國立臺灣大學公共衛生學院流行病學與預防醫學研究所 博士論文
Institute of Epidemiology and Preventive Medicine College of Public Health
National Taiwan University Doctoral Dissertation
喀麥隆細菌學陽性肺結核患者的治療前失落調查 Pre-Treatment Loss to Follow-up of Bacteriologically
confirmed Pulmonary Tuberculosis Patients and Its Determinants in Two Regions of Cameroon
歐以利
Elias Fomunyam Onyoh 指導教授: 林先和 博士
Advisor: Hsien-Ho Lin, M.D, Sc.D.
中華民國 107 年 1 月 January 2018
i
ABBREVIATIONS
AFB: Acid Fast Bacilli
AIDS: Acquired Immunodeficiency Syndrome
CBCHBIRB: Cameroon Baptist Convention Health Board Institutional Review Board CBCHS: Cameroon Baptist Convention Health Services
CI: Confidence Intervals
DTU: Diagnostic and Treatment Units HIV: Human Immunodeficiency Virus HR: Hazards Ratio
IQR: Interquartile Range LTFU: Lost to Follow-Up
MDG: Millennium Development Goals MDR: Multi-Drug Resistant
NTCP: National Tuberculosis Control Program of Cameroon NTU: National Taiwan University
OR: Odds Ratio
PLTFU: Pre-treatment loss to follow-up SDG: Sustainable Development Goals
SPPTB: Smear-Positive Pulmonary Tuberculosis TB: Tuberculosis
WHO: World Health Organization
iii
ABSTRACT
Background: Infectious pulmonary tuberculosis (TB) patients are universally expected to initiate therapy promptly after diagnosis in order to quickly halt the transmission of TB within any community. In reality, not all these diagnosed cases finally initiate TB therapy; hence, they become what is known as pre-treatment loss to follow-up (PLTFU) patients. Current figures of PLTFU range between 4 and 38% with great geographic heterogeneity. We aimed to investigate the proportion and risk factors of PLTFU of TB patients and the reasons of PLTFU in two regions of Cameroon. We also evaluated the impact of patient counseling and phone reminder on PLTFU.
Methods: The three studies conducted include a retrospective (Jul-Dec 2015), prospective (Feb-Jul 2016) and an impact evaluation study, involving thirty-nine TB diagnostic and treatment units (DTUs). Pre-prepared data collection forms and semi- structured questionnaires were used to retrieve information from TB laboratory and treatment registers for all bacteriologically confirmed cases diagnosed during the study period. Data retrieved from both TB registers were cross-linked to identify any PLTFU cases (defined by failure to initiate treatment 7 days after diagnosis). Socio-
demographic, sputum examination results and treatment information were collected.
Travel distance/travel time between patient’s residence and DTU’s location were obtained using geographic information system tools. In the prospective study, all confirmed TB patients received counseling on the importance of treatment and the objectives for the study. Those who did not return for treatment on time were further contacted by phone or messages. Reasons for loss to follow-up were inquired and the patients were reminded to return for treatment. In the retrospective and prospective
studies, we conducted univariable and multivariable logistic regression analyses to determine the risk factors of PLTFU. We also conducted Cox proportional hazard regression to determine the determinants of time to treatment in these patients. To evaluate the intervention of patient counseling and phone reminder (which was
implemented in the prospective study), we combined the retrospective and prospective studies. Univariable and multivariable logistic regression analyses of the merged data were conducted to determine whether the intervention was associated with PLTFU, adjusting for other risk factors. We also performed a regression discontinuity analysis by adding a linear term of time trend and an interaction term between the intervention and the linear term of time trend to the logistic regression model.
Results: In the retrospective study, 1174 cases of bacteriologically confirmed TB were identified. The PLTFU proportion was 16.7% (95% CI: 14.6-18.8%) in these patients.
Median time from first positive TB result to therapy initiation was two days (IQR: 2–3).
In the multivariable logistic regression, significant risk factors for PLTFU included urban DTUs ([urban versus rural], adjusted odds ratio (aOR): 2.51, 95% CI: 1.51–4.17);
travel time from home to DTUs (>30 minutes versus ≤30.0 minutes, aOR: 2.19, 95%
CI: 1.56–3.09); and travel distance from home to DTU (>30 km versus ≤30.0 km, aOR:
2.31, 95% CI: 1.63–3.27). In the multivariable Cox regression, significant determinants of time to treatment included urban DTUs ([urban versus rural], adjusted hazards ratio (aHR): 0.72, 95% CI: 0.60–0.86); travel time from home to DTUs (>30 minutes versus
≤30.0 minutes, aHR: 0.80, 95% CI: 0.69–0.92); and travel distance from home to DTU (>30 km versus ≤30.0 km, aHR: 0.76, 95% CI: 0.66–0.89).
In the prospective study, 1060 cases of bacteriologically confirmed TB were identified, and 10.6% (95% CI: 8.7–12.4%) had PLTFU. Risk factors for PLTFU and determinants
v
of time to treatment in the prospective study were similar to those in the retrospective study. Major reasons for loss to follow-up included lack of transport money to get back to hospital (50%), DTU was too far away from home (29.3%), and 14.6% had travelled out of town.
In the impact evaluation study, patient counseling and phone reminder was associated with reduced odds of PLTFU both in the univariable (odds ratio [OR]: 0.56; 95% CI:
0.44–0.72) and multivariable (OR: 0.61; 95% CI: 0.47–0.79) analysis. In the regression discontinuity analysis using logistic regression, the association between the intervention and PLTFU was not statistically significant (aOR: 0.71, 95% CI 0.25–2.01), and the associations for the linear time trend (aOR: 0.999, 95% CI 0.996– 1.002) per day; and for the interaction between intervention and time (aOR: 1.0001, 95% CI 0.996–1.005) were not significant either.
Conclusion: Access to TB treatment following diagnosis was still a major problem in Cameroon. This may be hampered by risk factors related to the patients and the TB care providers. The presence of PLTFU introduced a significant barrier to TB control.
Measures such as adequate pre-and post-diagnosis counselling and phone call reminders may have a positive effect on reducing PLTFU, but their effectiveness needs to be assessed in subsequent studies.
TABLE OF CONTENTS
CERTIFICATION ... i
ABBREVIATIONS ... ii
ABSTRACT ...iii
TABLE OF CONTENTS ... 1
CHAPTER 1. BACKGROUND AND LITERATURE REVIEW ... 5
1.1 Global tuberculosis epidemiology and control ... 5
1.2 Pre-treatment loss to follow-up (PLTFU) ... 6
1.3 Literature review of pre-treatment loss to follow-up ... 6
1.3.1 Proportion of pre-treatment loss to follow-up ... 6
1.3.2 Determinants or risk factors for pre-treatment loss to follow-up ... 7
1.3.3 Patients’ reasons for pre-treatment loss to follow-up ... 8
1.3.4 Interventions directed towards ameliorating pre-treatment loss to follow-up ... 9
1.4 Tuberculosis prevention and care in Cameroon ... 9
1.5 Knowledge gaps. ... 11
CHAPTER 2. STUDY OBJECTIVES ... 12
2.1 Retrospective study objectives: ... 12
2.2 Prospective study objectives: ... 12
2.3 Impact evaluation of patient counselling and phone reminder study objectives: . 13 CHAPTER 3. METHODS ... 14
3.1 Overview ... 14
3.2 Study population ... 14
3.3 Data collection and management ... 15
3.4 Measurement of pre-treatment loss to follow-up ... 17
3.5 Measurement of the determinants of pre-treatment loss to follow-up ... 17
3.6 Statistical analysis ... 18
3.6.1 Retrospective study ... 18
3.6.2 Prospective study ... 19
2
3.6.3 Impact evaluation of patient counselling and phone reminder study ... 19
3.7 Sample size and power estimation ... 20
3.8 Ethical clearance ... 21
CHAPTER 4. RESULTS ... 22
4.1 Retrospective study ... 22
4.2 Prospective study ... 23
4.3 Impact evaluation of patient counselling and phone reminder study ... 24
CHAPTER 5. DISCUSSIONS ... 26
5.1 Retrospective study: ... 26
5.2 Prospective study: ... 29
5.3 Impact evaluation of patient counselling and phone reminder study: ... 30
5.4 Implications for tuberculosis control in Cameroon and worldwide ... 31
CHAPTER 6. CONCLUSION ... 32
REFERENCES ... 34
Figures ... 37
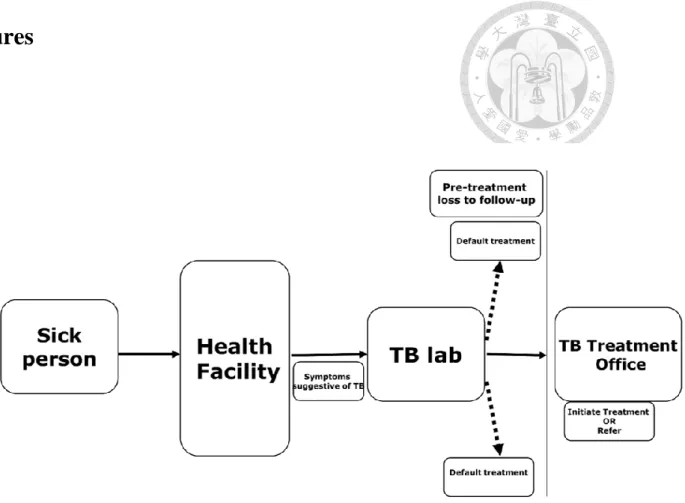
Figure 1. TB diagnostic and care pathway... 37
Figure 2. Location of Cameroon within Africa ... 38
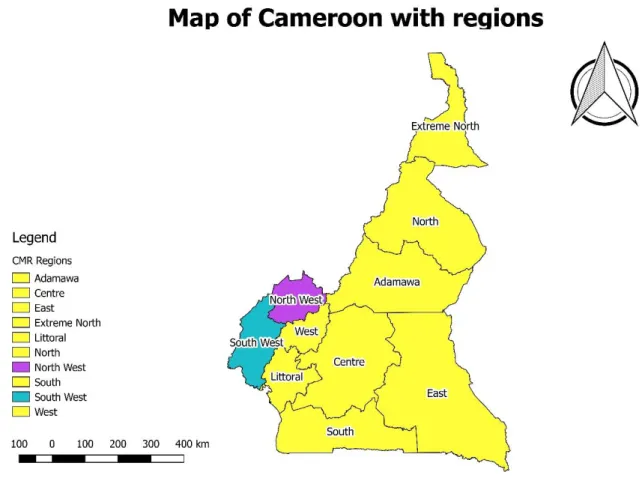
Figure 3. Regions of Cameroon ... 39
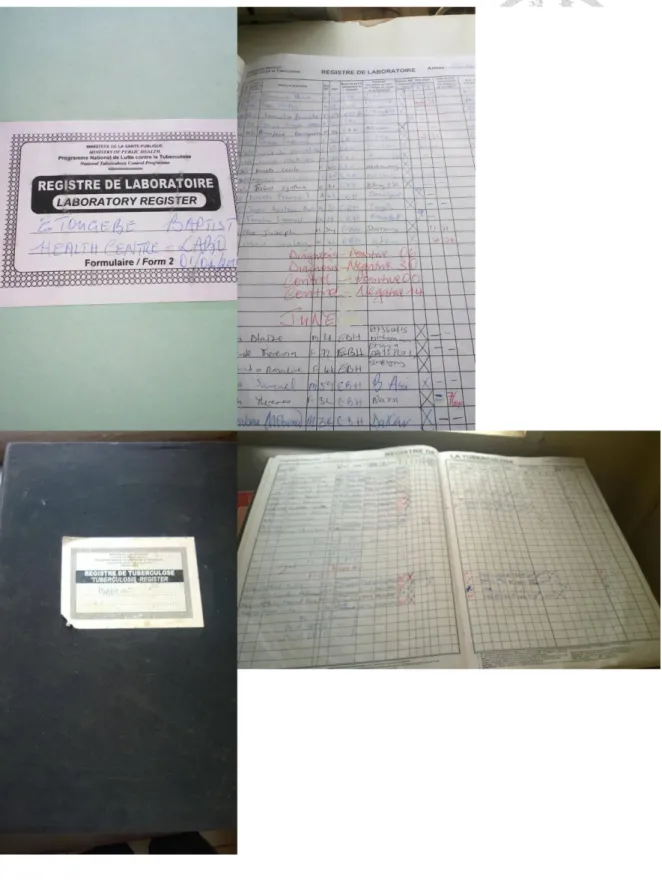
Figure 4. Cameroon TB laboratory and treatment registers ... 40
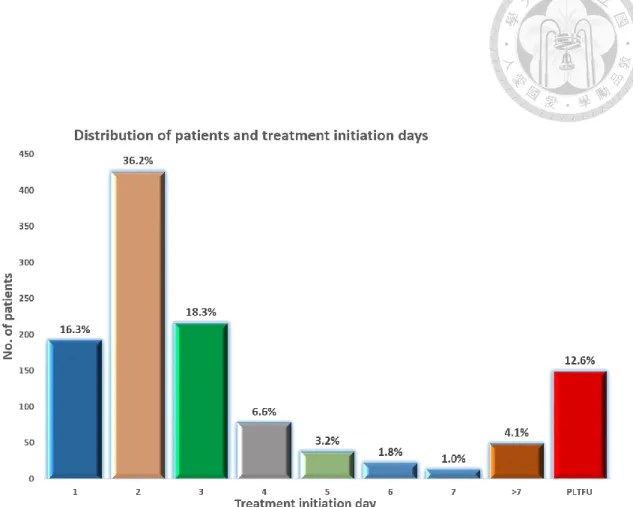
Figure 5. Distribution of treatment delay by days among all bacteriologically- confirmed pulmonary tuberculosis patients diagnosed in the North West and South West Regions of Cameroon. ... 41
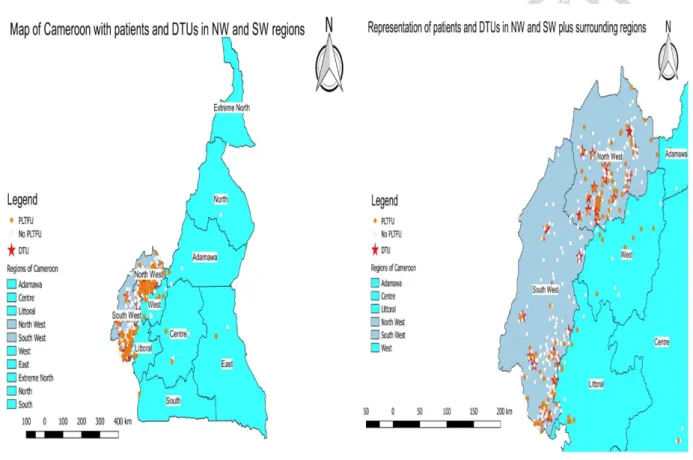
Figure 6. Geospatial distribution of tuberculosis diagnostic and treatment units (DTUs) and patients diagnosed within the North West (NW) and South West (SW) Regions of Cameroon. ... 42
Figure 7. Non-linear spline depicting the Odds Ratios of PLTFU and travel distance to DTU ... 43
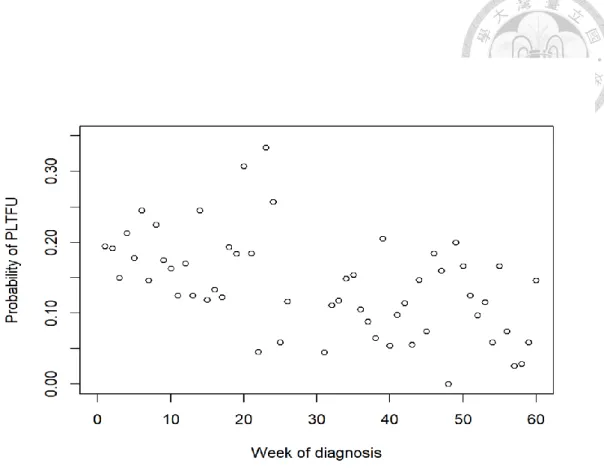
Figure 8. Scatterplot showing the probability of PLTFU over time during the study period. ... 44
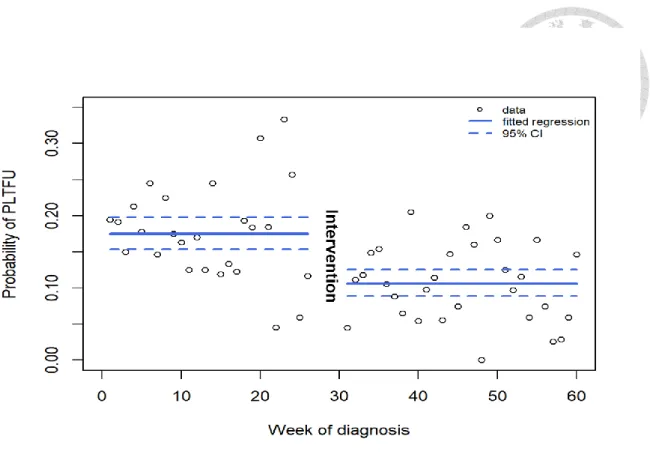
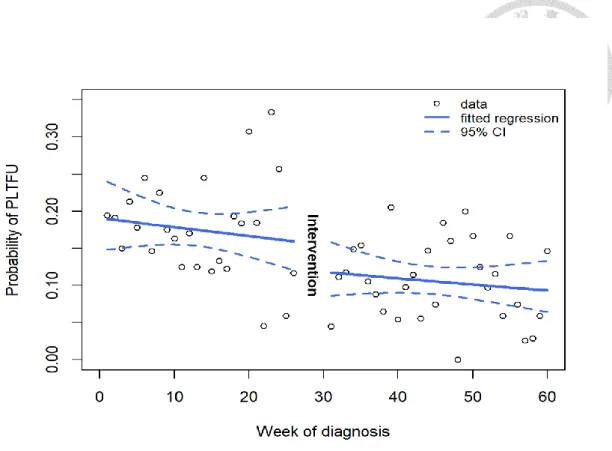
Figure 9. Probability of PLTFU over time during the study period and the predicted probability with 95% confidence bands from the univariable logistic regression model of the intervention and PLTFU. ... 45 Figure 10. Probability of PLTFU over time during the study period and the predicted probability with 95% confidence bands from the multivariable logistic regression
model including the intervention, the linear term of time trend, and the interaction
term of the intervention and time. ... 46
Tables ... 47
Table 1. TB incidence rate within Middle African region, 2012. ... 47
Table 2. General characteristics of retrospective study population ... 48
Table 3. Comparison of characteristics of patients with PLTFU to those who accessed antituberculosis treatment within 7 days of diagnosis in the retrospective study ... 49
Table 4. Factors associated with PLTFU in patients with bacteriologically-confirmed pulmonary tuberculosis: Univariable and Multivariate Logistic Regression Analyses in the retrospective study 7 days post-diagnosis (n=1112) ... 50
Table 5. Factors associated with PLTFU in patients with bacteriologically-confirmed pulmonary tuberculosis: Univariable and Multivariate Cox Proportional Hazards Regression Analyses in the retrospective study after 30 days follow-up (n=1112) ... 51
Table 6. General characteristics of the prospective study population (N=1060) ... 52
Table 7. Comparison of characteristics of patients with PLTFU to those who accessed anti-tuberculosis treatment within 7 days of diagnosis in the prospective study (N=1060) ... 54
Table 8. Factors associated with PLTFU in patients with bacteriologically confirmed pulmonary tuberculosis: Univariable and Multivariate Logistic Regression Analyses in the prospective study, 7 days post-diagnosis (n=1060) ... 56
Table 9. Factors associated with PLTFU in patients with bacteriologically confirmed pulmonary tuberculosis: ... 58
Univariable and Multivariate Cox Proportional Hazards Regression Analyses in the prospective study after 30 days follow-up (n=1060) ... 58
Table 10. Reasons for PLTFU from patients in the prospective study population ... 60
Table 11. General characteristics of the impact evaluation study population ... 61
Table 12. Univariable and Multivariate Logistic Regression Analyses of PLTFU for the impact evaluation study, 7 days post-diagnosis (n=2160) ... 62
Table 13. Univariable and Multivariate Cox Proportional Hazards Regression Analyses of PLTFU for the impact evaluation study after 30 days follow-up (n=2160) ... 63
APPENDICES ... 64
Publication ... 64
Letter of acceptance ... 82
ANNEXES ... 83
1. Participant’s information notice ... 84
2. Informed consent ... 86
4
3. Questionnaires ... 88 4. Ethical approval letters ... 93
CHAPTER 1. BACKGROUND AND LITERATURE REVIEW
1.1 Global tuberculosis epidemiology and control
Currently, tuberculosis (TB) is the ninth leading cause of death worldwide and the only single infectious agent, and second to the human immunodeficiency virus (HIV) to be known as the greatest killer disease with TB itself being equally the number one killer of those infected with HIV.1,2 In 2016, 6.3 million newly diagnosed TB cases were reported, an equivalent of about 61% of the estimated incidence of 10.4 million with a global success treatment rate of 83%, while treatment success rate for drug-resistant tuberculosis remains low at 54% globally.2 The incident TB cases for 2016 were highest in the WHO South-East Asia Region (45%) followed by the WHO African Region (25%).2 The human immunodeficiency virus (HIV) remains the most reported co-infection with tuberculosis for the year 2016, with an estimated incidence of 46% (476,774 TB-HIV cases) among TB cases and only 85% of these number were started on antiretroviral therapy (ART). In 2016, only 57% of notified TB patients had a documented HIV test result with 82% of TB patients had a documented HIV result in the WHO African Region.2 The WHO’s End TB strategy and the United Nations’ Sustainable Development Goals (SDGs) share a collective aim to end the global TB burden for the period of 2016–2035.
The WHO’s End TB strategy sets specific targets including a 90% reduction in TB deaths and 80% reduction in TB incidence by 2030 comparing with 2015; while no patients and their households should suffer catastrophic costs as a result of TB disease.2 Globally, the TB death rate is dropping at a 3% fall per year, with more deaths in men than women; and gaps in case detection and reporting are higher in men.2,3 Most of these deaths could be prevented with early diagnosis and appropriate treatment.2,4 Previous targets set before 2015 were at 85%
treatment success rate and 70% case detection rate,5 however, currently the recommended
6
target level for 2025 (post-2015) are at a treatment success rate of ≥90% and a case detection rate of ≥90%.2,6
1.2 Pre-treatment loss to follow-up (PLTFU)
Measures to improve TB control have mainly centered on rapid detection and treatment of all patients with smear-positive pulmonary TB.7 The TB care-seeking behavior is usually complex.8 The pathway from presumptive TB patient’s symptoms through diagnosis to treatment is a bit long as shown in Figure 1. Focusing only on diagnoses and treatment will miss certain components, e.g. pre-diagnosis care and linkage between diagnosis and treatment.
Pre-treatment loss to follow-up, previously known as initial default, refers to the situation where newly diagnosed TB patients do not receive anti-TB treatment after diagnosis.9 Following the WHO, the National TB Programs (NTPs) usually evaluate TB treatment outcomes as indicators which are usually reported as: treatment loss to follow-up, cured, treatment failure, completed treatment, died or relapse. However, patients who are lost to follow-up for TB treatment may also be categorized into two groups: a) delay or loss to follow- up after diagnosis with sputum-smear positive results (PLTFU) and b) loss to follow-up (LTFU) during treatment. Currently most of the NTPs only measure and report routinely the treatment loss to follow-up but not PLTFU.7,10
Usually without treatment of these patients who are lost to follow-up, there will be a sustained TB transmission within the community and while some may later develop drug resistant TB, some may even die.11
1.3 Literature review of pre-treatment loss to follow-up 1.3.1 Proportion of pre-treatment loss to follow-up
Different studies and settings have used different definitions to measure PLTFU among TB patients. With the current definition of PLTFU of TB patients, there is still no
formal or any standardized duration limit (a cut-off point) for not initiating TB treatment after diagnosis to be considered as PLTFU.
The proportion or magnitude of PLTFU among TB patients globally ranges between 4 and 38%.7 Studies from sub-Saharan Africa showed a higher proportion of PLTFU (6 to 38%) while those from Asia revealed a little lower magnitude (4 to 28%).7,10 In a study conducted in Nigeria, any newly diagnosed sputum smear-positive pulmonary TB patient who did not start TB treatment two days post-diagnosis was considered as PLTFU.12 The few studies already conducted around the world on PLTFU showed startling results. For example, within Africa, in Nigeria, PLTFU was at 16.9%, Ghana (38%)13 and in South Africa it was at 22.8%.14,15 Within Asia, the PLTFU rate recorded in Vietnam was 8.3%;16 in India it was 50%;9 in Pakistan it was as low as 5.2% with more males delaying to initiate treatment than women.17 In another study from Pakistan, the proportion of PLTFU was as high as 21.2%.18 In Fiji, the proportion of PLTFU was as high as 33% in the Western Division of the country following a 10-year audit of the national data.10 However, the definition of PLTFU duration and study population were not the same in all these studies, with some as short as 2 days after the first AFB positive sputum result and others up to 30 days; and with some studies including everyone diagnosed with TB while some included only diagnosed adults.7,10,12,14-16
1.3.2 Determinants or risk factors for pre-treatment loss to follow-up Pre-treatment loss to follow-up is usually related to either factors associated with the patient or with the healthcare provider including the NTPs itself.7 Presently in most countries where TB is a great burden certain identified risk factors such as poverty, gender, alcoholism, distance from DTU, lack of TB knowledge, etc. have been
associated with PLTFU thereby hampering tuberculosis control endeavours.16,19-22 For
8
example, being male was found to be a risk factor for PLTFU in Pakistan.18 In Vietnam, DTUs located in urban areas were more associated with PLTFU than those in rural settings.16 In China, Xu and colleagues found that risk factors for PLTFU in Hunan Province included: age greater than 60 years, residing in a rural setting, and being unemployed.23 Having a lower income, unemployment, non-skilled professions, aged population and living in rural areas were found to be associated with PLTFU.16,24-27 Importantly, distance or lack of geographic access from patient’s residence to treatment facility in addition to the involved financial burden (catastrophic costs), have been found to be associated with the delay of TB diagnosis and treatment.2,28
1.3.3 Patients’ reasons for pre-treatment loss to follow-up
A few studies have attempted to trace and identify the patients who had not initially initiated treatment in order to understand the reasons of PLTFU.25,27,29-31 Following the tedious patient’s pathway from diagnosis to treatment, some reasons for PLTFU have been suggested by Gopu et al in South India, including unwillingness to initiate
treatment, symptoms being mild, personal reasons and dissatisfaction.32 Still in India, it was also seen that, private practitioners were preferable (64.4%), limited trust in public health facilities (26.7%) and working hours of the Directly Observed Treatment (DOT) DTUs (18.5%). In Vietnam, patient’s negative perceptions of the working and treatment procedures of the NTP were the likely reasons for PLTFU, including the unsuitable opening hours of the DTUs, complicated administrative procedure and the limited trust of TB treatability by the DTU.16 In Hunan Province of China, reasons for non-
enrollment to treatment of tuberculosis included financial difficulties, out-migration for work and concerns about work and studies.23
1.3.4 Interventions directed towards ameliorating pre-treatment loss to follow-up
Globally, early diagnosis and treatment alone may not be adequate in the control of tuberculosis, therefore in order to achieve universal access to TB care services, there is need to identify certain interventions that could mitigate the high levels of PLTFU in many countries. In India, Sharma et al proposed an intervention model to reduce PLTFU by involving Resident Welfare Associations (RWAs) to work with private health practitioners. These local civil society organizations have a greater advantage of a two-way influence on community establishments as well as public institutions.
Therefore, their knowledge and understanding of local situations and adaptability plus flexibility toward the local community’s realities may be appropriate.11 The local leaders (called ‘Pradhans’) of these communities may be contact persons for all TB patients within their localities, thereby reducing the spread of TB and other diseases within the community.11 Currently however, no studies have actually been conducted to evaluate any interventions to reduce the proportion of PLTFU.
1.4 Tuberculosis prevention and care in Cameroon
Cameroon is a multi-ethnic nation located in west-central Africa with a population of 24,994,885 inhabitants spread over 10 geopolitical regions. It has boundaries with Nigeria, Chad, Central African Republic, Congo, Gabon and Equatorial Guinea (Figures 2 and 3). It has a GDP per capita of US$3300 with a total government expenditure on health at 4.1% of total GDP.33
Cameroon is among the first 41 nations in the world with very high level of TB and one of the highest within its region; with an incidence rate of 238 per 100,000 population as at 2013 (Table 1). It has 178 health districts with over 3000 health facilities and in order to curb the spread of TB in the country, the government increased the number of DTUs from 222 in 2011
10
to 238 across the nation in 2013 with various regions having accordingly: Adamawa (9), Centre (48), East (20), Far North (28), Littoral (39), North (17), North West (21), West (20), South (17), South West (19), with an average of 1 DTU per 90,000 inhabitants.34 In Cameroon, the tuberculosis case detection rate is still low (48%) and treatment after lost to follow-up increasing with a current rate of 25% as at 2012 (Table 1). In 2012, a total of 63% of tuberculosis cases were sputum-smear positive and about 40% of TB patients were co-infected with HIV. The targets of the Cameroon National Tuberculosis Control Programme (NTCP) in 2009 were to diagnose at least 70% of smear-positive pulmonary tuberculosis (SPPTB) cases and to cure not less than 85% detected cases.34,35 Therefore, prompt diagnosis and early treatment was considered the most important strategy in order to effectively prevent and control the spread of TB in the country. On the other hand, the incidence of PLTFU and associated risk factors among TB patients have not been studied in Cameroon. The issue of PLTFU among TB patients is very crucial especially in realizing the targets of the NTCP.34 The process of TB diagnosis and treatment in Cameroon is described as shown in the following diagram (Figure 1). Within healthcare facilities in Cameroon, persons with suspected TB are usually subjected to a battery of diagnostic investigations including sputum microscopy for acid-fast bacilli (AFB x 2), chest X-ray, tuberculin skin test (TST), LED fluorescence microscopy, HIV serology, etc. Routinely, patients suspected of having TB disease are asked to submit two sputum specimens (one on spot and the other the following morning) or same day, for acid-fast bacilli (AFB) identification. Light microscopy by Ziehl-Neelsen technique is the method commonly used for AFB identification and quantification in the laboratories, though some diagnostic centres also make use of LED fluorescence microscopy and GeneXpert. In addition, if any of these sputum specimens is positive for AFB by microscopy, culture, or GeneXpert, then such a patient will be classified as SPPTB case. In Cameroon, each DTU has a TB laboratory register (usually located at the laboratory) for all patients who
undergo sputum examination and another register at the treatment facility for all those who get on TB treatment, i.e. TB treatment register (Figure 4).
In Cameroon, all confirmed SPPTB patients are expected to undergo tuberculosis treatment immediately based on the National Tuberculosis Control Programme (NTCP) guidelines either by hospitalization or treated otherwise, following the directly observed therapy short course (DOTS) strategy. This therapy is a combination of Rifampicin [R], Isoniazid [H], Ethambutol [E] and Pyrazinamide [Z]) for at least 6 months (2 months intensive and 4 months continuation phases. Generally, majority of confirmed cases would get on treatment as soon as possible;
however unfortunately, an unknown proportion of these newly diagnosed SPPTB cases would dodge treatment for reasons not well understood, while they continuously infect close contacts within their vicinity and community.
1.5 Knowledge gaps.
In view of the aforementioned points, we found out that no study has been conducted in Cameroon to investigate the phenomenon and reasons of PLTFU of TB patients.
Globally, not many studies have been conducted to identify the reasons for pre- treatment loss among smear-positive tuberculosis patients. Moreover, no study has evaluated the impact of any intervention in the field on the reduction of PLTFU. It is therefore imperative to address the issue of PLTFU in order to curb the transmission of tuberculosis within communities.7
12
CHAPTER 2. STUDY OBJECTIVES
Therefore, this study would investigate the situation of pre-treatment loss to follow-up of persons with active tuberculosis within the Central African region using Cameroon as a case study. At the moment in Cameroon, the NTP does not recommend the searching and putting on treatment of all those that are lost after diagnosis, and does not also recommend TB treatment counselling of these patients before their test results are out from the laboratory. This is one of the main reasons why we went ahead with this study to determine the magnitude of this phenomenon in the first place, and the NTP will be advised to find solutions to this. This is the more reason why we equally characterized this group of patients for the Programme and healthcare providers so that they could target particularly those suspects who present with such characteristics. We hypothesized that the magnitude and risk factors for PLTFU may be different from that in other places. Therefore, in this study, the proportion of PLTFU, reasons for not initiating treatment and their risk factors were studied. This is the first study in Cameroon to look into the incidence of PLTFU of TB patients in Cameroon, thereby highlighting the problem of PLTFU versus programme performance. We aimed to conduct three studies with the following objectives:
2.1 Retrospective study objectives:
The study objectives included determining the incidence of PLTFU of patients with bacteriologically-confirmed pulmonary tuberculosis; and identifying risk factors associated with PLTFU of confirmed TB patients in the North West and South West regions of Cameroon, using routine TB program data.
2.2 Prospective study objectives:
Through prospectively counselling and tracing the newly diagnosed TB patients (i.e.
patients who were being diagnosed with TB for the first time), this study sought to
determine the incidence and risk factors of PLTFU of patients with bacteriologically- confirmed pulmonary tuberculosis; and importantly to identify reasons (from the
patient’s perspective) associated with PLTFU of bacteriologically-confirmed pulmonary tuberculosis TB patients in the North West and South West Regions of Cameroon.
2.3 Impact evaluation of patient counselling and phone reminder study objectives:
The counselling of patients and phone reminder in the prospective cohort study and the availability of the data from the retrospective study provide an opportunity to assess the impact of interventions implemented in the prospective study on PLTFU. We aimed to evaluate the impact of counselling of patients and phone reminder on the incidence of PLTFU using a before-and-after study design.
14
CHAPTER 3. METHODS
3.1 Overview
This study was conducted in two regions of Cameroon, the North West (NW) and South West (SW) Regions located in the southwestern part of the country (Figure 3). The study included 39 out of the total 40 TB diagnostic and treatment units (DTU) also known as TB basic management units. These sites are located in the majority English speaking area of Cameroon, with about 3.5 million inhabitants and at least 2000 TB cases detected annually from both regions. These DTUs are located in both rural and urban settings within the regions and are within public and private health facilities. This methods’ section will include three different study designs in view of the three studies: First, the retrospective study was used to understand the magnitude and determinants of PLTFU using routine program data under the business-as- usual setting. Second, the prospective study was designed to further understand the determinants of PLTFU by prospectively collecting information on sociodemographic factors (which were not available in routine data). It was also designed to identify the reasons of PLTFU through active tracing and calling the PLTFU patients in order to collect information on reasons for not initiating treatment. Lastly, the impact evaluation study is a post hoc analysis after the completion of the retrospective and prospective studies. We evaluated whether the patient counseling and phone reminder delivered in the prospective study would have an impact on PLTFU using a before-and-after study design.
3.2 Study population
The study included all consecutive bacteriologically-confirmed pulmonary tuberculosis patients diagnosed between July 1, 2015 and August 31, 2016 in 39 out of the total 40 DTUs of the NW and SW Regions during the study period with a total of 2160 bacteriologically- confirmed pulmonary tuberculosis cases. The mode of diagnosis of patients was mainly by
microscopy and GeneXpert. The month of January 2016 was however not included for data collection due to the investigators’ discretion. The retrospective study was conducted between July 1, 2015 and December 31, 2015 and 1174 cases were recorded. In the retrospective study, all diagnosed cases of all ages were included. While, the prospective study recorded 1060 cases and only those of age 21 and above were included. The prospective study was conducted between February 1, 2016 and August 31, 2016. The only exclusion criterion here was any patient that was transferred in from another DTU. The quasi-experimental study population included a total population of 2160 cases from the merging of the previous two study samples.
The patients were followed up for up to 30 days.
3.3 Data collection and management
A pre-prepared data collection form was used to collect information directly from the TB laboratory register to be cross-linked with the TB treatment register at each health facility by the primary investigator and trained data collection officers. All data collected were double- entered into a Microsoft Access database (Microsoft Corp, Redmond, WA, USA) to ensure data integrity. This information was securely saved in compliance with the rules and regulations of the Internal Review Board requirements and ethical protections. All the data collected were appropriately checked for accuracy and completeness, verified by data collectors and investigators for errors and missing information. All data collected for these three studies were processed and analyzed using Stata Statistical Software: Release 13.1 (College Station, TX: StataCorp LP.).
For the retrospective study, the data extracted from the registers included the patient’s socio- demographic information such as age, sex, residential address, sputum examination results and treatment status. Equally collected were the region of DTU’s location (NW versus SW), type
16
of health facility (public versus private), location of the DTU (rural or urban) and method of diagnosis.
For the prospective study, in addition to what were collected in the retrospective study, we used the pre-prepared data collection form to obtain information on socio-demographic and socioeconomic indices; and a semi-structured questionnaire to obtain their reasons for not initiating treatment. Before participating in the study, the patients were counselled about tuberculosis and the reasons for us conducting this study. Patients were told of the importance of completing the TB investigation and the need to start treatment immediately after diagnosis as is required by the NTCP. They were also informed that they would be called if not yet started treatment by the 8th day to remind them to come and initiate TB therapy. Finally, an informed consent was given by the index patient or a care-giver to participate in the study. The socio-demographic and socioeconomic indices obtain were educational level, marital status, employment status, financial status and other health-related conditions. The reasons (i.e. the patient’s perspective only) for not initiating treatment earlier than expected was collected only from those who had not started treatment using an interviewer-administered semi structured questionnaire through phone calls or messages through other patients or community health workers. At most, three call attempts were made to reach patients after 7 days post-diagnosis (on days 8th, 9th and 11th) if he or she had not initiated treatment. Once the patient was reached, reasons for not initiating treatment were collected and the study on that particular case ended at that point with no further calls or search; however, all patients were followed-up passively for 30 days (a month). Additionally, these forms of communication also served as a means of reminding patients to get back to care.
The quasi-experimental study population included a total of 2160 bacteriologically- confirmed pulmonary tuberculosis cases from the retrospective and prospective study groups by merging the two databases.
3.4 Measurement of pre-treatment loss to follow-up
A PLTFU case was defined as any bacteriologically-confirmed pulmonary TB patient that was recorded in the laboratory register, but was not placed on TB treatment at that particular facility within 7 days. The 7-day cut off, though arbitrary, was decided after reviewing the various studies already conducted on PLTFU across the world especially in Africa with consideration of the field knowledge of the most common treatment initiation day in these two regions of Cameroon.
In addition to PLTFU, we also measured the treatment delay by calculating the time taken for a patient from the date of first positive acid-fast bacilli or GeneXpert result to the date of starting tuberculosis therapy (i.e. time to treatment). The time to treatment information would not be affected by the current cut off definition of PLTFU.
3.5 Measurement of the determinants of pre-treatment loss to follow- up
Information on potential determinants of PLTFU was obtained from the structured questionnaire designed for this study, see Section 3.3 for details. One key determinant of PLTFU in this study was the geographical access to DTUs, which was evaluated using travel distance and travel time between patient’s residence and DTU’s location by means of both global positioning and geographic information systems tools. We
obtained the geocodes of the DTUs using a global positioning system tool (GPS coordinates). The geocodes of the patients’ residences were obtained by matching the patients’ addresses through online maps (MapQuest, OpenStreetMap, Google Maps, HERE WeGo) and other relevant websites such as http://latitude.to/,
http://nona.net/features/, www.worldplaces.net and www.geographic.org. Travel distance and travel time calculations were estimated using an application programming
18
interface (API) code that was freely donated by HERE map developer to be used in Stata data analysis software.
3.6 Statistical analysis
3.6.1 Retrospective study
Descriptive analyses of study participants were done by tabulating the frequency distribution.
The proportion of PLTFU among all participants was calculated for PLTFU.
Maps showing the locations of patients (i.e. those who initiated treatment and those who had not) and that of the DTUs were produced using Quantum Geographic Information System (QGIS 2.18) software, Las Palmas, Spain.36
Univariable and multivariable logistic regression analyses were conducted to analyze whether geographical access and other possible determinants were associated with PLTFU, with the estimation of the crude and adjusted odds ratios (ORs) and their 95% confidence intervals (95% CI).
Our analyses of PLTFU did not consider the variation in treatment delay among those who were eventually treated. We therefore conducted a separate time-to-event analysis to investigate the determinants of treatment delay using univariable and multivariable Cox proportional hazards model. In the Cox regression model, survival data was constructed and
‘initiated treatment’ was set as ‘failure = 1’ while ‘not initiated treatment’ as ‘censored =0’.
In addition to geographical access, we considered other determinants of PLTFU in the multivariable analyses, including age, sex, location of DTU, region of DTU, health facility type and method of diagnosis.
We also used restricted cubic spline regressions with 3 knots to model the dose-response relationship between travel distance and the probability of PLTFU using its odds ratios on
the Stata statistical software. Three knots were used because PLTFU did not change quickly over travel distance, though we also applied four and five knots in the sensitivity analyses.37
3.6.2 Prospective study
For the prospective study, descriptive analyses of study participants’ characteristics in this prospective study were done by tabulating the frequency distribution; and the proportions of PLTFU for the characteristics of the participants were calculated.
Geographical access and other possible determinants of PLTFU were also analyzed by conducting both univariable and multivariable logistic regression analyses as was done in the retrospective study. In addition to geographical access, age, sex, location of DTU, region of DTU, health facility type (public versus private) and method of diagnosis (smear microscopy versus GeneXpert); we further considered other information collected in the prospective study, including marital status, level of educational, employment status, monthly salary, transportation cost from patient’s home to health facility, time taken to travel from home to DTU, any history of doing a TB test, awareness of TB result after TB test, awareness of HIV status, duration of last HIV test done and presence of co-morbidity. A separate time-to-event analysis was conducted to investigate the determinants of treatment delay using univariable and multivariable Cox proportional hazards model.
3.6.3 Impact evaluation of patient counselling and phone reminder study
A post hoc quasi-experimental (before-and-after) analysis was conducted to evaluate the impact of patient counselling and phone reminder (an intervention delivered in the
prospective study) on the reduction of PLTFU. The period of the retrospective study, (July 2015–December 2015) was used as the baseline reference group, and the period of the prospective study, (February 2016-August 2016) was then used as the intervention group.
We conducted univariable and multivariable logistic regression analyses to estimate the
20
crude and adjusted odds ratios (ORs) and their 95% confidence intervals (95% CI) between the intervention and PLTFU. We adjusted for other potential determinants of PLTFU in the multivariable analysis, including age, sex, location of DTU, region of DTU, health facility type, geographical access, and method of diagnosis. A similar Cox regression analysis was conducted to estimate the association between the intervention and time to treatment initiation.
In addition, a regression discontinuity analysis was conducted to account for any linear underlying time trend of PLTFU during the study period. This was done by first visually plotting the proportion of PLTFU during the whole study period, including the baseline period and the intervention period. We then fitted two logistic regression models to estimate the effect of intervention.
The first model included only the intervention effect (Int) and assumed no underlying time trend:
Model 1: Logit (p) = α + 𝛽1∗ 𝐼𝑛𝑡
The second model accounted for a linear time trend of PLTFU and allowed the trend to be different before and after the intervention. This was done by including the intervention effect (Int), a linear time trend (Time), and an interaction term between the intervention and time.
Model 2: Logit (p) = α + 𝛽1∗ 𝐼𝑛𝑡 + 𝛽2∗ 𝑇𝑖𝑚𝑒 + 𝛽3∗ 𝐼𝑛𝑡 ∗ 𝑇𝑖𝑚𝑒
3.7 Sample size and power estimation
In estimating the sample size of this cohort study with a dichotomous outcome from a single sample, we took into consideration the following assumptions:
1. From each of these two regions, about 1100 cases of bacteriologically-confirmed pulmonary tuberculosis cases will be diagnosed each year based on historical data;
consequently 550 diagnosed cases would be expected within 6 months of data collection with at least 90 cases per month.
2. An estimated proportion of PLTFU among positive cases was 12% from each region, and was estimated from previous studies and field experience. Therefore, 460 cases from each region (a total of 960) at least 1000 diagnosed cases of tuberculosis from both regions will be required to give this study a power of 95% confidence interval of between 9.4 and 15.0%, two-sided significance level (α) = 0.05.
3.8 Ethical clearance
Ethical clearance was obtained from the Cameroon Baptist Convention Health Services Institutional Review Board (CBCHSIRB), the Cameroon National Ethical Committee of Research for Human Health (CNECRHH) and the National Taiwan University Hospital Research Ethics Committee (NTUHREC). Administrative approvals were sought from the Cameroon Ministry of Public Health through the National Tuberculosis Control Programme (NTCP), the Regional Delegation of Public Health and hospital authorities. The interviewee signed an informed consent before participating in the study.
22
CHAPTER 4. RESULTS
4.1 Retrospective study
Table 2 shows a total of 1174 cases with more males (56.2%) than females. About 82%
of patients attended care at urban DTUs and 41% of total patients were tested by GeneXpert. More than 30% of patients traveled for more than 30 minutes and over 30 km to get to the DTUs. The study population mean age was 37.6 years (SD ±13.2) with a PLTFU proportion of 16.7%, Table 3. After excluding those who were known to have been referred to other centers, the proportion of PLTFU dropped from 16.7% to 10.0%.
Figure 5 shows most of the patients (36.2%) initiated TB treatment on the second day following diagnosis.
In multivariable logistic regression, DTUs located in urban setting had a nearly 3-fold increase in odds of PLTFU compared to DTUs in the rural setting, aOR: 2.51, 95% CI:
1.51–4.17. A travel time of more than 30 minutes from home to DTU versus ≤30.0 minutes showed an increase in the odds of PLTFU, aOR: 2.19, 95% CI: 1.56–3.09; and travel distance from home to DTU (>30 km versus ≤30.0 km, aOR: 2.31, 95% CI: 1.63–
3.27). (Table 4). In the non-linear spline regression analysis, there is a steep increase in the odds for not initiating treatment immediately after diagnosis as patient’s distance away from DTU increases (Figure 7).
In the multivariable Cox regression analysis, the DTUs in urban setting had a 28%
decrease in initiating treatment compared with those in the rural setting, aHR: 0.72, 95%
CI: 0.60–0.86. However, private health facilities had a 7% increase in initiating treatment compared to public facilities, aHR: 1.07, 95% CI: 0.93–1.24. In the multivariable Cox regression, significant determinants of time to treatment included location of DTUs ([urban versus rural], adjusted hazards ratio (aHR): 0.72, 95% CI:
0.60–0.86); travel time from home to DTUs (>30 minutes versus ≤30.0 minutes, aHR:
0.80, 95% CI: 0.69–0.92); and travel distance from home to DTU (>30 km versus ≤30.0 km, aHR: 0.76, 95% CI: 0.66–0.89). (Table 5).
4.2 Prospective study
A total of 1060 bacteriologically-confirmed pulmonary tuberculosis cases were recorded with a mean age (M = 39.3, SD ±11.9) years. About 60% of patients were males. More than 70% of patients utilized services at DTUs located at urban settings. A slightly equal proportion of patients visited both health care facilities, public (51%) and private (49%). About 60% of patients were diagnosed by smear microscopy and sixty percent of total patients were married. About 10% of total patients never had any form of formal education. The proportion of those employed in this study was 82.2% with just 23.6% making more than 60,000 CFA frs (USD120) as monthly income.
Approximately 20% of total patients spent more than 6 hours to-and-from the DTU for care. Majority of the patients (71.1%) had recently done their HIV test within the last one year. HIV infection was a major co-morbid condition among these patients, with a 78.1% proportion among those with co-morbidities. See Table 6.
There was a PLTFU rate of 10.6% (112 out of 1060 cases); 95% CI: 8.7–12.4). In the multivariable logistic regression, the South West Region had a 90% increase in odds of PLTFU compared to the North West Region (aOR: 1.90, 1.27–2.85). Patients with a monthly salary of ≥60,000 CFA frs had a significantly lower odds of PLTFU compared with those of a lower salary, aOR: 0.54, 95% CI: 0.32–0.92. Those who tested for HIV
≥1y ago had an increased risk for not initiating treatment compared with those who did their test less than a year, aOR: 2.05, 95% CI: 1.36–3.09. See Tables 7 and 8.
The median time from first positive result to initiating therapy was 2 (IQR: 1–3) days.
In the Cox regression analysis on time-to-treatment, starting treatment was significantly
24
lower (15%) in the South West region than in the North West, aHR: 0.85, 95% CI:
0.74–0.97. The private health facility initiated treatment 50% quicker than in the public facility aHR: 1.50, 95% CI: 1.32–1.71, See Table 9. Among those who did not return for treatment by day 7, 50% claimed in the phone interview that they never had money to return to hospital to initiate treatment among other reasons for PLTFU, with 12.2% of PLTFU had no willingness of returning for care. See Table 10.
4.3 Impact evaluation of patient counselling and phone reminder study The analyses of impact evaluation included 2160 bacteriologically confirmed pulmonary tuberculosis cases with a mean age of 39.2 years (SD ±12.0). A total of 57.8% (1249 out of 2160) were males. The proportion of those diagnosed by GeneXpert (37.9%) was lower compared to those diagnosed by microscopy. See Table 11.
The proportion of PLTFU during the total study period (Jul 2015 to August 2016, except for the break in Jan 2016) was 14.1%; 95% CI: 12.6–15.4. The baseline or control group had a PLTFU of 17.5% while the intervention group’s PLTFU was 10.6%. Just to note that the baseline PLTFU of 17.5% is different from the previous one of the original retrospective study (16.7%) because certain patients were excluded due to the age cut-off of ≥21 years as inclusion criterion for the impact evaluation study. In the logistic regression analysis, there was a statistically significant decrease in PLTFU in the intervention group both in the univariable analysis (crude OR: 0.56, 95% CI:
0.44–0.72) and the multivariable analysis (aOR: 0.61, 95% CI: 0.47–0.79) (Tables 12).
There was also a 79% increase in odds of PLTFU among those diagnosed by GeneXpert compared with those diagnosed by microscopy, (aOR: 1.79, 95% CI: 1.22–2.63). Also statistically significant were travel time and travel distance. A travel time of more than 30 minutes from home to DTU versus ≤30.0 minutes showed an increase in the odds of
PLTFU, aOR: 1.81, 95% CI: 1.38–2.38. And travel distance of more than 30 km from home to DTU versus ≤30 km showed an increase in the odds of PLTFU, aOR: 1.81, 95% CI: 1.37–2.38.
Table 13 shows an approximately 30% significant increase in initiating treatment of the intervention group compared with the control, both in the univariable (crude HR: 1.31, 95% 1.20–1.44) and multivariable (aHR: 1.30, 95% CI: 1.18–1.42) Cox regression analyses. The South West Region had a lower rate of initiating treatment than the North West Region (aHR: 0.85, 95% CI: 0.75–0.95). Getting on treatment was quicker in the private health facilities compared to the public (aHR: 1.31, 95% CI: 1.18–1.45).
Initiating treatment was faster with those who traveled less than 30 minutes to the DTU compared to those who travelled more than that, (aHR: 0.86, 95% CI: 0.78–0.95), see Table 13.
The proportion of PLTFU during the whole study period decreased over time (Figure 8). The proportion appeared lower in the intervention period compared to the historical control period (Figure 9), consistent with a significant association between the
intervention and PLTFU (Model 1, crude OR: 0.56, 95% CI: 0.44–0.72). In the logistic regression model with the addition of a linear term of time trend and an interaction term between the intervention and time (Model 2), none of the associations were statistically significant: the adjusted odds ratio of the intervention was 0.71 (95% CI: 0.25–2.01);
the adjusted odds ratio of the linear time trend was 0.999 (95% CI: 0.996–1.002), and the adjusted odds ratio of the interaction between the intervention and time trend was 1.0001; 95% CI: 0.996–1.005. See Figure 10.
26
CHAPTER 5. DISCUSSIONS
5.1 Retrospective study:
This study brings out the fact that PLTFU of bacteriologically-confirmed pulmonary TB patients in Cameroon is still a crucial issue that requires urgent measures. The high PLTFU rate implied that these infectious TB patients could still transmit the disease in the community even after diagnosis. The analyses also revealed that many patients had to travel long distances to be diagnosed at a health facility, and poor geographical access to the facility was a significant risk factor for PLTFU.
From this study, 16.7% of bacteriologically-confirmed pulmonary TB patients did not initiate TB treatment within 7 days at the DTUs of diagnosis. In a previous systematic review, the proportion of PLTFU in some African countries ranged from 6% to 38%.
However, the estimates from different studies could not be directly comparable with that from this study since different methods were used to define and measure PLTFU.
The temporal definition of PLTFU ranged from two days to three months in prior studies 7. For example, patients might be classified as having PLTFU in other studies if they did not receive treatment within two days of diagnosis. The temporal definition of PLTFU in the present study was 7 days and the follow-up duration was at least 60 days.
When the two-days’ criterion used by Uchenna and colleagues in Nigeria was applied, the proportion of PLTFU increased from 16.7% to 47.5%.
After excluding those who were known to have been referred to other centers, the proportion of PLTFU dropped from 16.7% to 10.0%. Noteworthy is that the 10.0%
figure might be an underestimate since we do not know whether those referred to start treatment elsewhere eventually received treatment. Fewer studies attempted to trace the true outcome of those who were initially lost to follow-up. In several Asia studies, a
common reason for PLTFU was receiving treatment at a private clinic. However, true outcome and reason for PLTFU remained largely under-studied in Africa.
A key and unique finding from this study was that longer travel distance from patient’s home to DTU was associated with PLTFU. Compared to the patients who traveled 30 km or less to the DTU where they were diagnosed, those who travelled over 30 km to the DTU had a 2.4-fold increased odds of PLTFU. A similar pattern was also observed for travel time and PLTFU. A possible reason for this finding could be that, living far away from the DTU caused some patients to give up on receiving treatment. Another possibility is that living far away caused some of the patients to be referred to the DTU nearer their homes. Few studies have equally examined geographical access as a potential reason for PLTFU. In a Vietnam study, the DTU being far away from the household was one of the reasons given by patients who had not initiated treatment. On the other hand, the distance between patient’s residence and the health facility was not associated with PLTFU in a single-hospital study from Ghana.
About 32% of the patients in our study had to travel for more than 30 km and 36%
traveled for more than 30 minutes from their homes to the DTUs where they were diagnosed. One possibility for this long travel could be that the DTUs may not be evenly distributed within these two regions where the patients lived. It could also be a matter of patients’ preferences of health facility. In other words, patients may not seek TB diagnosis at the nearest DTU with regard to their residence. Indeed, we did observe this phenomenon in our study when we visually inspected the distribution of TB patients by DTUs. Further explorative analyses on patients’ care seeking pathway will generate critical information on how to overcome the patients’ barrier to TB diagnosis
28
and treatment. Our future study will also look at identifying these TB hotspots of PLTFU after adjusting for population size.
The Xpert MTB/RIF assay is an automated, nucleic acid amplification test with a turn- around time of two hours. With the possibility of “same-day” TB diagnosis, use of Xpert MTB/RIF might lead to a decrease in PLTFU compared to smear microscopy, which requires multiple visits to the clinic. In a previous randomized controlled trial in southern Africa, the use of Xpert MTB/RIF at the point of care was associated with a lower proportion of PLTFU (2/182, 1%) when compared with smear microscopy (3/114, 3%), although the difference was not statistically significant.38 In our study, being diagnosed by Xpert MTB/RIF was however not associated with a decreased odds of PLTFU when compared to sputum microscopy in the multivariable analysis. In fact, in our third analysis where the retrospective and prospective data were combined, diagnosis by Xpert MTB/RIF was associated with a significantly increased odds of PLTFU (crude OR: 1.78, 95% CI: 1.29–2.47), which should be further investigated in future studies.
The DTUs located in urban settings need special attention in the sense that people being diagnosed at DTUs located in urban settings had a nearly 3-fold increased odds of not initiating treatment as compared with those who were diagnosed at DTUs located at rural areas (adjusted OR= 2.51, 95% CI: 1.51–4.17). One reason could be that some patients diagnosed at DTUs in urban areas may decide to travel to their localities of origin, usually at rural areas to be treated at DTUs closest to their family members for better family support. Another reason could be that those in urban settings may not want to be absent from work so as not to lose their daily wages. The rural/urban difference was also seen as a significant factor in a study conducted in Vietnam.
This study has some limitations. As a retrospective cohort study, it lacked certain key information about the patients such as marital status, income level, level of education, knowledge about TB, and medical co-morbidities. Although we collected information about referral status (i.e. those who were sent to initiate treatment at other centres) among those who did not initiate treatment, we were not able to conduct an active follow-up to ascertain the true outcome of those who had not initiated treatment as well as the reasons for PLTFU. Lastly, the geolocation of patient’s residence was estimated using an online geodatabase based on self-reported address, instead of onsite measurement.
5.2 Prospective study:
Being the first study in Cameroon to look at risk factors for PLTFU amongst TB patients, it has brought out some socioeconomic factors such as unemployment and lower salary. A higher salary of more than 60,000frs CFA (US$120) had a lower odds for not initiating TB treatment (aOR: 0.54, 95% CI: 0.32, 0.92). Salary discrepancies amongst TB patients have been found to affect their TB health-seeking behavior with lower salary having a higher tendency for PLTFU.9 This may probably be due to fear of the catastrophic costs usually incurred by TB sufferers and their families during TB treatment. Having a longer history of HIV test done (≥1 year) was found to have a higher odds of PLTFU compared to those who had a recent history (aOR: 2.05, 95% CI:
1.36, 3.09). The reasons for this might not be clear, but probably maybe due to the fact that these persons with longer history may not be taking their health very serious. HIV infection was equally found to be the main co-morbid condition amongst these patients.
Those from the South West region had a 90% increase odds for PLTFU compared to those in the North West region, (OR: 1.90, 95% CI: 1.27, 2.85). Patients attending
30
private health facilities were found to have a slightly higher odds for PLTFU compared with those attending public facilities (OR: 1.05, 95% CI: 0.71, 1.55), moreover, these patients attending private facilities were initiating treatment earlier (time-to-treatment) than those in public facilities (aHR: 1.45, 95% CI: 1.27, 1.64).
Importantly, our prospective study added the unique contribution of understanding the reasons of not initiating treatment timely (within seven days) by tracing the patients and inquiring about the reasons for PLTFU.
Though TB treatment itself is free in Cameroon, the issue of not initiating TB treatment as a result of inadequate money was also corroborated by 50% of PLTFU patients who gave their reasons as such. Additionally, some PLTFU patients (29.3%) said their homes were too far away from the DTU while about 12.2% of them were not willing to take TB treatment.
5.3 Impact evaluation of patient counselling and phone reminder study:
There was a significant difference or fall of PLTFU (6.9% absolute difference in terms of proportion of PLTFU) between the control group and the intervention group.
Therefore, counselling of TB patients and phone call reminders may have had an effect on this drop in PLTFU in the intervention group. In the regression discontinuity
analysis, however, neither of the intervention effect and the time trend effect were statistically significant, suggesting that the study did not have sufficient statistical power to precisely estimate the effect of the intervention after taking the underlying time trend into consideration. Therefore, our results need to be interpreted with caution. In
addition, it is unclear from the present analysis which component of the intervention (patient counselling or phone reminder) could be responsible for the decrease in PLTFU. Further studies may be required to decipher this change in PLTFU. Currently,
we are not aware of any study that had evaluated the impact of any intervention in reducing PLTFU, except a model that was suggested by Sharma et al.11 Randomized controlled trials could be conducted to further evaluate the impact of patients
counselling and phone reminders from the first day of diagnosis instead of a week after diagnosis.
5.4 Implications for tuberculosis control in Cameroon and worldwide
Being the first set of studies in Cameroon to look into the incidence and predictors of PLTFU of TB patients in the country, the importance of this phenomenon (PLTFU) amongst TB patients in the nation has been established. The results obtained from these studies have highlighted the problem of PLTFU versus programme performance. As a result, it will assist policy makers and the government of Cameroon in improving the potentials of the National TB Control Programme; thereby ameliorating the treatment outcome variables. Additionally, knowing some of the reasons why most patients do not initiate treatment earlier has brought to light some of the problems which majority of TB patients in Cameroon and likely most developing countries face.
Therefore, there is need for the National Tuberculosis Control Programme in Cameroon and the rest of the world to consider PLTFU as a relevant indicator in the global TB control effort especially as an attempt in the realization of the post-2015 sustainable development goals (SDGs).
32
CHAPTER 6. CONCLUSION
Although tuberculosis treatment is free in Cameroon, PLTFU amongst bacteriologically confirmed pulmonary tuberculosis patients is still a significant issue in these regions.
Access to TB diagnosis and treatment services remains a significant barrier to presumptive TB cases. There is still a considerable treatment delay amongst
bacteriologically confirmed pulmonary tuberculosis patients in Cameroon. Government will need to create more DTUs especially in far-away and enclaved places so that patients won’t spend a lot of money and time travelling long distances to access TB care. Patients need encouragement to seek care closest to their homes. Therefore, there is need for an increase in public awareness of the risk and consequences of TB
transmission within communities especially amongst the most active population in the society with more emphasis on those attending DTUs in urban areas. Strengthening civil society groups and encouraging public-private partnerships may help in tuberculosis control.
In these studies, we showed that PLTFU of bacteriologically confirmed pulmonary TB patients in Cameroon could be reduced significantly by including adequate pre- and post-test counseling of TB patients before they leave the laboratories, as a
recommendation to the NTP. There is a need to reconcile both TB laboratory and treatment registers in order to identify and trace those who had not initiated treatment.
Both government and non-governmental organizations could look for means of providing a national health insurance scheme so that patients could easily assess care irrespective of their income levels. Establishing poverty alleviation schemes may equally improve their income power, thereby affording care soonest. Increasing PLTFU awareness amongst healthcare providers will be very necessary in order to help mitigate the PLTFU trend.
More studies are required to study the impact of any intervention that could reduce the phenomenon of PLTFU in Cameroon or elsewhere.