服務 Service 信賴 Trust 關懷 Mercy
王 中 敬
天主教聖馬爾定醫院 醫療副院長 副教授
7 February, 2015
成人夜尿治療和現況
服務 Service 信賴 Trust 關懷 Mercy
Nocturia, defined by ICS as waking to void during the night, is a common manifestation of BPH, that is not only bothersome but can also have a negative impact on QoL and sleep patterns,
potentially leading to traumatic falling accidents.
The prevalence of nocturia in older men is high and increases with age: a systematic review on this subject showed that in men in their 70s and 80s, 68.9–93% reported at least 1 void per night, and 29–59.3% reported at least 2 voids per night. Up to 61% of elderly women and up to 59% of elderly men report two or more voids per night; [Bosch JL, J Urol 2010;184(2):440–6.]
服務 Service 信賴 Trust 關懷 Mercy
Nocturnal polyuria, defined by ICS as a nocturnal urine output (including the first morning void) of >33% of the total 24-h voided volume in the elderly, is one of the main causes(80%) of nocturia.
An Austrian study in nocturia patients showed that 50% of all men had NP. [Klingler HC, Neurourol Urodyn 2009;28(5):427–31.].
van Doorn et al. pointed out that in a general population of older men the prevalence of NP according to this definition is very high as well: it ranges from 41.8% in 50–55 year-old men to 56.9% in 70–78 year old men [van Doorn, Neurourol Urodyn 2009;28(7):765–6.35].
服務 Service 信賴 Trust 關懷 Mercy
3-day FV chart should be included as an integral part of the evaluation for LUTS in both sexes, because FV
charts may provide more accurate information regarding nocturia.
[Ja Hyeon Ku, Urol Res (2004) 32: 181–4; UROLOGY (2004) 64:966–9.]
[Matthiesen TB et al, BJU international (1999) 83:1017-1022.]
服務 Service 信賴 Trust 關懷 Mercy
Management of Nocturia
Behavioural therapy(Lifestyle modifications, Alarm Therapy)
Pharmacotherapy: α-blockers and 5-ARI,alone or in combination Anti-muscarinics (Oxbu (5mg) , Tolterodine (2mg)) , alone or as add-on α-blocker
Timed diuretic therapy Anti-diuretic therapy
Alternative pharmacotherapy (Imipramine 25-50mg HS, tranquilizer, anxiolytic)
Surgical options
[van Doorn, Maturitas 2012;71:8–12]
服務 Service 信賴 Trust 關懷 Mercy
Kreder & Dmochowski (eds). The overactive bladder:
evaluation and management. London, UK: CRC Press, 2007
Medical treatment of the prostate is an
inefficient way to treat nocturia"
"
So these patients still experience fragmented sleep and poor QoL
服務 Service 信賴 Trust 關懷 Mercy
Chung Jing Wang et al, J Urol (2011) 185: 219-223.
• Eligible patients with BPH older than 65 years were enrolled in the study using frequency volume charts and I-PSS.
• All patients with nocturia, nocturnal polyuria and I-PSS 14 or greater were included in the study.
服務 Service 信賴 Trust 關懷 Mercy
Placebo Desmopressin p Value Mean SD pt age (range) 74.52±5.99 (65–87) 73.56±7.71 (65–88) 0.459 Mean SD history of BPH 69.55±13.36 68.60±14.35 0.723 Mean SD body mass index 24.81±2.84 25.07±2.71 0.617 No. comorbidity (%): 29 (50) 27 (47.4) 0.723 H/T cardiovascular disease 9 (15.5) 7 (12.3) 0.898 DM 10 (17.2) 10 (17.5) 0.944 DM H/T cardiovascular disease 11 (19.0) 10 (17.5) 0.514 No. α-blocker: 58 57 0.955
Tamsulosin (0.4 mg) 29 28
Doxazosin (2 mg) 14 13
Terazosin (4 mg) 14 10
Alfuzosin (10 mg) 1 6
No. antimuscarinics 21 12 0.989
服務 Service 信賴 Trust 關懷 Mercy
0 2 4 6 8
Baseline 1 3 6 12
Mean time of nocturnal voids
Time (month)
Placebo
Desmopressin
服務 Service 信賴 Trust 關懷 Mercy
0 200 400 600 800
Baseline 1 3 6 12
Mean volume of nocturnal volume
Time (month)
Placebo
Desmopressin
服務 Service 信賴 Trust 關懷 Mercy
0 20 40 60 80 100 120 140 160
Baseline 1 3 6 12
Mean duration of first sleep period
Time (month)
Placebo Desmopressin
服務 Service 信賴 Trust 關懷 Mercy
Summary of adverse events
No. Placebo No. Desmopressin
Headache 4 3
Dizziness 4 4
Nausea 1
Hyponatremia without clinical symptoms 10 9
Total adverse events (%)* 19 (32.8) 16 (28.1)
* 2-Sample independent t test p 0.972.
服務 Service 信賴 Trust 關懷 Mercy
12 month P Value
Nocturia, decrease 2,n <0.01#
Placebo 8
(13.80%)
Desmopressin 35
(61.40%)
Nocturnal volume 30% of daily total urine volume <0.01#
Placebo 11
(19.0%)
Desmopressin 35
(61.40%) First sleep period,
increase 30min,n
<0.01#
Placebo 10
(17.20%)
Desmopressin 27
(47.40%)
First sleep period,min <0.01#
Placebo 101.6
±19.5
Desmopressin 120.0
±17.7
Parameter of Flow Chart
#:2-sample independent t test
服務 Service 信賴 Trust 關懷 Mercy
Baseline 1 month 3 month
6 month 12 month Hyponatremia without
clinical manifestation
9
(15.80%)
6
(10.50%)
4 (7.02%)
3 (5.30%)
#:2-sample independent t test
Asian food style?
服務 Service 信賴 Trust 關懷 Mercy
Song et al, Int Urol Nephrol (2014) 46:1495-1499
This was retrospective cohort study, and the patients who were >65 years old and had NP and had been treated with desmopressin in tertiary center were analyzed.
The basic screening test included the recording of the patient history, a physical examination,blood pressure measurement, blood chemistry
analyses including electrolyte levels, urine analysis and in men transrectal ultrasonography and prostate-specific antigen (PSA) measurement.
All patients initially received 0.1 mg oral desmopressin (Minirin )
which was to be taken before sleep. The dose was escalated to 0.2 mg if the NUV or night-time frequency was not reduced. The dose never exceeded 0.2 mg.
The voiding diary, serum sodium level and adverse drug effects including hyponatremic symptoms were evaluated at baseline, 3–7 days after starting treatment, every 3–6 months and when the dosage was changed.
服務 Service 信賴 Trust 關懷 Mercy
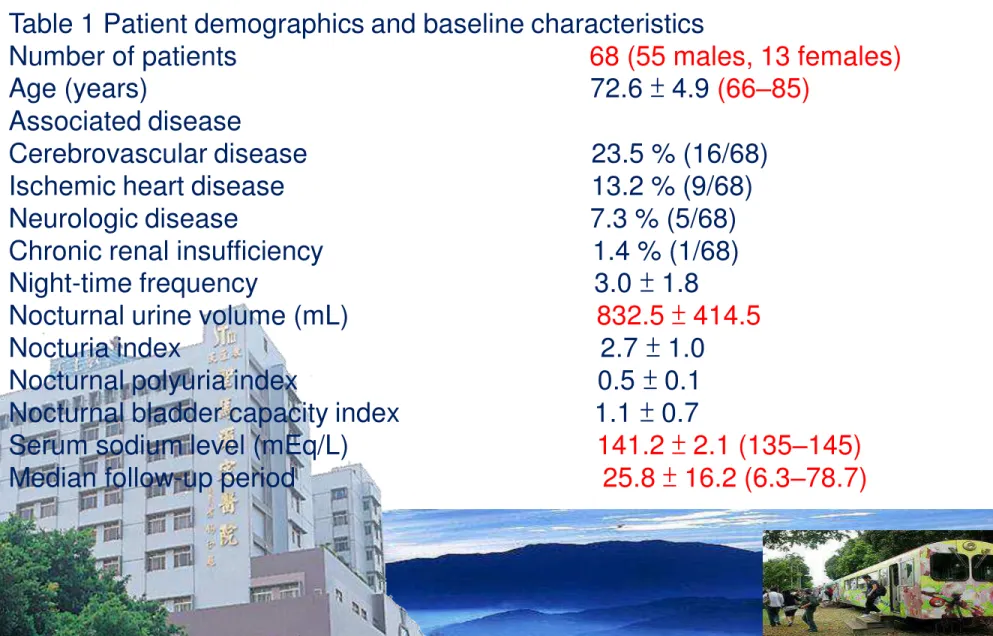
Song et al, Int Urol Nephrol (2014) 46:1495-1499
Table 1 Patient demographics and baseline characteristics
Number of patients 68 (55 males, 13 females) Age (years) 72.6 ± 4.9 (66–85)
Associated disease
Cerebrovascular disease 23.5 % (16/68) Ischemic heart disease 13.2 % (9/68) Neurologic disease 7.3 % (5/68) Chronic renal insufficiency 1.4 % (1/68) Night-time frequency 3.0 ± 1.8
Nocturnal urine volume (mL) 832.5 ± 414.5 Nocturia index 2.7 ± 1.0
Nocturnal polyuria index 0.5 ± 0.1 Nocturnal bladder capacity index 1.1 ± 0.7
Serum sodium level (mEq/L) 141.2 ± 2.1 (135–145) Median follow-up period 25.8 ± 16.2 (6.3–78.7)
服務 Service 信賴 Trust 關懷 Mercy
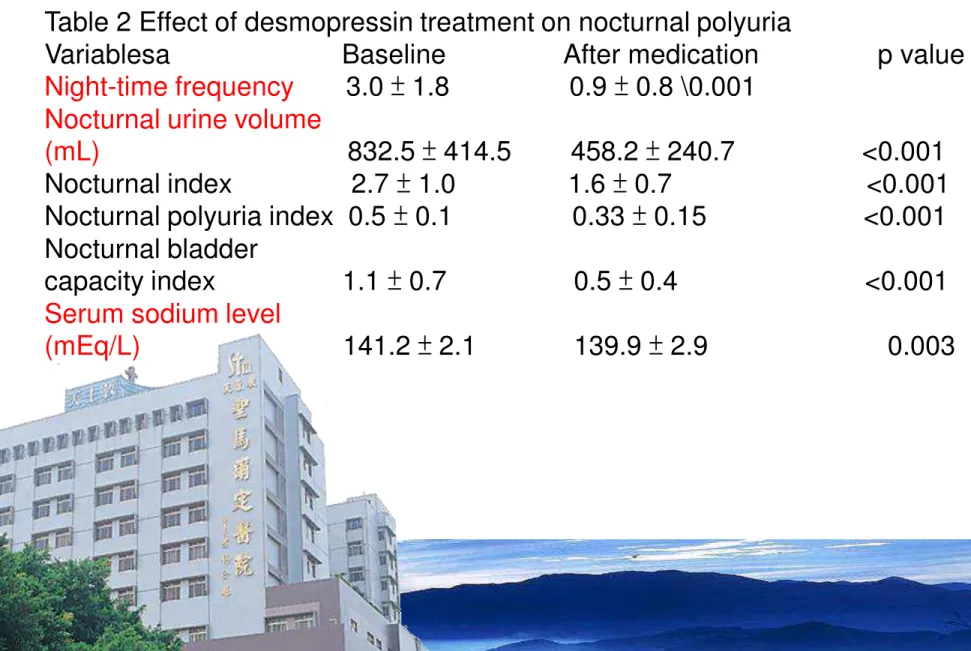
Table 2 Effect of desmopressin treatment on nocturnal polyuria
Variablesa Baseline After medication p value Night-time frequency 3.0 ± 1.8 0.9 ± 0.8 \0.001
Nocturnal urine volume
(mL) 832.5 ± 414.5 458.2 ± 240.7 <0.001 Nocturnal index 2.7 ± 1.0 1.6 ± 0.7 <0.001 Nocturnal polyuria index 0.5 ± 0.1 0.33 ± 0.15 <0.001 Nocturnal bladder
capacity index 1.1 ± 0.7 0.5 ± 0.4 <0.001 Serum sodium level
(mEq/L) 141.2 ± 2.1 139.9 ± 2.9 0.003
服務 Service 信賴 Trust 關懷 Mercy
Conclusions
Long-term treatment with desmopressin is safe and effective for NP in elderly patients if the patients are well informed about the
disease and are closely followed up.
服務 Service 信賴 Trust 關懷 Mercy
Woong JB et al, J Urol (2014) 190: 180-186
Desmopressin Add-On Therapy for Refractory Nocturia in Men Receiving Blockers for Lower Urinary Tract Symptoms
Purpose: Alpha-blockers improve lower urinary tract symptoms associated with benign prostatic obstruction. Nocturia, a storage symptom, is a common complaint in men. However, it does not fully respond to blocker therapy, likely due to its multifactorial pathophysiology. We evaluated the
efficacy and safety of desmopressin as add-on therapy for refractory nocturia in men previously treated with an blocker for lower urinary tract symptoms.
Materials and Methods: Eligible patients were men 50 years old or older with lower urinary tract symptoms and persistent nocturia despite blocker treatment for a minimum of 4 weeks. The
optimum dose of oral desmopressin was determined during a 4-week dose titration period and this dose was maintained for 24 weeks. Flow volume charts, International Prostate Symptom Score total and subscores, uroflowmetry and post-void residual urine volume were assessed.
Results: A total of 216 patients were enrolled in the study. Of these patients there were 158 (76%) with nocturnal polyuria, 15 (7.2%) with decreased nocturnal bladder capacity and 35 (16.8%) with nocturia due to both causes. The number of nocturnal voids significantly decreased from a baseline mean of 7.0 to 5.7 episodes for 3 days at the 24-week visit. The average International Prostate
Symptom Score total and subscore significantly decreased by 4 weeks and were maintained at 24 weeks. In patients younger than 65 years, International Prostate Symptom Score voiding subscores were significantly improved at 24 weeks compared to those age 65 years or older.
Conclusions: Desmopressin add-on therapy for refractory nocturia in men previously
treated with an blocker for lower urinary tract symptoms improved voiding symptoms as well as nocturia, storage symptoms.
服務 Service 信賴 Trust 關懷 Mercy
服務 Service 信賴 Trust 關懷 Mercy
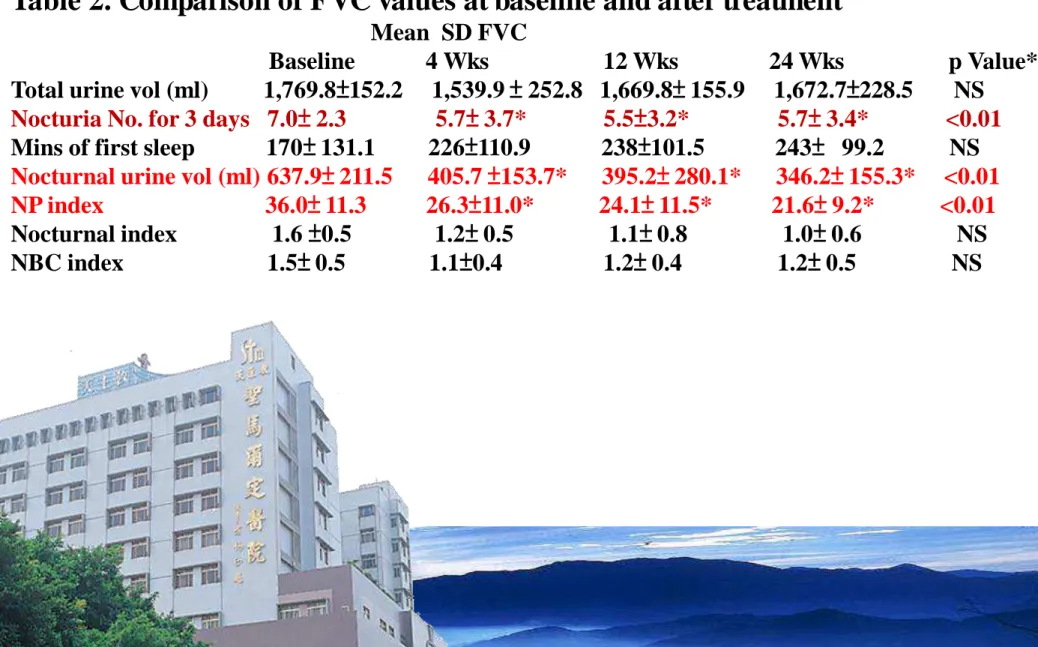
Table 2. Comparison of FVC values at baseline and after treatment
Mean SD FVC
Baseline 4 Wks 12 Wks 24 Wks p Value*
Total urine vol (ml) 1,769.8±152.2 1,539.9 ± 252.8 1,669.8± 155.9 1,672.7±228.5 NS Nocturia No. for 3 days 7.0± 2.3 5.7± 3.7* 5.5±3.2* 5.7± 3.4* <0.01 Mins of first sleep 170± 131.1 226±110.9 238±101.5 243± 99.2 NS Nocturnal urine vol (ml) 637.9± 211.5 405.7 ±153.7* 395.2± 280.1* 346.2± 155.3* <0.01 NP index 36.0± 11.3 26.3±11.0* 24.1± 11.5* 21.6± 9.2* <0.01 Nocturnal index 1.6 ±0.5 1.2± 0.5 1.1± 0.8 1.0± 0.6 NS NBC index 1.5± 0.5 1.1±0.4 1.2± 0.4 1.2± 0.5 NS
服務 Service 信賴 Trust 關懷 Mercy
Desmopressin in the treatment of nocturia:clinical evidence and experience Fara M. Friedman and Jeffrey P. Weiss Ther Adv Urol (2013) 5(6) 310–317
服務 Service 信賴 Trust 關懷 Mercy
Conclusion
A number of studies have in fact demonstrated its efficacy in decreasing nocturia severity while improving quality of life as compared with placebo. The safety of desmopressin, however, is paramount to its clinical utility. Desmopressin is generally well
tolerated, the newer ‘melt’ formulation at lower doses being nearly as effective and better tolerated than tablet (‘high dose’). A
minimum dosage of 25 μg orally disintegrating sublingual
desmopressin appears to be ideal for women, whereas men may benefit from a minimum of 50 μg. Regardless of formulation or dosing, judicious care should be taken for elderly patients
(≥65 years of age) due to the increased risk of hyponatremia in such vulnerable individuals.
服務 Service 信賴 Trust 關懷 Mercy
Desmopressin for the treatment of female storage lower urinary tract symptoms Konstantinos Giannitsas, Anastasios Athanasopoulos
World J Obstet Gynecol 2014 February 10; 3(1): 7-13
服務 Service 信賴 Trust 關懷 Mercy
Conclusion
The switch to desmopressin tablet and more recently to the orally disintegrating formulation has been associated with a decrease in the incidence of hyponatremia[23,24]. Indeed, in all the recently reviewed trials for the role of desmopressin in the management of female
storage LUTS, the incidence of hyponatremia and more specifically of clinically relevant hyponatremia was low. The superior
pharmacokinetic and pharmacodynamic properties of the orally administered formulations are only one of the reasons for this
observation[25-27]. Another reason is the identification of age and low baseline plasma sodium concentration as important risk factors for
hyponatremia[23]. Finally, the awareness of a lower minimum effectivedose in female patients compared to males[12] has led to more appropriate dosing The incidence of hyponatremia is currently less than3%[23]. Evidence in this review suggests that desmopressin is currently a well-tolerated and safe treatment for females with LUTS.
服務 Service 信賴 Trust 關懷 Mercy
Weiss et al. BJU Int 2011;108:6–21
Combination therapy of desmopressin with α-blocker and antimuscarinics can address night-time as well as
… Day-Time LUTS,
… in both Men and Women
服務 Service 信賴 Trust 關懷 Mercy
A Systematic Review of the Efficacy and Safety of Desmopressin for Nocturia in Adults
Mark H. Ebell,* Taylor Radke and Jack Gardner
J Urol 192, 829-835, September 2014
服務 Service 信賴 Trust 關懷 Mercy
Materials and Methods: After a literature search we identified 10 articles (2,191 patients) that met our inclusion criteria of parallel group design, randomized, controlled trials with information on at least 1 benefit or harm of desmopressin inpatients with nocturia. We evaluated the quality of included trials based on The Cochrane Collaboration criteria, assessed heterogeneity using the I2 statistic and performed random effects meta-analysis.
Results: Studies were generally of high quality, although 4 used an active run-in period to titrate the dose and exclude patients with adverse effects or who were nonresponders. Thus, they were at high risk for bias. Desmopressin doses of at least 25 mcg or greater decreased nocturnal voids and increased time to first void. A dose of 100 mcg provided just more than an hour of additional sleep
before the first void compared with placebo as well as 0.72 fewer voids per night.
Higher doses provided no significant increase in benefit. Hyponatremia (RR 5.1) and headache (RR 4.3) were the most common adverse effects. Serious adverse effects were rare.
服務 Service 信賴 Trust 關懷 Mercy
Desmopressin appears to offer a modest benefit for treating
nocturia in generally healthy adults with adequate safety. The initial dose should be between 50 and 100 mcg. Higher doses should only be used with caution and a lower initial dose of 25 to 50 mcg is
appropriate in elderly patients. All patients should be monitored for hyponatremia. The drug should be used with caution in patients with chronic lung disease due to the rare occurrence of respiratory
failure. Additional well designed, adequately powered studies 1 or more years induration are needed.
Conclusion
服務 Service 信賴 Trust 關懷 Mercy