol. 1988;27 Suppl 2:12-8.
17. Madden DR et al. The structure of HLA-B27 reveals nonamer self-peptides bound in an extended conformation. Nature. 1991 Sep 26;353(6342):321-5.
18. Falk K et al. Peptide motifs of HLA-B58, B60, B61, and B62 molecules. Immunogenetics.
1995;41(2-3):165-8.
19. Dean LE et al. Global prevalence of ankylosing spondylitis. Rheumatology (Oxford).
2014 Apr;53(4):650-7.
13
20. Madsen OR et al. Reproducibility of the Bath Ankylosing Spondylitis Indices of disease activity (BASDAI), functional status (BASFI) and overall well-being (BAS-G) in anti- tumour necrosis factor-treated spondyloarthropathy patients. Clin Rheumatol. 2010 Aug;29(8):849-54.
21. Rachlis AC et al. A24: Validation of BASDAI and BASFI in Children with Spondyloarthritis. Arthritis Rheumatol. 2014 Mar;66 Suppl 11:S38.
22. Barton A et al. Macrophage migration inhibitory factor (MIF) gene polymorphism is associated with susceptibility to but not severity of inflammatory polyarthritis. Genes Immun. 2003 Oct;4(7):487-91.
14
Table 1 Basal characteristics of patients with ankylosing spondylitis (AS) and control subjects.
Characteristics Patients with AS Control subjects
Number of subjects 471 557
Gender: male (No (%)) 320 (67.9%) 435 (78.0%)
Age (years)a 39.0 11.3 39.0 12.2
Range 17-82 17-77
HLA-B27(+) 431 (91.5%) 133 (23.8%)
HLA-B60(+) 102 (21.7%) 69 (12.4%)
aMean SD. SD:standard deviation.
15
Figure 1: AS: ankylosing spondylitis; CI: confidence interval; No: number of individuals; OR: odds ratio.
AS No (%) Controls No (%) OR (95% CI)1 P-value2 HLA-B27+/HLA-B60+ 88 (18.7) 7 (1.3) 201 (85-475) 2.5007×10-69 HLA-B27+/HLA-B60- 343 (72.8) 36 (6.5) 152 (91-255) 1.222×10-157 HLA-B27-/HLA-B60+ 12 (2.6) 66 (11.8) 2.9 (1.4-6.0) 7.167×10-3
HLA-B27-/HLA-B60- 28 (5.9) 448 (80.4) 1 -
All 471 (100) 557 (100)
1Odds ratio was calculated by unconditional maximum likelihood estimation and 95%
confidence intervals were calculated using normal approximation. 2P-value was calculated by Fisher-exact test.
16
Table 2: Logistic regression analysis to identify the independency of two risk factors HLA-B27 and HLA-B60.
Coefficients Estimate ß Standard error P-value
Intercept -2.7726 0.1948 <0.001***
HLA-B27-/HLA-B60+ 1.0678 0.3694 0.0038**
HLA-B27+/HLA-B60- 5.0268 0.2620 <0.001***
HLA-B27+/HLA-B60+ 5.3040 0.4384 <0.001***
Significant (p<0.01) value is in bold** and p<0.001 is in bold***.
17
Table 3: Difference in the scores of BASDAI, BASFI, and BAS-G among AS patients stratified by different HLA-B27/ HLA-B60 genotype
Patient Number
BASDAI BASFI BAS-G
HLA-B27 + /HLA-B60 + 88 4.37 2.20a 2.17 2.33 4.17 2.79
HLA-B27 + /HLA-B60 – 334 4.28 2.16 2.02 2.19 4.30 2.73
HLA-B27 – /HLA-B60 + 12 4.72 1.61 1.64 1.40 3.65 2.26
HLA-B27 – /HLA-B60 – 25 4.94 2.58 2.60 2.32 4.91 3.05
Kendall’s rank P-value
(tau)
0.5607
(-0.0216)
0.6976
(-0.0145)
0.4588
(0.0279)
aData represent means S.D.
科技部補助計畫衍生研發成果推廣資料表
日期:2014/10/31
科技部補助計畫
計畫名稱: 藥物基因組學分析強直性脊柱炎患者TNFα-受體阻滯劑治療的反應預測 計畫主持人: 魏正宗
計畫編號: 102-2314-B-040-017- 學門領域: 血液科腫瘤科風濕免疫及感染
無研發成果推廣資料
102 年度專題研究計畫研究成果彙整表
計畫主持人:魏正宗 計畫編號:102-2314-B-040-017-
計畫名稱:藥物基因組學分析強直性脊柱炎患者 TNFα-受體阻滯劑治療的反應預測 量化
成果項目 實際已達成
數(被接受 或已發表)
預期總達成 數(含實際已
達成數)
本計畫實 際貢獻百
分比
單位
備 註 ( 質 化 說 明:如 數 個 計 畫 共 同 成 果、成 果 列 為 該 期 刊 之 封 面 故 事 ...
等)
期刊論文 0 1 100%
研究報告/技術報告 0 1 100%
研討會論文 0 1 100%
論文著作 篇
專書 0 0 100%
申請中件數 0 0 100%
專利 已獲得件數 0 0 100% 件
件數 0 0 100% 件
技術移轉
權利金 0 0 100% 千元
碩士生 0 1 100%
博士生 0 0 100%
博士後研究員 0 0 100%
國內
參與計畫人力
(本國籍)
專任助理 0 0 100%
人次
期刊論文 0 0 100%
研究報告/技術報告 0 0 100%
研討會論文 0 0 100%
論文著作 篇
專書 0 0 100% 章/本
申請中件數 0 0 100%
專利 已獲得件數 0 0 100% 件
件數 0 0 100% 件
技術移轉
權利金 0 0 100% 千元
碩士生 0 0 100%
博士生 0 0 100%
博士後研究員 0 0 100%
國外
參與計畫人力
(外國籍)
專任助理 0 0 100%
人次
其他成果
(
無法以量化表達之成果如辦理學術活動、獲 得獎項、重要國際合 作、研究成果國際影響 力及其他協助產業技 術發展之具體效益事 項等,請以文字敘述填 列。)
無
成果項目 量化 名稱或內容性質簡述
測驗工具(含質性與量性) 0
課程/模組 0
電腦及網路系統或工具 0
教材 0
舉辦之活動/競賽 0
研討會/工作坊 0
電子報、網站 0
科 教 處 計 畫 加 填 項
目 計畫成果推廣之參與(閱聽)人數 0