國立臺灣大學醫學院物理治療學系暨研究所 碩士論文
School and Graduate Institute of Physical Therapy College of Medicine
National Taiwan University Master Thesis
作業優先性對姿勢-上姿勢作業與大腦活動的影響:
年齡效應
The Effects of Task Prioritization on Postural-suprapostural Task and Cortical Activity: Age-related Differences
游舒涵 Shu-Han Yu
指導教授:黃正雅 博士 Advisor: Cheng-Ya Huang, Ph.D.
中華民國 104 年 7 月
July, 2015
I
II
致謝
人生中每一個里程碑的到達都伴隨許多人的協助,而長達兩年的研究所生
涯,也同樣接受到很多人的幫助。首先,由衷地感謝指導教授黃正雅老師的協
助,從研究架構的形成、實驗基礎的訓練、實驗困境的突破到碩士論文的撰寫,
每一個階段都受到老師很大的幫助及引導,總是在身旁給予許多建議及鼓勵,使
我的研究之路一直都相當順遂,也從中獲得很多的成就感及收穫。此外,感謝口
試委員吳瑞美醫師、周立偉老師、陸哲駒老師和張雅如老師在研究及論文上給予
許多寶貴的建議,使我能對於研究有更多不同面向的思考,而使研究與論文都能
更臻於完善。
這兩年的研究生活中,感謝好朋友郁婷、甯雅和嘉容提供能夠談心歡笑的時
間和空間,紓解準備研究和論文時的煩惱及壓力,也感謝學系老師給予許多的關
心與指導,更感謝所有受試者熱心地參與實驗,包含臺大醫院志工阿姨伯伯和醫
院員工、其他單位的志工阿姨伯伯、大學部的學弟妹、碩士班和博士班的學長
姊,給予相當大的協助與鼓勵而使實驗進度能順利推展。最後,真心感謝父母提
供無憂的環境可以專心的進行研究及撰寫論文,這兩年間默默給予強大的支援。
「學問如逆水行舟,不進則退」,感謝過去已無法細數的所有協助,成為了
推動的助力,幫助我在學問的逆流中一路前進,而能在今日邁向了新的里程碑。
III
中文摘要
研究背景與目的:姿勢-上姿勢作業為於維持身體平衡下,同時進行另一項動
作或認知活動。由於注意力資源的有限性,適當且有效率的注意力配置,亦即作
業優先性選擇,為獲得較佳姿勢-上姿勢作業表現的關鍵因素。此外,隨年齡增
長,大腦注意力資源及其注意力配置的能力會逐漸下降,更加突顯作業優先性選
擇的重要性。然而,目前關於姿勢-上姿勢控制的作業優先性(姿勢優先、上姿勢
優先)探討及其相對應的神經機制仍尚未被仔細探討。因此,本研究的主要目的為
探討年輕及老年族群,在使用不同作業優先策略下,對姿勢-上姿勢作業表現及大
腦活動的影響。
研究方法:本研究共招募 16 位健康年輕受試者(平均年齡:24.4 ± 4.6 歲)及
16 位健康年長受試者(平均年齡:69.1 ± 2.7 歲)進行姿勢-上姿勢作業測試。實驗
中受試者站立於平衡板上維持平衡(姿勢作業),並同時執行右手大拇指與食指的
精準按壓動作(上姿勢作業)。姿勢作業之目標角度設為受試者前傾平衡板最大角
度的一半,而上姿勢作業之目標力量設為受試者執行精準按壓最大力量數值的一
半。實驗過程中須分別將主要注意力放置於姿勢平衡(姿勢優先)或精準按壓動作
(上姿勢優先)來執行姿勢-上姿勢作業。實驗過程中記錄平衡板角度變化、精準按
壓力量、右手第一背側指間肌肌電圖,並同步測量受試者之腦電圖。本研究之分
IV
析參數包含:姿勢作業角度誤差、精準按壓力量誤差、平衡板晃動之近似熵
(approximate entropy)、精準按壓反應時間及腦電圖事件相關電位(P1, N1, P2)振
幅。統計分析使用 2 × 2 混合變異數分析(2 × 2 mixed ANOVA)及最小顯著差異
法(least significant difference)進行事後檢定,分析作業優先性與年齡效應對各行為
表現參數及事件相關電位的影響。
結果與討論:相較於姿勢優先策略,於使用上姿勢優先策略時,年輕族群與
老年族群皆會有較少的姿勢作業誤差,尤其老年族群於上姿勢優先策略時,同時
會呈現較高的姿勢近似熵數值與較低的精準按壓力量誤差。於腦電圖事件相關電
位振幅結果,在使用上姿勢優先策略時,年輕與老年族群的 N1 振幅皆較使用姿
勢優先策略時小,反應上姿勢優先策略可降低姿勢作業所需之注意力資源的需求
量,代表上姿勢優先策略是個較有效率的策略。此外,相較於年輕族群,老年族
群於 N1 波與 P2 波之前,多呈現 P1 波,顯示老年族群於執行姿勢-上姿勢作業的
準備初期會先進行感覺訊息的促進與整合。
結論:在執行姿勢-上姿勢作業時,上姿勢優先策略對健康年輕族群及老年族
群皆是較佳的動作控制策略,不但能產生較高的作業精準度且有較佳的大腦注意
力資源配置情形。
V
重要性與預期貢獻:本研究結果可提供健康族群,尤其是老年族群在執行姿
勢-上姿勢作業時,一個較適當的動作控制策略,以提升整體動作表現,並可對姿
勢-上姿勢控制的神經生理機制有進一步的瞭解。未來將進一步推展至神經疾患之
患者,以期提供臨床治療時適當的訓練策略。
關鍵字:作業優先性、姿勢平衡、雙重作業、事件相關電位、年齡效應
VI
Abstract
Background and Purpose: Postural-suprapostural task is defined as achievement
of a motor or cognitive task performed simultaneously with successful postural control.
Due to limited attentional resource, appropriate task prioritization is required for better
performance during postural-suprapostural task, especially in elderly adults, who may
have decreased attentional capacity and impaired attentional allocation. However,
research on the suitable strategy of task prioritization (posture-first (PF) vs. supraposture-
first (SF)) in younger and older adults is limited and lacks direct neural evidences. The
purpose of this study was to investigate the effects of task-priority strategies on postural-
suprapostural performance and its related cortical activity in younger and older
populations.
Methods: Sixteen younger healthy and sixteen elderly healthy adults were recruited
in this study. Each participant was requested to perform a force-matching precision grip
task (suprapostural task) while maintaining balance on a stabilometer (postural task) with
postural task or suprapostural task as the first-priority task. Both behavioral and cortical
data, including task accuracy (postural error and force-matching error), postural ApEn
(approximate entropy), reaction time of precision-grip, and event-related potentials
(ERPs), including P1, N1, and P2 amplitudes, were recorded.
VII
Results and Discussions: With SF strategy, less postural error was found in both
younger and older groups. Furthermore, smaller force-matching error and larger postural
ApEn were observed under the SF condition in the older group. ERP results revealed a
task priority-dependent N1 response, which was smaller in the SF condition, indicating
that SF is an efficient strategy for postural-suprapostural control. In addition, besides N1
and P2 waves, P1 positivity was observed only in the older adults, implying more
facilitation of sensory processing was invested in the initial preparation phase of postural-
suprapostural performance for older adults.
Conclusion: SF strategy may be the adequate strategy for both healthy younger and
older adults, with better postural-suprapostural accuracy and more efficient attentional
allocation than PF strategy. Further study is needed to be confident in this conclusion for
patients with neurological disease, such as Parkinson’s disease.
Significance and Contribution: The study not only provided an optimal task-
priority strategy for healthy adults, especially older adults, to increase their movement
quality of postural-suprapostural task, but also gain a better insight to neural correlates of
concurrent postural and motor-suprapostural tasks.
Keywords: task prioritization; postural balance; dual task; event-related potential; age
effect
VIII
Contents
Page
Verification Letter from the Oral Examination Committee……… I
Acknowledgement……… II
Chinese Abstract……….. III
Abstract……… VI List of Abbreviation………. XI
List of Figures……….. XIII
List of Tables……… XV
Chapter 1 Introduction……… 1
1.1 Overview of Postural-suprapostural Task……… 1
1.1.1 Definition………... 1
1.1.2 Theoretical Framework of Postural-suprapostural Task………… 2
1.1.3 Age-related Models of Postural-suprapostural Performance……. 3
1.2 Related Literature………. 5
1.2.1 Task Prioritization on Postural-suprapostural Performance…….. 5
1.2.2 Age Difference on Postural-suprapostural Performance………… 7
IX
1.2.3 Limitation of Previous Study About Postural-suprapostural
Task……… 8
1.2.4 Characterization of Cortical activity with Event-related Potentials……… 10
1.3 Rationales ……… 12
1.4 Purpose and Significance………. 13
1.5 Hypothesis……… 14
Chapter 2 Methods……… 16
2.1 Participants……….. 16
2.2 System Set-up and Data Recording………. 17
2.3 Experimental Conditions and Procedures……… 19
2.4 Data Analysis………... 22
2.4.1 Behavioral Data………. 22
2.4.2 ERPs Data……….. 23
2.5 Statistical Analysis………... 24
Chapter 3 Results………. 26
3.1 Behavioral Performance……….. 26
3.1.1 Error and Regularity of Postural Performance……….. 26
X
3.1.2 Error and Reaction Time of Force-matching Task……… 27
3.2 ERP Amplitudes………... 29
3.2.1 Task Prioritization Effect on ERP Amplitudes……….. 29
3.2.2 Age Effect on ERP Amplitudes………. 31
Chapter 4 Discussions……….. 33
4.1 Improved Task Accuracy with SF Strategy……… 33
4.2 Facilitated P1 Wave in the Older Group in SF Condition………. 36
4.3 Age Effect on ERPs in Postural-suprapostural Tasks……… 39
4.4 Methodological Issues……… 40
Chapter 5 Conclusion………... 44
References………. 45
Figures……… 54
Tables……… 72
Appendices……… 74
Appendix 1 Mini Mental State Examination (MMSE)……….. 74
Appendix 2 Approved document form the research ethics board at the National Taiwan University Clinical Trail Center…………. 78
XI
List of Abbreviation
ANOVA analysis of variance
ApEn approximate entropy
CV_PPF coefficient of variance of peak precision grip force
EEG electroencephalography
EMG electromyogram
ERP event-related potential
FDI first dorsal interosseous
LSD least significant difference
MMSE Mini Mental State Examination
MVC maximum voluntary contraction
PF posture-first
PPF peak precision-grip force
RMS root mean square
RT reaction time
SA stabilometer tilting-angle
SF supraposture-first
XII
TA target angle
TF target force
XIII
List of Figures
Page
Figure 1. Thinking process of the study……….. 54
Figure 2. Experimental setup of the study………... 55
Figure 3. Flow diagram of the study………... 56
Figure 4. Visual information for the PF and SF conditions……….... 57
Figure 5. Means and standard errors of absolute and normalized postural error of younger and older groups in the SF and PF conditions………... 58
Figure 6. Means and standard errors of absolute and normalized ApEn of younger and older groups in the SF and PF conditions………... 59
Figure 7. Means and standard errors of absolute and normalized force-matching error of younger and older groups in the SF and PF conditions……….. 60
Figure 8. Means and standard errors of absolute and normalized force-matching RT of younger and older groups in the SF and PF conditions…………. 61
Figure 9. Typical ERP waveforms of younger and older groups……… 62
XIV
Figure 10. Task prioritization effect on ERP waveforms 63
Figure 11. Task prioritization effect on grand-averaged ERP topological plots 65
Figure 12. Age effect on grand-averaged ERP topological plots 67
Figure 13. Population means of topological plots of all task priority condition (PF
and SF conditions) and age groups (younger and older groups)………. 68
Figure 14. Force CV and postural error of pilot study……….. 70
Figure 15. Graphic summary of the study………. 71
XV
List of Tables
Page
Table 1. Baseline characteristics of the participants.………. 72
Table 2. Comparison of collected normalized postural error, postural ApEn,
force-matching error, and force-matching RT between the first and
second experimental days.………... 73
1
Chapter 1 Introduction
1.1 Overview of Postural-suprapostural Task
1.1.1 Definition
Postural task is defined as the control of body posture in a stable, upright position in
space for the purpose of balance or orientation, such as standing and walking.
1,2
It hasbeen traditionally considered as an automatic controlled task which required little
attention, but recent evidences have been found significant attentional requirements for
postural control in facilitating multi-sensory integration and generation of motor
execution.
1,3
In daily activities, upright stance is rarely undertaken without other tasks.Any task that is superordinate to the control of posture is defined as a suprapostural task.
2,4
The evaluation or behavioral goal of the suprapostural task is different from postural
control and information of suprapostural performance cannot be acquired from the value
of postural parameter.
4
Performing a postural-suprapostural task is frequent for human being in daily life,
such as using mobile phone while standing on a bus or carrying a bowl of soup while
2
walking. When postural task and suprapostural task are performed together, the two
attention-demanding tasks require common attentional resource simultaneously, which
challenges the brain for prioritizing the two tasks.
1,5
Thus, the appropriate allocation ofattention is important when performing a postural-suprapostural task for better
performance of both tasks.
1.1.2 Theoretical Framework of Postural-suprapostural Task
Two theoretical frameworks have been commonly described to explain the allocation
of attention in postural-suprapostural task, which are resource-competition model and
adaptive resource-sharing model.
6,7
According to the resource-competition model,attention is assumed as a capacity-limited resource. When performing a postural-
suprapostural task, postural task and suprapostural task compete for the same attentional
resource.
6
With the available attentional capacity, both tasks are well performed. However,when attentional requirements of both tasks exceed the capacity, the concurrent tasks
interfere with each other and lead to the adverse effect on the both postural and
suprapostural performance.
7
Similar to resource-competition model, the adaptive resource-sharing model
postulates that postural task and suprapostural task share the same capacity-limited
3
resource, but the concept of cost-benefit in the postural-suprapostural sharing situation is
included in this model. The central system prioritizes between both tasks during postural-
suprapostural task and leads the performance of both tasks to the trade-off results.
6
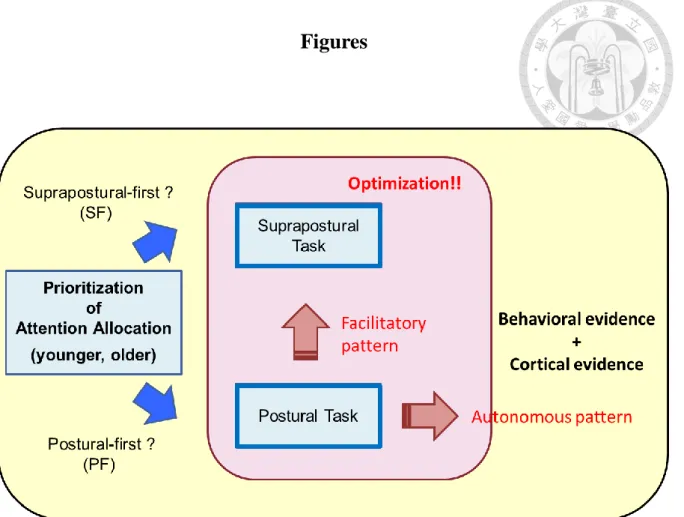
Furthermore, two possible patterns in the adaptive resource-sharing model are proposed
based on some behavioral findings of postural-suprapostural performance, which are
autonomous and facilitatory patterns. The autonomous pattern emphasizes that postural
control would be acted as the primary task (the task gets more attentional resource) and
is engaged in sway minimization automatically no matter which suprapostural task is
added to a postural task. In contrast, the facilitatory pattern (also called as facilitatory
hypothesis) emphasizes that the postural stability may improve for facilitating the
suprapostural performance, especially when the suprapostural task gets more attentional
resource.
6,8
Both resource-competition model and adaptive resource-sharing model imply that
the attention is a critical issue for postural-suprapostural control. Specially, how the
attentional allocation (or task prioritization) operates the postural task and suprapostural
task is a worth issue to study.
1.1.3 Age-related Models of Postural-suprapostural Performance
4
Age-related structural and functional changes have been found in musculoskeletal,
neuromuscular, cardiovascular, and sensory system, which affected the ability of postural
control.
9,10
To compensate the deterioration of postural control, older adults need moreattentional requirement for balance comparing to younger adults, even in simple postural
condition.
1,11
However, attentional capacity has been found decreased with aging, leadingto greater age-related differences of attentional allocation in postural-suprapostural
tasks.
12
Lacour et al. (2008)
13
summarized three age-related models for explaining the poorpostural control in postural-suprapostural task, including the cross-domain competition
model, the nonlinear interaction model, and the task-prioritization model. First, the cross-
domain competition model assumed that the postural task and suprapostural task shared
and competed for the attentional resource, leading to less sufficient resource for postural
control.
13,14
The increase of the age enlarges the adverse effect of posture during thecompetition of the both tasks due to reduced attentional capacity.
13
Second, the linearinteraction model proposed that the postural performance depended upon the attentional
requirement of the suprapostural task.
3,13
With adding a low demanding supraposturaltask, postural task improves in both younger and older adults. However, with adding a
high demanding suprapostural task, the beneficial effect of suprapostural task reduces
with aging.
13
5
Different from the two models, the task prioritization model emphasized the
importance of task-priority strategy for older adults while performing a postural-
suprapostural task. Due to decreased attentional resource with aging, the older adults may
tend to select the safer strategy for postural control, allocating more attentional resource
to postural task for responding the age-related decline.
13,15
The model predicts thatprioritization of postural control, which is also called “posture-first” strategy, is often
selected on postural-suprapostural task in older adults as a compensatory attentional
reallocation.
11-13
However, if the “posture-first” is the optimal control strategy for olderadults while performing a postural-suprapostural task is not completely lucid.
1.2 Related Literature
1.2.1 Task Prioritization on Postural-suprapostural Performance
In a postural-suprapostural task, accomplishing the suprapostural goal and keeping
balance as well is the basic purpose of the task. To achieve the better performance,
appropriate task prioritization becomes an important issue in postural-suprapostural task.
Recently, some previous studies manipulated participants’ major attention between
postural and suprapostural tasks by verbal instruction to examine the effect of attentional
6
allocation. Some studies showed that allocating major attention on suprapostural task
would result in better postural-suprapostural performance. For example, in Siu et al.’s
study (2007), the participants were requested to perform a visual spatial memory task
while standing with feet together with focusing on the memory task or their balance.
Participants had significantly shorter response time when prioritizing the memory task
compared to prioritizing postural task and no postural sway difference between the two
prioritizing conditions.
16
Also, in the research of Jehu et al. (2015), subjects were askedto perform a choice reaction time task while standing on a force platform with prioritizing
the choice reaction time task or the postural task. Both less postural sway and shorter
reaction time were observed under prioritizing the choice reaction time task.
17
In Kelly etal.’s study (2013),
18
participants were asked to perform a auditory Stroop task whilewalking. The results showed that with a cognitive-focus instruction, both cognitive and
walking performance would not decrease, but with a walking-focus instruction, the
performance of cognitive task deteriorated significantly but the walking speed did not
improve, indicating focusing on a postural task may not a suitable strategy in a postural-
suprapostural task.
However, the study of Yogev-Selignmann et al. (2010) had opposite results,
reporting that a worse postural-suprapostural performance was observed under
prioritization of a cognitive task.
19
In this study, participants were asked to perform a7
verbal fluency task while walking with focusing on the verbal fluency task or on walking.
The results showed that the number of words generated in verbal fluency task was similar
between the two conditions. But with focusing on the verbal fluency task, the walking
speed decreased relative to focusing on walking. In addition, in study of Yogev-
Seligmann et al. (2012), both word-generation number and walking speed improved when
subjects focused on walking.
20
Taken together, the inconsistency in current empiricalliterature on postural-suprapostural task suggests that the effects of task prioritization on
postural-suprapostural performance merits further scrutiny.
1.2.2 Age Difference on Postural-suprapostural Performance
Age-related change on postural-suprapostural dual tasking has been found in clinic
and been examined in many studies. In clinic, we may observe that older adults stop
walking while talking. In attention-related studies, impaired attention functions and
impaired working memory have been evident in older adults.
12
Specially, aging-relateddeclines in attentional capacity and resource processing efficiency are noted in multiple-
tasking conditions, such as postural-suprapostural task.
3,21-23
Besides, decreasedflexibility and optimality of attentional allocation across tasks are also presented in aging
studies.
23,24
For instance, Doumas and Krample (2013)21
found that when performing a8
auditory n-back task with standing on a sway-reference platform, the performance of
postural task decreased in older adults, but not in younger adults. Huxhold et al. (2006)
3
showed that increased center of pressure displacement was found in older adults when
performing more demanding cognitive task with postural task , but not in younger adults.
Moreover, it had similar findings while older adults need to walk with performing a
suprapostural task. Hollman et al. (2006)
25
found slower gait velocity in older adults thanyounger adults when spelling five-letter words in reverse and walking across the walkway
concurrently. Also, comparing to younger adults, older adults had less word-generation
number and less walking distance when performing a word-fluency task concurrent with
walking on a narrow track.
19
All these studies showed deterioration of both postural andsuprapostural performance in support of the view of more limited attentional capacity and
attentional control ability in older adults.
1.2.3 Limitation of Previous Study About Postural-suprapostural Task
The results about task prioritization of postural-suprapostural tasks still exited
inconsistency. The inconsistency was probably due to the instruction of how the subjects
should focus their attention and the nature of suprapostural task (cognitive-supraposture
or motor-supraposture).
26
The lack of specification in instruction of prioritization has9
been considered a major limitation of postural-suprapostural related studies,
16,19
and littledifference of the instruction may significantly affect the performance.
17
Most previousstudies only instructed the primary task to subjects, such as “focus on the cognitive task
and perform it as quickly and accurately as possible”, or “focus on your posture and keep
balance as still as possible”, and even did not tell subjects the focused task is the primary
task. Without specific instruction for both primary and secondary tasks, subjects may
allocate their attention between the primary and secondary tasks differently and result in
inconsistency performance. Hence, the instruction of how to allocate their attention
between postural and suprapostural tasks should be more specific and clear to avoid
discrepancy in attentional allocation between subjects.
On the other hand, the type of suprapostural tasks is also one of the critical factors
that may affect the interaction between postural and suprapostural tasks. Most previous
literatures used cognitive tasks to be the suprapostural task, such as Stroop task or verbal-
fluency task.
19,27
However, growing literatures suggested that combination of motor taskand postural task may increase the sensitivity to detect the attentional resource
capacity.
28,29
Due to similar nature of postural control and motor task, motor task andpostural task compete for the same input and output resources, resulting in larger
interference between postural balance and motor-suprapostural performance compared
with a traditional dual tasking with a posture-cognition setup. Moreover, the greater
10
interference between postural task and motor task was found in older adults than in
younger adults, due to age-related ability decline to manipulate two similar motor tasks
concurrently.
23,30
Thus, postural task combined with motor task may be the proper designto observe the interaction between postural and suprapostural tasks, especially in older
adults.
Next, most of previous studies about task prioritization of postural-suprapostural
control just focused on the behavioral outcome but very were limited to examine the
related cortical activation for central resource allocation in a postural-suprapostural task.
However, only behavioral evidence is unable to well explain the brain organization for
attentional allocation between postural and suprapostural tasks.
31,32
Thus, it appears thatthe cortical activity and behavioral measurement must be integrated to examine the
interaction between postural and suprapostural tasks for providing comprehensive
information of postural-suprapostural control.
1.2.4 Characterization of Cortical activity with Event-related Potentials
Event-related potential (ERP), derived from electroencephalogram (EEG), is a
common electrophysiological technique for investigating information processing of
cognitive or motor task.
33
As a stimulus-locked cortical potential, ERP would be labeled11
as “N” or “P” waveform for representing negative-going or positive-going component
respectively. The number following the label represents the peak latency of the
waveform,
34
such as N1 represents the negative waveform which peaks around 100 msafter stimulus and P2 represents the positive waveform which peaks around 200 ms after
stimulus. Recently, because of precise temporal resolution, ERP components have been
used in dual tasks for investigating attention shift between the two tasks and the stage of
neural information processing.
31,32,35-37
In dual-task paradigm, early ERP (P1, N1, and P2) and late ERP (P300) amplitudes
have been known as an index of resource allocation of cognitive processing.
32,35,36
P1amplitude was reported associated with sensory input to attended task and arousal.
38,39
For postural-suprapostural dual tasking, it was found that N1 amplitude was associated
with the information processing of postural control
32,37
and P2 amplitude was related tosuprapostural (a precision-grip force-matching task) control.
32
Both Huang and Hwang(2013)
32
and Little and Woollacott (2015)37
reported that the amplitude of N1 increasedwhen posture demand increased. Besides, P2 amplitude would be modulated by
suprapostural difficulty. With high difficulty of suprapostural task, P2 amplitude would
be decreased, representing more attentional resource allocated to the suprapostural task.
32
Based on previous studies, P1, N1 and P2 amplitudes were known to play an important
role on attention processing in postural-suprapostural task. Therefore, both P1, N1 and
12
P2 amplitudes were focused in the ERP analysis for representing attentional allocation
between postural and suprapostural tasks in the present study.
1.3 Rationales
1. There is inconsistency on advantage and defects between posture-first (PF) strategy
and supraposture-first (SF) strategy. It is valuable to realize which task-priority
strategy is the suitable strategy when performing a postural-suprapostural task.
2. Because appropriate attentional allocation or attentional shift is a critical factor for
successful postural-suprapostural execution, ERP signals could be helpful to identify
the neural mechanism of critical level in different task-priority strategies. The
understanding of cortical activation of postural-suprapostural execution may facilitate
innovative and pertinent treatment strategy for people who are multi-tasking
disturbances and prevent them from falling.
3. Comparing to younger adults, older adults may suffer from decreased attentional
capacity and impaired attentional allocation,
3
and this may affect the applicability oftask-priority strategy between younger and older adults. In this study, both younger
and older adults would be included to investigate the effects task prioritization on
postural-suprapostural tasks.
13
4. The instruction affects the way participants allocating their attention in a postural-
suprapostural task.
17
Unclear instruction may confuse the participants, leading todifferent attentional allocation between subjects. In the present study, the “optimum-
maximum method”
40
would be used for instructing subjects and enhancing theguidance of task prioritization.
5. Most postural-suprapostural studies use a cognitive task as the suprapostural task.
However, a motor-suprapostural task can increase the phenomenon of resource-
competition or resource-sharing.
28,29
Besides, a motor-suprapostural task is verycommon in our daily life, such as cooking on moist floor or texting on the bus. In the
present study, we would choose a motor task, precision-grip task, as the suprapostural
task.
1.4 Purpose and Significance
The purpose of this study was to investigate the effects of different task prioritization
(PF vs. SF) on postural-suprapostural performance and its related cortical activity in
younger and older populations. The significance of the present study was addressed in the
academic and clinical aspects. In the academic aspect, this study provided a better insight
of the behavioral results and neural mechanism of attentional allocation under different
14
task prioritization in both younger and older populations. Especially, through this study,
we could clarify the applicability of “facilitatory hypothesis” or “posture-first principle”
with behavioral and cortical evidences (Figure 1). In clinical aspect, the results may
provide the clinical value for the physical therapists to instruct older adults who have
multi-tasking difficulty with a suitable movement strategy in their daily life and prevent
them from falling.
1.5 Hypotheses
1. Both postural and suprapostural performance are different between a postural-
suprapostural task with PF or SF strategy. In addition, the suitable task-priority
strategy for younger and older adults is different. These hypotheses would be
systematically tested by postural and suprapostural accuracy, postural regularity and
reaction time of the suprapostural task. We expected that optimal postural-
suprapostural overall performance was found with SF strategy in younger adults,
whereas optimal postural-suprapostural overall performance was found with PF
strategy in older adults.
2. Attentional resource allocation between postural and suprapostural tasks is different
depending the participants performing a postural-suprapostural task with PF or SF
15
strategy. This hypothesis would be tested by P1, N1, and P2 amplitudes of ERP
signals, for representing the allocated attention for posture and supraposture
respectively. We expected that P1, N1, and P2 amplitudes were significantly affected
between PF and SF strategies. Moreover, frontal area was found related to
information processing of working memory under dual-task condition and motor-
type suprapostural task was found related to parietal area.
32,41,42
Therefore,significant effects were expected found in frontal and parietal areas when adopting
PF and SF strategies.
16
Chapter 2 Methods
2.1 Participants
Thirty two healthy right-handed volunteers (16 younger adults, mean age: 24.4 ± 4.6
years; 16 older adults, mean age: 69.1 ± 2.7 years) without history of neurological,
vestibular, orthopedic, or cardiovascular disorders were recruited in this study. All
subjects had normal or corrected-to-normal vision. For older subjects, they were able to
ambulate independently without walking aids and had no history of falling. Besides, Mini
Mental State Examination (MMSE) score was measured for older adults and only the
subjects with more than 24 points were included (Appendix 1). Because the subjects were
asked to perform an suprapostural task while standing on a stabilometer (67-cm length ×
50-cm width × 24-cm height, anterior-posterior tilting angle: 0-100 degrees), the subjects
who were pregnant, had prior experience with tasks, unable to maintain balance on the
stabilometer for at least 80 seconds, or took any medications that could affect balance
were excluded from this study. Telephone interview with the subjects was done before
recruiting. Table 1 is the demographic data of both younger and older groups.
The protocol was approved by the research ethics board at the National Taiwan
17
University Clinical Trail Center (Appendix 2). Study procedure was explained by the
researcher for each subject and an inform consent was signed by the subjects prior to
participating in this experiment.
2.2 System Set-up and Data Recording
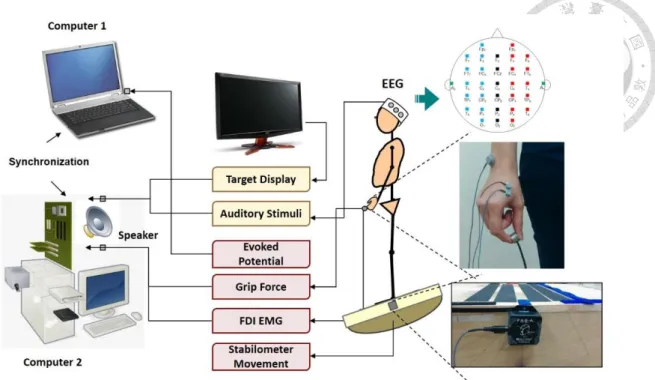
The experiment consisted of postural task and suprapostural task. Participants were
requested to perform a force-matching precision grip task with their right index and thumb
(suprapostural task) while standing on a stabilometer (postural task) (Figure 2). For the
postural task, participants were asked to maintain their balance on the stabilometer (67-
cm length × 50-cm width × 24-cm height, anterior-posterior tilting angle: 0-100 degrees)
with an inclinometer (Model: FAS-A, MicroStrain, USA) mounted on the center of the
stabilometer plate to measure the tilting angle of the stabilometer. The maximal anterior
tilting was recorded for each participant before the experiment and the 50% of the
maximal anterior tilting angle was set as the target angle for the postural task. For the
suprapostural task, participants were asked to execute a force-matching task, and the level
of force output was recorded with a load cell (15-mm diameter × 10-mm thickness, net
weight = 7 grams; Model: LCS, Nippon Tokushu Sokki Co., Japan). Maximum voluntary
contraction (MVC) of precision grip was also recorded before the experiment and the
18
50% of the MVC force was set as the target force for the suprapostural task. The
participants needed to execute the thumb-index precision grip task in response to auditory
cues. The auditory cues consisted of 80-second sequences of tone pips, with a total of
fifteen warning-executive signal pairs. The interval between a warning tone (frequency:
800 Hz, duration: 100 ms) and an executive tone (frequency: 500 Hz, duration: 100 ms)
was 1.5 seconds for the first three warning-executive pairs, but was random presented at
different intervals of 1.5, 1.8, 2.1, 2.4, 2.7 or 3.0 seconds form the fourth to fifteenth
warning-executive pairs. The interval between the executive tone and the next warning
tone was 3.5 seconds. Participants performed a quick thumb-index precision grip (force
impulse duration < 0.5 second) to couple the peak precision force with the force target
when receiving the executive tone. In order to determine the reaction time (RT) of force-
matching, the initial activation of the first dorsal interosseous (FDI) muscle was recorded
with surface electromyogram (EMG) in a bipolar arrangement (Ag/AgCl, 1.1 cm in
diameter, Model: F-E9M-40-5, GRASS) and an AC amplifier (gain: 5000, cut-off
frequency: 1 and 300 Hz; Model: QP511, GRASS).
For recording cortical activation, electroencephalogram (EEG) data was recorded
from a 32 Ag-AgCl scalp electrodes with a NuAmps amplifier (NeuroScan, EI Paso, TX).
The placement of the EEG electrodes was according to the 10-20 International System at
the following locations: Fp
1/2
, Fz
, F3/4
, F7/8
, FT7/8
, FCz
, FC3/4
, FC7/8
, Cz
, C3/4
, CPz
, CP3/4
,19
P
z
, P3/4
, T3/4
, TP7/8
, Oz
, and O1/2
. The ground electrode was placed along the midline aheadof F
z
and the recording references were placed on the mastoids of the both sides. Inaddition, two electrodes were attached above the arch of the left eyebrow and below the
eye to monitor eye movements and blinks. The impedances of all electrodes were
maintained below 5 kΩ, and data was recorded with a band-pass filter set at 0.1 to 100
Hz with a notch filter at 60 Hz to remove the noise from the environment. Both behavioral
and cortical signals, including stabilometer movement, precision grip force, EMG of FDI
muscle, and EEG data, were synchronized with a sampling rate of 1 kHz.
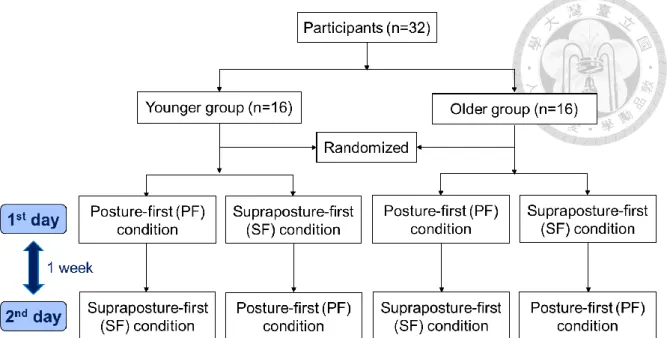
2.3 Experimental Conditions and Procedures
This study was conducted in two separate days with one-week apart. Participants in
both age groups were randomly assigned to either PF or SF conditions in the first day and
to the other in the second day (Figure 3). In each experimental day, participants were
requested to perform three experimental tasks, including one postural-suprapostural task,
and two corresponding control tasks (a single corresponding postural task and a single
corresponding suprapostural task). There were six trials for each experimental task.
In most previous researches related to task prioritization, the lack of specification
instruction for how participants directing their attention when performing dual tasks was
20
a major limitation.
16
For the better improvement of task prioritization instruction, aprocedure derived from “optimum-maximum method” proposed by Navon (1990) was
used in this study for manipulating task prioritization.
40
The optimum-maximum methodwas used to guard subjects’ attention with specific instruction for both high-priority and
low-priority tasks.
23,43
With this method, the high-priority task was designed the “to-be-optimized” task, and low-priority task was the “to-be-maximized” task. Participants were
instructed to execute the high-priority task with their “optimum” level and to perform
their best on the low-priority task. Such a procedure required participants to optimize the
high-priority task and not to “give up” on the low-priority task. Besides, individually
determined performance standard and performance feedback were provided in the high-
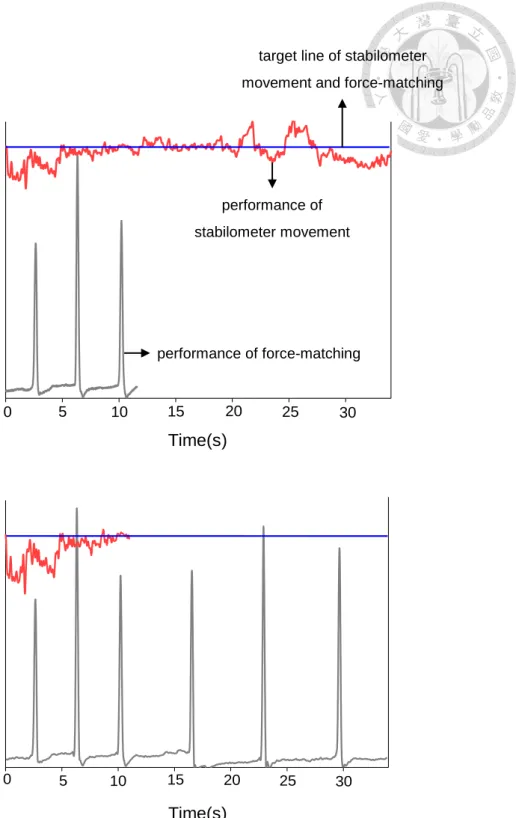
priority task but not for low-priority task. Therefore, in this study, visual feedback about
the target and performance of stabilometer movement or force-matching task was used
for enhancing the prioritization of the attention (Figure 4). For example, participants in
the PF condition were instructed to pay their primary attention on the postural task with
maintaining the tilting angle of the stabilometer at the target angle precisely, and to
maximize the precision of force-matching task. Visual feedback of stabilometer target
angle and instantaneous stabilometer tilting angle was provided in the PF condition, but
visual information about the force-matching target and force output was not provided.
Because the visual feedback was only provided for postural performance, the
21
corresponding control tasks of the PF condition were that 1) performing the postural task
on the stabilometer with visual feedback and did not execute the force-matching task, and
2) performing the force-matching task without visual feedback on a stable box (67-cm
length × 50-cm width × 24-cm height). In contrast, participants in the SF condition were
instructed to pay their major attention on the precision grip task with coupling the force
peak with the target precisely, and to maximize the precise tilting angle of the stabilometer.
Visual feedback of the force-matching target and force output was provided in the SF
condition, but visual information about the stabilometer and its target angle was not
provided. The corresponding control tasks of the PF condition were that 1) performing
the postural task on the stabilometer without visual feedback and did not execute the
force-matching task, and 2) performing the force-matching task with visual feedback on
a stable box (67-cm length × 50-cm width × 24-cm height). Besides, in order to remind
the force-matching target for the PF condition and the tilting angle target for the SF
condition, the visual feedback about the first 3 force-matching performances and the first
10-second stabilometer tilting angle with their target was provided in each trial for the PF
and the SF conditions, respectively. All the visual information was displayed on a 22-inch
computer monitor with 60 cm in front of the subjects at eye-level.
22
2.4 Data Analysis
2.4.1 Behavioral Data
For postural performance, the inclinometer data was conditioned with 6-Hz low-pass
filter and the units were converted to degrees. The inclinometer data from every executive
tone to next warning tone was selected for calculation of absolute postural error and
absolute postural approximate entropy (ApEn). The absolute postural error was presented
by calculating the root mean square (RMS) of the mismatch between the target angle and
the stabilometer tilting angle and then divided by the target angle, presenting as
RMS(SA-TA)
×100%
TA
(SA: stabilometer tilting-angle, TA: target angle). The absolute postural ApEn of the stabilometer tilting angle’s trajectory was used to represent thevariability property of the postural performance. According to previous study, the
calculation of postural ApEn was calculated after the trajectory of stabilometer tilting
angle normalized with standard deviation of time series, presenting as ApEn (m, r) =
log[C
m
(r)/Cm+1
(r)].44
Where m represents the length of the compared time windows and rrepresents the tolerance range of the regularity.
44-46
If a completely predictable time-serieswith high regularity, value of C
m
(r) will be very close to Cm+1
(r), yielding a log-probability(ApEn) of zero.
44
In this study, m equaled 2 and the tolerance range of r was 0.15× the23
standard deviation of the time series
44
. The value of the ApEn was between 0 and 2. AnApEn value of closer to 2 represented higher irregularities, or larger complexity of the
postural movement changes. In contrast, an ApEn value of closer to 0 represented greater
regularity.
47
For suprapostural performance, the absolute force-matching error was presented as PPF-TF
×100%
TF (PPF: peak precision-grip force, TF: target force). The absolute force- matching RT of suprapostural task was recorded by calculating the time delay from the
presentation of executive tone to the EMG onset of FDI muscle. All behavioral
parameters of postural-suprapostural task were normalized in reference to its
corresponding control task.
_ _
postural-suprapostural 100%
corresponding control
absolute value normalized value
absolute value
2.4.2 ERPs Data
The manipulation of Event-related potentials (ERPs) data mainly referred to the
previous ERP study.
32
The recorded EEG data was processed with NeuroScan’s 4.3software (NeuroScan Inc., EI Paso, TX, USA) and the off-line analysis was used for the
analysis. The DC shift of each channel on entire EEG data was corrected with third-order
24
correction. The eye movements and blinks were removed from the EEG data. After eye
movements were removed, the EEG data was low-pass filtered with cut-off frequency of
40 Hz (48 dB/octave), and segmented into epochs of 700 ms, including a 100 ms before
the onset of executive signals. The 100 ms-data prior the executive signals was used for
the baseline correction of each EEG epoch. A visual inspection for each epoch was
applied, and those epochs with artifacts, including excessive drift, eye movements or
blinks, were removed from analysis. Those epochs with adequate responses were
averaged. ERPs from the six trials of each task were group averaged separately at each
condition for each subject. According to the previous ERP studies, P1 amplitude was
reported associated with sensory input to attended task
38
, N1 was associated with theattention modulation related to postural control, and P2 was associated with the attention
modulation related to perceptual-motor suprapostural task,
32,44
Therefore, in the presentstudy, we analyzed the peak amplitudes of P1 (70-110 ms), N1 (80-150 ms), and P2 (150-
240 ms) components across all EEG electrodes to characterize the attention allocation
between postural and precision-grip tasks.
2.5 Statistical Analysis
The task prioritization conditions (PF condition, SF condition) and age groups
25
(younger group, older group) effects on behavioral and electrophysiological parameters
of postural and suprapostural tasks, including the normalized force-matching error,
normalized force-matching RT, normalized postural error, normalized postural ApEn, and
ERP amplitudes of P1, N1, and P2 components were compared with 2 × 2 mixed analysis
of variance (ANOVA). When necessary, post hoc least significant difference (LSD)
comparisons were performed. The level of significance was set at p < 0.05. Signal
processing of behavioral data and statistical analysis was completed by using MatLab v.
R2008a (Mathworks, Natick, MA, USA) and the statistical package for SPSS statistics v.
17.0 (SPSS Inc., Chicago, IL, USA).
26
Chapter 3 Results
3.1 Behavioral Performance
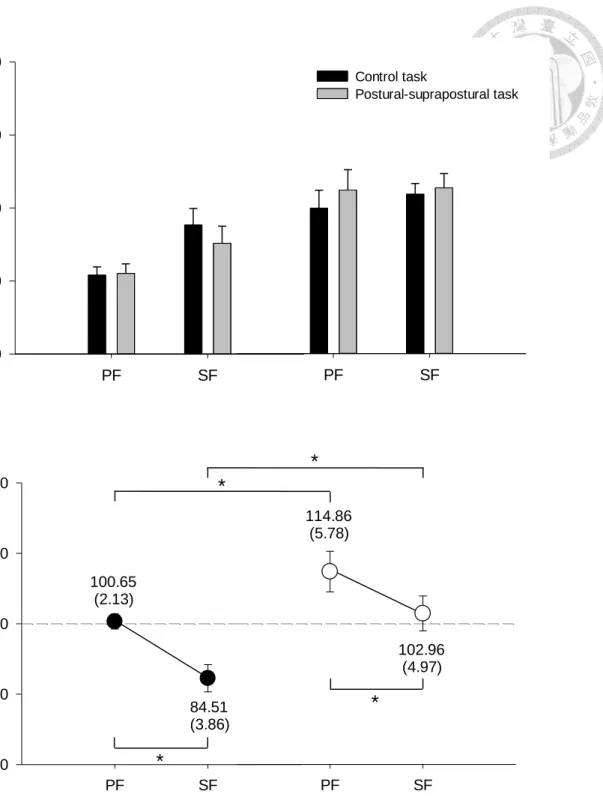
3.1.1 Error and Regularity of Postural Performance
Figure 5 shows the absolute and normalized postural error of SF and PF conditions
in the younger and older groups. ANOVA results suggested that normalized postural error
was subject to task prioritization (F
1, 30
= 12.99, p < 0.01) and age difference (F1, 30
= 11.28,p < 0.01) without interaction (F 1, 30
= 0.30, p = 0.59). Larger normalized postural errorwas observed in the PF condition than that in the SF condition for both younger and older
groups (p < 0.05). Besides, normalized postural error was larger in the older group than
that in the younger group across task prioritization conditions (p < 0.05). The normalized
postural error of SF condition in the younger group was below 100% (84.51 ± 3.86%),
but the others were above 100%, indicating that younger adults had better postural
performance during the postural-suprapostural dual-task condition than that during the
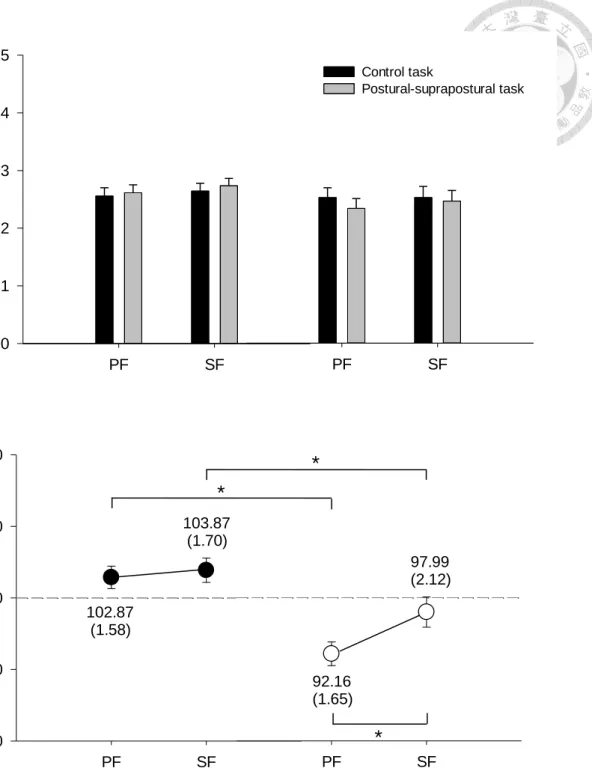
single postural task condition. For postural regularity, Figure 6 displayed the absolute and
normalized postural ApEn results of SF and PF conditions in the younger and older
27
groups. ANOVA results showed a significant main effect of task prioritization (F
1, 30
=4.41, p < 0.05) and age difference (F
1, 30
= 18.82, p < 0.001) on the normalized ApEnvalues without a significant interaction (F
1, 30
= 2.21, p < 0.15). Post-hoc testing showeda larger normalized ApEn in the younger group than that in the older group (PF condition:
younger (102.87 ± 1.58%) > older (92.16 ± 1.65%)), p <0.01; SF condition: younger
(103.87 ± 1.70%) > older (97.99 ± 2.12%), p <0.05), indicating that younger adults had
higher postural irregularity when performed a postural-suprapostural task than older
adults. Also, we noted that normalized ApEn was above 100% in the younger for both PF
and SF conditions, but was below 100% in the older group, indicating that addition of the
force-matching task led to an opposite effect on postural regularity between younger and
older groups. On the other hand, the task prioritization effect on normalized ApEn was
only shown in the older group with larger value in the SF condition than that in the PF
condition (p < 0.05).
3.1.2 Error and Reaction Time of Force-matching Task
For suprapostural performance, force-matching error of PF and SF conditions in
younger and older groups is shown in Figure 7. ANOVA results suggested that normalized
force-matching error was subject to task prioritization (F
1, 30
= 12.31, p < 0.01), but not to28
age effect (F
1, 30
= 2.25, p = 0.14) with no significant interaction effect (F1, 30
= 1.69, p <0.20). Post-hoc evaluation revealed that normalized force-matching error in older group
was higher in PF condition than that in SF condition (p < 0.05). Besides, all normalized
force-matching errors were above 100% (younger group: PF condition = 118.90 ± 5.63%,
SF condition = 103.16 ± 5.49%; older group: PF condition = 139.88 ± 11.57%, SF
condition = 105.65 ± 5.31%), indicating that force-matching error tended to increase
when subjects were requested to perform a force-matching task and kept their balance on
a stabilometer concurrently compared to perform the force-matching task in a stable
posture (stand on a stable box).
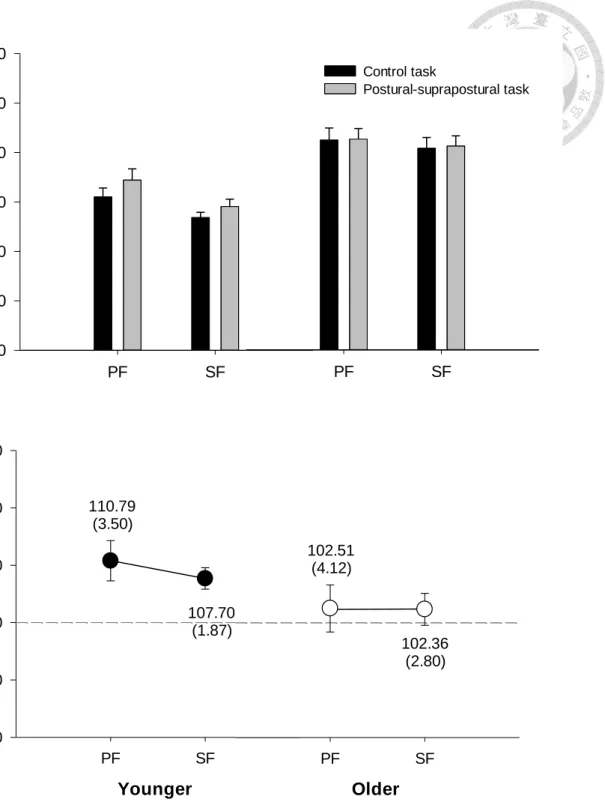
Figure 8 displays the RT of force-matching task of PF and SF conditions in younger
and older groups. Similar as force-matching error, all normalized force-matching RT
values were above 100% (younger group: PF condition = 110.79 ± 3.50%, SF condition
= 107.70 ± 1.87%; older group: PF condition = 102.51 ± 4.12%, SF condition = 102.36
± 2.80%), indicating that RT would be longer when subjects were requested to perform a
force-matching task and kept their balance on a stabilometer concurrently compared to
perform the force-matching task in a stable posture. However, the RT of force-matching
did not vary with either task-priority strategy or age difference (task-priority effect: F =
0.48, p = 0.50; age effect: F = 3.15, p = 0.09).
29
3.2 ERP Amplitudes
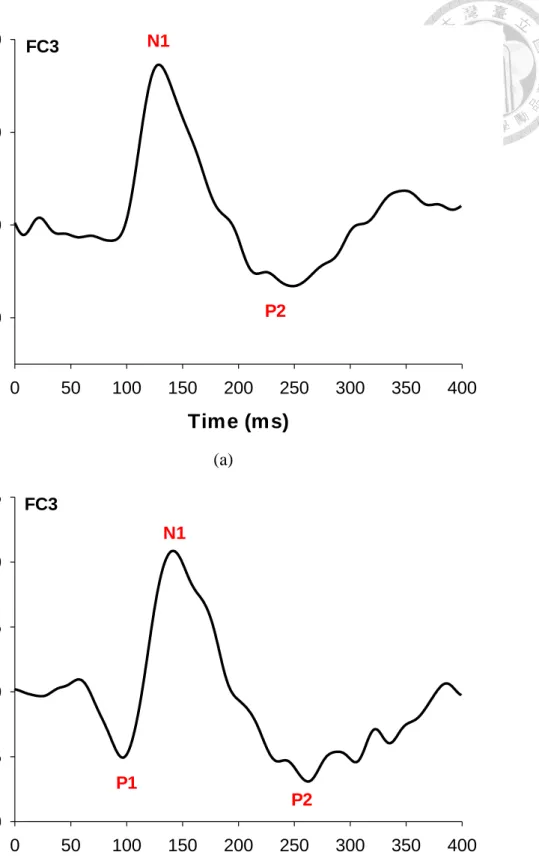
Figure 9 displays the typical ERP waveforms of younger group and older group in
postural-suprapostural tasks. It is interesting to find that the ERP characteristics were
different between the younger and older groups. In the younger group, only the N1 and
P2 waves presented after the presentation of the executive signals across postural-
suprapostural conditions (Figure 9(a)); however, the P1, N1, and P2 waves were all
observed in sequence after the presentation of the executive signals in the older group
(Figure 9(b)). Therefore, for statistical analysis of ERP amplitude, N1 and P2 amplitudes
were analyzed via a 2 (task prioritization: PF vs. SF) × 2 (age: younger vs. older) mixed
ANOVA, with repeated measure on the first variable, while P1 amplitudes was analyzed
via a paired t-test to examine the task prioritization effect for the older adults.
3.2.1 Task Prioritization Effect on ERP Amplitudes
Figures 10(a-e) are typical ERP recordings showing the effects of task prioritization
P1, N1, and P2 amplitudes. ANOVA results suggested that in the younger group, the N1
amplitudes of most electrodes around left frontal (F
3
: F1, 30
= 9.34, p < 0.01; FC3
: F1, 30
=9.05, p < 0.01), central (C
3
: F1, 30
= 8.93, p < 0.01) and parietal (CP3
: F1, 30
= 21.26, p <30
0.001; P
3
: F1, 30
= 16.36, p < 0.001) cortices, and midline electrodes (FCz
: F1, 30
= 4.37, p< 0.05; C
z
: F1, 30
= 6.61, p < 0.05) were subject to a significant task prioritization effect.Post-hoc analysis further indicated that the N1 amplitudes on these electrodes (F 3
, FC3
,FC
z
, C3
, Cz
, and CP3
,) in the PF condition was generally greater than that in the SFcondition (p < 0.05)(Figure 11(a)). On the other hand, a significant supraposture effect on
P2 amplitude was noted in the left temporal (T
5
: F1, 30
= 6.32, p < 0.05) and parietal (Pz
:F
1, 30
= 4.68, p < 0.05) cortices. Besides, some electrodes had significant interactionbetween task prioritization and age factors on P2 amplitudes (T
5
: F1, 30
= 4.90, p < 0.05;P
3
: F1, 30
= 4.28, p < 0.05; O1
: F1, 30
= 4.47, p < 0.05). Further post-hoc analysis indicatedthat P2 amplitudes on T
5
, P3
, PZ
, and O1
electrodes were greater in the SF condition thanthat in the PF condition (p < 0.05)(Figure 11(b)).
For the older group, paired t-test revealed that compared to with PF strategy, P1
amplitudes were larger at frontal (FC
3
and F8
), central (C3
and CZ
), parietal (CP3
, CPZ
, PZ
and P
4
), and right temporal (FT8
and T4
) areas with SF strategy (p < 0.05)(Figure 11(c)).ANOVA results suggested that the N1 amplitudes of the electrodes around parietal (CP
3
:F
1, 30
= 21.26, p < 0.001; CPZ
: F1, 30
= 8.97, p < 0.01; P3
: F1, 30
= 16.36, p < 0.001; PZ
: F1,
30
= 7.39, p < 0.05) and temporal (T5
: F1, 30
= 10.81, p < 0.01) areas were subject to a significant task prioritization effect. Post-hoc testing showed that N1 amplitudes on theseelectrodes (T
5
, CP3
, CPZ
, P3
, and PZ
) were larger in the PF condition than that in the SF31
condition (p < 0.05)(Figure 11(d). On the other hand, the P2 amplitudes of electrode FT
8
had a significant main effect of task prioritization (F
1, 30
= 5.16, p < 0.05). Besides, someelectrodes showed significant interaction effect between task prioritization and age
factors around right frontal (F
8
: F1, 30
= 4.39, p < 0.05; FT8
: F1, 30
= 5.26, p < 0.05) andtemporal (T
4
: F1, 30
= 4.63, p < 0.05) areas. Further post-hoc analysis indicated that F8
,FT
8
, and T4
electrodes had larger P2 amplitudes in the PF condition than that in the SFcondition (p < 0.05)(Figure 11(e)).
3.2.2 Age Effect on ERP Amplitudes
The age effect on N1 and P2 amplitudes is displayed in Figures 12(a)-(b). For the
PF condition, ANOVA results revealed a significant main effect of age difference on N1
amplitudes at frontal (F
3
: F1, 30
= 5.60, p < 0.05; FC3
: F1, 30
= 4.86, p < 0.05), central (C3
:F
1, 30
= 5.14, p < 0.05), and parietal (CP3
: F1, 30
= 4.86, p < 0.05; CPZ
: F1, 30
= 4.22, p <0.05; P
3
: F1, 30
= 4.95, p < 0.05) areas. Post-hoc evaluation showed that the N1 amplitudeof these electrodes (F
3
, FC3
, C3
, CP3
, CPZ
, and P3
) in the older group was generally greaterthan that in the younger group (p < 0.05)(Figure 12(a)). However, the P2 amplitude was
independent of the age effect for all cortical areas in the PF condition (p > 0.05)(Figure
12(b)).
32
For the SF condition, ANOVA results revealed the a significant main effects of age
groups difference on N1 amplitudes at left fronto-parietal cortex (F
3
: F1, 30
= 5.60, p <0.05; FC
3
: F1, 30
= 4.86, p < 0.05; C3
: F1, 30
= 5.14, p < 0.05; CP3
: F1, 30
= 4.86, p < 0.05;P
3
: F1, 30
= 4.95, p < 0.05) with larger N1 amplitudes in the older group (Figure 12(c)). Onthe other hand, ANOVA results showed a significant main effects of age difference on P2
amplitudes at occipital area (O
1
: F1, 30
= 4.40, p < 0.05; Oz
: F1, 30
= 6.94, p < 0.05; O2
: F1,
30
= 4.55, p < 0.05) and a significant interaction between task prioritization and age factors at Pz
electrode (F1, 30
= 4.47, p < 0.05)(Figure 12(d)). Post-hoc analysis indicated that P2amplitudes on these electrodes (P
Z
, O1/2
, and Oz
) were greater in the younger group thanthat in the older group (p < 0.05).
Figure 13 displays the topological plots of the younger and older groups in each
postural-suprapostural condition. It seems that task prioritization affected the activation
duration of N1 and P2 waves in the younger and older groups respectively. In the younger
group, with activation duration of N1 wave was shorter in the SF condition and P1
activation of the older group seemed earlier in the SF condition than in the PF condition.
In addition, the age difference also affected the activation of N1 and P2, with greater
activation intensity and area of N1 wave in the older group but greater activation intensity
and area of P2 wave in the younger group.
33
Chapter 4 Discussions
4.1 Improved Task Accuracy with SF Strategy
The results showed significant task prioritization effect on postural and
suprapostural tasks in both younger and older adults. First, better postural/ suprapostural
performance was found in both age groups when paying major attention on force-
matching task in postural-suprapostural task (Figures 5, 7), which in line with some
studies related to task prioritization.
17,48
Burcal et al. (2014) showed greatest posturalimprovements when focusing on suprapostural task compared with focusing on balance
and no focusing instruction.
48
Jehu et al. (2015) also reported that less postural sway wasobserved when prioritizing reaction time task than prioritizing posture.
17
These researchessuggested that focusing on suprapostural task allowed attention shifted attention away
from control of posture, leading to more automatic and efficient postural control. The
results may also support the constrained-action hypothesis, which proposed that
consciously controlling posture or movement close to the body may interfere with the
automatic control processes and thus negatively affected postural performance.
49
Inaddition, the postural improvement with SF strategy was also consistent with the
34
facilitatory pattern in adaptive-resource sharing model, which proposed that postural
stability may get improved in order to facilitate suprapostural performance.
6,8
Thefacilitatory effect was especially dominant in the older adults, because both force-
matching error and postural error was less in the SF condition than that in the PF condition
(Figures 5, 7). However, Yogev-Seligmann et al.’s study (2010) reported the opposite
results.
19
In the study, subjects (younger and older adults) were requested to perform acognitive task (verbal fluency task) during walking with different attention instruction,
including no specific prioritization instructions, prioritization of gait and prioritization of
the verbal fluency task. They found that gait speed was reduced when prioritization was
given to the verbal fluency task in both age groups, indicating that SF strategy might
decreased postural performance. The discrepancy between our results and Yogev-
Seligmann et al.’s finding may result from different type of suprapostural task. With a
motor suprapostural task, such as force-matching, attentional resource would be enforced
to integrate for optimal outcome.
On the other hand, postural performance was found to be significantly better in the
younger group than that in the older group for both PF and SF conditions. Age-related
decline of postural performance in older adults may represent the inability to adequately
allocate attentional resource between two tasks and inefficient postural control in older
adults.