Journal of Intellectual Disability Research doi: 10.1111/j.1365-2788.2006.00822.x
pp –
101
Blackwell Publishing LtdOxford, UKJIRJournal of Intellectual Disability Research0964-2633Blackwell Publishing Ltd, 20052101108Original ArticleInpatient care and intellectual disabilityC.-H. Loh et al.
Correspondence: Ching-Hui Loh, Department of Family &
Community Medicine, Tri-Service General Hospital, No. , Chenggong Road, Section , Nei-Hu, Taipei , Taiwan (e-mail: twdoc@mail.ndmctsgh.edu.tw).
Longitudinal analysis of inpatient care utilization among people with intellectual disabilities: 1999–2002
C.-H. Loh,1 J.-D. Lin,2 I.-C. Choi,3 C.-F. Yen,4 S.-W. Hsu,5 J.-L. Wu4 & C. C. Tang6
1Department of Family & Community Medicine, Tri-Service General Hospital, Taipei, Taiwan 2School of Public Health, National Defense Medical Center, National Defense University, Taipei, Taiwan 3Mentally Developmental Professional Study Center, Shih-Chien University, Taipei, Taiwan
4Research Center for Intellectual Disabilities Taiwan, Chung-Hua Foundation for Persons with Intellectual Disabilities, Taipei County, Taiwan
5Graduate Institute of Healthcare Administration, Asia University, Taichung, Taiwan 6Department of Nursing, I-Shou University, Kaohsiung County, Taiwan
Abstract
Background There has been no longitudinal study in Taiwan to identify the nature and the scale of medical care utilization of people with intellectual disabilities (IDs) up to the present. The aim of this study is to describe inpatient utilization among peo- ple under ID care in institutions in order to identify the pattern of medical care needs and the factors affecting utilization in Taiwan.
Method The subject cohort was individuals with ID who were cared for by a large public disability institution from to in Taipei, Taiwan.
Results On the examination of the inpatient care that these persons underwent, it was found that these individuals had a heightened need (inpatient rate:
.–.%) for inpatient care compared with the general population with disabilities (.%) in Taiwan. The main reasons for hospitalization were pneumonia, gastrointestinal disorders, cellulites,
orthopaedic problems, epilepsy and bronchitis. Using the full model of Generalized Estimating Equations for inpatient care utilization, the factors including low income family, living in an institution, being a subject with cerebral palsy and being a high outpatient user all influenced the use of inpatient care.
Conclusions This study highlights that health authorities need to promote health planning more in order to ensure an excellent quality of health moni- toring and health promotion among people with ID cared for by institutions.
Keywords health management, inpatient care, institution, longitudinal study
Introduction
Historically, public health has focused on preventing disabling conditions; people with disabilities have not been a target of healthcare policy (Lollar & Crews
). However, disability ranks as one of the great- est priorities among public health problems (Pope &
Tarlov ). To ensure the quality of health care for people with intellectual disabilities (IDs), The Euro- pean Manifesto on Basic Standards of Health Care for
Journal of Intellectual Disability Research
C.-H. Loh et al. • Inpatient care and intellectual disability 102
People with Intellectual Disabilities (Meijer et al. ) stated that health care should have greater availability and access for people with ID, that there should be increased competencies among ID health profes- sional, educators and researchers, that a greater reliance needs to be placed on multidisciplinary approaches to health care, that more specialist ser- vices are needed, and that a proactive emphasis on personal health management is required. Further- more, the six core goals of US Surgeon General Report for improving the health of people with ID included integration of health promotion into community environments, increased knowledge and understand- ing, improved quality of health care, better training of healthcare providers, more effective healthcare financing and increases in sources of health care (US Public Health Service ).
Numerous studies have reported that people with ID suffer from a range of accompanying medical conditions (Bond et al. ; Jones & Kerr ; Lin et al. a, a) and have a higher rate of medical care utilization (Meerding et al. ; Lin et al.
a, ). In securing access to the medical care system, people with ID experience challenges that are different in kind and degree from those that face other individuals (Singer et al. ; Palfrey et al.
). Vital questions about medical care are often addressed by analysing medical care utilization data (Diehr et al. ). Adequate information concerning medical care utilization is critical to the success of efforts to improve the quality of care for people with ID. However, data concerning the medical care utili- zation of people with ID in Taiwan is very limited.
The medical needs and problems of people with ID have received limited attention in the medical care system, and have been largely overlooked during the current medical care policy debate in Taiwan (Lin et al. a). The aim of the present study is to pro- vide a profile of medical care utilization and its deter- minants for people with ID who are cared for by a large institution through reviewing inpatient care data between and .
Methods Setting
The study setting is the largest residential institution in Taipei, Taiwan that mainly cares for persons with
severe or profound ID and multiple disabilities (indi- viduals with ID accompanied with another disabil- ity). This institution is a public institution that was set up in ; the Social Welfare Department of Taipei Municipal Government supervises and finan- cially supports the operation of the institution directly.
Subjects
There are two branches of this institution that are located in different areas. We chose the better orga- nized of the two branches with more complete med- ical records. A total of individuals with ID were cared for by this branch of the institution during
. The subject cohort was made up of of these
persons with ID who have been cared for contin- uously in this institution from to , thus providing years of medical data. The individuals with ID were either residing in or accepting day care from the institution. The remaining non- participants were excluded from the study because they did not have four consecutive years of care at the institution. We found that the age and gender charac- teristics of the two groups, participants and non- participants, did not significantly differ.
Data collection
One contracted public regional teaching hospital in Taipei has catered for the clinical care of people with ID cared for by this institution since . If a resi- dent of the institution requires inpatient care, they are transferred to the public regional teaching hospi- tal. The disability institution has set up a specific outpatient clinic (health station) and recruited skilled nurses to run the clinic. The medical care procedure for people with ID in this institution is the same as for the general population in the society; namely the ID individuals need to hold a Taiwanese National Insurance Card to register at the clinic. The main difference is that no co-payment is needed when vis- iting a physician at the clinic, while persons from general society need to provide co-payment at a clinic. This hospital offered between six and seven different clinics per week between the years and
. The medical care data included medical history and medical care utilization by persons with ID from the institution and were stored in the medical center,
Journal of Intellectual Disability Research
C.-H. Loh et al. • Inpatient care and intellectual disability 103
which was managed by the institutional nursing chief.
After obtaining approval from the institutional authority after showing adequate protection of the confidentiality of the medical records, the second author recorded all the information related to the
subjects’ information from their medical charts. The information included medical care utilization, demo- graphic data (age, gender, disability status, physical weight and height), number of years cared for by the institution and family economic information.
Data analysis
The data were entered into a database and analysed using . and . software. Analyses included frequency distributions and percentages for the demographic data and inpatient care utilization.
We used Generalized Estimating Equations (GEEs) to compare the relationship of the demographic pro- file and the four consecutive years of inpatient care utilization.
Results
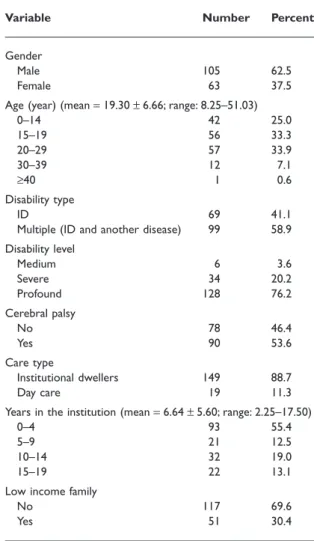
Based on the demographic data of the year , Table shows that the average age of the subjects was
. years and .% were male. In total, .% of subjects suffered from ID only, while .% suffered from multiple disabilities. There were .% of sub- jects who suffered profound disabilities and more than half of the subjects have a cerebral palsy. The average length of stay in the institution was . years and nearly one-third of the subjects had stayed more than years. With regard to the household eco- nomic status, more than % of the subjects come from low income families with their total family annual income . times less than the average annual income of the general population in Taiwan (Ministry of the Interior ). Nearly % of the subjects resided at this institution while about .% received daycare service and commuted between their families and the institutional setting. Generally speaking, the demographic characteristics between males and females showed no statistically difference except for height (males taller than females, P < .).
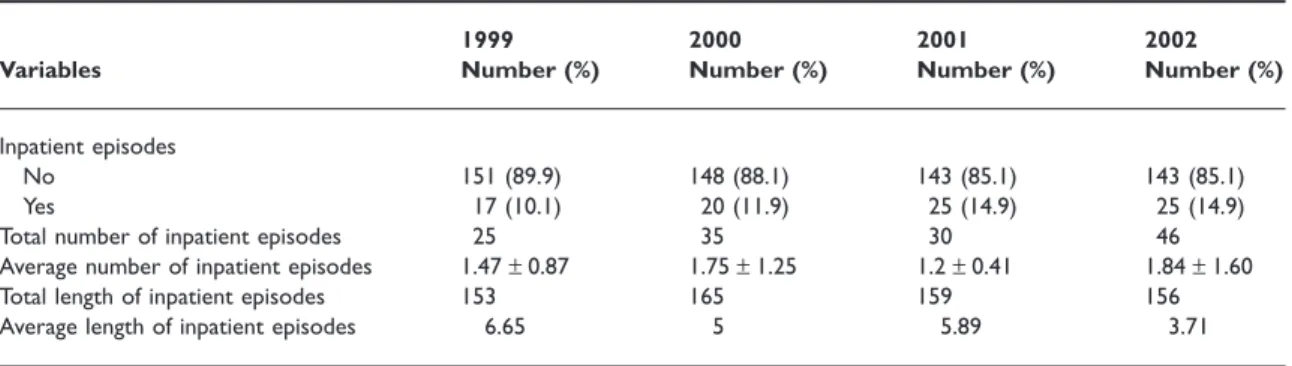
Tables and summarize the inpatient care utili- zation of the study subjects for the years –.
Between .% and .% of the subjects had
received inpatient care during these years. The average annual inpatient care utilization over these
years was . times. The annual rate for year
was significantly higher than those for the other years. The average length of stay in hospital varied from . to . days over the years. Table summarizes the main reasons for hospitalization as pneumonia, gastrointestinal disorders, cellulites, orthopaedic problems, epilepsy and bronchitis, all common diseases that affected people with ID in the institution.
When the four successive years of inpatient care utilization are correlated, they need to be treated as
Table 1 Distribution of demographic characteristics of the study subjects*
Variable Number Percent
Gender
Male 105 62.5
Female 63 37.5
Age (year) (mean = 19.30 ± 6.66; range: 8.25–51.03)
0–14 42 25.0
15–19 56 33.3
20–29 57 33.9
30–39 12 7.1
≥40 1 0.6
Disability type
ID 69 41.1
Multiple (ID and another disease) 99 58.9 Disability level
Medium 6 3.6
Severe 34 20.2
Profound 128 76.2
Cerebral palsy
No 78 46.4
Yes 90 53.6
Care type
Institutional dwellers 149 88.7
Day care 19 11.3
Years in the institution (mean = 6.64 ± 5.60; range: 2.25–17.50)
0–4 93 55.4
5–9 21 12.5
10–14 32 19.0
15–19 22 13.1
Low income family
No 117 69.6
Yes 51 30.4
*Based on the subjects’ demographic data in the year .
ID, intellectual disability.
Journal of Intellectual Disability Research
C.-H. Loh et al. • Inpatient care and intellectual disability 104
fixed samples statistically. Therefore, we used GEEs to compare the differences and to identify determi- nants for use/non-use of inpatient care. We first tested the use of inpatient care (yes/no) for different years and showed that there was no significant difference in the percentage hospitalization of subjects over the past years (P > .).
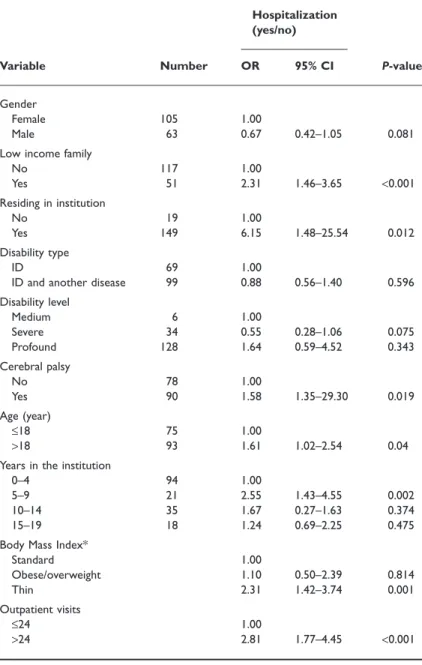
Table summarized the determinants of inpatient care utilization. Family economic status, residential status, age, length of stay, body mass index (BMI = kg/m2) and rate of outpatient visits were all related to hospitalization by the GEEs single variable model. Those ID individuals from low income fami- lies were . times more likely to be inpatient care users than those ID individuals who were not. The residential status of the subjects indicated that a per- son in residence was . times more likely to become an inpatient care user than those individuals who were only accepting daycare services at the institu- tion. Adults with ID were more likely to use inpatient
care (. times) than children with ID. Those sub- jects who also suffered from cerebral palsy were also more likely to become an inpatient care user (.
times) than individuals without cerebral palsy. The subject group who had stayed – years in the insti- tution was . times more likely to use inpatient care than those subjects who had stayed less than years.
Body stature was also a factor that affected inpatient care with thin subjects being . times more likely to use inpatient care than those subjects with a stan- dard, overweight or obese BMI. In addition, an out- patient care user with more than visits annually was . times more likely to be an inpatient care user than a subject who was not a high outpatient care user. The remaining factors such as gender, age, dis- ability type and level were not significantly correlated with inpatient care.
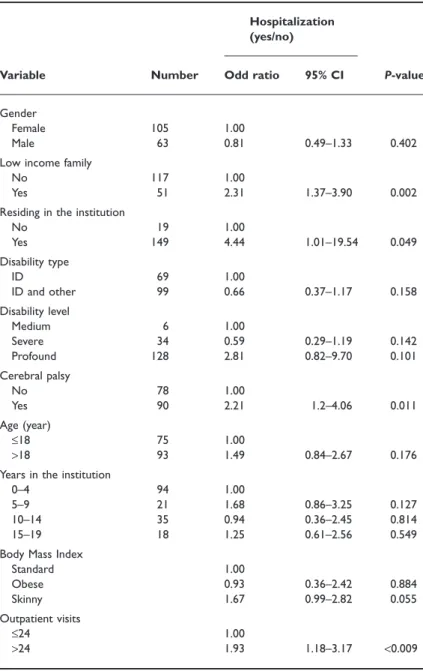
The full GEEs model was used to evaluate the factors determining inpatient care utilization while controlling the interaction of the factors tested.
Table 2 Distribution of inpatient care characteristics
Variables
1999 Number (%)
2000 Number (%)
2001 Number (%)
2002 Number (%)
Inpatient episodes
No 151 (89.9) 148 (88.1) 143 (85.1) 143 (85.1)
Yes 17 (10.1) 20 (11.9) 25 (14.9) 25 (14.9)
Total number of inpatient episodes 25 35 30 46
Average number of inpatient episodes 1.47 ± 0.87 1.75 ± 1.25 1.2 ± 0.41 1.84 ± 1.60
Total length of inpatient episodes 153 165 159 156
Average length of inpatient episodes 6.65 5 5.89 3.71
Table 3 Frequency of hospitalization from to
Frequency
Year (persons)
1999 2000 2001 2002
1 12 13 20 17
2 3 3 5 3
3 1 1 0 2
4 1 2 0 0
5 0 1 0 2
6 0 0 0 0
7 0 0 0 1
Total (person-times) 25 35 30 46
Table 4 The main reasons for hospitalization between and
Year Diseases or disorders (number of persons)
1999 Pneumonia (5), gastrointestinal disorders (3), cellulites (3), epilepsy (3), choke (2), others (0) 2000 Orthopaedic problems (6), pneumonia (3),
cellulites (3), bronchitis (3), epilepsy (2), others (0)
2001 Pneumonia (7), allergy (6), gastrointestinal disorders (4), bronchitis (3), fever (3), others (0) 2002 Pneumonia (10), gastrointestinal disorders (8),
cellulites (2), wound infection (2), others (0)
Journal of Intellectual Disability Research
C.-H. Loh et al. • Inpatient care and intellectual disability 105
Table shows that low income family (OR = .), institutional dwellers (OR = .), subjects who also suffered from cerebral palsy (OR = .) and high outpatient use (OR = .) were variables that were able to significantly predict the inpatient care use level.
Discussion
There has been no previous longitudinal study that has identified the nature and scale of medical care utilization by people with ID in Taiwan. Medical care utilization data have several valuable characteristics
Table 5 Determinants related to hospital- ization as determined by the Generalized Estimating Equations – single variable model
Variable Number
Hospitalization (yes/no)
P-value
OR 95% CI
Gender
Female 105 1.00
Male 63 0.67 0.42–1.05 0.081
Low income family
No 117 1.00
Yes 51 2.31 1.46–3.65 <0.001
Residing in institution
No 19 1.00
Yes 149 6.15 1.48–25.54 0.012
Disability type
ID 69 1.00
ID and another disease 99 0.88 0.56–1.40 0.596
Disability level
Medium 6 1.00
Severe 34 0.55 0.28–1.06 0.075
Profound 128 1.64 0.59–4.52 0.343
Cerebral palsy
No 78 1.00
Yes 90 1.58 1.35–29.30 0.019
Age (year)
≤18 75 1.00
>18 93 1.61 1.02–2.54 0.04
Years in the institution
0–4 94 1.00
5–9 21 2.55 1.43–4.55 0.002
10–14 35 1.67 0.27–1.63 0.374
15–19 18 1.24 0.69–2.25 0.475
Body Mass Index*
Standard 1.00
Obese/overweight 1.10 0.50–2.39 0.814
Thin 2.31 1.42–3.74 0.001
Outpatient visits
≤24 1.00
>24 2.81 1.77–4.45 <0.001
*Body Mass Index (Department of Health ): () age ≤ years calculated by their percentile; thin: BMI ≤ th; standard: th < BMI < th; overweight: th ≤ BMI ≤ th;
obese: BMI ≥ th. () age > years; thin: BMI < .; standard: . ≤ BMI < ;
overweight: ≤ BMI < ; obese: BMI > .
CI, confidence interval; ID, intellectual disability.
Journal of Intellectual Disability Research
C.-H. Loh et al. • Inpatient care and intellectual disability 106
that are helpful to decision makers. The present study described the four successive years of data for inpa- tient care utilization among people with ID in an institution. The findings show that .–.% of the subjects used inpatient care over the years. This steady figure is higher than the general population with disabilities in Taiwan, for whom the inpatient care rate was .% in (Ministry of the Interior
).
The average length of stay in hospital varied from
. to . days over the present study. This figure is similar to the result of Lin et al. () who con- ducted a study among disability institutions in
and showed an average hospital stay of days.
The main reasons for hospitalization in the present study were infections or disorders such as pneumo- nia, gastrointestinal disorders, cellulites and bronchi- tis. Many of these disorders are acute and can easily
Table 6 Factors related to hospitalization as determined by the Generalized Estimating Equations – full model
Variable Number
Hospitalization (yes/no)
P-value Odd ratio 95% CI
Gender
Female 105 1.00
Male 63 0.81 0.49–1.33 0.402
Low income family
No 117 1.00
Yes 51 2.31 1.37–3.90 0.002
Residing in the institution
No 19 1.00
Yes 149 4.44 1.01–19.54 0.049
Disability type
ID 69 1.00
ID and other 99 0.66 0.37–1.17 0.158
Disability level
Medium 6 1.00
Severe 34 0.59 0.29–1.19 0.142
Profound 128 2.81 0.82–9.70 0.101
Cerebral palsy
No 78 1.00
Yes 90 2.21 1.2–4.06 0.011
Age (year)
≤18 75 1.00
>18 93 1.49 0.84–2.67 0.176
Years in the institution
0–4 94 1.00
5–9 21 1.68 0.86–3.25 0.127
10–14 35 0.94 0.36–2.45 0.814
15–19 18 1.25 0.61–2.56 0.549
Body Mass Index
Standard 1.00
Obese 0.93 0.36–2.42 0.884
Skinny 1.67 0.99–2.82 0.055
Outpatient visits
≤24 1.00
>24 1.93 1.18–3.17 <0.009
CI, confidence interval; ID, intellectual disability.
Journal of Intellectual Disability Research
C.-H. Loh et al. • Inpatient care and intellectual disability 107
start in an institution. In addition, many chronic diseases such as epilepsy or orthopaedic problems always affect people with ID at an institution. There- fore, it is necessary to examine the health manage- ment policy of the institution for these disorders in order to monitor the effectiveness and efficacy of the disease management for people with ID cared for at the institution.
With regard to the determinants of hospital care utilization, the present study shows that factors including family economic status, being an institu- tional dweller, being a subject with cerebral palsy and being a high outpatient user were variables correlated with inpatient care utilization by the GEEs full model. Family income status is known to affect peo- ple’s health and healthcare utilization (Andersen
). In order to ensure the health equity of people in Taiwan, the Taiwanese National Health Insurance programme regulates that people with disabilities have their insurance premiums partly paid by the government. Within medical care utilization, people with disabilities also receive additional support in the form of ambulatory care and inpatient care (Bureau of National Health Insurance ). This kind of universal healthcare system seeks to ensure that peo- ple have access to care on a basis of need, rather than income. However, more than % of people with disabilities say that medical care expenditure still affects their healthcare utilization under National Health Insurance Plan (Report of the Living Survey of People with Disabilities , Ministry of the Inte- rior ). One possible explanation for the linking of family income with in-care utilization in the present study is that participants who came from low income families may have poorer health or be frailer;
if this is true, they would proportionately utilize more healthcare services. The real reason for the linkage of household economic status with inpatient care utili- zation found by the present study needs to be exam- ined further.
People with ID often carry a greater burden of diseases that require treatment than people in the general population (Lin et al. b; van Schrojen- stein Lantman-de Valk ). Moreover, those peo- ple with ID residing in the institutions tend to suffer from ill health or comorbidity and thus need contin- uous monitoring of their health (Lin et al. b).
Individuals with ID who also suffer from cerebral palsy and those who are higher outpatient users also
show an increased risk of hospitalization. Therefore, the health authorities need careful promotion of health planning for people with ID within disability programmes in order to ensure a high quality of health care and health promotion for people with ID who are cared for by institutions (Lin et al.
c).
The present study has several limitations. In this study, we did not examine the effects of a range of further factors that may affect inpatient care utiliza- tion. The determinants of inpatient care in this study are different from the results of Lin et al. (), who found that the subject’s and carer’s age, poor health- care accessibility, time consumed in health care, need for rehabilitation, ill health and having multiple dis- abilities, were all factors that resulted in increased inpatient care utilization. The main reason is that we collected the information for this study from existing medical care charts and the other variables men- tioned above were not available. In addition, we did not analyse follow-up treatments after discharge from hospitals to evaluate the effectiveness or efficiency of care at the institution.
Conclusion
The evidence-based data on medical care utilization provides opportunities to improve the health of peo- ple with ID and this, in turn, will foster better scien- tific health policy making. From this examination of the inpatient care of people with ID cared for by an institution, it was found that these individuals have a heightened need for inpatient care compared to the general population with disabilities in Taiwan. The health authorities need to evaluate more carefully the determinants of inpatient care use and topromote health planning and healthy life style (such as nutri- tion) to ensure that there is good quality health mon- itoring among people with ID who are cared for at institutions.
Acknowledgements
This study was supported by the National Council of Sciences, Taiwan in − (grant no.
NSC---B--). We thank Ms L.-Y. Hsu and Miss S.-L. Cheng for their help with data collection.
Journal of Intellectual Disability Research
C.-H. Loh et al. • Inpatient care and intellectual disability 108
References
Andersen A. () Exploring dimensions of access medical care. Health Services Research , –.
Bond L., Kerr M., Dunstan F. & Thapar A. () Atti- tudes of general practitioners towards health care for peo- ple with intellectual disability and the factors underlying these attitudes. Journal of Intellectual Disability Research
, –.
Bureau of National Health Insurance () National Health Insurance Profile . Department of Health, Taiwan.
Department of Health () The Definition of Obesity and Management Principles. Available at:
http://www.doh.gov.tw/NewVersion/
content.asp?class_ no=&now_fod_list_no=&array (retrieved April ).
Diehr P., Yanez D., Ash A., Hornbrook M. & Lin D. () Methods for analyzing health care utilization and costs.
Annual Review of Public Health , –.
Jones R. G. & Kerr M. P. () A randomized control trial of an opportunistic health screening tool in primary care for people with intellectual disability. Journal of Intellectual Disability Research , –.
Lin J. D., Wu J. L. & Lee P. N. (a) Healthcare needs of people with intellectual disability in institutions in Taiwan: outpatient care utilization and implications.
Journal of Intellectual Disability Research , –.
Lin J. D., Lee P. N., Wu J. L. & Yen J. F. (b) Health profile of persons with intellectual disabilities in institutions in Taiwan. Journal of Medical Sciences ,
–.
Lin J. D., Wu J. L. & Lee P. N. () Utilization of inpatient care and its determinants among people with intellectual disabilities in daycare centers in Taiwan.
Journal of Intellectual Disability Research , –.
Lin J. D., Yen J. F., Li C. W. & Wu J. L. (a) Patterns of obesity among children and adolescents with intellec- tual disabilities in Taiwan. Journal of Applied Research in Intellectual Disabilities , –.
Lin J. D., Yen J. F. & Wu J. L. (b) Importance and satisfaction of preventive health strategies in institutions for people with intellectual disabilities: a perspective of institutional directors. Research in Developmental Disabili- ties , –.
Lin J. D., Yen J. F., Loh C. H., Chow M. J., Wu J. L. &
Tung H. J. (c) Perceptions of program administra- tors toward health planning for persons with intellectual
disabilities: a national survey in Taiwan. Journal of Policy and Practice in Intellectual Disabilities , –.
Lollar D. J. & Crews J. E. () Redefining the roles of public health in disability. Annual Review of Public Health
, –.
Meerding W. J., Binneux L., Polder J. J., Koopmanschap M. A. & Maas P. J. () Demographic and epidemi- ological determinants of healthcare costs in Nether- lands: cost of illness study. British Medical Journal ,
–.
Meijer M. M., Carpenter S. & Scholte F. A. () Euro- pean manifesto on basic standards of health care for peo- ple with intellectual disabilities. Journal of Policy and Practice in Intellectual Disabilities , –.
Ministry of the Interiors () Report of Living Survey of People with Disabilities . Ministry of the Interior, Taiwan.
Ministry of the Interior () The Living Survey of People with Disabilities (II): Healthcare in . Ministry of the Interior, Taiwan.
Ministry of the Interior () Living Assistance for the Low- Income Households. Available at: http://sowf.moi.gov.tw/
/new.htm (retrieved March ).
Palfrey J. S., Samuels R. C., Haynie M. & Cammisa M. L.
() Health care reform: what’s in it for children with chronic illness and disability. Journal of School Health ,
–.
Pope A. M. & Tarlov A. R. () Disability in America:
Toward A National Agenda for Prevention. National Academic Press, Washington, DC.
van Schrojenstein Lantman-de Valk H. M. J., te Wierik M.
J. M., van de Akker M., Wullink M., Schellevis F. G., Dinant G. J. & Metsemakers J. F. M. () Morbidity and health-care use in people with intellectual disabilities in general practice: first results of a survey in the Netherlands. Journal of Policy and Practice in Intellectual Disabilities , –.
Singer J. D., Butler J. A. & Palfrey J. S. () Health care access and use among handicapped students in five public school system. Medical Care , –.
US Public Health Service () Closing the Gap: A National Blueprint for Improving the Health of Individuals with Mental Retardation. Report of the Surgeon General’s Conference of Health Disparities and Mental Retarda- tion, . US Department of Health and Human Services, Washington, DC.
Accepted December